
Abstract
Introduction
Ketamine’s efficacy in depressive disorders has been established in several controlled trials. The aim of the present study was to determine whether or not ketamine administration significantly improves depressive symptomatology in depression and more specifically in major depressive disorder (MDD), bipolar depression, resistant depression (non-ECT studies), and as an anesthetic agent in electroconvulsive therapy (ECT) for resistant depression (ECT studies). Secondary outcomes were the duration of ketamine’s effect, the efficacy on suicidal ideations, the existence of a dose effect, and the safety/tolerance of the treatment.
Methods
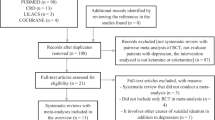
Studies were included if they met the following criteria (without any language or date restriction): design: randomized controlled trials, intervention: ketamine administration, participants: diagnosis of depression, and evaluation of severity based on a validated scale. We calculated standardized mean differences (SMDs) with 95 % confidence intervals (CIs) for each study. We used fixed and random effects models. Heterogeneity was assessed using the I2 statistic.
Results
We included nine non-ECT studies in our quantitative analysis (192 patients with major depressive disorder and 34 patients with bipolar depression). Overall, depression scores were significantly decreased in the ketamine groups compared to those in the control groups (SMD = −0.99; 95 % CI −1.23, −0.75; p < 0.01). Ketamine’s efficacy was confirmed in MDD (resistant to previous pharmacological treatments or not) (SMD = −0.91; 95 % CI −1.19,−0.64; p < 0.01), in bipolar depression (SMD = −1.34; 95 % CI −1.94, −0.75), and in drug-free patients as well as patients under medication. Four ECT trials (118 patients) were included in our quantitative analysis. One hundred and three patients were diagnosed with major depressive disorder and 15 with bipolar depression. Overall, depression scores were significantly improved in the 58 patients receiving ketamine in ECT anesthesia induction compared to the 60 patients (SMD = −0.56; 95 % CI −1.10, −0.02; p = 0.04; I2 = 52.4 %). The duration of ketamine’s effects was assessed in only two non-ECT studies and seemed to persist for 2–3 days; this result needs to be confirmed. Three of four studies found significant decrease of suicidal thoughts and one found no difference between groups, but suicidal ideations were only studied by the suicide item of the depressive scales. It was not possible to determine a dose effect; 0.5 mg/kg was used in the majority of the studies. Some cardiovascular events were described (mostly transient blood pressure elevation that may require treatment), and ketamine’s use should remain cautious in patients with a cardiovascular history.
Conclusion
The present meta-analysis confirms ketamine’s efficacy in depressive disorders in non-ECT studies, as well as in ECT studies. The results of this first meta-analysis are encouraging, and further studies are warranted to detail efficacy in bipolar disorders and other specific depressed populations. Middle- and long-term efficacy and safety have yet to be explored. Extrapolation should be cautious: Patients included had no history of psychotic episodes and no history of alcohol or substance use disorders, which is not representative of all the depressed patients that may benefit from this therapy.






Similar content being viewed by others


References
Abdallah CG, Fasula M, Kelmendi B, Sanacora G, Ostroff R (2012) Rapid antidepressant effect of ketamine in the electroconvulsive therapy setting. J ECT 28:157–161
Berman RM, Cappiello A, Anand A, Oren DA, Heninger GR, Charney DS, Krystal JH (2000) Antidepressant effects of ketamine in depressed patients. Biol Psychiatry 47:351–354
Borenstein M, Hedges LV, Higgins JPT, Rothstein HR (2009) Introduction to meta-analysis. Wiley, Chichester
Brewer CL, Davidson JR, Hereward S (1972) Ketamine (“Ketalar”): a safer anaesthetic for ECT. Br J Psychiatry 120:679–680
Calabrese JR, Huffman RF, White RL, Edwards S, Thompson TR, Ascher JA, Monaghan ET, Leadbetter RA (2008) Lamotrigine in the acute treatment of bipolar depression: results of five double-blind, placebo-controlled clinical trials. Bipolar Disord 10:323–333
Collins PY, Patel V, Joestl SS, March D, Insel TR, Daar AS, Scientific Advisory B, the Executive Committee of the Grand Challenges on Global Mental H, Anderson W, Dhansay MA, Phillips A, Shurin S, Walport M, Ewart W, Savill SJ, Bordin IA, Costello EJ, Durkin M, Fairburn C, Glass RI, Hall W, Huang Y, Hyman SE, Jamison K, Kaaya S, Kapur S, Kleinman A, Ogunniyi A, Otero-Ojeda A, Poo MM, Ravindranath V, Sahakian BJ, Saxena S, Singer PA, Stein DJ (2011) Grand challenges in global mental health. Nature 475:27–30
Cusin C, Hilton GQ, Nierenberg AA, Fava M (2012) Long-term maintenance with intramuscular ketamine for treatment-resistant bipolar II depression. Am J Psychiatry 169:868–869
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Diazgranados N, Ibrahim L, Brutsche NE, Newberg A, Kronstein P, Khalife S, Kammerer WA, Quezado Z, Luckenbaugh DA, Salvadore G, Machado-Vieira R, Manji HK, Zarate CA Jr (2010) A randomized add-on trial of an N-methyl-D-aspartate antagonist in treatment-resistant bipolar depression. Arch Gen Psychiatry 67:793–802
Ghasemi M, Kazemi MH, Yoosefi A, Ghasemi A, Paragomi P, Amini H, Afzali MH (2014) Rapid antidepressant effects of repeated doses of ketamine compared with electroconvulsive therapy in hospitalized patients with major depressive disorder. Psychiatry Res 215:355–361
Green CD (1973) Ketamine as an anaesthetic for ECT. Br J Psychiatry 122:123–124
Gross RA, Johnston KC (2009) Levels of evidence: taking neurology to the next level. Neurology 72:8–10
Harihar C, Dasari P, Srinivas JS (2013) Intramuscular ketamine in acute depression: a report on two cases. Indian J Psychiatry 55:186–188
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Higgins JPT, Altman DG, Sterne JAC (2011) Assessing risk of bias in included studies. In J. P. T. Higgins, & S. Green (Eds.), Cochrane handbook for systematic reviews of interventions version 5.1.0 (updated March 2011). The Cochrane Collaboration
Jarventausta K, Chrapek W, Kampman O, Tuohimaa K, Bjorkqvist M, Hakkinen H, Yli-Hankala A, Leinonen E (2013) Effects of S-ketamine as an anesthetic adjuvant to propofol on treatment response to electroconvulsive therapy in treatment-resistant depression: a randomized pilot study. J ECT 29:158–161
Kitagawa H, Yamazaki T, Akiyama T, Mori H, Sunagawa K (2001) Effects of ketamine on in vivo cardiac sympathetic nerve endings. J Cardiovasc Pharmacol 38(Suppl 1):S39–S42
Kranaster L, Hoyer C, Janke C, Sartorius A (2011) Preliminary evaluation of clinical outcome and safety of ketamine as an anesthetic for electroconvulsive therapy in schizophrenia. World J Biol Psychiatry
Krystal AD, Weiner RD, Dean MD, Lindahl VH, Tramontozzi LA 3rd, Falcone G, Coffey CE (2003) Comparison of seizure duration, ictal EEG, and cognitive effects of ketamine and methohexital anesthesia with ECT. J Neuropsychiatry Clin Neurosci 15:27–34
Kudoh A, Takahira Y, Katagai H, Takazawa T (2002) Small-dose ketamine improves the postoperative state of depressed patients. Anesth Analg 95:114–118
Loo CK, Katalinic N, Garfield JB, Sainsbury K, Hadzi-Pavlovic D, Mac-Pherson R (2012) Neuropsychological and mood effects of ketamine in electroconvulsive therapy: a randomised controlled trial. J Affect Disord 142:233–240
Mantel N, Haenszel W (1959) Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 22:719–748
McDaniel WW, Sahota AK, Vyas BV, Laguerta N, Hategan L, Oswald J (2006) Ketamine appears associated with better word recall than etomidate after a course of 6 electroconvulsive therapies. J ECT 22:103–106
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339:b2535
Morgan CJ, Curran HV (2011) Ketamine use: a review. Addiction 107:27–38
Murrough JW, Iosifescu DV, Chang LC, Al Jurdi RK, Green CM, Perez AM, Iqbal S, Pillemer S, Foulkes A, Shah A, Charney DS, Mathew SJ (2013) Antidepressant efficacy of ketamine in treatment-resistant major depression: a two-site randomized controlled trial. Am J Psychiatry
Okamoto N, Nakai T, Sakamoto K, Nagafusa Y, Higuchi T, Nishikawa T (2010) Rapid antidepressant effect of ketamine anesthesia during electroconvulsive therapy of treatment-resistant depression: comparing ketamine and propofol anesthesia. J ECT 26:223–227
Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, Niederehe G, Thase ME, Lavori PW, Lebowitz BD, McGrath PJ, Rosenbaum JF, Sackeim HA, Kupfer DJ, Luther J, Fava M (2006) Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry 163:1905–1917
Sos P, Klirova M, Novak T, Kohutova B, Horacek J, Palenicek T (2013) Relationship of ketamine’s antidepressant and psychotomimetic effects in unipolar depression. Neuro Endocrinol Lett 34:287–293
Souery D, Papakostas GI, Trivedi MH (2006) Treatment-resistant depression. J Clin Psychiatry 67(Suppl 6):16–22
Valentine GW, Mason GF, Gomez R, Fasula M, Watzl J, Pittman B, Krystal JH, Sanacora G (2011) The antidepressant effect of ketamine is not associated with changes in occipital amino acid neurotransmitter content as measured by [(1)H]-MRS. Psychiatry Res 191:122–127
Vassos E, Collier DA, Fazel S (2013) Systematic meta-analyses and field synopsis of genetic association studies of violence and aggression. Mol Psychiatry
Wang X, Chen Y, Zhou X, Liu F, Zhang T, Zhang C (2012) Effects of propofol and ketamine as combined anesthesia for electroconvulsive therapy in patients with depressive disorder. J ECT 28:128–132
Zarate CA Jr, Brutsche NE, Ibrahim L, Franco-Chaves J, Diazgranados N, Cravchik A, Selter J, Marquardt CA, Liberty V, Luckenbaugh DA (2012) Replication of ketamine’s antidepressant efficacy in bipolar depression: a randomized controlled add-on trial. Biol Psychiatry
Zarate CA Jr, Singh JB, Carlson PJ, Brutsche NE, Ameli R, Luckenbaugh DA, Charney DS, Manji HK (2006) A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry 63:856–864
Acknowledgments
We express all our thanks to the patients who participated in the studies included in the present meta-analysis and all the authors that answered our requests for missing data. This work was supported by INSERM, Assistance Publique—Hôpitaux de Paris, RTRS Santé Mentale (Fondation FondaMental), and by the Investissements d’Avenir program managed by the ANR under reference ANR-11-IDEX-0004-02.
Funding
No funding source.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix

Funnel plot
Rights and permissions
About this article

Cite this article
Fond, G., Loundou, A., Rabu, C. et al. Ketamine administration in depressive disorders: a systematic review and meta-analysis. Psychopharmacology 231, 3663–3676 (2014). https://doi.org/10.1007/s00213-014-3664-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-014-3664-5