
Abstract
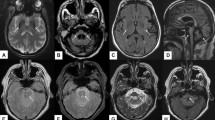
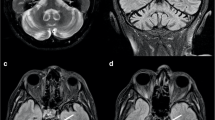
Fragile X-associated tremor ataxia syndrome (FXTAS) is caused by FMR1 premutation. The features include ataxia, action tremor and middle cerebellar peduncle (MCP) hyperintensity, the latter being the only major radiological criterion in the diagnosis of definite FXTAS until very recently. The importance of corpus callosum splenium (CCS) hyperintensity was recently reported and this sign is now considered as an additional major radiological diagnostic criterion in the diagnosis of FXTAS. However, little is known about its relevance for the diagnosis of FXTAS in clinical practice. We report a practical justification of the relevance of CCS hyperintensity in parallel with MCP hyperintensity for the diagnosis of FXTAS. Clinical and radiological study of 22 FMR1 premutation carriers with neurological signs that may be encountered in FXTAS compared to series of patients with essential tremor, multiple system atrophy of cerebellar type, Parkinson’s disease, Alzheimer’s disease and stroke. Among the 22 patients with FMR1 premutation [17 men, 5 women; mean age, 63 ± 7.5 (46–84)], 14 were diagnosed with definite FXTAS with the initial criteria. Considering CCS hyperintensity as a new major radiological criterion permitted the diagnosis of definite FXTAS in 3 additional patients. Overall CCS proved as frequent as MCP hyperintensity (64 versus 64 %), while 23 % of patients had CCS but not MCP hyperintensity, 14 % of patients had CCS hyperintensity but neither MCP, nor brainstem hyperintensity. In contrast with CCS hyperintensity, MCP hyperintensity proved less frequent in women than in men. CCS and MCP hyperintensity were more frequent in FXTAS than in the other neurodegenerative disorders. The combination of CCS and MCP hyperintensity was specific of FXTAS. We confirmed the relevance of CCS hyperintensity in FXTAS and we clarified its interest compared to MCP hyperintensity. Our results support the inclusion of CCS hyperintensity in the diagnostic criteria as a new major radiological criterion.

Similar content being viewed by others

References
Hagerman RJ, Leehey M, Heinrichs W, Tassone F, Wilson R, Hills J, Grigsby J, Gage B, Hagerman PJ (2001) Intention tremor, Parkinsonism, and generalized brain atrophy in male carriers of fragile X. Neurology 57:127–130
Jacquemont S, Hagerman RJ, Leehey M, Grigsby J, Zhang L, Brunberg JA, Greco C, Des Portes V, Jardini T, Levine R, Berry-Kravis E, Brown WT, Schaeffer S, Kissel J, Tassone F, Hagerman PJ (2003) Fragile X premutation tremor/ataxia syndrome: molecular, clinical, and neuroimaging correlates. Am J Hum Genet 72:869–878
Berry-Kravis E, Abrams L, Coffey SM, Hall DA, Greco C, Gane LW, Grigsby J, Bourgeois JA, Finucane B, Jacquemont S, Brunberg JA, Zhang L, Lin J, Tassone F, Hagerman PJ, Hagerman RJ, Leehey MA (2007) Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines. Mov Disord 22:2018–2030
Hall DA, Berry-Kravis E, Jacquemont S, Rice CD, Cogswell J, Zhang L, Hagerman RJ, Hagerman PJ, Leehey MA (2005) Initial diagnoses given to persons with the fragile X associated tremor/ataxia syndrome (FXTAS). Neurology 65:299–301
Leehey MA (2009) Fragile X-associated tremor/ataxia syndrome: clinical phenotype, diagnosis, and treatment. J Investig Med 57:830–836
Greco CM, Berman RF, Martin RM, Tassone F, Schwartz PH, Chang A, Trapp BD, Iwahashi C, Brunberg J, Grigsby J, Hessl D, Becker EJ, Papazian J, Leehey MA, Hagerman RJ, Hagerman PJ (2006) Neuropathology of fragile X-associated tremor/ataxia syndrome (FXTAS). Brain 129:243–255
Tassone F, Hagerman RJ, Taylor AK, Hagerman PJ (2001) A majority of fragile X males with methylated, full mutation alleles have significant levels of FMR1 messenger RNA. J Med Genet 38:453–456
Hagerman R, Hagerman P (2013) Advances in clinical and molecular understanding of the FMR1 premutation and fragile X-associated tremor/ataxia syndrome. Lancet Neurol 12:786–798
Ngai S, Tang YM, Du L, Stuckey S (2006) Hyperintensity of the middle cerebellar peduncles on fluid-attenuated inversion recovery imaging: variation with age and implications for the diagnosis of multiple system atrophy. AJNR Am J Neuroradiol 27:2146–2148
Apartis E, Blancher A, Meissner WG, Guyant-Marechal L, Maltete D, De Broucker T, Legrand AP, Bouzenada H, Thanh HT, Sallansonnet-Froment M, Wang A, Tison F, Roue-Jagot C, Sedel F, Charles P, Whalen S, Heron D, Thobois S, Poisson A, Lesca G, Ouvrard-Hernandez AM, Fraix V, Palfi S, Habert MO, Gaymard B, Dussaule JC, Pollak P, Vidailhet M, Durr A, Barbot JC, Gourlet V, Brice A, Anheim M (2012) FXTAS: new insights and the need for revised diagnostic criteria. Neurology 79:1898–1907
Hall DA, Birch R, Anheim M, Jonch AE, Pintado E, O’Keefe J, Troller J, Hagerman RJ, Fahn S, Berry-Kravis E, Leehey MA (2014) Emerging topics in FXTAS. J Neurodev Disord 6:31
Schmitz-Hubsch T, du Montcel ST, Baliko L, Berciano J, Boesch S, Depondt C, Giunti P, Globas C, Infante J, Kang JS, Kremer B, Mariotti C, Melegh B, Pandolfo M, Rakowicz M, Ribai P, Rola R, Schols L, Szymanski S, van de Warrenburg BP, Durr A, Klockgether T, Fancellu R (2006) Scale for the assessment and rating of ataxia: development of a new clinical scale. Neurology 66:1717–1720
Dubois B, Slachevsky A, Litvan I, Pillon B (2000) The FAB: a frontal assessment battery at bedside. Neurology 55:1621–1626
Folstein MF, Folstein SE, McHugh PR (1975) “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198
Fu YH, Kuhl DP, Pizzuti A, Pieretti M, Sutcliffe JS, Richards S, Verkerk AJ, Holden JJ, Fenwick RG Jr, Warren ST et al (1991) Variation of the CGG repeat at the fragile X site results in genetic instability: resolution of the Sherman paradox. Cell 67:1047–1058
Juncos JL, Lazarus JT, Graves-Allen E, Shubeck L, Rusin M, Novak G, Hamilton D, Rohr J, Sherman SL (2011) New clinical findings in the fragile X-associated tremor ataxia syndrome (FXTAS). Neurogenetics 12:123–135
Baba Y, Uitti RJ (2005) Fragile X-associated tremor/ataxia syndrome and movements disorders. Curr Opin Neurol 18:393–398
Leehey MA, Berry-Kravis E, Goetz CG, Zhang L, Hall DA, Li L, Rice CD, Lara R, Cogswell J, Reynolds A, Gane L, Jacquemont S, Tassone F, Grigsby J, Hagerman RJ, Hagerman PJ (2008) FMR1 CGG repeat length predicts motor dysfunction in premutation carriers. Neurology 70:1397–1402
Battistella G, Niederhauser J, Fornari E, Hippolyte L, Gronchi Perrin A, Lesca G, Forzano F, Hagmann P, Vingerhoets FJ, Draganski B, Maeder P, Jacquemont S (2013) Brain structure in asymptomatic FMR1 premutation carriers at risk for fragile X-associated tremor/ataxia syndrome. Neurobiol Aging 34:1700–1707
Conflicts of interest
The final manuscript has been read and approved by all authors who accepted full responsibility for the design and undertaking of the original article, had access to the data and controlled the decision to publish. MA declares conflict of interest with Novartis, Abbvie, TEVA/Lundbeck and Actelion. WM declares conflict of interest with TEVA/Lundbeck, Novartis, UCB, Affiris and GSK. The other authors have no conflict of interest to declare.
Ethical standard
Local ethics committees approved the study and all participants being informed gave written consent.
Author information
Authors and Affiliations
Corresponding author
Additional information
M. Renaud and J. Perriard contributed equally to this manuscript and should be considered as first author.
Rights and permissions
About this article

Cite this article
Renaud, M., Perriard, J., Coudray, S. et al. Relevance of corpus callosum splenium versus middle cerebellar peduncle hyperintensity for FXTAS diagnosis in clinical practice. J Neurol 262, 435–442 (2015). https://doi.org/10.1007/s00415-014-7557-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-014-7557-7