
Abstract
Objective
The identification of risk factors for COVID-19 adverse course in autoimmune rheumatic diseases (ARDs) is of the utmost importance when approaching patient management; however, data are scarce in relation to the Latin American population. The objective of this study was to determine predictors of hospitalization for COVID-19 patients from an ARD community cohort.
Methods
A real setting longitudinal study (March to November 2020) in an ARD community cohort was carried out. Potential predictors of hospitalization for COVID-19 examined included (1) sociodemographic variables (age, gender, education, tobacco use, socioeconomic status, and co-inhabitants), (2) comorbidities, (3) time to COVID-19 diagnosis, and (4) ARD’s features: clinical (disease type, disease duration, activity), treatment [corticosteroids use/doses, use of synthetic DMARDs (cDMARDs, tsDMARDs, and bDMARDs)], treatment schedule and non-adherence, and the Multidimensional Health Assessment Questionnaire (MDHAQ). Univariable and multivariable regression analysis were conducted; OR and 95% CI (p < 0.05) were determined.
Results
One thousand and one hundred forty-eight patients with ARDs were included; 154 had COVID-19; of these 139 (90.3%) were women, aged 52.5 (13.7) years; 33.1% had hypertension and 61.0% an affected organ by ARD. Infection was detected 8.4 (10.1) days after symptoms started; there were 33 hospitalized patients (rate 21.4%). Predictors of hospitalization by multivariable analysis were age (OR: 1.06; CI: 1.01–1.10; p: 0.01), comorbidities: hypertension (OR: 3.95; 95% CI: 1.40–10.95, p: 0.01) and neoplasm (OR: 9.0; 95% CI: 1.6–52.3; p: 0.01), number of organs involved by ARD (OR: 2.26; 95% CI: 1.16–4.41; p: 0.02), and infection diagnosis delay (OR: 1.36; 95% CI: 1.03–1.80; p: 0.01).
Conclusions
In our ARD patients with COVID-19, older age, comorbidities (neoplasm and hypertension), and a delay in COVID-19 diagnosis were predictors of hospitalization. The only ARD-associated predictor feature was the number of organs involved.
Key Points • Patients with ARD and COVID-19 have an adverse course in comparison to the general population. • Previous predictors of COVID-19 hospitalization, including known risk factors (such as older age and comorbidities) and systemic manifestations, should be taken into account in the management of these patients. • Delayed diagnosis of COVID-19 impacts negatively on prognosis. • Availability of diagnostic tests is of utmost importance. |
Similar content being viewed by others

Introduction
The new coronavirus disease (COVID-19) may cause severe acute respiratory syndrome and was declared a pandemic by the World Health Organization (WHO) in March 2020; case zero was reported in our country around the same time. Currently, Perú is one of the most affected countries in the world with over 1,460,779 COVID-19 cases confirmed by March 20, 2021 [1], a health problem which has had a severe impact on the general population and especially in patients with autoimmune rheumatic disease (ARD). Risk factors for the development of an adverse COVID-19 course include older age, male gender, the presence of chronic comorbidities such as diabetes mellitus (DM), lung disease (LD), obesity, chronic renal failure (CRF), neoplasms, cardiovascular diseases (CVD), chronic liver disease (CLD), among others [2,3,4,5,6]; several of them have been already described in ARD patients; however, there is inconsistent data about the impact of ARD clinical features such as the type of disease, activity status, or immunosuppressive treatment on the course and outcome of this infection. Published data about ARD and COVID-19 at the time this study began were limited to case reviews and case series, most of them coming from either China or Europe; conclusions from these initial reports assumed little risk of an adverse course in ARD patients in whom this infection had occurred; however, these studies included a relatively small number of patients [7,8,9,10,11,12,13]. Analysis carried out later by the Global Rheumatology Alliance Registry (GRA), the largest database of patients with rheumatological diseases affected by COVID-19, described the clinical characteristics of patients with this infection [14]; higher rates of hospitalization and lethality and risk factors for hospitalization such as comorbidities (hypertension, LD, DM, and CRF), and corticosteroid use were found [15].
The COVID-19 pandemic has been and continues to be critical in Latin America and that includes patients with ARDs; analysis from GRA USA data showed a higher risk of hospitalization in patients with a Latin American background (OR: 1.71, 95% CI: 1.18–2.49) in comparison to whites, with a three-fold increased risk of ventilatory support (OR: 3.25, 95% CI 1.75, 6.05) [16]; such adverse disease course could be explained by several factors including geographic location, socioeconomic disparities [17], and the near collapse of the health system in some of the countries of the region with the consequent reduction of opportunities for receiving care in their corresponding centers; determining early adverse predictors of COVID-19 in the context of community care is of utmost importance. The objective of our study was to determine the predictors of hospitalization in a cohort of ARD patients from a single rheumatological center followed up over several months in the community; the starting point for this study was March 11, 2020 which is the date the Peruvian government declared our country’s health to be in a state of emergency.
Methods
A longitudinal study of an ARD cohort followed up at a single medical center (Hospital Nacional Guillermo Almenara Irigoyen-EsSalud), a component of the Peruvian Social Security System, was conducted between March and November 2020 during the COVID-19 health emergency in our country. The study had the approval of the Hospital Ethics Committee and informed consent was obtained from the patients before they were enrolled and followed up. All ARD patients 18 years of age and older with a confirmed diagnosis and a minimum of 3 months of follow-up at our institution prior to enrollment were included. ARD included the following diagnosis: rheumatoid arthritis (RA), seronegative spondyloarthropathy including psoriatic arthropathy (PsA), systemic lupus erythematosus (SLE), systemic autoimmune vasculitis (SAV) including small, medium, and large vessels vasculitis, idiopathic inflammatory myopathies (polymyositis, dermatomyositis, and inclusion body myopathies, IIM), systemic sclerosis, Sjogren’s syndrome (SS), and other ARDs; in this category uncommon/infrequent rheumatologic diagnosis such as undifferentiated connective tissue diseases, overlapping syndromes, relapsing polychondritis, antiphospholipid syndrome, Bechet’s disease, IgG4 disease, polymyalgia rheumatica, and others were included. Patients without clinical or laboratory evidence of autoimmunity, even if an ARD diagnosis was noted on the medical records, were excluded. At the baseline visit the medical records were reviewed and sociodemographic and clinical data were obtained; the subjects were then followed up (Law 30,036, Supreme Decree No. 009–2015-TR) by a trained rheumatologist, by means of virtual or face-to-face visits; presential visits were performed depending on clinical status according to pre-defined investigators’ established criteria; in each visit, in addition to the assessment of clinical and treatment features, an electronic survey that included the study variables was administered, which also included symptoms of COVID-19 infection. The potential predictors of hospitalization considered were (1) sociodemographic: age, gender, education level, tobacco use, socioeconomic status (measured by the GRAFAR scale) [18], and the number of home co-inhabitants (shared common space); (2) pre-existing comorbidities: LD, hypertension, DM, cerebrovascular disease (CD), CVD such as valvular heart disease and cardiac arrhythmias [additionally, congestive heart failure (CHF) was collected as an independent variable], neoplasm, hypothyroidism, dyslipidemia, CRF including end stage renal disease, CLD, body mass index (BMI), and obesity (BMI of 30 or more kg/m2); (3) COVID-19 diagnostic delay defined as the number of days between the onset of symptoms and the diagnosis made by a physician; and (4) ARD’s clinical and treatment features including (a) disease features: disease type, disease duration, and disease activity status defined by the Clinical Disease Activity Index (CDAI) and the Routine Assessment of Patient Index Data 3 (RAPID-3) for RA, the SLE Disease Activity Index (SLEDAI), the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) for axial spondyloarthritis, and the Birmingham Vasculitis Activity Score version 3 (BVAS-v3) for SAV; for the rest of ARD disease activity status was defined by the investigator based on the number of organs involved, (b) treatment features such as (b.1) treatment non-adherence, (b.2) use and dose of corticosteroids (as a prednisone dose equivalence), (b.3) disease-modifying antirheumatic drugs (DMARDs): synthetic DMARDs [conventional (cDMARDs) and targeted synthetic (tsDMARDs)], biological (bDMARDs), and antimalarials, and (b.4) treatment schedule (mono or combined therapy), and (c) functional capacity assessed with the Multidimensional Health Assessment Questionnaire (MDHAQ). The cDMARDs considered were methotrexate, leflunomide, azathioprine, sulfasalazine, cyclosporine, mycophenolate mofetil, tacrolimus, cyclophosphamide, D penicillamine, and antimalarials. The bDMARDs included were anti-tumor necrosis factor (anti-TNF), rituximab, abatacept and within the tsDMARDs, tofacitinib and baricitinib. Use of these drugs was considered if the patients had received the drug for at least 3 months before the baseline visit; in addition, adherence to treatment was assessed at each follow-up visit using an open-ended question.
Clinical COVID-19 was defined if the subject had known associated symptoms (fever, headache, cough, sore throat, chest pain, odynophagia, respiratory distress, anosmia, dysgeusia, myalgia, or other reported), had compatible images on computerized tomography (CT) of the chest, and/or a positive epidemiological history (contact with a known subject infected by COVID-19); a confirmatory test (molecular and/or serological) was required. Incident cases were recorded at each visit; new COVID-19 cases were reported during the virtual visits using a platform developed during the emergency/contingency period.
The total incidence of COVID-19 infections was calculated dividing the number of new cases by the total number of patients in the cohort during the study period. In the same manner specific incidence by pathology was calculated dividing the number of new cases by the total number of patients for each ARD. COVID-19 cases were followed up to determine their clinical outcome (recovery, hospitalization, or death). In addition, lethality (number of deaths between total number of infected patients per 100) and mortality (number of deaths for the total number of patients in the cohort per 1000) rates were calculated.
Statistical analysis
Data for the continuous variables are described as means and standard deviations (SD), and for categorical variables as numbers and percentages. In order to evaluate the predictors of hospitalization, univariable and then multivariable binary logistic regression models were performed; variables with a p-value < 0.1 were entered into this model using a backward selection method; the alpha to stay in the model was set at 0.05. Results are reported as OR and their 95% confidence interval (CI). All statistical analyses were performed using SPSS v. 28.0 (IBM, Chicago, IL).
Results
A total of 1148 patients with ARD were followed up from March to November 2020; 154 of them developed COVID-19 with an incidence of 13.4%. The ARDs with the highest number of incident cases were SAV (17.8%), followed by RA (14.7%) and SLE (13.1%).
The mean age of the 154 patients afflicted by COVID-19 was 52.5 (13.7) years; the great majority of whom were women (139, 90.3%). There were no differences between patients who developed COVID-19 and the rest of the cohort in terms of age [54.8 (13.39) vs 52.5 (13.7) years; p = 0.07] and gender (86.8% vs 90.3% females; p = 0.23). The majority of patients were urban residents (143, 92.9%) and were from a medium low and low socioeconomic background (118, 76.6%). General baseline features of all ARD patients with SARS-CoV-2 infection are shown in Table 1. Ninety (58.4%) of the COVID-19 patients had some type of comorbidity, the most frequent being hypertension (33.1%) and LD (22.1%) with interstitial lung disease (ILD) secondary to ARD being the most frequent type (70.6%). More than half the patients had systemic manifestations with at least one organ involved (61.0%); kidneys (31.9%) and lungs (18.1%) were the most frequently affected organs. Almost a third of the patients (29.9%) were in clinical remission at the time the infection ensued. The mean CDAI and RAPID-3 index were 18.5(14.0) and 4.3(2.0), the mean SLEDAI was 2.0 (2.9), the mean BASDAI 3.2 (1.9), and the mean BVAS-v3 4.0 (8.7). Table 2 shows additional baseline clinical features of the ARD-COVID-19 patients.
The most frequently reported symptoms of COVID-19 infection were headache (57.8%), fever (51.1%), and cough (49.4%). Confirmatory CT of clinical pneumonia was demonstrated in 62 (40.5%) of all infected patients. The infection was confirmed in the majority of the cases by a serological test (86.3%). The mean (SD) delay in the diagnosis of the infection was 8.4 (10.1) days. Table 3 shows the clinical characteristics of COVID-19 infection in our ARD patients. There were thirty-three hospitalized (21.4%) of 154 COVID-19 infected patients being the mean (SD) number of days of hospitalization 5.5 (8.1). Laboratory tests at admission demonstrated a high level of ferritin [1762.02 (2332.9) ng/mL; cutoff: 5–148 in women and 28–365 in men], C-reactive protein [108.48 (90.27) IU/mL; cutoff: 5–10 IU/ml], aspartate aminotransferase [223.18 (28.77) IU/L; cutoff: 10–49 IU/L], and alanine aminotransferase [225.82 (31.83) IU/L; cutoff: 10–34 IU/L]. The white cell count was 11.2 (46.3) 103/μL, lymphocyte 0.2 (0.3) 103/μL, and platelet level 201.28 (81.072) 103/µL; cutoff: 150–500 103/µL. The mean D-dimer was 1.73 (1.29) µg/mL; cutoff < 0.40 µg/mL and fibrinogen 4.45 (0.68) g/L; cutoff 2–4.2 g/L. Twelve patients died, being the lethality rate 7.8% and the mortality rate 10.45 per 1000.
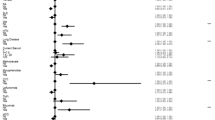
Predictors of hospitalization in univariable analysis were age (OR: 1.04; 95% CI: 1.00–1.08; p: 0.03), the number of cohabitants in the household (OR: 0.76; 95% CI: 0.61–0.95; p: 0.02), the presence and number of comorbidities (OR: 3.37; 95% CI: 1.26–9.01; p: 0.02 and OR: 7.28 95% CI: 2.42–21.89; p < 0.01, respectively), neoplasms (OR: 7.96; 95% CI: 1.77–35.77; p: 0.01), hypertension (OR: 3.77; 95% CI = 1.56–9.09; p: 0.01), and LD (OR: 2.94; 95% CI: 1.16–7.46: p: 0.02); clinical and treatment features of ARD associated with hospitalization were the presence of systemic involvement (OR: 3.03; 95% CI: 1.28–7.22; p: 0.01), the number of organs involved (OR: 2.17; 95% CI = 1.28–3.63; p: 0.00), the diagnosis of systemic autoimmune vasculitis (OR: 7.33; 95% CI: 1.42–37.87; p: 0.02), the use of corticosteroids (as prednisone) (OR: 1.13; 95% CI: 1.03–1.25; p: 0.02), and medium/high dose of this drug (OR: 4.08; 95% CI: 1.04–16.03; p: 0.04). Delay in the diagnosis of the infection was also a predictor (OR: 1.31; 95% CI = 1.05–1.63; p: 0.02). Variables significant in the multivariable analyses were age (OR: 1.06; 95% CI: 1.01–1.10; p: 0.01), comorbidities including neoplasms (OR: 9.06; 95% CI: 1.57–52.25; p: 0.01) and hypertension (OR: 3.95; 95% CI: 1.40–10.95, p: 0.01), the number of organs involved by the ARD (OR: 2.26; 95% CI: 1.16–4.41; p: 0.02), and the diagnostic delay of the infection (OR: 1.36; 95% CI: 1.03–1.80; p: 0.01). These data are depicted in Table 4.
Due to the non-homogeneous clinical manifestations of ARD disease, further analyses were performed considering three ARD’s subsets: (1) inflammatory joint diseases (RA and spondyloarthritis including PsA), (2) systemic connective tissue disease (SLE, inflammatory myopathies, and systemic sclerosis), and (3) a group including systemic vasculitis and other autoimmune conditions. In these analyses, we did not find differences in the rates of hospitalization or lethality (data not shown).
Discussion
In this longitudinal real-setting study of an ARD cohort followed up during several months, we have identified previously reported predictors of hospitalization in COVID-19, but, most importantly, we have identified factors associated with ARDs per se and a critical variable in terms of health community care: the delay in the diagnosis of this infection. To our knowledge, these data have not yet emanated from our region and up until now there is contradictory and scarce information from other parts of the world.
We found a higher incidence rate of COVID-19 infection with respect to our general population (the incidence of COVID-19 in Perú was about 4.1% for the period of this study) [19]; divergent data about this issue has been reported. Similarly to ours, a study from Spain found a cumulative incidence rate of 1.21%; 95% CI: 0.42–1.99% in ARD vs 0.58: 95% CI: 0.56–0.60 in the general population; although confirmatory tests were performed on both, symptomatic and asymptomatic ARD subjects that was not the case for the general population which could have led to an increase in the rate of infection in the first group [20]. In a study from the USA, a higher incidence of COVID-19 infections in ARD patients of Latin origin (17.97%) was found with respect to those of non-Latin origin (4.69 to 5.89%); the non-ARD Latin patients also had a higher infection rate than the non-Latin ones (1.54 to 3.43%) patients [21]. By contrast, in a study from China, a higher incidence of COVID-19 in the general population as compared to ARD patients (0.0142 vs 0.0126%) [22] was found. Finally, a systematic review and meta-analysis of 26 observational studies showed that patients with ARD had an increased risk of developing COVID-19 compared with the general population [23]. In addition, although the possible role of ethnicity per se cannot be discarded, our higher rates could be explained by the fact that we identified cases over a longer period of time and we also included patients from the community many of whom had a mild COVID-19 disease [24].
Our data provide indirect evidence of an adverse COVID-19 course in ARD patients with respect to the general Peruvian population, in terms of hospitalization and lethality rates reported during the same time period [19]; although these rates are variable in different studies around the world, two well designed studies indicate an adverse COVID-19 course in ARD patients. The first is the GRA registry in which higher rates in comparison with the data we are now reporting were found [15]; the differences between our study and the data from GRA could be related to the data collection methods (from each health service center in GRA and from the community in our study). The second study is a recent meta-analysis of 1138 patients from 38 studies; an even higher hospitalization and lethality rates (58% and 7%, respectively) were found [25]; however, no Latin American centers were included in these analyses. The design of our study did not permit us, however, to evaluate the risk of hospitalization in ARD in comparison to non-ARD patients, although currently there are no conclusive data about higher risks of hospitalization, lethality, or respiratory failure in ARD patients as compared with the general population [26,27,28,29,30].
Concerning previously described predictors of adverse course of COVID-19, we were able to corroborate the role of older age and chronic comorbidities (hypertension and neoplasm) as previously reported [15, 26, 31,32,33,34,35,36]. A recent meta-analysis found comorbidities (OR = 2.41, 95%; CI = 1.04–5.61; p = 0.041), hypertension (OR = 3.69; 95% CI = 1.41–9.69; p = 0.008), and lung diseases (OR = 2.93; 95% CI = 1.64–5.23; p = 0.000) significantly associated with hospitalizations [23]. We identified predictors of hospitalization; however, we were unable to do the same analysis for lethality due to the relatively small sample size.
Few data have been published so far about the possible role ARD’s clinical features may exert in the course of COVID-19 either as an additional risk or a protective one against the infection. We found the presence of systemic ARD clinical manifestations but no other clinical parameters, to be predictive of an adverse course. Although there is some evidence about the impact of active disease [36] or having systemic connective disease including SLE [33] and certain types of inflammatory arthritis (PsA and RA, for example) as risk factors for severe course including death [37, 38] and hospital admissions [30, 33, 39], no data about the impact of systemic or target organ involvement on COVID-19 course has been reported.
Divergent results about the impact of ARD’s treatment features in adverse COIVD 19 courses exist in terms of hospitalization [15, 30, 36, 40, 41], lethality [40, 42, 43], and intensive care unit admissions [33, 44]; the majority of these studies have explored the role of bDMARDs and tsDMARDs and have shown evidence that monotherapy (b/DMARDs or tsDMARDs) could be protective against adverse course [15, 45]. We have not been able to demonstrate that any treatment type or schedule confer a deleterious or protective risk for the course of COVID-19; however, our cohort had a small number of patients on bDMARDs and tsDMARDs which could have impacted on our results. Regarding antimalarials, we did not find any protective effect and no conclusive data are currently available [28, 30, 31, 45, 46]; we did not identify corticosteroids use or doses as a risk factor for hospitalization (doses higher than 5 [32, 34] or 10 mg/day [15] have been reported previously); however, these differences could be explained by the low doses of corticosteroid use in the majority of our patients (and none on a high doses). The low number of each ARD type did not permit us to examine the impact of the treatment on each subset of disease.
An important result in our study relates to community health care: a longer time to confirm COVID-19 diagnosis after initial symptoms (a mean of 8 days, considered late) was found to be a predictor of hospitalization. The COVID-19 pandemic has had a serious impact on the health care system around the world, with middle/low-income countries experiencing worse impact. No studies about this delay in COVID-19 diagnosis have been described before in ARDs and even in the general population there is a scarcity of data. A systematic review which examined predictors of hospitalization for COVID-19 in ARD patients found few studies exploring this variable [47] and the data currently available are still controversial [48,49,50]; however, this variable could be critical in terms of mortality if the health system collapses or is near collapse; for example, a low level of oxygen saturation at admission has been found to be associated with mortality in a recent Peruvian study; once again a delay in hospitalization of about 8 days since initial symptoms was observed in that study [51]. We considered our results to be of the utmost importance in the care of patients with ARDs in the community.
Our study has some limitations, the most important being the potential underreporting of cases due to the confirmatory serologic method being used instead of molecular tests, due to their relative inaccessibility and cost in our country; the same situation relates to the opportunity for hospitalization (patients with moderate/severe forms of infection could not have been admitted and thus, are not recorded); and the requirement for intensive care admissions. Given that COVID-19 disease was defined by a confirmatory test or images, it is likely that mild forms with negative serological tests (especially during the initial days of the pandemic), no molecular tests and without imaging evidence, may have not been properly recorded. We have, nevertheless, the advantage of collecting potential clinical parameters predictors adequately before the event and over a long follow-up period. On the other hand, our center forms part of a social security health care system with a regularity in visits, access to health services, and baseline features fully corroborated by an electronic medical record. Also, the remote follow-up model with electronic questionnaire surveys in each visit and the virtual platform created guarantees the collection of most incident cases.
In conclusion, we were able to identify previously described predictive factors of hospitalization in patients with ARD and COVID-19, such as age and comorbidities including a predictor related to the clinical features of the ARD (the number of organs involved). Of greater interest in community medical care, we have identified delay in diagnosis of COVID-19 infection as a predictor of adverse course. The profile of this type of ARD patient must be considered for an opportune management in the context of the COVID-19 pandemic.
References
Johns Hopkins University Coronavirus resource center. Available from https://coronavirus.jhu.edu/map.html. Cited March 20, 2021
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z et al (2020) Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 395(10229):1054–1062. https://doi.org/10.1016/S0140-6736(20)30566-3
Galbadage T, Peterson BM, Awada J, Buck AS, Ramirez DA, Wilson J et al (2020) Systematic review and meta-analysis of sex-specific COVID-19 clinical outcomes. Front Med (Lausanne) 7:348. https://doi.org/10.3389/fmed.2020.00348
Földi M, Farkas N, Kiss S, Zádori N, Váncsa S, Szakó L et al (2020) Obesity is a risk factor for developing critical condition in COVID-19 patients: a systematic review and meta-analysis. Obes Rev 21(10):e13095. https://doi.org/10.1111/obr.13095
Awortwe C, Cascorbi I (2020) Meta-analysis on outcome-worsening comorbidities of COVID-19 and related potential drug-drug interactions. Pharmacol Res 161:105250. https://doi.org/10.1016/j.phrs.2020.105250
Udwadia ZF, Tripathi AR, Nanda VJ, Joshi SR (2020) Prognostic factors for adverse outcomes in COVID-19 infection. J Assoc Physicians India 68(7):62–66
Sharmeen S, Elghawy A, Zarlasht F, Yao Q (2020) COVID-19 in rheumatic disease patients on immunosuppressive agents. Semin Arthritis Rheum 50(4):680–686. https://doi.org/10.1016/j.semarthrit.2020.05.010
Cheng C, Li C, Zhao T, Yue J, Yang F, Yan Y et al (2020) COVID-19 with rheumatic diseases: a report of 5 cases. Clin Rheumatol 39(7):2025–2029. https://doi.org/10.1007/s10067-020-05160-x
Emmi G, Bettiol A, Mattioli I, Silvestri E, Di Scala G, Urban ML et al (2020) SARS-CoV-2 infection among patients with systemic autoimmune diseases. Autoimmun Rev 19(7):102575. https://doi.org/10.1016/j.autrev.2020.102575
Monti S, Balduzzi S, Delvino P, Bellis E, Quadrelli VS, Montecucco C (2020) Clinical course of COVID-19 in a series of patients with chronic arthritis treated with immunosuppressive targeted therapies. Ann Rheum Dis 79(5):667–668. https://doi.org/10.1136/annrheumdis-2020-217424
Favalli E, Agape E, Caporali R (2020) Incidence and clinical course of COVID-19 in patients with connective tissue diseases: a descriptive observational analysis. J Rheumatol 7(8):1296. https://doi.org/10.3899/jrheum.200507
Zen M, Fuzzi E, Astorri D, Saccon F, Padoan R, Ienna L et al (2020) SARS-CoV-2 infection in patients with autoimmune rheumatic diseases in northeast Italy: a cross-sectional study on 916 patients. J Autoimmun 112:102502. https://doi.org/10.1016/j.jaut.2020.102502
Murray K, Quinn S, Turk M, O’Rourke A, Molloy E, O’Neill L et al (2021) COVID-19 and rheumatic musculoskeletal disease patients: infection rates, attitudes and medication adherence in an Irish population. Rheumatology (Oxford) 60(2):902–906. https://doi.org/10.1093/rheumatology/keaa694In
Gianfrancesco MA, Hyrich KL, Gossec L, Strangfeld A, Carmona L, Mateus EF et al (2020) Rheumatic disease and COVID-19: initial data from the COVID-19 Global Rheumatology Alliance provider registries. Lancet Rheumatol 2(5):e250–e253. https://doi.org/10.1016/S2665-9913(20)30095-3
Gianfrancesco M, Hyrich KL, Al-Adely S, Carmona L, Danila MI, Gossec L et al (2020) Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: data from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann Rheum Dis 79(7):859–866. https://doi.org/10.1136/annrheumdis-2020-217871
Gianfrancesco MA, Leykina LA, Izadi Z, Taylor T, Sparks JA, Harrison C, et al (2020) Race/ethnicity association with COVID-19 outcomes in rheumatic disease: data from the COVID-19 Global Rheumatology Alliance Physician Registry. Arthritis Rheumatol. https://doi.org/10.1002/art.41567
Elera-Fitzcarrald C, Ugarte-Gil MF, Alarcón GS (2020) COVID-19 and its potential effect on patients with rheumatic diseases in Latin America. J Clin Rheumatol 26(6):215–217. https://doi.org/10.1097/RHU.0000000000001493
Méndez H, de Méndez MC (1994) Sociedad y estratificación: método Graffar-Méndez Castellano. Caracas: Fundacredesa
Sala situacional COVID-19 MINSA. https://covid19.minsa.gob.pe/sala_situacional.asp. Acceded Jan 11, 2021
Michelena X, Borrell H, López-Corbeto M, López-Lasanta M, Moreno E, Pascual-Pastor M et al (2020) Incidence of COVID-19 in a cohort of adult and paediatric patients with rheumatic diseases treated with targeted biologic and synthetic disease-modifying anti-rheumatic drugs. Semin Arthritis Rheum 50(4):564–570. https://doi.org/10.1016/j.semarthrit.2020.05.001
Fike A, Hartman J, Redmond C, Williams SG, Ruiz-Perdomo Y, Chu J, et al (2021) Risk factors for COVID-19 and rheumatic disease flare in a US cohort of Latino patients. Arthritis Rheumatol. https://doi.org/10.1002/art.41656
So H, Mak JW, So J, Lui G, Lun F, Lee J et al (2020) Incidence and clinical course of COVID-19 in patients with rheumatologic diseases: a population-based study. Semin Arthritis Rheum 50(5):885–889. https://doi.org/10.1016/j.semarthrit.2020.07.012
Wang Q, Liu J, Shao R, Han X, Su C, Lu W (2021) Risk and clinical outcomes of COVID-19 in patients with rheumatic diseases compared with the general population: a systematic review and meta-analysis. Rheumatol Int 41(5):851–861. https://doi.org/10.1007/s00296-021-04803-9
Favalli EG, Ingegnoli F, Cimaz R, Caporali R (2021) What is the true incidence of COVID-19 in patients with rheumatic diseases? Ann Rheum Dis 80(2):e18. https://doi.org/10.1136/annrheumdis-2020-217615
Xu C, Yi Z, Cai R, Chen R, Thong BY, Mu R (2021) Clinical outcomes of COVID-19 in patients with rheumatic diseases: a systematic review and meta-analysis of global data. Autoimmun Rev 20(4):102778. https://doi.org/10.1016/j.autrev.2021.102778
Haberman RH, Castillo R, Chen A, Yan D, Ramirez D, Sekar V et al (2020) COVID-19 in patients with Inflammatory arthritis: a prospective study on the effects of comorbidities and disease-modifying antirheumatic drugs on clinical outcomes. Arthritis Rheumatol 72(12):1981–1989. https://doi.org/10.1002/art.41456
Wu Z, McGoogan JM (2020) Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 323(13):1239–1242. https://doi.org/10.1001/jama.2020.2648
Ye C, Cai S, Shen G, Guan H, Zhou L, Hu Y et al (2020) Clinical features of rheumatic patients infected with COVID-19 in Wuhan. China Ann Rheum Dis 79(8):1007–1013. https://doi.org/10.1136/annrheumdis-2020-217627
D’Silva KM, Serling-Boyd N, Wallwork R, Hsu T, Fu X, Gravallese EM et al (2020) Clinical characteristics and outcomes of patients with coronavirus disease 2019 (COVID-19) and rheumatic disease: a comparative cohort study from a US ‘hot spot.’ Ann Rheum Dis 79(9):1156–1162. https://doi.org/10.1136/annrheumdis-2020-217888
Cordtz R, Lindhardsen J, Soussi B, Vele J, Uhrenholt L, Westermann R, et al (2020) Incidence and severeness of COVID-19 hospitalisation in patients with inflammatory rheumatic disease: a nationwide cohort study from Denmark. Rheumatology (Oxford) 28:keaa897. https://doi.org/10.1093/rheumatology/keaa897
Freites Nuñez DD, Leon L, Mucientes A, Rodriguez-Rodriguez L, Font Urgelles J, Madrid García A et al (2020) Risk factors for hospital admissions related to COVID-19 in patients with autoimmune inflammatory rheumatic diseases. Ann Rheum Dis 79(11):1393–1399. https://doi.org/10.1136/annrheumdis-2020-217984
Montero F, Martínez-Barrio J, Serrano-Benavente B, González T, Rivera J, Molina Collada J et al (2020) Coronavirus disease 2019 (COVID-19) in autoimmune and inflammatory conditions: clinical characteristics of poor outcomes. Rheumatol Int 40(10):1593–1598. https://doi.org/10.1007/s00296-020-04676-4
Pablos JL, Galindo M, Carmona L, Lledó A, Retuerto M, Blanco R et al (2020) Clinical outcomes of hospitalised patients with COVID-19 and chronic inflammatory and autoimmune rheumatic diseases: a multicentric matched cohort study. Ann Rheum Dis 79(12):1544–1549. https://doi.org/10.1136/annrheumdis-2020-218296
Nuño L, Novella Navarro M, Bonilla G, Franco-Gómez K, Aguado P, Peiteado D et al (2020) Clinical course, severity and mortality in a cohort of patients with COVID-19 with rheumatic disease. Ann Rheum Dis 79(12):1659–1661. https://doi.org/10.1136/annrheumdis-2020-218054
FAI2R /SFR/SNFMI/SOFREMIP/CRI/IMIDIATE consortium and contributors (2020) Severity of COVID-19 and survival in patients with rheumatic and inflammatory diseases: data from the French RMD COVID-19 cohort of 694 patients. Ann Rheum Dis 80(4):527–538. https://doi.org/10.1136/annrheumdis-2020-218310
Hasseli R, Mueller-Ladner U, Hoyer BF, Krause A, Lorenz HM, Pfei et al (2021) Older age, comorbidity, glucocorticoid use and disease activity are risk factors for COVID-19 hospitalisation in patients with inflammatory rheumatic and musculoskeletal diseases. RMD Open 7(1):e001464. https://doi.org/10.1136/rmdopen-2020-001464
Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE et al (2020) Factors associated with COVID-19-related death using OpenSAFELY. Nature 584(7821):430–436. https://doi.org/10.1038/s41586-020-2521-4
Ji W, Huh K, Kang M, Hong J, Bae GH, Lee R et al (2020) Effect of underlying comorbidities on the infection and severity of COVID-19 in Korea: a nationwide case-control study. J Korean Med Sci 35(25):e237
Pablos JL, Abasolo L, Alvaro-Gracia JM, Blanco FJ, Blanco R, Castrejón I et al (2020) Prevalence of hospital PCR-confirmed COVID-19 cases in patients with chronic inflammatory and autoimmune rheumatic diseases. Ann Rheum Dis 79(9):1170–1173. https://doi.org/10.1136/annrheumdis-2020-217763
Sanchez-Piedra C, Diaz-Torne C, Manero J, Pego-Reigosa JM, Rúa-Figueroa Í, Gonzalez-Gay MA et al (2020) Clinical features and outcomes of COVID-19 in patients with rheumatic diseases treated with biological and synthetic targeted therapies. Ann Rheum Dis 79(7):988–990. https://doi.org/10.1136/annrheumdis-2020-217948
Salvarani C, Bajocchi G, Mancuso P, Galli E, Muratore F, Boiardi L et al (2020) Susceptibility and severity of COVID-19 in patients treated with bDMARDS and tsDMARDs: a population-based study. Ann Rheum Dis 79(7):986–988. https://doi.org/10.1136/annrheumdis-2020-217903
Santos CS, Morales CM, Álvarez ED, Castro CÁ, Robles AL, Sandoval TP (2020) Determinants of COVID-19 disease severity in patients with underlying rheumatic disease. Clin Rheumatol 39(9):2789–2796. https://doi.org/10.1007/s10067-020-05301-2-
Strangfeld A, Schäfer M, Gianfrancesco MA, Lawson-Tovey S, Liew JW, Ljung L, et al (2021) Factors associated with COVID-19-related death in people with rheumatic diseases: results from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann Rheum Dis annrheumdis-2020–219498. https://doi.org/10.1136/annrheumdis-2020-219498
Quartuccio L, Valent F, Pasut E, Tascini C, De Vita S (2020) Prevalence of COVID-19 among patients with chronic inflammatory rheumatic diseases treated with biologic agents or small molecules: a population-based study in the first two months of COVID-19 outbreak in Italy. Joint Bone Spine 87(5):439–443. https://doi.org/10.1016/j.jbspin.2020.05.003
Akiyama S, Hamdeh S, Micic D, Sakuraba A (2020) Prevalence and clinical outcomes of COVID-19 in patients with autoimmune diseases: a systematic review and meta-analysis. Ann Rheum Dis annrheumdis-2020–218946. https://doi.org/10.1136/annrheumdis-2020-218946
Mathian A, Mahevas M, Rohmer J, Roumier M, Cohen-Aubart F, Amador-Borrero B et al (2020) Clinical course of coronavirus disease 2019 (COVID-19) in a series of 17 patients with systemic lupus erythematosus under long-term treatment with hydroxychloroquine. Ann Rheum Dis 79(6):837–839. https://doi.org/10.1136/annrheumdis-2020-217566
Wynants L, Van Calster B, Collins GS, Riley RD, Heinze G, Schuit E et al (2020) Prediction models for diagnosis and prognosis of covid-19 infection: systematic review and critical appraisal. BMJ 369:m1328. https://doi.org/10.1136/bmj.m1328
Cobre AF, Böger B, Fachi MM, Vilhena RO, Domingos EL, Tonin FS et al (2020) Risk factors associated with delay in diagnosis and mortality in patients with COVID-19 in the city of Rio de Janeiro. Brazil Cien Saude Colet 25(suppl 2):4131–4140. https://doi.org/10.1590/1413-812320202510.2.26882020
Pfoh ER, Hariri EH, Misra-Hebert AD, Deshpande A, Jehi L, Rothberg MB (2020) Late diagnosis of COVID-19 in patients admitted to the hospital. J Gen Intern Med 35(9):2829–2831. https://doi.org/10.1007/s11606-020-05949-1
Li L, Sun W, Han M, Ying Y, Wang Q (2020) A study on the predictors of disease severity of COVID-19. Med Sci Monit 26:e927167. https://doi.org/10.12659/MSM.927167
Mejía F, Medina C, Cornejo E, Morello E, Vásquez S, Aleva J et al (2020) Oxygen saturation as a predictor of mortality in hospitalized adult patients with COVID-19 in a public hospital in Lima. Peru PLoS One 15(12):e0244171. https://doi.org/10.1371/journal.pone.0244171
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gamboa-Cárdenas, RV., Barzola-Cerrón, S., Toledo-Neira, D. et al. Predictors of hospitalization for COVID-19 in patients with autoimmune rheumatic diseases: results from a community cohort follow-up. Clin Rheumatol 40, 4725–4734 (2021). https://doi.org/10.1007/s10067-021-05833-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-021-05833-1