
Abstract
Dromedary, or one-humped, camels Camelus dromedarius are an almost exclusively domesticated species that are common in arid areas as both beasts of burden and production animals for meat and milk. Currently, there are approximately 30 million dromedary camels, with highest numbers in Africa and the Middle East. The hardiness of camels in arid regions has made humans more dependent on them, especially as a stable protein source. Camels also carry and may transmit disease-causing agents to humans and other animals. The ability for camels to act as a point source or vector for disease is a concern due to increasing human demands for meat, lack of biosafety and biosecurity protocols in many regions, and a growth in the interface with wildlife as camel herds become sympatric with non-domestic species. We conducted a literature review of camel-borne zoonotic diseases and found that the majority of publications (65%) focused on Middle East respiratory syndrome (MERS), brucellosis, Echinococcus granulosus, and Rift Valley fever. The high fatality from MERS outbreaks during 2012–2016 elicited an immediate response from the research community as demonstrated by a surge of MERS-related publications. However, we contend that other camel-borne diseases such as Yersinia pestis, Coxiella burnetii, and Crimean–Congo hemorrhagic fever are just as important to include in surveillance efforts. Camel populations, particularly in sub-Saharan Africa, are increasing exponentially in response to prolonged droughts, and thus, the risk of zoonoses increases as well. In this review, we provide an overview of the major zoonotic diseases present in dromedary camels, their risk to humans, and recommendations to minimize spillover events.
Similar content being viewed by others

Introduction
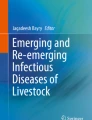
Worldwide there are roughly 30 million dromedary camels, with highest numbers found in Africa and the Middle East (Figure 1). Due to increased consumption and contact with camel meat and milk, camels represent a significant point source for zoonotic disease transmission to humans. Pastoralist camel production, in particular, is associated with a risk of disease spillover from wildlife into camel populations, and from camels to wildlife, as well as less opportunities for disease surveillance and control. By 2050 the human population is projected to grow by 2.5 billion, with nearly half of all population growth occurring in the African continent (Roser 2018). Along with the increase in human population in Africa and the Middle East, the camel population has also experienced steady growth as the demand and production of camel meat and milk escalates (FAOSTAT 2016). More and more, nomadic herders are switching to an agricultural or urban setting to raise camels and this change in camel production brings potential risks of disease emergence and transmission. In addition, with the realities of climate change and the increase in drought conditions, camel hardiness has led to a shift in livestock choice in many regions of the world from cattle to camels, making camels even more abundant (Watson et al. 2016)

Map of domesticated dromedary camel population by country in 2016; data from Food and Agricultural Organization (Food and Agricultural Organization, 2016)
Limited resources, low levels of regulation, poor hygiene, high mobility of animals and herders, and lack of consistent veterinary care also act as drivers for disease spillover (Gossner et al. 2016; Megersa et al. 2011). Knowledge of camel-borne diseases, clinical signs, and pathways of transmission is thus important to mitigate human risks of camel-associated zoonoses. Many infectious diseases that have been an issue in Africa and the Middle East during the last decades, such as Middle East respiratory syndrome (MERS) and brucellosis, have an association with camel contact (Ahmed et al. 2010; Ferguson and Van Kerkhove 2014). Additionally, novel camel-borne diseases continue to be identified, as best exemplified by reports of a prion disease from Algerian abattoir camels published during the editing of this review paper (Babelhadj et al. 2018)
Significant research on seropositivity and detection of specific diseases of camels, those that have implications for human health, has been conducted; however, to the authors’ knowledge no publication has summarized the current literature on these zoonotic diseases. Realizing the need for a thorough review of the literature to identify the risks that camels pose to human health was the impetus for this review. In this paper, we review publications of the most common confirmed and potential camel zoonoses of interest: bacterial, viral, and parasitic, and offer recommendations for surveillance and control of the diseases of highest priority.
Methods
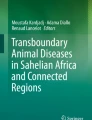
We utilized two search engines, Google Scholar and PubMed, to search for publications related to camel-borne disease and zoonotic spillover. We chose Google Scholar for breadth and volume of content, while PubMed was chosen from medical and public health-specific search engines for its specificity. Publications on Bactrian camels Camelus bactrianus were excluded because they are primarily wild but are used as beasts of burden and food in select countries and only account for 2 million out of 30 million total camels (IUCN 2008). To cast a wide net for possible diseases we did not search for specific zoonotic diseases and instead classified publications by disease after the initial literature search. All search terms included the words camel and human as well as one of six other words keywords: camel + human + zoonotic, illness, spillover, outbreak, transmission, or disease. For each set of search terms, we reviewed the first 100 results for relevancy or all results if < 100. Included publications were restricted to those written in English, but there was no date limit, no other restrictions were set, and papers were sorted by relevance. From a total of 1054 papers, 619 were unique or non-duplicates and 304 of these were relevant (Figure 2). Five of these 304 papers reported on multiple diseases. Results that were excluded included papers that inconclusively related to transmission from camels n = 96, non-camelid animals n = 40, studies that focused on vaccines n = 25, camel-specific diseases n = 22, articles/seminars n = 15, and non-relevant topics n = 117. Examples of non-relevance were papers that did not mention camels at all, papers that did not discuss transmission of disease, papers on human-to-human transmission, or papers that discussed laboratory testing and techniques related to these diseases. Food-borne bacterial diseases from pathogens such as Escherichia coli, Salmonella, and Campylobacter were consolidated into one category termed “food-borne” because they share transmission pathways, have similar symptoms, and were pre-grouped by several publications in this review. We also elected to present these pathogens in this fashion because there was a precedence set by said publications. Papers with positive serologic testing in camels, probable disease through an explained epidemiologic link between human disease and camel-borne pathogens, and isolation of similar strains in humans and camels fit criteria for inclusion. Relevant papers were sorted into bacterial, viral, and parasitic categories along with recorded counts for each disease. Results were separated out in this manner to cover scope number of diseases as well as depth number of papers per disease. Figures were created in Quantum GIS 3.6 (QGIS Development Team 2019). We completed the literature search in February and March of 2018.

Methodology for inclusion and exclusion of publications of camel-borne zoonoses. Out of an initial 1054 eligible publications, 619 were unique and non-duplicate and 304 of those were included in the final selection of journal articles for further analysis
Results
Through this literature review, we identified 304 papers published between 1970 and 2018 that described disease agents in camels with probable (see above definition) or confirmed transmission to humans. Thirty-seven camel-borne diseases were identified, comprised of 12 bacterial diseases, 13 viral diseases, and 12 parasitic diseases (Table 1). The most frequently occurring diseases or disease-causing agents in this study were MERS n = 118, Echinococcus granulosus n = 46, brucellosis n = 35, and Rift Valley fever n = 19. In this study, 42 countries were represented in the literature, with most papers originating from Saudi Arabia n = 36, Iran n = 27, Kenya n = 15, and Egypt n = 14 (Figure 3). There has been a dramatic increase in publications over the last eight years with a peak during 2012–2016, when research on MERS was undertaken in a number of laboratories following the first diagnosis of a human fatality reported in 2012 (Fig. 4) (Kupferschmidt 2014).

Number of publications by country of study, range n = 1 Finland, Argentina to n = 36 Saudi Arabia

Frequency of camel-borne disease publications between 1970 and 2018 identified in this review
Viral
The large majority of publications were related to MERS n = 118, a novel coronavirus. Genetic comparisons between camel and human isolated MERS are highly similar and camels continue to exhibit positive seropositivity for MERS in recent tests (Chu et al. 2018).
The review identified 19 papers on Rift Valley fever (RVF) transmission, most of which detailed how common seropositivity to RVF virus was in camel herds. Four of these papers emphasized that livestock like camels, cattle, and sheep served as important amplifiers for the virus, especially prior to outbreaks in Kenya and Mauritania (Bird et al. 2008; Britch et al. 2013; El Mamy et al. 2011, 2014).
Four of nine publications on Camelpox discussed human transmission, including a paper that reported the first laboratory-confirmed case of human Camelpox (Bera et al. 2011).
There were five papers on hepatitis E, one of the five known human hepatitis virus strains, in which camel meat and milk were implicated as risk factors in humans through whole-genome sequencing, HEV IgM, or HEV RNA detection (Pavio et al. 2015 Khuroo and Khuroo 2016; Lee et al. 2016; Rasche et al. 2016; Spahr et al. 2018). In one of these reports, a liver transplant patient in the United Arab Emirates consumed camel meat and milk regularly and was chronically infected with hepatitis E (Lee et al. 2016).
While no publication documented clinical evidence of camel–human rabies transmission, one paper presented probable evidence of camel-to-human rabies transmission (Bloch and Diallo 1995).
A 2018 publication noted that HCoV-229E, a primarily non-lethal coronavirus responsible for a proportion of upper and lower respiratory tract infections, can be transmitted from camels to humans similar to MERS transmission, thus implicating dromedary camels as a possible reservoir of coronaviruses (Corman et al. 2018). Woo et al. (2014) identified a novel betacoronavirus UAE-HKU23 or dromedary camel coronavirus DcCOV in the United Arab Emirates that was detected in 52% of tested camel serum samples.
Other viruses that were found in camels include Alkhurma hemorrhagic fever (AHF) virus n = 1, Crimean–Congo hemorrhagic fever (CCHF) virus n = 4, rotavirus n = 2, camel contagious ecthyma n = 2, torque teno virus n = 1, and Dera Ghazi Khan virus n = 1 (Moallin and Zessin 1988; Khan et al. 1997; Al-Moslih et al. 2007; Bazargani et al. 2010; Carletti 2010; Ghosh et al. 2011; Horton et al. 2014; Jere et al. 2014; Champour et al. 2016; Walker et al. 2016).
Bacterial
A total of 35 papers discussed the risk of brucellosis as a public health threat from camels. Most of these 35 papers (18; 51%) were seroprevalence studies of brucellosis in camels, which reported a prevalence range of between 1.4 and 37.5% (Schelling et al. 2004; Omer et al. 2010a, b).
Bacterial diseases that are transmitted through food, water, or other types of fecal–oral transmission were grouped together as “food-borne.” This group included Salmonella, E. coli, Helicobacter, Staphylococcus, Enterococci, Campylobacter, and Leptospirosis. These diarrheal bacteria were reported in 15 papers, four of which discussed testing for antimicrobial resistance in camels and camel products (Rahimi et al. 2010; Tadesse 2015; Tejedor-Junco et al. 2015; Fadlelmula et al. 2016).
Ten papers described camel transmission of plague, Yersinia pestis. In fact, three papers documented plague infection in patients who directly consumed raw camel meat (Christie et al. 1980; Arbaji et al. 2005; Cabanel et al. 2013).
Seven papers detailed high Q fever Coxiella burnetii seropositivity in camels (Schelling et al. 2003; Schelling et al. 2004; Vanderburg et al. 2014; Pirouz et al. 2015; Njeru et al. 2016; Mohabbati Mobarez et al. 2017; Klemmer et al. 2018). Seroprevalence levels of up to 73% were present in camels in Chad (Schelling et al. 2004). Humans that work in close contact with camels such as herders, farmers, and breeders are especially at risk of Q fever transmission, with one study finding a high odds ratio (OR = 9) for the association of being a camel breeder and Q fever seropositivity (Schelling et al. 2003).
The four papers on camel tuberculosis all discussed positive detection of M. bovis, indicating that camels are likely also a reservoir for human transmission (Cosivi et al. 1995; Moda et al. 1996; Gumi et al. 2012; Garine-Wichatitsky et al. 2013). Gumi et al. (2012) found isolated M. tuberculosis from camels and M. bovis from humans, which suggests cross-species transmission of both strains of bacteria.
One of three papers on anthrax conclusively extracted anthrax spores from infected camel meat, which led to illness in ten people (Musa et al. 1993).
Other bacterial diseases in the literature but occurring less frequently included Rickettsia aeschlimannii 1, Klebsiella pneumoniae 1, Aeromonas spp. 1, Bartonella spp. 1, Burkholderia mallei 1, and M. avium subsp. paratuberculosis 1 (Ghenghesh et al. 2001; Ghosh et al. 2012; Kleinerman et al. 2013; Sharma et al. 2013a, b; Rasis et al. 2014; Scholz et al. 2014).
Parasitic
The most common zoonotic parasite transmitted from camels to humans was Echinococcus granulosus n = 46. This parasite has a variety of hosts but is often found in livestock as intermediate hosts, including camels. A review by Alvarez Rojas et al. (2014) estimated that the camel strain of E. granulosus causes between 7 and 11% of all hydatid infections in humans. This attributable risk estimate likely varies by geographic location; a molecular survey by Omar et al. (2010a, b) found that 59% of camels in Sudan were infected with E. granulosus, and a subsequent Sudanese paper found that camels and cattle were the principal intermediate host, not sheep as previously believed (Elmahdi et al. 2004).
There were two papers on the parasite Trypanosoma evansi. Prevalence rates of up to 14% were found in camels in Algeria which is comparatively high to other countries and increases risk for human transmission (Bennoune et al. 2013). Human cases, confirmed with ELISA and stained blood films, of T. evansi have been reported in India and Egypt (Haridy et al. 2011).
Parasitic diseases are commonly passed from camels to humans through meat and milk consumption. One paper on a trichinellosis outbreak in Germany detailed how camel meat brought from Egypt was responsible for zoonotic transmission (Bommer et al. 1980), and in 2013, researchers detected Toxoplasma gondii in camel milk (Dehkordi et al. 2013). Other fecal- and meat-/milk-transmitted parasites included Leishmania spp. n = 1, Babesia bovis n = 1, Cryptosporidium spp. n = 1, and Sarcocystis spp. n = 1 (Ashford 2000; Sazmand et al. 2012; Chhabra and Samantaray 2012; Ereqat et al. 2016). Four other parasite species found in this cohort were helminths Haemonchus tataricus, Trichostrongylus hamatus, and Trichuris infundibulus n = 2; Linguatula serrata n = 7; Onchocerca volvulus n = 1; and Fasciola hepatica or Fasciola gigantica n = 1 (Sadjjadi et al. 1998; McCarthy and Moore 2000; Shakerian et al. 2008; Haddadzadeh et al. 2010; Oryan et al. 2011; Rezaei et al. 2012; Anvari-Tafti et al. 2013; Bamorovat et al. 2014; Youssef and Uga 2014; El-Bahnasawy et al. 2015; Farjanikish and Shokrani 2016).
Discussion
As determined by publication count as well as known mortality rates, viruses in this review are of highest interest, followed by bacteria and parasites (Table 1). Camels are as ubiquitous as cattle or sheep in many parts of the world; yet, knowledge on potential health risks lags behind that of other livestock species. The combination of human-related climate change, population growth, decline in biodiversity, and land-use change are major drivers for the evolution and spread of zoonotic disease (Engering et al. 2013).
The emergence of MERS, with outbreaks between 2012 and 2016, was an outcome of these realities, and it is no surprise that MERS continues to receive high amounts of publicity and funding due to its high human fatality rates ~35% and pandemic potential (World Health Organization 2017). There are currently no widely used vaccines against MERS, but knowledge of its transmission is critical to better implement food safety and sanitation practices within the camel value chain. Rift Valley fever (RVF) was the second most common camel-borne zoonosis in this review and is not a significant source of mortality as less than 3% of patients develop lethal symptoms. However, it is a significant cause of morbidity especially in high-risk populations such as veterinarians, butchers, scientists, animal health workers, farmers, and herders (Ikegami and Makino 2011). The same goes for Camelpox, which is a minor health problem for camel farmers but incurs significant economic damages from the death of young camels, reduced milk yield, and lasting morbidity (Balamurugan et al. 2013). MERS, RVF, and Camelpox were some of the most commonly reported camel-borne zoonotic viruses in this literature review, but for preventive purposes awareness of the following viruses is important to promote. Crimean–Congo hemorrhagic fever is listed as a disease with epidemic potential due to its high mortality rate, growing prevalence in Asia and Europe, and lack of vaccines (Mertens et al. 2013). Alkhurma hemorrhagic fever (AHF) is also a disease of interest because of its hemorrhagic symptoms, recent emergence, and lack of detailed knowledge of its symptoms and transmission. Mortality rates for these viruses along with other hemorrhagic fevers are high because of difficulties in disease diagnosis (World Health Organization 2016). Alkhurma hemorrhagic fever, CCHF, and Dera Ghazi Khan are mosquito- and tick-borne diseases where camels act as reservoirs and amplifiers (Carletti 2010; Walker et al. 2016). Thus, vector surveillance and management around camels in addition to the aforementioned sanitation practices could be highly beneficial to control the spread of these diseases.
The bacterial disease of greatest concern is brucellosis, which is not only zoonotic but also causes severe economic losses for farmers and ranchers across the world in lost milk, reduced fertility, stillbirths, and abortions (Akakpo et al. 2010). Camel farmers should be cautious and aware when handling camels, and this exemplifies another area where increased attention to sanitation practices would be beneficial. Food-borne diseases are of high importance as evidenced by the rapid establishment of complex camel milk value chains in urban Kenya as well as the breadth of food-borne pathogens found in our review (Muloi et al. 2018). These locations exemplify the high-risk transmission interfaces that are formed due to a lack of proper protocol and oversight by government agencies in regard to food safety training and hygienic practices (Muloi et al. 2018). Camels contract plague from infected fleas and may infect humans through contact with infected bodily fluids or consumption of infected meat (Leslie et al. 2011). However, vaccination in humans can be used to control the spread and occurrence of outbreaks. For example, vaccination rates have steadily increased in Kazakhstan since 2001 and the usage of vaccines in combination with antibiotics has greatly reduced case fatality across the country (Aikimbajev et al. 2003). The abundance of publications on brucellosis, plague, and food-borne bacterial illnesses reaffirms their presence in camels.
The earliest papers in this review came from the 1970s and almost exclusively discussed parasites like E. granulosus with occasional papers on viral and bacterial disease. This finding is consistent with a historical lack of widespread high-quality technology for viral and bacterial detection, as well as increased focus on viruses today as compared to 30–40 years ago. Parasitic diseases in this review were not significant sources of mortality. Cysts from E. granulosus occur on lung and liver tissue along with other internal organs and contribute to morbidity in humans through pressure effects and problematic locations of cysts (Mandal and Deb Mandal 2012). Vaccination of camels against E. granulosus is not widely practiced because sheep and dogs are considered to be more important hosts: This, in combination with unsanitary practices and high camel and sheep densities, creates higher risk for humans in these areas (Zhang and McManus 2006). No other publications on parasites showed that they were significant sources of human mortality, and there were low paper counts for most parasites, which could indicate their rarity in camels and largely non-lethal status.
Many studies demonstrated a high seroprevalence to a variety of zoonotic pathogens in camel populations along with current or past examples of camel–human transmission. However, few validated standardized tests exist for camels, making disease detection and confirmation difficult (Gwida et al. 2011). Seropositivity is an indication of antibodies and not antigens, so while this shows that a camel was exposed, it does not provide information on the infection status of the individual or the ability of the camel to transmit a pathogen. These papers may not have exact confirmation for each strain in each country or population, but high prevalence coupled with known instances of transmission provides a guideline for prospective risks. Additionally, because we did not analyze our results with statistical methods we were unable to assess the strength of association between pathogens and human risk. Another limitation of our review was the absence of certain pivotal papers; this may have been due to the use of Google Scholar as one of the two major search engines. A serosurvey of Q fever in Laikipia County, Kenya, that revealed high seroprevalence 18.6% in dromedaries was one such paper that fit our inclusion and search criteria keywords: camel, zoonotic, human, but did not appear in any searches (Browne et al. 2017). A common critique of Google Scholar is the limited ability to sort results, which thus provides evidence that it misses important literature in many case studies (Haddaway et al. 2015). Although we did use PubMed we still may have missed eligible publications because of relevance sorting and/or using only the first 100 results. Our study was limited to peer-reviewed material in English and excludes a thorough review of French, Turkish, Farsi, and Arabic literature which could have provided more information in target regions. The use of additional search engines or search terms may improve the scope of literature reviews, which we will make note of for the future.
Lastly, a limitation not necessary related to methodology but rather the epidemiology of diseases relates to missing diseases at the camel–other livestock/wildlife–human interface that we would not have captured in our review. Although we did not include them as part of this review there were papers found in our initial searches that described camel–livestock and camel–wildlife transmission. These shared pathogens may be zoonotic and include camels as part of the transmission cycle but are not necessarily identified as a camel-borne zoonosis. For example, other animals may be the original or primary source of many pathogens, such as the case of MERS in bats, with the camel being an intermediate host in the transmission from animal to human (Corman et al. 2014a, b).
Dromedary camels are a staple in the diets and lives of humans like their cattle and pig counterparts, but research on their zoonotic disease potential is lacking in comparison. When the map of camel population density is compared to the geographic site of published papers found in this review, we see that the two have high levels of intersection in Africa, Asia, and the Middle East (Figures 1 and 3). However, these maps also show that in many instances camel-borne zoonoses are not restricted to areas of high camel numbers and human infections can and do occur in countries with very low camel populations, and even in countries with no camels as a person may be exposed in one region and travel to another. Therefore, veterinarians, farmers, and others working in close contact with camels and camel products should be cognizant of these potential pathogens, not just in areas where camels are raised but also where camel products may be processed and transported. Additionally, physicians must be aware of where their patients have traveled. Knowledge of potential camel-borne diseases is thus important for researchers and health workers to consider globally.
Conclusion
Camels are not common outside of hot and arid areas such as sub-Saharan Africa or the Middle East, but knowledge of their potential carrier status is important to researchers, zoo personnel, and travelers. The MERS and Ebola outbreaks in recent years have shown how rapidly pathogens can travel and erupt in novel human populations; population expansion and a lack of extensive healthcare systems make camel-endemic areas a potential hot spot for zoonotic spillover. Many of the zoonotic pathogens of camels are a current or possible future risk to human health and must be considered by medical professionals, especially in light of the increased use of camels as a growing protein source globally. As we collect epidemiologic data on the routes of transmission and sources of these infectious agents, we become better prepared to manage and mitigate their impact on humans. Camel milk and meat act as a point source for infection and should be managed with proper slaughter protocols, pasteurization, and improved overall sanitation practices. Dromedary camels also act as a significant source and amplifier for vector-borne disease; therefore, vaccination of camels, control of mosquitoes and ticks, insecticide application, and consistent screening will help control infection rates in camels and humans. In this literature review, we highlight a number of camel-borne zoonotic diseases. The number of pathogens and spillover events will most likely continue to grow as human and camel populations increase and increasingly intersect.
References
Abbas B, Agab H 2002 A review of camel brucellosis. Preventive Veterinary Medicine 55:47–56. https://doi.org/10.1016/s0167-58770200055-7
Abdel Aaty HE, Abdel-Hameed DM, Alam-Eldin YH, El-Shennawy SF, Aminou HA, Makled SS, Darweesh SK 2012 Molecular genotyping of Echinococcus granulosus in animal and human isolates from Egypt. Acta Tropica 121:125–128. https://doi.org/10.1016/j.actatropica.2011.10.014
Abdo-Salem S, Gerbier G, Bonnet P, Al-Qadasi M, Tran A, Thiry E, Al-Eryni G, Roger F 2006 Descriptive and spatial epidemiology of rift valley fever outbreak in Yemen 2000–2001. Annals of the New York Academy of Sciences 1081:240–242. https://doi.org/10.1196/annals.1373.028
Abushhewa MH, Abushhiwa MHS, Nolan MJ, Jex AR, Campbell BE, Jabbar A, Gasser RB 2010 Genetic classification of Echinococcus granulosus cysts from humans, cattle and camels in Libya using mutation scanning-based analysis of mitochondrial loci. Molecular and Cellular Probes 24:346–351. https://doi.org/10.1016/j.mcp.2010.07.005
Adney DR, van Doremalen N, Brown VR, Bushmaker T, Scott D, de Wit E, Bowen RA, Munster VJ 2014 Replication and shedding of MERS-CoV in upper respiratory tract of inoculated dromedary camels. Emerging Infectious Diseases 20:1999–2005. https://doi.org/10.3201/eid2012.141280
Ahmadi NA 2005 Hydatidosis in camels Camelus dromedarius and their potential role in the epidemiology of Echinococcus granulosus in Iran. Journal of Helminthology 79:119–125. https://doi.org/10.1079/joh2005279
Ahmed AE 2017a Diagnostic delays in 537 symptomatic cases of Middle East respiratory syndrome coronavirus infection in Saudi Arabia. International Journal of Infectious Diseases 62:47–51. https://doi.org/10.1016/j.ijid.2017.07.008
Ahmed AE 2017b The predictors of 3- and 30-day mortality in 660 MERS-CoV patients. BMC Infectious Diseases. https://doi.org/10.1186/s12879-017-2712-2
Ahmed Kamal S 2011 Observations on rift valley fever virus and vaccines in Egypt. Virology Journal 8:532. https://doi.org/10.1186/1743-422x-8-532
Ahmed MO, Elmeshri SE, Abuzweda AR, Blauo M, Abouzeed YM, Ibrahim A, Salem H, Alzwam F, Abid S, Elfahem A, Elrais A 2010 Seroprevalence of brucellosis in animals and human populations in the western mountains region in Libya, December 2006–January 2008. Euro Surveill 15:30.
Aikembayev AM, Lukhnova L, Temiraliyeva G, Meka-Mechenko T, Pazylov Y, Zakaryan S, Denissov G, Easterday WR, Van Ert MN, Keim P, Francesconi SC, Blackburn JK, Hugh-Jones M, Hadfield T 2010 Historical Distribution and Molecular Diversity of Bacillus anthracis, Kazakhstan. Emerging Infectious Diseases 16:789–796. https://doi.org/10.3201/eid1605.091427
Aikimbajev A, Meka-Mechenko T, Temiralieva G, Bekenov J, Sagiyev Z, Kaljan K, Mukhambetova AK 2003 Plague in Kazakhstan at the present time. Przegl Epidemiol 57:593–598
Akakpo A, Têko-Agbo A, Koné P 2010 The impact of brucellosis on the economy and public health in Africa. In: Compendium of technical items presented to the OIE World Assembly of Delegates or to OIE Regional Commissions, vol 2009, pp 71–84.
Al Dahouk S, Sprague LD, Neubauer H 2013 New developments in the diagnostic procedures for zoonotic brucellosis in humans. Revue Scientifique Et Technique International Office of Epizootics 32:177–188.
Al Hammadi ZM, Chu DKW, Eltahir YM, Al Hosani F, Al Mulla M, Tarnini W, Hall AJ, Perera RAPM, Abdelkhalek MM, Peiris JSM, Al Muhairi SS, Poon LLM 2015 Asymptomatic MERS-CoV Infection in Humans Possibly Linked to Infected Dromedaries Imported from Oman to United Arab Emirates, May 2015. Emerging Infectious Diseases 21:2197–2200. https://doi.org/10.3201/eid2112.151132
Al-Moslih MI, Perkins H, Hu Y-W 2007 Genetic relationship of Torque Teno virus TTV between humans and camels in United Arab Emirates UAE. Journal of Medical Virology 79:188–191. https://doi.org/10.1002/jmv.20776
Al salihi SF, Alrodhan M 2017 Phylogenetic analysis of MERSCoV in human and camels in Iraq. International Journal of Pharmaceutical Research and Allied Sciences 6: 120–129
Al-Tawfiq J, Memish ZA 2014a Middle East respiratory syndrome coronavirus: epidemiology and disease control measures. Infection and Drug Resistance. https://doi.org/10.2147/idr.s51283
Al-Tawfiq J, Memish ZA 2014b Middle East respiratory syndrome coronavirus: transmission and phylogenetic evolution. Trends in Microbiology 22:573–579. https://doi.org/10.1016/j.tim.2014.08.001
Al-Tawfiq J, Zumla A, Memish ZA 2014 Travel implications of emerging coronaviruses: SARS and MERS-CoV. Travel Medicine and Infectious Disease 12:422–428. https://doi.org/10.1016/j.tmaid.2014.06.007
Alagaili AN, Briese T, Mishra N, Kapoor V, Sameroff SC, de Wit E, Munster VJ, Hensley LE, Zalmout IS, Kapoor A, Epstein JH, Karesh WB, Daszak P, Mohammed OB, Lipkin WI 2014 Middle East respiratory syndrome coronavirus infection in dromedary camels in Saudi Arabia. mBio. https://doi.org/10.1128/mbio.00884-14
Alanazi AD 2013 Determination of seropositivity for toxoplasma gondii in sheep, goats and camels slaughtered for food and human consumptions in Riyadh Municipal Abattoirs, Saudi Arabia. Journal of the Egyptian Society of Parasitology 43:569–576. https://doi.org/10.12816/0006414
Aleanizy FS, Mohmed N, Alqahtani FY, El Hadi Mohamed RA 2017 Outbreak of Middle East respiratory syndrome coronavirus in Saudi Arabia: a retrospective study. BMC Infect Dis. https://doi.org/10.1186/s12879-016-2137-3
Alexandersen S, Kobinger GP, Soule G, Wernery U 2014 Middle East Respiratory Syndrome Coronavirus Antibody Reactors Among Camels in Dubai, United Arab Emirates, in 2005. Transboundary Emerging Disease 61:105–108. https://doi.org/10.1111/tbed.12212
Alhakeem RF, Midgley CM, Assiri AM, Alessa M, Al Hawaj H, Saeed AB, Almasri MM, Lu X, Abedi GR, Abdalla O, Mohammed M, Algarni HS, Al-Abdely HM, Alsharef AA, Nooh R, Erdman DD, Gerber SI, Watson JT 2016 Exposures among MERS case-patients, Saudi Arabia, January–February 2016. Emerging Infectious Diseases 22:2020–2022. https://doi.org/10.3201/eid2211.161042
Alhamlan FS, Majumder MS, Brownstein JS, Hawkins J, Al-Abdely HM, Alzahrani A, Obaid DA, Al-Ahdal MN, BinSaeed A 2017 Case characteristics among Middle East respiratory syndrome coronavirus outbreak and non-outbreak cases in Saudi Arabia from 2012 to 2015. BMJ Open 7:e011865. https://doi.org/10.1136/bmjopen-2016-011865
Ali MA, Shehata MM, Gomaa MR, Kandeil A, El-Shesheny R, Kayed AS, El-Taweel AN, Atea M, Hassan N, Bagato O, Moatasim Y, Mahmoud SH, Kutkat O, Maatouq AM, Osman A, McKenzie PP, Webby RJ, Kayali G 2017 Systematic, active surveillance for Middle East respiratory syndrome coronavirus in camels in Egypt. Emerging Microbes and Infections 6:e1–e1 . https://doi.org/10.1038/emi.2016.130
Alraddadi BM, Watson JT, Almarashi A, Abedi GR, Turkistani A, Sadran M, Housa A, Almazroa MA, Alraihan N, Banjar A, Albalawi E, Alhindi H, Choudhry AJ, Meiman JG, Paczkowski M, Curns A, Mounts A, Feikin DR, Marano N, Swerdlow DL, Gerber SI, Hajjeh R, Madani TA 2016 Risk factors for primary Middle East respiratory syndrome coronavirus Illness in Humans, Saudi Arabia, 2014. Emerging Infectious Diseases 22:49–55. https://doi.org/10.3201/eid2201.151340
Alsolamy S, Yousif S, Alotabi B, Aljerian N, Alrajhi K, Al Somali S, Alsaawi A 2017 Middle East respiratory syndrome: global outbreak data analysis. Journal of Ancient Diseases and Preventive Remedies. https://doi.org/10.4172/2329-8731.1000159
Alvarez Rojas CA, Romig T, Lightowlers MW 2014 Echinococcus granulosus sensu lato genotypes infecting humans—review of current knowledge. International Journal for Parasitology 44:9–18. https://doi.org/10.1016/j.ijpara.2013.08.008
Anvari-Tafti M, Sazmand A, Hekmatimoghaddam S, Moobedi I 2013 Gastrointestinal helminths of camels Camelus dromedarius in center of Iran. Trop Biomed 30:56–61
Arbaji A, Kharabsheh S, Al-Azab S, Al-Kayed M, Amr ZS, Abu Baker M, Chu MC 2005 A 12-case outbreak of pharyngeal plague following the consumption of camel meat, in north–eastern Jordan. Annals of Tropical Medicine and Parasitology 99:789–793. https://doi.org/10.1179/136485905x65161
Ashford R. 2000 The leishmaniases as emerging and reemerging zoonoses. International Journal for Parasitology 30:1269–1281. https://doi.org/10.1016/s0020-75190000136-3
Assiri AM, Midgley CM, Abedi GR, Bin Saeed A, Almasri MM, Lu X, Al-Abdely HM, Abdalla O, Mohammed M, Algarni HS, Alhakeem RF, Sakthivel SK, Nooh R, Alshayab Z, Alessa M, Srinivasamoorthy G, AlQahtani SY, Kheyami A, HajOmar WH, Banaser TM, Esmaeel A, Hall AJ, Curns AT, Tamin A, Alsharef AA, Erdman D, Watson JT, Gerber SI 2016 Epidemiology of a Novel Recombinant Middle East Respiratory Syndrome Coronavirus in Humans in Saudi Arabia. Journal of Infectious Diseases 214:712–721. https://doi.org/10.1093/infdis/jiw236
Azab ME, Bishara SA, Helmy H, Oteifa NM, El-Hoseiny LM, Ramzy RMR, Ahmed MA 2004 Molecular characterization of Egyptian human and animal Echinococcus granulosus isolates by RAPD-PCR technique. J Egypt Soc Parasitol 34:83–96
Azhar EI, El-Kafrawy SA, Farraj SA, Hassan AM, Al-Saeed MS, Hashem AM, Madani TA 2014 Evidence for Camel-to-Human Transmission of MERS Coronavirus. New England Journal of Medicine 370:2499–2505. https://doi.org/10.1056/nejmoa1401505
Azhar EI, Hashem AM, El-Kafrawy SA, Sohrab SS, Aburizaiza AS, Farraj SA, Hassan AM, Al-Saeed MS, Jamjoom GA, Madani TA 2014 Detection of the Middle East respiratory syndrome coronavirus genome in an air sample originating from a camel barn owned by an infected patient. mBio. https://doi.org/10.1128/mbio.01450-14
Babelhadj B, Di Bari MA, Pirisinu L, Chiappini B, Gaouar SBS, Riccardi G, Marcon S, Agrimi U, Nonno R, Vaccari G 2018 Prion Disease in Dromedary Camels, Algeria. Emerging Infectious Diseases 24:1029–1036. https://doi.org/10.3201/eid2406.172007
Balamurugan V, Venkatesan G, Bhanuprakash V, Singh RK 2013 Camelpox, an emerging orthopox viral disease. Indian Journal of Virology 24:295–305. https://doi.org/10.1007/s13337-013-0145-0
Balkhy HH, Alenazi TH, Alshamrani MM, Baffoe-Bonnie H, Al-Abdely HM, El-Saed A, Al Arbash HA, Al Mayahi ZK, Assiri AM, Bin Saeed A 2016 Notes from the field: nosocomial outbreak of Middle East respiratory syndrome in a large tertiary care hospital — Riyadh, Saudi Arabia, 2015. MMWR Morbidity and Mortality Weekly Report 65:163–164. https://doi.org/10.15585/mmwr.mm6506a5
Bamorovat M, Zarandi MB, Mostafavi M, Kheirandish R, Sharifi I, Radfar MH 2014 The prevalence of Linguatula serrata nymphs in mesenteric and mediastinal lymph nodes in one-humped camels Camelus dromedarius slaughtered in Rafsanjan slaughterhouse, Iran. Journal of Parasitic Diseases 38:374–377. https://doi.org/10.1007/s12639-013-0258-9
Banik GR, Khandaker G, Rashid H 2015 Middle East respiratory syndrome coronavirus “MERS-CoV”: current knowledge gaps. Paediatric Respiratory Reviews 16:197–202. https://doi.org/10.1016/j.prrv.2015.04.002
Bardonnet K, Benchikh-Elfegoun M., Bart J., Harraga S, Hannache N, Haddad S, Dumon H, Vuitton D., Piarroux R 2003 Cystic echinococcosis in Algeria: cattle act as reservoirs of a sheep strain and may contribute to human contamination. Veterinary Parasitology 116:35–44. https://doi.org/10.1016/s0304-40170300255-3
Bardonnet K, Piarroux R, Dia L, Schneegans F, Beurdeley A, Godot V, Vuitton DA 2002 Combined eco-epidemiological and molecular biology approaches to assess Echinococcus granulosus transmission to humans in Mauritania: occurrence of the ‘camel’ strain and human cystic echinococcosis. Transactions of the Royal Society of Tropical Medicine and Hygiene 96:383–386. https://doi.org/10.1016/s0035-92030290369-x
Bazargani TT, Nikjou D, Tafty A, Varshovi HR, Niasari-Naslaji A 2010 A regional outbreak of contagious camel echtyma in Iran. Journal of Camel Practice and Research 17:221–224
Bekele W, Tessema T, Melaku S 2013 Camelus dromedarius brucellosis and its public health associated risks in the Afar National Regional State in northeastern Ethiopia. Acta Veterinaria Scandinavica 55:89. https://doi.org/10.1186/1751-0147-55-89
Bennoune O, Adili N, Amri K, Bennecib L, Ayachi A 2013 Trypanosomiasis of camels Camelus dromedarius in Algeria: first report. Vet Res Forum 4:273–275
Bera BC, Barua S, Shanmugasundaram K, Anand T, Riyesh T, Vaid RK, Virmani N, Kundu S, Yadav NK, Malik P, Singh RK 2015 Genetic characterization and phylogenetic analysis of host-range genes of Camelpox virus isolates from India. VirusDisease 26:151–162. https://doi.org/10.1007/s13337-015-0266-8
Bera BC, Shanmugasundaram K, Barua S, Gupta A, Riyesh T, … Singh RK 2010 IBT/033 Sequence analysis of Schlafen gene of Camelpox virus CMLV isolated from recent outbreak 2009 in Rajasthan. Journal of Immunology and Immunopathology 12:2
Bera BC, Shanmugasundaram K, Barua S, Venkatesan G, Virmani N, Riyesh T, Gulati BR, Bhanuprakash V, Vaid RK, Kakker NK, Malik P, Bansal M, Gadvi S, Singh RV, Yadav V, Sardarilal, Nagarajan G, Balamurugan V, Hosamani M, Pathak KML, Singh RK 2011 Zoonotic cases of camelpox infection in India. Veterinary Microbiology 152:29–38. https://doi.org/10.1016/j.vetmic.2011.04.010
Bird BH, Githinji JWK, Macharia JM, Kasiiti JL, Muriithi RM, Gacheru SG, Musaa JO, Towner JS, Reeder SA, Oliver JB, Stevens TL, Erickson BR, Morgan LT, Khristova ML, Hartman AL, Comer JA, Rollin PE, Ksiazek TG, Nichol ST 2008 Multiple virus lineages sharing recent common ancestry were associated with a large rift valley fever outbreak among Livestock in Kenya during 2006-2007. Journal of Virology 82:11152–11166. https://doi.org/10.1128/jvi.01519-08
Bloch N, Diallo I 1995 A probable outbreak of rabies in a group of camels in Niger. Veterinary Microbiology 46:281–283. https://doi.org/10.1016/0378-11359500092-o
Bommer W, Kaiser H, Mergerian H, Pottkämper G 1980 Outbreak of trichinelliasis in a youth centre in Neidersachsen by air-dried imported camel meat. In: Proceedings of the 1st world congress on foodborne infections and intoxications, 29 June–3 July 1980, West Berlin, Germany, vol 1, pp 441–444
Bramanti B, Stenseth NC, Walløe L, Lei X 2016 Plague: a disease which changed the path of human civilization. In: Yersinia pestis: retrospective and perspective. Springer Netherlands, Dordrecht, pp 1–26
Britch SC, Binepal YS, Ruder MG, Kariithi HM, Linthicum KJ, Anyamba A, Small JL, Tucker CJ, Ateya LO, Oriko AA, Gacheru S, Wilson WC 2013 Rift Valley Fever Risk Map Model and Seroprevalence in Selected Wild Ungulates and Camels from Kenya. PLoS ONE 8:e66626. https://doi.org/10.1371/journal.pone.0066626
Browne AS, Fèvre EM, Kinnaird M, Muloi DM, Wang CA, Larsen PS, O’Brien T, Deem SL 2017 Serosurvey of Coxiella burnetii Q fever in Dromedary Camels Camelus dromedarius in Laikipia County, Kenya. Zoonoses and Public Health 64:543–549. https://doi.org/10.1111/zph.12337
Buchholz U, Müller MA, Nitsche A, Sanewski A, Wevering N, Bauer-Balci T, Bonin F, Drosten C, Schweiger B, Wolff T, Muth D, Meyer B, Buda S, Krause G, Schaade L, Haas W 2013 Contact investigation of a case of human novel coronavirus infection treated in a German hospital, October–November 2012. Euro Surveillance 18
Cabanel N, Leclercq A, Chenal-Francisque V, Annajar B, Rajerison M, Bekkhoucha S, Bertherat E, Carniel E 2013 Plague Outbreak in Libya, 2009, Unrelated to Plague in Algeria. Emerging Infectious Diseases 19:230–236. https://doi.org/10.3201/eid1902.121031
Carletti F 2010 Alkhurma hemorrhagic fever in travelers returning from Egypt, 2010. Emerging Infectious Diseases. https://doi.org/10.3201/eid1612101092
Casulli A, Zeyhle E, Brunetti E, Pozio E, Meroni V, Genco F, Filice C 2010 Molecular evidence of the camel strain G6 genotype of Echinococcus granulosus in humans from Turkana, Kenya. Transactions of the Royal Society of Tropical Medicine and Hygiene 104:29–32. https://doi.org/10.1016/j.trstmh.2009.08.001
Champour M, Chinikar S, Mohammadi G, Razmi G, Shah-Hosseini N, Khakifirouz S, Mostafavi E, Jalali T 2016 Molecular epidemiology of Crimean–Congo hemorrhagic fever virus detected from ticks of one humped camels Camelus dromedarius population in northeastern Iran. Journal of Parasitic Diseases 40:110–115. https://doi.org/10.1007/s12639-014-0458-y
Chan RWY, Hemida MG, Kayali G, Chu DKW, Poon LLM, Alnaeem A, Ali MA, Tao KP, Ng HY, Chan MCW, Guan Y, Nicholls JM, Peiris JSM 2014 Tropism and replication of Middle East respiratory syndrome coronavirus from dromedary camels in the human respiratory tract: an in-vitro and ex-vivo study. The Lancet Respiratory Medicine 2:813–822. https://doi.org/10.1016/s2213-26001470158-4
Chan JFW, Lau SKP, To KKW, Cheng VCC, Woo PCY, Yuen K-Y 2015 Middle East Respiratory syndrome coronavirus: another zoonotic betacoronavirus causing SARS-Like Disease. Clinical Microbiology Reviews 28:465–522. https://doi.org/10.1128/cmr.00102-14
Chevalier V, Pépin M, Plée L, Lancelot R 2010 Rift Valley fever–a threat for Europe? Euro Surveill 15:19506
Chhabra MB, Samantaray S 2012 Sarcocystis and sarcocystosis in India: status and emerging perspectives. Journal of Parasitic Diseases. https://doi.org/10.1007/s12639-012-0135-y
Chinikar S, Shah-Hosseini N, Mostafavi E, Moradi M, Khakifirouz S, Jalali T, Fooks AR 2013 Surveillance of Rift Valley fever in Iran between 2001 and 2011. The All Results Journals: Biol 4:16–18
Christie AB, Chen TH, Elberg SS 1980 Plague in Camels and Goats: Their Role in Human Epidemics. Journal of Infectious Diseases 141:724–726. https://doi.org/10.1093/infdis/141.6.724
Chu DKW, Hui KPY, Perera RAPM, Miguel E, Niemeyer D, Zhao J, Channappanavar R, Dudas G, Oladipo JO, Traoré A, Fassi-Fihri O, Ali A, Demissié GF, Muth D, Chan MCW, Nicholls JM, Meyerholz DK, Kuranga SA, Mamo G, Zhou Z, So RTY, Hemida MG, Webby RJ, Roger F, Rambaut A, Poon LLM, Perlman S, Drosten C, Chevalier V, Peiris M 2018 MERS coronaviruses from camels in Africa exhibit region-dependent genetic diversity. Proceedings of the National Academy of Sciences 115:3144–3149. https://doi.org/10.1073/pnas.1718769115
Chu DK, Oladipo JO, Perera RA, Kuranga SA, Chan SM, Poon LL, Peiris M 2015 Middle East respiratory syndrome coronavirus MERS-CoV in dromedary camels in Nigeria, 2015. Eurosurveillance. https://doi.org/10.2807/1560-7917.es.2015.20.49.30086
Chu DKW, Poon LLM, Gomaa MM, Shehata MM, Perera RAPM, Abu Zeid D, El Rifay AS, Siu LY, Guan Y, Webby RJ, Ali MA, Peiris M, Kayali G 2014 MERS Coronaviruses in Dromedary Camels, Egypt. Emerging Infectious Diseases 20:1049–1053. https://doi.org/10.3201/eid2006.140299
Cooper CW 1992 Risk factors in transmission of brucellosis from animals to humans in Saudi Arabia. Transactions of the Royal Society of Tropical Medicine and Hygiene 86:206–209. https://doi.org/10.1016/0035-92039290575-w
Corman VM, Eckerle I, Memish ZA, Liljander AM, Dijkman R, Jonsdottir H, Juma Ngeiywa KJZ, Kamau E, Younan M, Al Masri M, Assiri A, Gluecks I, Musa BE, Meyer B, Müller MA, Hilali M, Bornstein S, Wernery U, Thiel V, Jores J, Drexler JF, Drosten C 2016 Link of a ubiquitous human coronavirus to dromedary camels. Proceedings of the National Academy of Sciences 113:9864–9869. https://doi.org/10.1073/pnas.1604472113
Corman VM, Ithete NL, Richards LR, Schoeman MC, Preiser W, Drosten C, Drexler JF (2014a) Rooting the phylogenetic tree of Middle East respiratory syndrome coronavirus by characterization of a conspecific virus from an African Bat. J Virol 88:11297–11303. https://doi.org/10.1128/jvi.01498-14
Corman VM, Jores J, Meyer B, Younan M, Liljander A, Said MY, Gluecks I, Lattwein E, Bosch B-J, Drexler JF, Bornstein S, Drosten C, Müller MA (2014b) Antibodies against MERS coronavirus in dromedary camels, Kenya, 1992–2013. Emerg Infect Dis. https://doi.org/10.3201/eid2008.140596
Corman VM, Muth D, Niemeyer D, Drosten C (2018) Hosts and sources of endemic human coronaviruses. In: Advances in virus research, Kielian M, Mettenleiter TC, Roossinck MJ (editors), Academic Press, pp 163–188
Cosivi O, Meslin FX, Daborn CJ, Grange JM 1995 Epidemiology of Mycobacterium bovis infection in animals and humans, with particular reference to Africa. Revue Scientifique et Technique de l’OIE 14:733–746. https://doi.org/10.20506/rst.14.3.875
Cotten M, Watson SJ, Kellam P, Al-Rabeeah AA, Makhdoom HQ, Assiri A, Al-Tawfiq JA, Alhakeem RF, Madani H, AlRabiah FA, Hajjar SA, Al-nassir WN, Albarrak A, Flemban H, Balkhy HH, Alsubaie S, Palser AL, Gall A, Bashford-Rogers R, Rambaut A, Zumla AI, Memish ZA 2013 Transmission and evolution of the Middle East respiratory syndrome coronavirus in Saudi Arabia: a descriptive genomic study. The Lancet 382:1993–2002. https://doi.org/10.1016/s0140-67361361887-5
Cotten M, Watson SJ, Zumla AI, Makhdoom HQ, Palser AL, Ong SH, Al Rabeeah AA, Alhakeem RF, Assiri A, Al-Tawfiq JA, Albarrak A, Barry M, Shibl A, Alrabiah FA, Hajjar S, Balkhy HH, Flemban H, Rambaut A, Kellam P, Memish ZA 2014 Spread, Circulation, and Evolution of the Middle East Respiratory Syndrome Coronavirus. mBio 5: e01062-13. https://doi.org/10.1128/mbio.01062-13
Crameri G, Durr PA, Barr J, Yu M, Graham K, Williams OJ, Kayali G, Smith D, Peiris M, Mackenzie JS, Wang L-F 2015 Absence of MERS-CoV antibodies in feral camels in Australia: Implications for the pathogen’s origin and spread. One Health 1:76–82. https://doi.org/10.1016/j.onehlt.2015.10.003
Deem SL, Fèvre EM, Kinnaird M, Browne AS, Muloi D, Godeke G-J, Koopmans M, Reusken CB 2015 Serological Evidence of MERS-CoV Antibodies in Dromedary Camels Camelus dromedaries in Laikipia County, Kenya. PLOS ONE 10:e0140125. https://doi.org/10.1371/journal.pone.0140125
Dehkordi FS, Haghighi Borujeni MR, Rahimi E, Abdizadeh R 2013 Detection of Toxoplasma gondii in Raw Caprine, Ovine, Buffalo, Bovine, and Camel Milk Using Cell Cultivation, Cat Bioassay, Capture ELISA, and PCR Methods in Iran. Foodborne Pathogens and Disease 10:120–125. https://doi.org/10.1089/fpd.2012.1311
Devi JP, Noraini W, Norhayati R, Chee Kheong C, Badrul AS, Zainah S, Fadzilah K, Hirman I, Lokman Hakim S, Noor Hisham A 2014 Laboratory-confirmed case of Middle East respiratory syndrome coronavirus MERS-CoV infection in Malaysia: preparedness and response, April 2014. Eurosurveillance 19: 20797. https://doi.org/10.2807/1560-7917.es2014.19.18.20797
Dinkel A, Njoroge EM, Zimmermann A, Wälz M, Zeyhle E, Elmahdi IE, Mackenstedt U, Romig T 2004 A PCR system for detection of species and genotypes of the Echinococcus granulosus-complex, with reference to the epidemiological situation in eastern Africa. International Journal for Parasitology 34:645–653. https://doi.org/10.1016/j.ijpara.2003.12.013
Drancourt M, Houhamdi L, Raoult D 2006 Yersinia pestis as a telluric, human ectoparasite-borne organism. The Lancet Infectious Diseases 6:234–241. https://doi.org/10.1016/s1473-30990670438-8
Drosten C, Muth D, Corman VM, Hussain R, Al Masri M, HajOmar W, Landt O, Assiri A, Eckerle I, Al Shangiti A, Al-Tawfiq JA, Albarrak A, Zumla A, Rambaut A, Memish ZA 2015 An Observational, Laboratory-Based Study of Outbreaks of Middle East Respiratory Syndrome Coronavirus in Jeddah and Riyadh, Kingdom of Saudi Arabia, 2014. Clinical Infectious Diseases 60:369–377. https://doi.org/10.1093/cid/ciu812
Du L, Han G-Z 2016 Deciphering MERS-CoV Evolution in Dromedary Camels. Trends in Microbiology 24:87–89. https://doi.org/10.1016/j.tim.2015.12.013
Ducrotoy MJ, Ammary K, Ait Lbacha H, Zouagui Z, Mick V, Prevost L, Bryssinckx W, Welburn SC, Benkirane A 2015 Narrative overview of animal and human brucellosis in Morocco: intensification of livestock production as a driver for emergence? Infectious Diseases of Poverty 4:57. https://doi.org/10.1186/s40249-015-0086-5
Dudas G, Carvalho LM, Rambaut A, Bedford T 2018 MERS-CoV spillover at the camel-human interface. eLife 7. https://doi.org/10.7554/elife.31257
Duraffour S, Meyer H, Andrei G, Snoeck R 2011 Camelpox virus. Antiviral Research 92:167–186. https://doi.org/10.1016/j.antiviral.2011.09.003
Durai P, Batool M, Shah M, Choi S 2015 Middle East respiratory syndrome coronavirus: transmission, virology and therapeutic targeting to aid in outbreak control. Experimental & Molecular Medicine 47:e181. https://doi.org/10.1038/emm.2015.76
Eckerle I, Corman VM, Müller MA, Lenk M, Ulrich RG, Drosten C 2014 Replicative Capacity of MERS Coronavirus in Livestock Cell Lines. Emerging Infectious Diseases 20:276-279. https://doi.org/10.3201/eid2002.131182
Eckert J, Deplazes P 2004 Biological, Epidemiological, and Clinical Aspects of Echinococcosis, a Zoonosis of Increasing Concern. Clinical Microbiology Reviews 17:107–135. https://doi.org/10.1128/cmr.17.1.107-135.2004
Eckert J, Thompson RCA, Michael SA, Kumaratilake LM, El-Sawah HM 1989 Echinococcus granulosus of camel origin: development in dogs and parasite morphology. Parasitology Research 75:536–544. https://doi.org/10.1007/bf00931162
El-Ansary EH, Mohammed BA, Hamad AR, Karom AG 2001 Brucellosis among animals and human contacts in eastern Sudan. Saudi Med J 22:577–579
El-Bahnasawy MM, Gabr MSA, Abdel-Fattah MA, Gaber WAI, Morsy TA 2012 Is plague a problem in the Egyptians returning back from Libya? J Egypt Society of Parasitology 42:329–348
El-Bahnasawy MMM, Morsy ATA, Morsy TA 2015 The arthropod-borne onchocerciasis: is it deserved to be neglected? J Egypt Soc Parasitol 45:639–654
El Bushra HE, Abdalla MN, Al Arbash H, Alshayeb Z, Al-Ali S, Latif ZA-A, Al-Bahkit H, Abdalla O, Mohammed M, Al-Abdely H, Chahed M, Lohiniva AL, Saeed AB 2016 An outbreak of Middle East Respiratory Syndrome MERS due to coronavirus in Al-Ahssa Region, Saudi Arabia, 2015. Eastern Mediterranean Health Journal 22:468–475
El Mamy ABO, Baba MO, Barry Y, Isselmou K, Dia ML, Hampate B, Diallo MY, El Kory MOB, Diop M, Lo MM, Thiongane Y, Bengoumi M, Puech L, Plee L, Claes F, de La Rocque S, Doumbia B 2011 Unexpected Rift Valley Fever Outbreak, Northern Mauritania. Emerging Infectious Diseases 17:1894–1896. https://doi.org/10.3201/eid1710.110397
El Mamy AB, Lo MM, Thiongane Y, Diop M, Isselmou K, Doumbia B, Baba MO, El Arbi AS, Lancelot R, Kane Y, Albina E, Cêtre-Sossah C 2014 Comprehensive Phylogenetic Reconstructions of Rift Valley Fever Virus: The 2010 Northern Mauritania Outbreak in the Camelus dromedarius Species. Vector-Borne and Zoonotic Diseases 14:856–861. https://doi.org/10.1089/vbz.2014.1605
Elmahdi IE, Ali QM, Magzoub MMA, Ibrahim AM, Saad MB, Romig T 2004 Cystic echinococcosis of livestock and humans in central Sudan. Annals of Tropical Medicine & Parasitology 98:473–479. https://doi.org/10.1179/000349804225003578
Engering A, Hogerwerf L, Slingenbergh J 2013 Pathogen–host–environment interplay and disease emergence. Emerging Microbes and Infections 2:e5. https://doi.org/10.1038/emi.2013.5
Ereqat S, Nasereddin A, Vayssier-Taussat M, Abdelkader A, Al-Jawabreh A, Zaid T, Azmi K, Abdeen Z 2016 Molecular Evidence of Bartonella Species in Ixodid Ticks and Domestic Animals in Palestine. Frontiers in Microbiology. https://doi.org/10.3389/fmicb.2016.01217
Fadlelmula A, Al-Hamam NA, Al-Dughaym AM 2016 A potential camel reservoir for extended-spectrum β-lactamase-producing Escherichia coli causing human infection in Saudi Arabia. Tropical Animal Health and Production 48:427–433. https://doi.org/10.1007/s11250-015-0970-9
Fanoy EB, van der Sande MA, Kraaij-Dirkzwager M, Dirksen K, Jonges M, van der Hoek W, Koopmans MP, van der Werf D, Sonder G, van der Weijden C, van der Heuvel J, Gelinck L, Bouwhuis JW, van Gageldonk-Lafeber AB, on behalf of the members of the MERS-CoV outbreak investigation team of The Netherlands 2014 Travel-related MERS-CoV cases: an assessment of exposures and risk factors in a group of Dutch travellers returning from the Kingdom of Saudi Arabia, May 2014. Emerging Themes in Epidemiology 11:16. https://doi.org/10.1186/1742-7622-11-16
Farag EABA, Reusken CBEM, Haagmans BL, Mohran KA, Raj VS, Pas SD, Voermans J, Smits SL, Godeke G-J, Al-Hajri MM, Alhajri FH, Al-Romaihi HE, Ghobashy H, El-Maghraby MM, El-Sayed AM, Al Thani MHJ, Al-Marri S, Koopmans MPG 2015 High proportion of MERS-CoV shedding dromedaries at slaughterhouse with a potential epidemiological link to human cases, Qatar 2014. Infection Ecology & Epidemiology 5:28305. https://doi.org/10.3402/iee.v5.28305
Farjanikish G, Shokrani H 2016 Prevalence and morphopathological characteristics of linguatulosis in one-humped camel Camelus dromedarius in Yazd, Iran. Parasitology Research 115:3163–3167. https://doi.org/10.1007/s00436-016-5074-6
Faye O, Ba H, Ba Y, Freire CCM, Faye O, Ndiaye O, Elgady IO, Zanotto PMA, Diallo M, Sall AA 2014 Reemergence of rift valley fever, Mauritania, 2010. Emerging Infectious Diseases 20:300–303. https://doi.org/10.3201/eid2002.130996
Fehr AR, Channappanavar R, Perlman S 2017 Middle East respiratory syndrome: emergence of a pathogenic human coronavirus. Annual Review of Medicine 68:387–399. https://doi.org/10.1146/annurev-med-051215-031152
Ferguson NM, Van Kerkhove MD 2014 Identification of MERS-CoV in dromedary camels. The Lancet Infectious Diseases 14:93–94. https://doi.org/10.1016/s1473-30991370691-1
Fiori PL, Mastrandrea S, Rappelli P, Cappuccinelli P 2000 Brucella abortus infection acquired in microbiology laboratories. Journal of Clinical Microbiology 38: 2005–2006.
Food and Agriculture Organization of the United Nations FAO (2017) Human exposure to Middle East respiratory syndrome coronavirus from livestock or wildlife species August 2017. FAO Animal Health Risk Analysis—Assessment, Issue No. 4. Rome, FAO
FAOSTAT (2016) Food and agriculture organization corporate statistical database. http://www.fao.org/faostat/en/#data. Accessed 12 Apr 2018
Funk AL, Goutard FL, Miguel E, Bourgarel M, Chevalier V, Faye B, Peiris JSM, Van Kerkhove MD, Roger FL 2016 MERS-CoV at the animal–human interface: inputs on exposure pathways from an expert-opinion elicitation. Frontiers in Veterinary Science 3. https://doi.org/10.3389/fvets.2016.00088
Garcell HG, Garcia EG, Pueyo PV, Martín IR, Arias AV, Alfonso Serrano RN 2016 Outbreaks of brucellosis related to the consumption of unpasteurized camel milk. Journal of Infection and Public Health 9:523–527. https://doi.org/10.1016/j.jiph.2015.12.006
Gardner LM, MacIntyre C 2014 Unanswered questions about the Middle East respiratory syndrome coronavirus MERS-CoV. BMC Research Notes 7:358. https://doi.org/10.1186/1756-0500-7-358
Garine-Wichatitsky MD, Caron A, Kock R, Tschopp R, Munyeme M, Hofmeyr M, Michel A 2013 A review of bovine tuberculosis at the wildlife–livestock–human interface in sub-Saharan Africa. Epidemiology and Infection 141:1342–1356. https://doi.org/10.1017/s0950268813000708
Gautret P, Benkouiten S, Gaillard C, Parola P, Brouqui P 2013 Camel milk-associated infection risk perception and knowledge in French Hajj Pilgrims. Vector-Borne and Zoonotic Diseases 13:425–427. https://doi.org/10.1089/vbz.2012.1010
Gerdes GH 2004 Rift valley fever. Revue scientifique et technique- International Office of Epizootics. 23:613-24.
Ghenghesh KS, El-Ghodban A, Dkakni R, Abeid S, Altomi A, Abdussalam T, Marialigeti K 2001 Prevalence, species differentiation, haemolytic activity, and antibiotic susceptibility of aeromonads in untreated well water. Memórias do Instituto Oswaldo Cruz 96:169–173. https://doi.org/10.1590/s0074-02762001000200006
Ghoneim NH, Abdel-Moein KA, Zaher H 2017 Camel as a transboundary vector for emerging exotic Salmonella serovars. Pathogens and Global Health 111:143–147. https://doi.org/10.1080/20477724.2017.1309343
Ghosh S, Gatheru Z, Nyangao J, Adachi N, Urushibara N, Kobayashi N 2011 Full genomic analysis of a G8P[1] rotavirus strain isolated from an asymptomatic infant in Kenya provides evidence for an artiodactyl-to-human interspecies transmission event. Journal of Medical Virology 83:367–376. https://doi.org/10.1002/jmv.21974
Ghosh P, Hsu C, Alyamani EJ, Shehata MM, Al-Dubaib MA, Al-Naeem A, Hashad M, Mahmoud OM, Alharbi KBJ, Al-Busadah K, Al-Swailem AM, Talaat AM 2012 Genome-Wide Analysis of the Emerging Infection with Mycobacterium avium Subspecies paratuberculosis in the Arabian Camels Camelus dromedarius. PLoS ONE 7:e31947. https://doi.org/10.1371/journal.pone.0031947
Godfroid J, Cloeckaert A, Liautard J-P, Kohler S, Fretin D, Walravens K, Garin-Bastuji B, Letesson J-J 2005 From the discovery of the Malta fever?s agent to the discovery of a marine mammal reservoir, brucellosis has continuously been a re-emerging zoonosis. Veterinary Research 36:313–326. https://doi.org/10.1051/vetres:2005003
Godfroid J, Al Dahouk S, Pappas G, Roth F, Matope G, Muma J, Marcotty T, Pfeiffer D, Skjerve E 2013 A “One Health” surveillance and control of brucellosis in developing countries: Moving away from improvisation. Comparative Immunology, Microbiology and Infectious Diseases 36:241–248. https://doi.org/10.1016/j.cimid.2012.09.001
Gossner C, Danielson N, Gervelmeyer A, Berthe F, Faye B, Kaasik Aaslav K, Adlhoch C, Zeller H, Penttinen P, Coulombier D 2016 Human-Dromedary Camel Interactions and the Risk of Acquiring Zoonotic Middle East Respiratory Syndrome Coronavirus Infection. Zoonoses and Public Health 63:1–9. https://doi.org/10.1111/zph.12171
Gumaa MM, Osman HM, Omer MM, El Sanousi EM, Godfroid J, Ahmed AM 2014 Seroprevalence of brucellosis in sheep and isolation of Brucella abortus biovar 6 in Kassala State, Eastern Sudan. Revue Scientifique Et Technique International Office of Epizootics 33:957-965.
Gumi B, Schelling E, Berg S, Firdessa R, Erenso G, Mekonnen W, Hailu E, Melese E, Hussein J, Aseffa A, Zinsstag J 2012 Zoonotic Transmission of Tuberculosis Between Pastoralists and Their Livestock in South-East Ethiopia. EcoHealth 9:139–149. https://doi.org/10.1007/s10393-012-0754-x
Gutiérrez C, Tejedor-Junco MT, González M, Lattwein E, Renneker S 2015 Presence of antibodies but no evidence for circulation of MERS-CoV in dromedaries on the Canary Islands, 2015. Eurosurveillance 20. https://doi.org/10.2807/1560-7917.es.2015.20.37.30019
Gwida M, Al Dahouk S, Melzer F, Rösler U, Neubauer H, Tomaso H 2010 Brucellosis – Regionally Emerging Zoonotic Disease? Croatian Medical Journal 51:289–295. https://doi.org/10.3325/cmj.2010.51.289
Gwida M, El-Gohary A, Melzer F, Khan I, Rösler U, Neubauer H 2012 Brucellosis in camels. Research in Veterinary Science 92:351–355. https://doi.org/10.1016/j.rvsc.2011.05.002
Gwida MM, El-Gohary AH, Melzer F, Tomaso H, Rosler U, Wernery U, Wernery R, Elschner MC, Khan I, Eickhoff M, Schoner D, Neubauer H 2011 Comparison of diagnostic tests for the detection of Brucella spp. in camel sera. BMC Research Notes 4:525. https://doi.org/10.1186/1756-0500-4-525
Haagmans BL, Al Dhahiry SHS, Reusken CBEM, Raj VS, Galiano M, Myers R, Godeke G-J, Jonges M, Farag E, Diab A, Ghobashy H, Alhajri F, Al-Thani M, Al-Marri SA, Al Romaihi HE, Al Khal A, Bermingham A, Osterhaus ADME, AlHajri MM, Koopmans MPG 2014 Middle East respiratory syndrome coronavirus in dromedary camels: an outbreak investigation. The Lancet Infectious Diseases 14:140–145. https://doi.org/10.1016/s1473-30991370690-x
Haagmans BL, van den Brand JMA, Raj VS, Volz A, Wohlsein P, Smits SL, Schipper D, Bestebroer TM, Okba N, Fux R, Bensaid A, Solanes Foz D, Kuiken T, Baumgartner W, Segales J, Sutter G, Osterhaus ADME 2016 An orthopoxvirus-based vaccine reduces virus excretion after MERS-CoV infection in dromedary camels. Science 351:77–81. https://doi.org/10.1126/science.aad1283
Haddadzadeh HR, Athari SS, Abedini R, Khazraii nia S, Khazraii nia P, Nabian S, Haji-Mohamadi B 2010 One-humped camel Camelus dromedarius infestation with Linguatula serrata in Tabriz, Iran. Iranian Journal of Arthropod-Borne Diseases 4:54–59.
Haddaway NR, Collins AM, Coughlin D, Kirk S 2015 The Role of Google Scholar in Evidence Reviews and Its Applicability to Grey Literature Searching. PLOS ONE 10:e0138237. https://doi.org/10.1371/journal.pone.0138237
Hailemariam Z, Nakao M, Menkir S, Lavikainen A, Yanagida T, Okamoto M, Ito A 2012 Molecular identification of unilocular hydatid cysts from domestic ungulates in Ethiopia: Implications for human infections. Parasitology International 61:375–377. https://doi.org/10.1016/j.parint.2012.01.007
Hajialilo E, Harandi MF, Sharbatkhori M, Mirhendi H, Rostami S 2012 Genetic characterization of Echinococcus granulosus in camels, cattle and sheep from the south-east of Iran indicates the presence of the G3 genotype. Journal of Helminthology 86:263–270. https://doi.org/10.1017/s0022149x11000320
Han HJ, Yu H, Yu XJ 2016 Evidence for zoonotic origins of Middle East respiratory syndrome coronavirus. Journal of General Virology 97:274–280. https://doi.org/10.1099/jgv.0.000342
Fasihi Harandi M, Hobbs RP, Adams PJ, Mobedi I, Morgan-Ryan UM, Thompson RCA 2002 Molecular and morphological characterization of Echinococcus granulosus of human and animal origin in Iran. Parasitology 125:367-373. https://doi.org/10.1017/s0031182002002172
Haridy FM, El-Metwally MT, Khalil HH, Morsy TA 2011 Trypanosoma evansi in dromedary camel: with a case report of zoonosis in greater Cairo, Egypt. Journal of the Egyptian Society of Parasitology 41:65–76.
Hassanain MA, Shaapan RM, Khalil FAM 2016 Sero-epidemiological value of some hydatid cyst antigen in diagnosis of human cystic echinococcosis. Journal of Parasitic Diseases 40:52–56. https://doi.org/10.1007/s12639-014-0443-5
Hemida MG, Al-Naeem A, Perera RAPM, Chin AWH, Poon LLM, Peiris M 2015 Lack of Middle East Respiratory Syndrome Coronavirus Transmission from Infected Camels. Emerging Infectious Diseases 21:699–701. https://doi.org/10.3201/eid2104.141949
Hemida MG, Chu DKW, Poon LLM, Perera RAPM, Alhammadi MA, Ng H, Siu LY, Guan Y, Alnaeem A, Peiris M 2014 MERS Coronavirus in Dromedary Camel Herd, Saudi Arabia. Emerging Infectious Diseases. https://doi.org/10.3201/eid2007.140571
Hemida MG, Elmoslemany A, Al-Hizab F, Alnaeem A, Almathen F, Faye B, Chu DKW, Perera RAPM, Peiris M 2017 Dromedary Camels and the Transmission of Middle East Respiratory Syndrome Coronavirus MERS-CoV. Transboundary and Emerging Diseases 64:344–353. https://doi.org/10.1111/tbed.12401
Hemida M, Perera R, Wang P, Alhammadi M, Siu L, Li M, Poon L, Saif L, Alnaeem A, Peiris M 2013 Middle East Respiratory Syndrome MERS coronavirus seroprevalence in domestic livestock in Saudi Arabia, 2010 to 2013. Eurosurveillance 18:20659. https://doi.org/10.2807/1560-7917.es2013.18.50.20659
Holmes D 2014 MERS-CoV enigma deepens as reported cases surge. The Lancet 383:1793. https://doi.org/10.1016/s0140-67361460866-7
Horton KC, Wasfy M, Samaha H, Abdel-Rahman B, Safwat S, Abdel Fadeel M, Mohareb E, Dueger E 2014 Serosurvey for Zoonotic Viral and Bacterial Pathogens Among Slaughtered Livestock in Egypt. Vector-Borne and Zoonotic Diseases 14:633–639. https://doi.org/10.1089/vbz.2013.1525
Hunter JC, Nguyen D, Aden B, Al Bandar Z, Al Dhaheri W, Abu Elkheir K, Khudair A, Al Mulla M, El Saleh F, Imambaccus H, Al Kaabi N, Sheikh FA, Sasse J, Turner A, Abdel Wareth L, Weber S, Al Ameri A, Abu Amer W, Alami NN, Bunga S, Haynes LM, Hall AJ, Kallen AJ, Kuhar D, Pham H, Pringle K, Tong S, Whitaker BL, Gerber SI, Al Hosani FI 2016 Transmission of Middle East Respiratory Syndrome Coronavirus Infections in Healthcare Settings, Abu Dhabi. Emerging Infectious Diseases 22:647–656. https://doi.org/10.3201/eid2204.151615
Ikegami T, Makino S 2011 The Pathogenesis of Rift Valley Fever. Viruses 3:493–519. https://doi.org/10.3390/v3050493
IUCN (2008) Camelus ferus: the IUCN red list of threatened species 2008: e. T63543a12689285
Jäckel S, Eiden M, EL Mamy BO, Isselmou K, Vina-Rodriguez A, Doumbia B, Groschup MH 2013 Molecular and Serological Studies on the Rift Valley Fever Outbreak in Mauritania in 2010. Transboundary and Emerging Diseases 60:31–39. https://doi.org/10.1111/tbed.12142
Jaros P, Cogger N, French N 2008 A systematic review of the human disease evidence associated with the consumption of raw milk and raw milk cheeses. Massey University 92:5.
Jere KC, Esona MD, Ali YH, Peenze I, Roy S, Bowen MD, Saeed IK, Khalafalla AI, Nyaga MM, Mphahlele J, Steele D, Seheri ML 2014 Novel NSP1 genotype characterised in an African camel G8P[11] rotavirus strain. Infection, Genetics and Evolution 21:58–66. https://doi.org/10.1016/j.meegid.2013.10.002
Jezek Z, Kríz B, Rothbauer V 1983 Camelpox and its risk to the human population. Journal of Hygiene, Epidemiology, Microbiology, and Immunology 27:29–42.
Kaindi DWM, Schelling E, Wangoh JM, Imungi JK, Farah Z, Meile L 2012 Risk Factors for Symptoms of Gastrointestinal Illness in Rural Town Isiolo, Kenya: Symptoms of Gastrointestinal Illness in Rural Town Isiolo. Zoonoses and Public Health 59:118–125. https://doi.org/10.1111/j.1863-2378.2011.01425.x
Kamenetzky L, Gutierrez AM, Canova SG, Haag KL, Guarnera EA, Parra A, Garcı́a GE, Rosenzvit MC 2002 Several strains of Echinococcus granulosus infect livestock and humans in Argentina. Infection, Genetics and Evolution 2:129–136. https://doi.org/10.1016/s1567-13480200131-4
Karimi M, Ghasemikhah R, Mirahmadi H, Spotin A, Rouhani S, Seyyed Tabaei SJ 2017 Discrimination of Mixed Infections of Echinococcus Species Based on in Silico Sequence Analysis: A New Way of Reflecting Overlapped Strains in Indigenous Areas. Archives of Clinical Infectious Diseases 12:4. https://doi.org/10.5812/archcid.14168
Kayali G, Peiris M 2015 A more detailed picture of the epidemiology of Middle East respiratory syndrome coronavirus. The Lancet Infectious Diseases 15:495–497. https://doi.org/10.1016/s1473-30991570128-3
Khalafalla AI, Lu X, Al-Mubarak AIA, Dalab AHS, Al-Busadah KAS, Erdman DD 2015 MERS-CoV in Upper Respiratory Tract and Lungs of Dromedary Camels, Saudi Arabia, 2013–2014. Emerging Infectious Diseases 21:1153–1158. https://doi.org/10.3201/eid2107.150070
Khalafalla AI, Abdelazim F 2017 Human and Dromedary Camel Infection with Camelpox Virus in Eastern Sudan. Vector-Borne and Zoonotic Diseases 17:281–284. https://doi.org/10.1089/vbz.2016.2070
Khan AS, Maupin GO, Rollin PE, Noor AM, Shurie HH, Shalabi AG, Wasef S, Haddad YM, Sadek R, Ijaz K, Peters CJ, Ksiazek TG 1997 An Outbreak of Crimean-Congo Hemorrhagic Fever in the United Arab Emirates, 1994–1995. The American Journal of Tropical Medicine and Hygiene 57:519–525. https://doi.org/10.4269/ajtmh.1997.57.519
Khuroo MS, Khuroo MS 2016 Hepatitis E: an emerging global disease—from discovery towards control and cure. Journal of Viral Hepatitis 23:68–79. https://doi.org/10.1111/jvh.12445
Kia EB, Rahimi H, Sharbatkhori M, Talebi A, Fasihi Harandi M, Mirhendi H 2010 Genotype identification of human cystic echinococcosis in Isfahan, central Iran. Parasitology Research 107:757–760. https://doi.org/10.1007/s00436-010-1947-2
Kiel FW, Yousuf KM 1989 Brucellosis in Saudi Arabia. Social Science & Medicine 29:999–1001. https://doi.org/10.1016/0277-95368990056-7
Kinkar L, Laurimäe T, Sharbatkhori M, Mirhendi H, Kia EB, Ponce-Gordo F, Andresiuk V, Simsek S, Lavikainen A, Irshadullah M, Umhang G, Oudni-M’rad M, Acosta-Jamett G, Rehbein S, Saarma U 2017 New mitogenome and nuclear evidence on the phylogeny and taxonomy of the highly zoonotic tapeworm Echinococcus granulosus sensu stricto. Infection, Genetics and Evolution 52:52–58. https://doi.org/10.1016/j.meegid.2017.04.023
Kleinerman G, Baneth G, Mumcuoglu KY, van Straten M, Berlin D, Apanaskevich DA, Abdeen Z, Nasereddin A, Harrus S 2013 Molecular Detection of Rickettsia africae, Rickettsia aeschlimannii, and Rickettsia sibirica mongolitimonae in Camels and Hyalomma spp. Ticks from Israel. Vector-Borne and Zoonotic Diseases 13:851–856. https://doi.org/10.1089/vbz.2013.1330
Klemmer J, Njeru J, Emam A, El-Sayed A, Moawad AA, Henning K, Elbeskawy MA, Sauter-Louis C, Straubinger RK, Neubauer H, El-Diasty MM 2018 Q fever in Egypt: Epidemiological survey of Coxiella burnetii specific antibodies in cattle, buffaloes, sheep, goats and camels. PLOS ONE 13:e0192188. https://doi.org/10.1371/journal.pone.0192188
Kupferschmidt K 2014 The Camel Connection. Science 343:1422–1425. https://doi.org/10.1126/science.343.6178.1422
Kupferschmidt K 2015 MERS surges again, but pandemic jitters ease. Science 347:1296–1297. https://doi.org/10.1126/science.347.6228.1296
Latif AA, Tanveer A, Maqbool A, Siddiqi N, Kyaw-Tanner M, Traub RJ 2010 Morphological and molecular characterisation of Echinococcus granulosus in livestock and humans in Punjab, Pakistan. Veterinary Parasitology 170:44–49. https://doi.org/10.1016/j.vetpar.2010.02.003
Lee G-H, Tan B-H, Chi-Yuan Teo E, Lim S-G, Dan Y-Y, Wee A, Kim Aw PP, Zhu Y, Hibberd ML, Tan C-K, Purdy MA, Teo C-G 2016 Chronic Infection with Camelid Hepatitis E Virus in a Liver Transplant Recipient Who Regularly Consumes Camel Meat and Milk. Gastroenterology 150:355–357.e3. https://doi.org/10.1053/j.gastro.2015.10.048
Leslie T, Whitehouse CA, Yingst S, Baldwin C, Kakar F, Mofleh J, Hami AS, Mustafa L, Omar F, Ayazi E, Rossi C, Noormal B, Ziar N, Kakar R 2011 Outbreak of gastroenteritis caused by Yersinia pestis in Afghanistan. Epidemiology and Infection 139:728–735. https://doi.org/10.1017/s0950268810001792
Liljander A, Meyer B, Jores J, Müller MA, Lattwein E, Njeru I, Bett B, Drosten C, Corman VM 2016 MERS-CoV Antibodies in Humans, Africa, 2013–2014. Emerging Infectious Diseases 22:1086–1089. https://doi.org/10.3201/eid2206.160064
Linthicum KJ, Britch SC, Anyamba A 2016 Rift Valley Fever: An Emerging Mosquito-Borne Disease. Annual Review of Entomology 61:395–415. https://doi.org/10.1146/annurev-ento-010715-023819
Lutomiah J, Omondi D, Masiga D, Mutai C, Mireji PO, Ongus J, Linthicum KJ, Sang R 2014 Blood Meal Analysis and Virus Detection in Blood-Fed Mosquitoes Collected During the 2006–2007 Rift Valley Fever Outbreak in Kenya. Vector-Borne and Zoonotic Diseases 14:656–664. https://doi.org/10.1089/vbz.2013.1564
Mackay IM, Arden KE 2015 Middle East respiratory syndrome: an emerging coronavirus infection tracked by the crowd. Virus Research 202:60–88. https://doi.org/10.1016/j.virusres.2015.01.021
Mackay I, Arden K 2017 An Opportunistic Pathogen Afforded Ample Opportunities: Middle East Respiratory Syndrome Coronavirus. Viruses 9:369. https://doi.org/10.3390/v9120369
Macpherson CNL, McManus DP 1982 A comparative study of Echinococcus granulosus from human and animal hosts in Kenya using isoelectric focusing and isoenzyme analysis. International Journal for Parasitology 12:515–521. https://doi.org/10.1016/0020-75198290046-7
Macpherson CNL, Smyth JD 1985 In vitro culture of the strobilar stage of Echinococcus granulosus from protoscoleces of human, camel, cattle, sheep and goat origin from Kenya and buffalo origin from India. International Journal for Parasitology 15:137–140. https://doi.org/10.1016/0020-75198590078-
Maillard S, Benchikh-Elfegoun MC, Knapp J, Bart JM, Koskei P, Gottstein B, Piarroux R 2006 Taxonomic position and geographical distribution of the common sheep G1 and camel G6 strains of Echinococcus granulosus in three African countries. Parasitology Research 100:495–503. https://doi.org/10.1007/s00436-006-0286-9
Majumder M (2015) Middle East respiratory syndrome in the Kingdom of Saudi Arabia: insights from publicly available data. Thesis, Massachusetts Institute of Technology
Mandal S, Deb Mandal M 2012 Human cystic echinococcosis: epidemiologic, zoonotic, clinical, diagnostic and therapeutic aspects. Asian Pacific Journal of Tropical Medicine 5:253–260. https://doi.org/10.1016/s1995-76451260035-2
McCarthy J, Moore TA 2000 Emerging helminth zoonoses. International Journal for Parasitology 30:1351–1359. https://doi.org/10.1016/s0020-75190000122-3
McManus DP 1981 A biochemical study of adult and cystic stages of Echinococcus granulosus of human and animal origin from Kenya. Journal of Helminthology 55:21–28. https://doi.org/10.1017/s0022149x00025414
McManus DP, Rishi AK 1989 Genetic heterogeneity within Echinococcus granulosus: isolates from different hosts and geographical areas characterized with DNA probes. Parasitology 99:17-29. https://doi.org/10.1017/s0031182000060984
Megersa B, Biffa D, Abunna F, Regassa A, Godfroid J, Skjerve E 2011 Seroprevalence of brucellosis and its contribution to abortion in cattle, camel, and goat kept under pastoral management in Borana, Ethiopia. Tropical Animal Health and Production 43:651–656. https://doi.org/10.1007/s11250-010-9748-2
Megersa B, Biffa D, Abunna F, Regassa A, Godfroid J, Skjerve E 2012 Seroepidemiological study of livestock brucellosis in a pastoral region. Epidemiology and Infection 140:887–896. https://doi.org/10.1017/s0950268811001178
Memish ZA, Alsahly A, Masri M, Heil GL, Anderson BD, Peiris M, Khan SU, Gray GC 2015 Sparse evidence of MERS-CoV infection among animal workers living in Southern Saudi Arabia during 2012. Influenza and Other Respiratory Viruses 9:64–67. https://doi.org/10.1111/irv.12287
Memish ZA, Balkhy HH 2004 Brucellosis and International Travel. Journal of Travel Medicine 11:49–55. https://doi.org/10.2310/7060.2004.13551
Memish ZA, Cotten M, Meyer B, Watson SJ, Alsahafi AJ, Al Rabeeah AA, Corman VM, Sieberg A, Makhdoom HQ, Assiri A, Al Masri M, Aldabbagh S, Bosch B-J, Beer M, Müller MA, Kellam P, Drosten C 2014 Human Infection with MERS Coronavirus after Exposure to Infected Camels, Saudi Arabia, 2013. Emerging Infectious Diseases 20:1012–1015. https://doi.org/10.3201/eid2006.140402
Memish ZA, Cotten M, Watson SJ, Kellam P, Zumla A, Alhakeem RF, Assiri A, Rabeeah AAA, Al-Tawfiq JA 2014 Community case clusters of Middle East respiratory syndrome coronavirus in Hafr Al-Batin, Kingdom of Saudi Arabia: A Descriptive Genomic study. International Journal of Infectious Diseases 23:63–68. https://doi.org/10.1016/j.ijid.2014.03.1372
Merrill HR, Khan SU, Anderson BD, Heil GL, Alsahly A, Memish ZA, Gray GC, Masri MA 2015 Elevated Antibodies Against Rift Valley Fever Virus Among Humans with Exposure to Ruminants in Saudi Arabia. The American Journal of Tropical Medicine and Hygiene 92:739–743. https://doi.org/10.4269/ajtmh.14-0575
Memish ZA, Zumla AI, Al-Hakeem RF, Al-Rabeeah AA, Stephens GM 2013 Family Cluster of Middle East Respiratory Syndrome Coronavirus Infections. New England Journal of Medicine 368:2487–2494. https://doi.org/10.1056/nejmoa1303729
Mertens M, Schmidt K, Ozkul A, Groschup MH 2013 The impact of Crimean-Congo hemorrhagic fever virus on public health. Antiviral Research 98:248–260. https://doi.org/10.1016/j.antiviral.2013.02.007
Meyer B, Juhasz J, Barua R, Das Gupta A, Hakimuddin F, Corman VM, Müller MA, Wernery U, Drosten C, Nagy P 2016 Time Course of MERS-CoV Infection and Immunity in Dromedary Camels. Emerging Infectious Diseases 22:2171–2173. https://doi.org/10.3201/eid2212.160382
Meyer B, Müller MA, Corman VM, Reusken CBEM, Ritz D, Godeke G-J, Lattwein E, Kallies S, Siemens A, van Beek J, Drexler JF, Muth D, Bosch B-J, Wernery U, Koopmans MPG, Wernery R, Drosten C 2014 Antibodies against MERS Coronavirus in Dromedary Camels, United Arab Emirates, 2003 and 2013. Emerging Infectious Diseases 20:552–559. https://doi.org/10.3201/eid2004.131746
Miguel E, Chevalier V, Ayelet G, Ben Bencheikh MN, Boussini H, Chu DK, El Berbri I, Fassi-Fihri O, Faye B, Fekadu G, Grosbois V, Ng BC, Perera RA, So T, Traore A, Roger F, Peiris M 2017 Risk factors for MERS coronavirus infection in dromedary camels in Burkina Faso, Ethiopia, and Morocco, 2015. Eurosurveillance 22:30498. https://doi.org/10.2807/1560-7917.es.2017.22.13.30498
Miguel E, Perera RAPM, Baubekova A, Chevalier V, Faye B, Akhmetsadykov N, Ng CY, Roger F, Peiris M 2016 Absence of Middle East Respiratory Syndrome Coronavirus in Camelids, Kazakhstan, 2015. Emerging Infectious Diseases 22:555–557. https://doi.org/10.3201/eid2203.151284
Mirzaei M, Rezaei H, Nematollahi A, Ashrafihelan J 2016 Survey of hydatidosis infection in slaughtered camel Camelus dromedarius in Tabriz area, Northwest Iran. Journal of Parasitic Diseases 40:444–447. https://doi.org/10.1007/s12639-014-0523-6
Moallin ASM, Zessin KH 1988 Outbreak of camel contagious ecthyma in central Somalia. Tropical Animal Health and Production 20:185–186. https://doi.org/10.1007/bf02240091
Mohabbati Mobarez A, Bagheri Amiri F, Esmaeili S 2017 Seroprevalence of Q fever among human and animal in Iran; A systematic review and meta-analysis. PLOS Neglected Tropical Diseases 11:e0005521. https://doi.org/10.1371/journal.pntd.0005521
Mobedi I, Madadi H, Arfaa F 1970 Camel, Camelus dromedarius, as Intermediate Host of Echinococcus granulosus in Iran. The Journal of Parasitology 56:1255. https://doi.org/10.2307/3277581
Moda G, Daborn CJ, Grange JM, Cosivi O 1996 The zoonotic importance of Mycobacterium bovis. Tubercle and Lung Disease 77:103–108. https://doi.org/10.1016/s0962-84799690022-2
Mohd HA, Al-Tawfiq JA, Memish ZA 2016 Middle East Respiratory Syndrome Coronavirus MERS-CoV origin and animal reservoir. Virology Journal 13:87. https://doi.org/10.1186/s12985-016-0544-0
M’rad S, Filisetti D, Oudni M, Mekki M, Belguith M, Nouri A, Sayadi T, Lahmar S, Candolfi E, Azaiez R, Mezhoud H, Babba H 2005 Molecular evidence of ovine G1 and camel G6 strains of Echinococcus granulosus in Tunisia and putative role of cattle in human contamination. Veterinary Parasitology 129:267–272. https://doi.org/10.1016/j.vetpar.2005.02.006
Muhairi SA, Hosani FA, Eltahir YM, Mulla MA, Yusof MF, Serhan WS, Hashem FM, Elsayed EA, Marzoug BA, Abdelazim AS 2016 Epidemiological investigation of Middle East respiratory syndrome coronavirus in dromedary camel farms linked with human infection in Abu Dhabi Emirate, United Arab Emirates. Virus Genes 52:848–854. https://doi.org/10.1007/s11262-016-1367-1
Muloi D, Alarcon P, Ombui J, Ngeiywa KJ, Abdullahi B, Muinde P, Karani MK, Rushton J, Fèvre EM 2018 Value chain analysis and sanitary risks of the camel milk system supplying Nairobi city, Kenya. Preventive Veterinary Medicine 159:203–210. https://doi.org/10.1016/j.prevetmed.2018.09.010
Müller MA, Corman VM, Jores J, Meyer B, Younan M, Liljander A, Bosch B-J, Lattwein E, Hilali M, Musa BE, Bornstein S, Drosten C 2014 MERS Coronavirus Neutralizing Antibodies in Camels, Eastern Africa, 1983–1997. Emerging Infectious Diseases 20:2093-2095. https://doi.org/10.3201/eid2012.141026
Müller MA, Meyer B, Corman VM, Al-Masri M, Turkestani A, Ritz D, Sieberg A, Aldabbagh S, Bosch B-J, Lattwein E, Alhakeem RF, Assiri AM, Albarrak AM, Al-Shangiti AM, Al-Tawfiq JA, Wikramaratna P, Alrabeeah AA, Drosten C, Memish ZA 2015 Presence of Middle East respiratory syndrome coronavirus antibodies in Saudi Arabia: a nationwide, cross-sectional, serological study. The Lancet Infectious Diseases 15:559–564. https://doi.org/10.1016/s1473-30991570090-3
Macharia J, Murithi RM, Wainwright S, Breiman RF, Munyua P, Bloland P, Njenga MK, Githinji J, Hightower A, Ithondeka PM, Mutonga D, Musaa J 2010 Rift Valley Fever Outbreak in Livestock in Kenya, 2006–2007. The American Journal of Tropical Medicine and Hygiene 83:58–64. https://doi.org/10.4269/ajtmh.2010.09-0292
Musa MT, Shomein AM, El Razig YA, Meki NT, El Hassan SM 1993 Anthrax in humans and camels in the Sudan with reference to the disease in the country. Journal of Tropical Livestock Science 46:438–439 https://doi.org/10.19182/remvt.9438
Ng DL, Al Hosani F, Keating MK, Gerber SI, Jones TL, Metcalfe MG, Tong S, Tao Y, Alami NN, Haynes LM, Mutei MA, Abdel-Wareth L, Uyeki TM, Swerdlow DL, Barakat M, Zaki SR 2016 Clinicopathologic, Immunohistochemical, and Ultrastructural Findings of a Fatal Case of Middle East Respiratory Syndrome Coronavirus Infection in the United Arab Emirates, April 2014. The American Journal of Pathology 186:652–658. https://doi.org/10.1016/j.ajpath.2015.10.024
Nimri LF 2003 Diagnosis of recent and relapsed cases of human brucellosis by PCR assay. BMC Infectious Diseases 3:5. https://doi.org/10.1186/1471-2334-3-5
Njeru J, Henning K, Pletz MW, Heller R, Neubauer H 2016 Q fever is an old and neglected zoonotic disease in Kenya: a systematic review. BMC Public Health 16. https://doi.org/10.1186/s12889-016-2929-9
Nowotny N, Kolodziejek J 2014 Middle East respiratory syndrome coronavirus MERS-CoV in dromedary camels, Oman, 2013. Eurosurveillance 19:20781. https://doi.org/10.2807/1560-7917.es2014.19.16.20781
Oksanen A, Lavikainen A 2015 Echinococcus canadensis transmission in the North. Veterinary Parasitology 213:182–186. https://doi.org/10.1016/j.vetpar.2015.07.03
Oladipo JO (2015) Virologic and sero-epidemiological studies of Middle East respiratory syndrome coronavirus MERS-CoV infections in dromedary camels in Nigeria. HKU Theses Online Retrieved
Olival KJ, Epstein J (2015) Animal Reservoirs of Middle East Respiratory Syndrome Coronavirus. In: Emerging viral diseases: the one health connection: workshop summary, vol 1. Washington, DC: National Academies Press, pp 119–132
Omer RA, Dinkel A, Romig T, Mackenstedt U, Elnahas AA, Aradaib IE, Ahmed ME, Elmalik KH, Adam A 2010 A molecular survey of cystic echinococcosis in Sudan. Veterinary Parasitology 169:340–346. https://doi.org/10.1016/j.vetpar.2010.01.004
Omer MM, Musa MT, Bakhiet MR, Perrett 2010 Brucellosis in camels, cattle and humans: associations and evaluation of serological tests used for diagnosis of the disease in certain nomadic localities in Sudan. Rev Sci Tech 29:663–669.
Omrani AS, Al-Tawfiq JA, Memish ZA 2015 Middle East respiratory syndrome coronavirus MERS-CoV: animal to human interaction. Pathogens and Global Health 109:354–362. https://doi.org/10.1080/20477724.2015.1122852
Omrani AS, Shalhoub S 2015 Middle East respiratory syndrome coronavirus MERS-CoV: what lessons can we learn? Journal of Hospital Infection 91:188–196. https://doi.org/10.1016/j.jhin.2015.08.002
Oryan A, Khordadmehr M, Ranjbar VR 2011 Prevalence, biology, pathology, and public health importance of linguatulosis of camel in Iran. Tropical Animal Health and Production 43:1225–1231. https://doi.org/10.1007/s11250-011-9830-4
Osoro EM, Munyua P, Omulo S, Ogola E, Ade F, Mbatha P, Mbabu M, Nganga A, Kairu S, Maritim M, Thumbi S, Bitek A, Gaichugi S, Rubin C, Njenga K, Guerra, M 2015 Strong association between human and animal brucella seropositivity in a linked study in Kenya, 2012–2013. The American Journal of Tropical Medicine and Hygiene 93:224–231 https://doi.org/10.4269/ajtmh.15-0113
Pappas G 2010 The changing Brucella ecology: novel reservoirs, new threats. International Journal of Antimicrobial Agents 36:S8–S11. https://doi.org/10.1016/j.ijantimicag.2010.06.013
Park SW, Perera RAPM, Choe PG, Lau EHY, Choi SJ, Chun JY, Oh HS, Song K-H, Bang JH, Kim ES, Kim HB, Park WB, Kim NJ, Poon LLM, Peiris M, Oh MD 2015 Comparison of serological assays in human Middle East respiratory syndrome MERS-coronavirus infection. Eurosurveillance 20. https://doi.org/10.2807/1560-7917.es.2015.20.41.30042
Pavio N, Meng X-J, Doceul V 2015 Zoonotic origin of hepatitis E. Current Opinion in Virology 10:34–41. https://doi.org/10.1016/j.coviro.2014.12.006
Paweska JT 2015 Rift Valley fever. Revue Scientifique Et Technique International Office of Epizootics 34:375–389.
Pearce-Duvet JMC 2006 The origin of human pathogens: evaluating the role of agriculture and domestic animals in the evolution of human disease. Biological Reviews 81:369-382. https://doi.org/10.1017/s1464793106007020
Pirouz HJ, Mohammadi G, Mehrzad J, Azizzadeh M, Nazem Shirazi MH 2015 Seroepidemiology of Q fever in one-humped camel population in northeast Iran. Tropical Animal Health and Production 47:1293–1298. https://doi.org/10.1007/s11250-015-0862-z
QGIS Development Team (2019) QGIS Geographic Information System. Open Source Geospatial Foundation Project. http://qgis.osgeo.org
Rabaan AA 2017 Middle East respiratory syndrome coronavirus: five years later. Expert Review of Respiratory Medicine 11:901–912. https://doi.org/10.1080/17476348.2017.1367288
Rahimi E, Ameri M, Kazemeini HR 2010 Prevalence and antimicrobial resistance of Campylobacter species isolated from raw camel, beef, lamb, and goat meat in Iran. Foodborne Pathogens and Disease 7:443–447. https://doi.org/10.1089/fpd.2009.0421
Rahimi E, Kazemeini HR, Salajegheh M 2012 Escherichia coli O157:H7/NM prevalence in raw beef, camel, sheep, goat, and water buffalo meat in Fars and Khuzestan provinces, Iran. Veterinary Research Forum 3:15–17.
Rahimi E, Kheirabadi EK 2012 Detection of Helicobacter pylori in bovine, buffalo, camel, ovine, and caprine milk in Iran. Foodborne Pathogens and Disease 9:453–456. https://doi.org/10.1089/fpd.2011.1060
Raj VS, Farag EABA, Reusken CBEM, Lamers MM, Pas SD, Voermans J, Smits SL, Osterhaus ADME, Al-Mawlawi N, Al-Romaihi HE, AlHajri MM, El-Sayed AM, Mohran KA, Ghobashy H, Alhajri F, Al-Thani M, Al-Marri SA, El-Maghraby MM, Koopmans MPG, Haagmans BL 2014 Isolation of MERS coronavirus from a dromedary camel, Qatar, 2014. Emerging Infectious Diseases 20:1339-1342. https://doi.org/10.3201/eid2008.140663
Rasche A, Saqib M, Liljander AM, Bornstein S, Zohaib A, Renneker S, Steinhagen K, Wernery R, Younan M, Gluecks I, Hilali M, Musa BE, Jores J, Wernery U, Drexler JF, Drosten C, Corman VM 2016 Hepatitis E virus infection in dromedaries, North and East Africa, United Arab Emirates, and Pakistan, 1983–2015. Emerging Infectious Diseases 22:1249–1252. https://doi.org/10.3201/eid2207.160168
Rasis M, Rudoler N, Schwartz D, Giladi M 2014 Bartonella dromedarii sp. nov. Isolated from domesticated camels Camelus dromedarius in Israel. Vector-Borne and Zoonotic Diseases 14:775–782. https://doi.org/10.1089/vbz.2014.1663
Rasmussen SA, Gerber SI, Swerdlow DL 2015 Middle East respiratory syndrome coronavirus: update for clinicians. Clinical Infectious Diseases 60:1686–1689. https://doi.org/10.1093/cid/civ118
Rasmussen SA, Watson AK, Swerdlow DL 2016 Middle East respiratory syndrome MERS. Microbiology Spectrum 4:3. https://doi.org/10.1128/microbiolspec.ei10-0020-2016
Raufu IA, Odetokun IA, Oladunni FS, Adam M, Kolapo UT, Akorede GJ, Ghali IM, Ameh JA, Ambali A 2015 Serotypes, antimicrobial profiles, and public health significance of Salmonella from camels slaughtered in Maiduguri central abattoir, Nigeria. Veterinary World 8:1068–1072. https://doi.org/10.14202/vetworld.2015.1068-1072
Reeves T, Samy AM, Peterson AT 2015 MERS-CoV geography and ecology in the Middle East: analyses of reported camel exposures and a preliminary risk map. BMC Research Notes 8:801. https://doi.org/10.1186/s13104-015-1789-1
Reusken C, Ababneh M, Raj V, Meyer B, Eljarah A, Abutarbush S, Godeke G, Bestebroer T, Zutt I, Müller M, Bosch B, Rottier P, Osterhaus A, Drosten C, Haagmans B, Koopmans M 2013 Middle East respiratory syndrome coronavirus MERS-CoV serology in major livestock species in an affected region in Jordan, June to September 2013. Eurosurveillance 18:20662. https://doi.org/10.2807/1560-7917.es2013.18.50.20662
Reusken CBEM, Farag EABA, Haagmans BL, Mohran KA, Godeke G-J, Raj S, Alhajri F, Al-Marri SA, Al-Romaihi HE, Al-Thani M, Bosch B-J, van der Eijk AA, El-Sayed AM, Ibrahim AK, Al-Molawi N, Müller MA, Pasha SK, Drosten C, AlHajri MM, Koopmans MPG 2015 Occupational exposure to dromedaries and risk for MERS-CoV infection, Qatar, 2013–2014. Emerging Infectious Diseases 21:1422–1425. https://doi.org/10.3201/eid2108.150481
Reusken CB, Farag EA, Jonges M, Godeke GJ, El-Sayed AM, Pas SD, Raj VS, Mohran KA, Moussa HA, Ghobashy H, Alhajri F 2014 Middle East respiratory syndrome coronavirus MERS-CoV RNA and neutralising antibodies in milk collected according to local customs from dromedary camels, Qatar, April 2014. Eurosurveillance. 19:23.
Reusken CB, Haagmans BL, Müller MA, Gutierrez C, Godeke G-J, Meyer B, Muth D, Raj VS, Vries LS-D, Corman VM, Drexler J-F, Smits SL, El Tahir YE, De Sousa R, van Beek J, Nowotny N, van Maanen K, Hidalgo-Hermoso E, Bosch B-J, Rottier P, Osterhaus A, Gortázar-Schmidt C, Drosten C, Koopmans MP 2013 Middle East respiratory syndrome coronavirus neutralising serum antibodies in dromedary camels: a comparative serological study. The Lancet Infectious Diseases 13:859–866. https://doi.org/10.1016/s1473-30991370164-6
Reusken CBEM, Messadi L, Feyisa A, Ularamu H, Godeke G-J, Danmarwa A, Dawo F, Jemli M, Melaku S, Shamaki D, Woma Y, Wungak Y, Gebremedhin EZ, Zutt I, Bosch B-J, Haagmans BL, Koopmans MPG 2014 Geographic Distribution of MERS Coronavirus among Dromedary Camels, Africa. Emerging Infectious Diseases 20:1370–1374. https://doi.org/10.3201/eid2008.140590
Reusken CB, Raj VS, Koopmans MP, Haagmans BL 2016 Cross host transmission in the emergence of MERS coronavirus. Current Opinion in Virology 16:55–62. https://doi.org/10.1016/j.coviro.2016.01.004
Reuss A, Litterst A, Drosten C, Seilmaier M, Böhmer M, Graf P, Gold H, Wendtner C-M, Zanuzdana A, Schaade L, Haas W, Buchholz U 2014 Contact investigation for imported case of middle east respiratory syndrome, Germany. Emerging Infectious Diseases 20:620–625. https://doi.org/10.3201/eid2004.131375
Rezaei F, Tavassoli M, Javdani M 2012 Prevalence and morphological characterizations of Linguatula serrata nymphs in camels in Isfahan Province, Iran. Veterinary Research Forum 3:61–65.
Rhodes HM, Williams DN, Hansen GT 2016 Invasive human brucellosis infection in travelers to and immigrants from the Horn of Africa related to the consumption of raw camel milk. Travel Medicine and Infectious Disease 14:255–260. https://doi.org/10.1016/j.tmaid.2016.03.013
Roser M (2018) Future population growth. Our world in data. https://ourworldindata.org/future-population-growth. Accessed May 3, 2018
Sabir JSM, Lam TT-Y, Ahmed MMM, Li L, Shen Y, Abo-Aba S, Qureshi MI, Abu-Zeid M, Zhang Y, Khiyami MA, Alharbi NS, Hajrah NH, Sabir MJ, Mutwakil MHZ, Kabli SA, Alsulaimany FAS, Obaid AY, Zhou B, Smith DK, Holmes EC, Zhu H, Guan Y 2016 Co-circulation of three camel coronavirus species and recombination of MERS-CoVs in Saudi Arabia. Science 351:81–84. https://doi.org/10.1126/science.aac8608
Sadjjadi SM 2006 Present situation of echinococcosis in the Middle East and Arabic North Africa. Parasitology International 55:S197–S202. https://doi.org/10.1016/j.parint.2005.11.030
Sadjjadi S, Ardehali S, Shojaei A 1998 A case report of linguatula serrata in human pharynx from Shiraz, southern Iran. Medical Journal of the Islamic Republic of Iran MJIRI 12:193–194.
Saeed AAB, Al-Hamdan NA, Fontaine RE 2005 Plague from eating raw camel liver. Emerging Infectious Diseases 11:1456–1457. https://doi.org/10.3201/eid1109.050081
Salehi TZ, Tonelli A, Mazza A, Staji H, Badagliacca P, Tamai IA, Jamshidi R, Harel J, Lelli R, Masson L 2012 Genetic characterization of Escherichia coli O157:H7 Strains isolated from the one-humped camel Camelus dromedarius by using microarray DNA technology. Molecular Biotechnology 51:283–288. https://doi.org/10.1007/s12033-011-9466-7
Salem CO, Schneegans F, Chollet J, Jemli M 2011 Epidemiological studies on echinococcosis and characterization of human and livestock hydatid cysts in Mauritania. Iranian Journal of Parasitology 6:49–57.
Salkeld DJ, Stapp P, Tripp DW, Gage KL, Lowell J, Webb CT, Brinkerhoff RJ, Antolin MF 2016 Ecological traits driving the outbreaks and emergence of zoonotic pathogens. BioScience 66:118–129. https://doi.org/10.1093/biosci/biv179
Saqib M, Sieberg A, Hussain MH, Mansoor MK, Zohaib A, Lattwein E, Müller MA, Drosten C, Corman VM 2017 Serologic evidence for MERS-CoV infection in dromedary camels, Punjab, Pakistan, 2012–2015. Emerging Infectious Diseases 23:550–551. https://doi.org/10.3201/eid2303.161285
Sazmand A, Rasooli A, Nouri M, Hamidinejat H, Hekmatimoghaddam S 2012 Prevalence of cryptosporidium spp. In camels and involved people in Yazd province, Iran. Iranian Journal of Parasitology 7:80–84.
Schelling E, Diguimbaye C, Daoud S, Nicolet J, Boerlin P, Tanner M, Zinsstag J 2003 Brucellosis and Q-fever seroprevalences of nomadic pastoralists and their livestock in Chad. Preventive Veterinary Medicine 61:279–293. https://doi.org/10.1016/j.prevetmed.2003.08.004
Schelling E, Diguimbaye C, Daoud S, Nicolet J, Zinsstag J 2004 Seroprevalences of zoonotic diseases in nomads and their livestock in Chari-Baguirmi, Chad. Medecine Tropicale: Revue Du Corps De Sante Colonial 64:474–477.
Scholz HC, Pearson T, Hornstra H, Projahn M, Terzioglu R, Wernery R, Georgi E, Riehm JM, Wagner DM, Keim PS, Joseph M, Johnson B, Kinne J, Jose S, Hepp CM, Witte A, Wernery U 2014 Genotyping of Burkholderia mallei from an outbreak of glanders in bahrain suggests multiple introduction events. PLoS Neglected Tropical Diseases 8:e3195. https://doi.org/10.1371/journal.pntd.0003195
Seleem MN, Boyle SM, Sriranganathan N 2010 Brucellosis: a re-emerging zoonosis. Veterinary Microbiology 140:392–398. https://doi.org/10.1016/j.vetmic.2009.06.021
Shaalan MA, Memish ZA, Mahmoud SA, Alomari A, Khan MY, Almuneef M, Alalola S 2002 Brucellosis in children: clinical observations in 115 cases. International Journal of Infectious Diseases 6:182–186. https://doi.org/10.1016/s1201-97120290108-6
Shabana II, Zaraket H, Suzuki H 2013 Molecular studies on diarrhea-associated Escherichia coli isolated from humans and animals in Egypt. Veterinary Microbiology 167:532–539. https://doi.org/10.1016/j.vetmic.2013.08.014
Shahnazi M, Hejazi H, Salehi M, Andalib AR 2011 Molecular characterization of human and animal Echinococcus granulosus isolates in Isfahan, Iran. Acta Tropica 117:47–50. https://doi.org/10.1016/j.actatropica.2010.09.002
Shakerian A, Shekarforoush SS, Ghafari Rad H 2008 Prevalence of Linguatula serrata nymphs in one-humped camel Camelus dromedarius in Najaf-Abad, Iran. Research in Veterinary Science 84:243–245. https://doi.org/10.1016/j.rvsc.2007.04.015
Shapiro M, London B, Nigri D, Shoss A, Zilber E, Fogel I 2016 Middle East respiratory syndrome coronavirus: review of the current situation in the world. Disaster and Military Medicine 2:9. https://doi.org/10.1186/s40696-016-0019-2
Shariatzadeh SA, Spotin A, Gholami S, Fallah E, Hazratian T, Mahami-Oskouei M, Montazeri F, Moslemzadeh HR, Shahbazi A 2015 The first morphometric and phylogenetic perspective on molecular epidemiology of Echinococcus granulosus sensu lato in stray dogs in a hyperendemic Middle East focus, northwestern Iran. Parasites and Vectors 8:409. https://doi.org/10.1186/s13071-015-1025-9
Sharif-Yakan A, Kanj SS 2014 Emergence of MERS-CoV in the middle east: origins, transmission, treatment, and perspectives. PLoS Pathogens 10:e1004457. https://doi.org/10.1371/journal.ppat.1004457
Sharma SK, Kataria AK, Shringi BN, Nathawat P, Bhati T, Mohammed N 2013 Detection of hypermucoviscous Klebsiella pneumoniae in camel Camelus dromedarius during an outbreak of acute respiratory tract infection. Journal of Camel Practice and Research 20:139–143.
Sharma M, Sehgal R, Fomda BA, Malhotra A, Malla N 2013 Molecular characterization of Echinococcus granulosus cysts in North Indian patients: identification of G1, G3, G5 and G6 genotypes. PLoS Neglected Tropical Diseases 7:e2262. https://doi.org/10.1371/journal.pntd.0002262
Shchelkunov SN 2013 An increasing danger of zoonotic orthopoxvirus infections. PLoS Pathogens 9:e1003756. https://doi.org/10.1371/journal.ppat.1003756
Shehata MM, Gomaa MR, Ali MA, Kayali G 2016 Middle East respiratory syndrome coronavirus: a comprehensive review. Frontiers of Medicine 10:120–136. https://doi.org/10.1007/s11684-016-0430-6
Shimol SB, Dukhan L, Belmaker I, Bardenstein S, Sibirsky D, Barrett C, Greenberg D 2012 Human brucellosis outbreak acquired through camel milk ingestion in southern Israel. Israel Medical Association Journal 14:475–478.
Singh BB, Dhand NK, Ghatak S, Gill JPS 2014 Economic losses due to cystic echinococcosis in India: need for urgent action to control the disease. Preventive Veterinary Medicine 113:1–12. https://doi.org/10.1016/j.prevetmed.2013.09.007
Smits HL, Kadri SM 2005 Brucellosis in India: a deceptive infectious disease. Indian Journal of Medical Research 122:375–384.
Spahr C, Knauf-Witzens T, Vahlenkamp T, Ulrich RG, Johne R 2018 Hepatitis E virus and related viruses in wild, domestic and zoo animals: a review. Zoonoses and Public Health 65:11–29. https://doi.org/10.1111/zph.12405
Spotin A, Gholami S, Najafi Nasab A, Fallah E, Oskouei MM, Semnani V, Shariatzadeh SA, Shahbazi A 2015 Designing and conducting in silico analysis for identifying of Echinococcus spp. with discrimination of novel haplotypes: an approach to better understanding of parasite taxonomic. Parasitology Research 114:1503–1509. https://doi.org/10.1007/s00436-015-4334-1
Spotin A, Mahami-Oskouei M, Harandi MF, Baratchian M, Bordbar A, Ahmadpour E, Ebrahimi S 2017 Genetic variability of Echinococcus granulosus complex in various geographical populations of Iran inferred by mitochondrial DNA sequences. Acta Tropica 165:10–16. https://doi.org/10.1016/j.actatropica.2016.03.002
Sprague LD, Al-Dahouk S, Neubauer H 2012 A review on camel brucellosis: a zoonosis sustained by ignorance and indifference. Pathogens and Global Health 106:144–149. https://doi.org/10.1179/2047773212y.0000000020
Stenseth NC, Atshabar BB, Begon M, Belmain SR, Bertherat E, Carniel E, Gage KL, Leirs H, Rahalison L 2008 Plague: past, present, and future. PLoS Medicine 5:e3. https://doi.org/10.1371/journal.pmed.0050003
Su S, Wong G, Shi W, Liu J, Lai ACK, Zhou J, Liu W, Bi Y, Gao GF 2016 Epidemiology, Genetic Recombination, and Pathogenesis of Coronaviruses. Trends in Microbiology 24:490–502. https://doi.org/10.1016/j.tim.2016.03.003
Sung JM-L, Lloyd DH, Lindsay JA 2008 Staphylococcus aureus host specificity: comparative genomics of human versus animal isolates by multi-strain microarray. Microbiology 154:1949–1959. https://doi.org/10.1099/mic.0.2007/015289-0
Swai ES, Sindato C 2015 Seroprevalence of Rift Valley fever virus infection in camels dromedaries in northern Tanzania. Tropical Animal Health and Production 47:347–352. https://doi.org/10.1007/s11250-014-0726-y
Tadesse G 2015 A meta-analysis of the proportion of animal Salmonella isolates resistant to drugs used against human salmonellosis in Ethiopia. BMC Infectious Diseases 15:84. https://doi.org/10.1186/s12879-015-0835-x
Tai W, Wang Y, Fett CA, Zhao G, Li F, Perlman S, Jiang S, Zhou Y, Du L 2017 Recombinant receptor-binding domains of multiple middle east respiratory syndrome coronaviruses MERS-CoVs induce cross-neutralizing antibodies against divergent human and camel MERS-CoVs and Antibody Escape Mutants. Journal of Virology 91:e01651-16. https://doi.org/10.1128/jvi.01651-16
Tejedor-Junco MT, González-Martín M, Noé Francisco RG 2015 Identification, antimicrobial susceptibility, and virulence factors of Enterococcus spp. strains isolated from Camels in Canary Islands, Spain. Veterinaria Italiana 179–183. https://doi.org/10.12834/vetit.322.1280.2
Teshome H, Molla B, Tibbo M 2003 A seroprevalence study of camel brucellosis in three camel-rearing regions of Ethiopia. Tropical Animal Health and Production 35:381–390. https://doi.org/10.1023/a:1025874310261
Tigre W, Deresa B, Haile A, Gabriël S, Victor B, Pelt JV, Devleesschauwer B, Vercruysse J, Dorny P 2016 Molecular characterization of Echinococcus granulosus s.l. cysts from cattle, camels, goats and pigs in Ethiopia. Veterinary Parasitology 215:17–21. https://doi.org/10.1016/j.vetpar.2015.10.022
Thompson RCA 2008 The taxonomy, phylogeny and transmission of Echinococcus. Experimental Parasitology 119:439–446. https://doi.org/10.1016/j.exppara.2008.04.016
Utuk AE, Simsek S, Koroglu E, McManus DP 2008 Molecular genetic characterization of different isolates of Echinococcus granulosus in east and southeast regions of Turkey. Acta Tropica 107:192–194. https://doi.org/10.1016/j.actatropica.2008.05.026
Vanderburg S, Rubach MP, Halliday JEB, Cleaveland S, Reddy EA, Crump JA 2014 Epidemiology of Coxiella burnetii Infection in Africa: A onehealth systematic review. PLoS Neglected Tropical Diseases 8:e2787. https://doi.org/10.1371/journal.pntd.0002787
Wachira TM, Bowles J, Zeyhle E, McManus DP 1993 Molecular examination of the sympatry and distribution of sheep and camel strains of echinococcus granulosus in Kenya. The American Journal of Tropical Medicine and Hygiene 48:473–479. https://doi.org/10.4269/ajtmh.1993.48.473
Walker PJ, Widen SG, Wood TG, Guzman H, Tesh RB, Vasilakis N 2016 A global genomic characterization of nairoviruses identifies nine discrete genogroups with distinctive structural characteristics and host-vector associations. The American Journal of Tropical Medicine and Hygiene 94:1107–1122. https://doi.org/10.4269/ajtmh.15-0917
Watson JT, Hall AJ, Erdman DD, Swerdlow DL, Gerber SI 2014 Unraveling the Mysteries of middle east respiratory syndrome coronavirus. Emerging Infectious Diseases 20:1054–1056. https://doi.org/10.3201/eid2006.140322
Watson EE, Kochore HH, Dabasso BH 2016 Camels and climate resilience: adaptation in Northern Kenya. Human Ecology 44:701–713. https://doi.org/10.1007/s10745-016-9858-1
Weaver SC, Reisen WK 2010 Present and future arboviral threats. Antiviral Research 85:328–345. https://doi.org/10.1016/j.antiviral.2009.10.008
Wernery U 2014 Camelid brucellosis: a review. Revue Scientifique Et Technique International Office of Epizootics 33:839–857.
Wernery U, Corman VM, Wong EYM, Tsang AKL, Muth D, Lau SKP, Khazanehdari K, Zirkel F, Ali M, Nagy P, Juhasz J, Wernery R, Joseph S, Syriac G, Elizabeth SK, Patteril NAG, Woo PCY, Drosten C 2015 Acute Middle East Respiratory Syndrome Coronavirus Infection in Livestock Dromedaries, Dubai, 2014. Emerging Infectious Diseases 21:1019–1022. https://doi.org/10.3201/eid2106.150038
Wernery U, Lau SKP, Woo PCY 2016 Genomics and zoonotic infections: Middle East respiratory syndrome. Revue Scientifique et Technique de l’OIE International Office of Epizootics 35:191–202. https://doi.org/10.20506/rst.35.1.2427
Widagdo W, Raj VS, Schipper D, Kolijn K, van Leenders GJLH, Bosch BJ, Bensaid A, Segalés J, Baumgärtner W, Osterhaus ADME, Koopmans MP, van den Brand JMA, Haagmans BL 2016 Differential Expression of the Middle East Respiratory Syndrome Coronavirus Receptor in the Upper Respiratory Tracts of Humans and Dromedary Camels. Journal of Virology 90:4838–4842. https://doi.org/10.1128/jvi.02994-15
Wit E de, van Doremalen N, Falzarano D, Munster VJ 2016 SARS and MERS: recent insights into emerging coronaviruses. Nature Reviews Microbiology 14:523–534. https://doi.org/10.1038/nrmicro.2016.81
Wit E de, Munster VJ 2013 MERS-CoV: the intermediate host identified? The Lancet Infectious Diseases 13:827–828. https://doi.org/10.1016/s1473-30991370193-2
Woo PCY, Lau SKP, Wernery U, Wong EYM, Tsang AKL, Johnson B, Yip CCY, Lau CCY, Sivakumar S, Cai J-P, Fan RYY, Chan K-H, Mareena R, Yuen K-Y 2014 Novel Betacoronavirus in dromedaries of the middle east, 2013. Emerging Infectious Diseases 20:560–572. https://doi.org/10.3201/eid2004.131769
Woods CW, Ospanov K, Myrzabekov A, Favorov M, Plikaytis B, Ashford DA 2004 Risk factors for human anthrax among contacts of anthrax-infected livestock in Kazakhstan. The American Journal of Tropical Medicine and Hygiene 71:48–52. https://doi.org/10.4269/ajtmh.2004.71.48
World Health Organization 2015 Middle East respiratory syndrome coronavirus MERS-CoV summary of current situation, literature update and risk assessment—7 July 2015. Geneva: WHO
World Health Organization 2016 Clinical management of patients with viral haemorrhagic fever: a pocket guide for front-line health workers: interim emergency guidance for country adaption. WHO, Geneva, Switzerland.
World Health Organization (2017) Middle East respiratory syndrome coronavirus MERS-CoV Summary of current situation, literature update and risk assessment—21 July 2017.
Yahya BAI (2015) Sero-epidemiological study of camel brucellosis Camelus dromedarius and associated risk factors in the Butana plain area and Al-gadarief state—Sudan. Thesis, Sudan University of Science and Technology
Younan M, Bornstein S, Gluecks IV 2016 MERS and the dromedary camel trade between Africa and the Middle East. Tropical Animal Health and Production 48:1277–1282. https://doi.org/10.1007/s11250-016-1089-3
Youssef AI, Uga S 2014 Review of parasitic zoonoses in Egypt. Tropical Medicine and Health 42:3–14. https://doi.org/10.2149/tmh.2013-23
Yusof MF, Eltahir YM, Serhan WS, Hashem FM, Elsayed EA, Marzoug BA, Abdelazim AS, Bensalah OKA, Al Muhairi SS 2015 Prevalence of Middle East respiratory syndrome coronavirus MERS-CoV in dromedary camels in Abu Dhabi Emirate, United Arab Emirates. Virus Genes 50:509–513. https://doi.org/10.1007/s11262-015-1174-0
Zewolda SW, Wereta MH 2012 Seroprevalence of brucella infection in camel and its public health significance in selected districts of Afar region, Ethiopia. Journal of Environmental and Occupational Science 12:91–98.
Zhang LH, Chai JJ, Jiao W, Osman Y, McManus DP 1998 Mitochondrial genomic markers confirm the presence of the camel strain G6 genotype of Echinococcus granulosus in north-western China. Parasitology 116:29–33.
Zhang W, McManus DP 2006 Recent advances in the immunology and diagnosis of echinococcosis. FEMS Immunology & Medical Microbiology 47:24–41. https://doi.org/10.1111/j.1574-695x.2006.00060.x
Zhang Z, Shen L, Gu X 2016 Evolutionary Dynamics of MERS-CoV: Potential recombination, positive selection and transmission. Scientific Reports 6:25049. https://doi.org/10.1038/srep25049
Zumla A, Dar O, Kock R, Muturi M, Ntoumi F, Kaleebu P, Eusebio M, Mfinanga S, Bates M, Mwaba P, Ansumana R, Khan M, Alagaili AN, Cotten M, Azhar EI, Maeurer M, Ippolito G, Petersen E 2016 Taking forward a ‘One Health’ approach for turning the tide against the Middle East respiratory syndrome coronavirus and other zoonotic pathogens with epidemic potential. International Journal of Infectious Diseases 47:5–9. https://doi.org/10.1016/j.ijid.2016.06.012
Zumla A, Hui DS, Perlman S 2015 Middle East respiratory syndrome. The Lancet 386:995–1007. https://doi.org/10.1016/s0140-67361560454-8
Zumla AI, Memish ZA 2014 Middle East respiratory syndrome coronavirus: epidemic potential or a storm in a teacup? European Respiratory Journal 43:1243–1248. https://doi.org/10.1183/09031936.00227213
Acknowledgements
This work was made possible by the generous support of the American people through the United States Agency for International Development (USAID) Emerging Pandemic Threats PREDICT Cooperative Agreement No. AID-OAA-A-14-00102. The contents are the responsibility of the authors and do not necessarily reflect the views or the policy of USAID or the US Government, and no official endorsement should be inferred. Thank you to Smithsonian Conservation Biology Institute and Saint Louis Zoo Institute for Conservation Medicine for additional funding to complete this research. Special thanks to our fellow camel researchers and their contributions over the years.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Zhu, S., Zimmerman, D. & Deem, S.L. A Review of Zoonotic Pathogens of Dromedary Camels. EcoHealth 16, 356–377 (2019). https://doi.org/10.1007/s10393-019-01413-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10393-019-01413-7