
Abstract
Background
The care transition is the time when more medication errors occur. The aim of this study is to analyze the usefulness of a pharmacotherapeutic report model at hospital discharge to prevent medication errors and to simplify pharmacotherapy during a patient’s transition from the hospital to primary care.
Methods
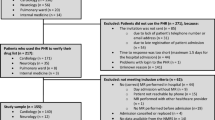
Prospective study including patients diagnosed with chronic obstructive pulmonary disease who were admitted to a short-stay unit or an emergency room. Relevant variables were extracted from the patients’ clinical history and SPSS software was used to carry out the statistical analysis. Direct costs were also calculated.
Results
79.3% of patients were polymedicated, 15.5% of patients were identified as nonadherent to the treatment, 12.1% were users of alternative therapies, and 10.3% had been prescribed drugs that could be monitored. In 32.8% of the reports, reference was made to the primary care pharmacists with a view to resolve any pharmacotherapeutic discrepancies. A total of 132 discrepancies were identified, the majority being related to medicinal requirements (necessary/unnecessary medication). The major cause of drug-related problems (DRPs) were prescription errors. The drugs that were mainly involved in the onset of DRPs belonged to the R group, and the degree of simplification of the pharmacotherapy was 7.6%. The total cost avoided with the reconciliation was 200€/patient.
Conclusion
A continuity program was implemented based on the drafting of a pharmacotherapeutic report, which allowed for detecting discrepancies and updating the patients’ pharmacotherapeutic history, resulting in financial savings after its implementation.
Similar content being viewed by others


References
Estrategia SERGAS 2014. La Sanidad Pública al servicio del Paciente. http://www.sefh.es/sefhpublicaciones/documentos/56_congreso/jueves_14.30_obradoiro_participativa_rubial.pdf. Accessed November 8, 2015.
Ibáñez G. Continuidad asistencial. Análisis conceptual, de los actores y amenazas. Propuestas y alternativas. Medicina de Familia (And). 2003;4:58–66.
Renaudin P, Boyer L, Esteve MA, Bertault-Peres P, Auquier P, Honore S. Do pharmacist-led medication reviews in hospitals help reduce hospital readmissions? A systematic review and meta-analysis. Br J Clin Pharmacol. 2016;82:1660–1673.
Sánchez Rodríguez A. El enfermo con pluripatología: la necesidad de una atención integral coordinada. Med Clín (Barc). 2005;125:12–13.
Lainscak M, Anker SD. Heart failure, chronic obstructive pulmonary disease, and asthma: numbers, facts, and challenges. ESC Heart Fail. 2015;2:103–107.
López Villar S, Fernández García S. Estrategias de Cronicidad en el Ámbito Nacional. Consejería de Sanidad de Asturias. https://www.asturias.es/Astursalud/Ficheros/AS_Salud%20Publica/Estrategias/Estrategia%20Cronicidad/Anexo_II_ESAPCA.pdf. Accessed November 5, 2016.
Laugaland K, Aase K, Barach P. Interventions to improve patient safety in transitional care—a review of the evidence. Work. 2012;41:2915–2924.
Mekonnen AB, McLachlan AJ, Brien JA. Effectiveness of pharmacist-led medication reconciliation programmes on clinical outcomes at hospital transitions: a systematic review and meta-analysis. BMJ Open 2016;6:e010003.
Almanasreh E, Moles R, Chen TF. The medication reconciliation process and classification of discrepancies: a systematic review. Br J Clin Pharmacol. 2016;82:645–658.
Gardner R, Li Q, Baier RR, Butterfield K, Coleman EA, Gravenstein S. Is implementation of the care transitions intervention associated with cost avoidance after hospital discharge? J Gen Intern Med. 2014;29:878–884.
Institute for Healthcare Improvement. Medication reconciliation to prevent adverse drug events. http://www.ihi.org/resources/Pages/Tools/MedicationReconciliationReview.aspx. Accessed December 9, 2016.
Unidad de Pacientes Pluripatológicos. Estándares y Recomendaciones. Informes, Estudios e Investigación. 2009. www.msc.es. Madrid: Ministerio de Sanidad y Política Social.
Villafaina Barroso A, Gavilán Moral E. Pacientes polimedicados frágiles, un reto para el sistema sanitario. Inf Ter Sist Nac Salud. 2011;35:114–123.
Cordón Granados F, Solanas Saura P, Duch Casanova M. Medicinas alternativas y complementarias. AMF 2011;7:4–14.
Rubio-Cebrián B, Santaolalla-García I, Martín-Casasempere I, Segura-Bedmar M. Medication reconciliation in patients over 75 years [in Spanish]. Rev Calid Asist. 2016;31(suppl 1):29–35.
Chan AH, Garratt E, Lawrence B, Turnbull N, Pratapsingh P, Black PN. Effect of education on the recording of medicines on admission to hospital. J Gen Intern Med. 2010;25:537–542.
Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chron Dis. 1987;40:373–383.
Bashir B, Schneider D, Naglak MC, Churilla TM, Adelsberger M. Evaluation of prediction strategy and care coordination for COPD readmissions. Hosp Pract (1995). 2016;44:123–128.
Dillaa T, Valladaresa A, Lizán L, Sacristán JA. Adherencia y persistencia terapéutica: causas, consecuencias y estrategias de mejora. Treatment adherence and persistence: causes, consequences and improvement strategies. Aten Primaria. 2009;41:342–348.
Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24:67–74.
Información Farmacoterapéutica de la Comarca (INFAC). Adherencia al tratamiento farmacológico en patologías crónicas. 19 Liburukia. 2011;19:1–6. http://www.osakidetza.euskadi.eus/contenidos/informacion/cevime_infac/es_cevime/adjuntos/infac_v19_n1.pdf. Accessed October 10, 2016.
Martínez Mir F. Adherencia al tratamiento en el paciente anciano. Inf Ter Sist Nac Salud 2014;28:113–120.
Ahmad A, Mast MR, Nijpels G, Elders PJ, Dekker JM, Hugtenburg JG. Identification of drug-related problems of elderly patients discharged from hospital. Patient Prefer Adherence 2014;8:155–165.
Surbhi S, Munshi KD, Bell PC, Bailey JE. Drug therapy problems and medication discrepancies during care transitions in super-utilizers. J Am Pharm Assoc (2003) 2016; 56:633–42.
Rafferty A, Denslow S, Michalets EL. Pharmacist-Provided Medication Management in Interdisciplinary Transitions in a Community Hospital (PMIT). Ann Pharmacother 2016;50:649–55.
Información terapéutica del Sistema Nacional de Salud. Subgrupos ATC y Principios activos de mayor consumo en el Sistema Nacional de Salud en 2010. Inf Ter Sist Nac Salud 2011;35:124–8. http://www.msssi.gob.es/ca/biblioPublic/publicaciones/recursos_propios/infMedic/docs/CompletoVol35n4.pdf. Accessed October 10, 2016.
Silva C, Ramalho C, Luz I, Monteiro J, Fresco P. Drug-related problems in institutionalized, polymedicated elderly patients: opportunities for pharmacist intervention. Int J Clin Pharm 2015;37:327–334.
Buckley MS, Harinstein LM, Clark KB, et al. Impact of a clinical pharmacy admission medication reconciliation program on medication errors in “high-risk” patients. Ann Pharmacother 2013;47:1599–610.
Polinski JM, Moore JM, Kyrychenko P, et al. An insurer’s care transition program emphasizes medication reconciliation, reduces readmissions and costs. Health Aff (Millwood) 2016;35:1222–1229.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Romero-Ventosa, E.Y., Gayoso-Rey, M., Samartín-Ucha, M. et al. Pharmacotherapeutic Reports as Tools for Detecting Discrepancies in Continuity of Care. Ther Innov Regul Sci 52, 94–99 (2018). https://doi.org/10.1177/2168479017716716
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1177/2168479017716716