Socioeconomic and Productive Disparity in Child Stunting in the Central Andes of Peru, Taking as a Model the Community of Tunanmarca, Jauja
Socioeconomic and Productive Disparity in Child Stunting in the Central Andes of Peru, Taking as a Model the Community of Tunanmarca, Jauja
Volume 5, Issue 3, Page No 135-141, 2020
Author’s Name: Jorge Castro-Bedriñana1,a), Doris Chirinos-Peinado1, Elva Ríos Ríos2
View Affiliations
1Zootechnic Faculty, Universidad Nacional del Centro del Perú, Huancayo 12000, Perú
2Science Faculty, Universidad Nacional Agraria. Lima 15012, Perú
a)Author to whom correspondence should be addressed. E-mail: jcastro@uncp.edu.pe
Adv. Sci. Technol. Eng. Syst. J. 5(3), 135-141 (2020); ![]() DOI: 10.25046/aj050318
DOI: 10.25046/aj050318
Keywords: Stunting, Agri-food production, Nutritional status, Breastfeeding, Nutritional survey, Public nutrition, Public Health

Export Citations
The differences of stunting through socio-economic and productive indicators in high Andean community of Peru were evaluated ((11°42′58.16′′ S, 75°37′31.13′′ W, altitude 3470 m). Cross-sectional study in 52 mothers with children under 5 years old was carried. A validated nutritional survey was applied. Z-scores height for age and nutritional status were determined using anthropometric methods and WHO criteria. The prevalence of stunting was evaluated by maternal educational level, food and health practices, economic level and family food production. Chi-square tests and Spearman correlations were performed in order to establish associations to P <0.05. Prevalence of stunting was 44.2%. The factors associated with stunting (P <0.05) were: Do not use gas for cooking (r=0.530), weekly economic income <50.00 dollars (r=0.503), weekly expenditure on family food <31.00 dollars (r=0.648), per capita / day expenditure on food <1.10 dollars (r=0.591), mother without studies (r=0.454), no own home ownership (r=0.413), consumption of food before 6 months old (r=0.410), low frequency of quinoa consumption (r=0.423), and fish (r=0.421), presence of childhood anemia (r=0.407); inadequate venting of smoke in the kitchen (r=0.491), not having soap for personal hygiene (r=0.413) and not having a bathroom (r=0.413). Stunting is associated with various socioeconomic, productive and access factors to food. These results demonstrate socio-economic and productive disparities for stunting in rural high Andean areas of central Peru, taking as a model the community of Tunanmarca in Jauja.
Received: 12 March 2020, Accepted: 14 April 2020, Published Online: 03 May 2020
1. Introduction
Food security is assessed at the local, family or individual level, determining indicators of food availability, access and use, and its sustainability [1], in a context of climate change and transition of eating habits [2,3]. In rural areas, availability depends directly on agro-food production and is directly related to access; families with crops and cattle have easy access to food [1]. The biological use of food depends on the capacity of the organism and the health state. Stability affects availability and access [4]. The greatest food insecurity is registered in poor, large families, with limited access to land and in low-income women [5], sustainable agriculture must be promoted to achieve family food security and stunting eradicate [6].
Stunting is associated with non-communicable diseases [7] linked to environmental and social factors that lead to a nutritional transition [7,8]; among them, the lack of education, health or other basic capacities that constitute the well-being of people [9]. The situational diagnosis of food security at the family level can be raised through surveys [10]-[12] and the nutritional evaluation of infants using anthropometric methods [12,13].
The age size index determines stunting and expresses the height of a child with respect to its age, shows if a child is stunted in its growth. Children whose height values for age are below -2 Z-score are classified as stunting; those with less than -3 Z-score are classified as severe stunting [13,14].
Worldwide, 149 million children under 5 years old have stunting. In Peru in 2000, the stunting average in children under 5 years old was 33%, it dropped to 18% in 2012, with an average of 32% in rural areas and 10.5% in urban areas; an average of 12% is reported in 2019; however, the fight against stunting does not end; although national averages show progress, regional data show deep gaps between the coast, highland and jungle regions [15]. There are regions of the highlands whose stunting average exceeds 30%; there are high Andean communities where stunting easily exceeds 60% [11,12]. Another nutritional problem that mainly affects children from 6 and 35 months is anemia, which in 2018 affected 43% [15].
Stunting is closely related to the food insecurity of rural families in the central highlands, especially with factors linked to availability and access [12], [16]; agro-food production levels do not meet its needs.
The production in the plots of the rural families is scarce, a part is stored for a short period, the children being the most vulnerable to a deficient intake of proteins and micro nutrients; their diet is eminently energetic (potato, corn, barley, noodles), the consumption of meat, milk, eggs, fish, fruits and vegetables is rare or null [11]. Similar studies conducted in the province of Jauja, report a stunting prevalence in children under 5 years old, of 21.9% [17].
In this context, the present study aimed to estimate the prevalence of stunting in children under 5 years old and determine the association between some variables of availability, access and use of food of the rural families of the Tunanmarca district, province of Jauja with the stunting prevalence of their children under 5 years old.
2. Materials and methods
2.1. Place and duration of the study
The study was carried out in September 2015, in the Tunanmarca district, province of Jauja, located between Coordinates 11°42′58.16″ S, 75°37′31.13″ W, at an average altitude of 3470 m, with an area of 30.07 km² and 1038 habitants, with a density of 34.5 hab/km². In this district is located the community of the same name whose families are engaged in agricultural work in rainfed conditions (Figure 1).
2.2. Aspecto bioético
The research protocol was evaluated and approved by the Research Institute of the Universidad Nacional del Centro del Perú. The objectives of the study were reported to the mothers, who voluntarily participated in the study, signing the informed consent, agreeing to measure the height and weight of their children.
2.3. Study population
60 peasant families are living in the rural community of Tunanmarca, who have at least one child under 5 years old and reside in the district for more than 5 years. The study worked with the entire population, not requiring a sample; therefore, the results are of high reliability. Of the 60 surveys and anthropometric evaluation of children under 5 years old, 52 had complete information, representing 86.6%. If the families had more than one child under 5 years old, the child in the study was the youngest.
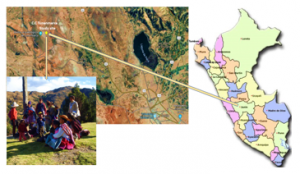
Figure 1. Map of the Peasant Community of Tunanmarca – Jauja, Peru. The community is 76.5 km away from the city of Huancayo and 17.9 km away from the city of Jauja by road. In this place, it is the Tunanmarca Archaeological Center, Pre Inca citadel “Siquillapucara”, cultural heritage of Peru. It was a fortified city, with circular and rectangular single-story houses made of stone and mud; it is a tourist destination in the center of Peru.
2.4. Techniques Applied in the Collection of Information and Measuring Instruments
A questionnaire was used as an instrument with questions about socio-economic, productive, food and health practices of families with children under 5 years old, considering indicators on educational level, monthly income and expenditure on family food, housing conditions, employment , breastfeeding, feeding frequency, vaccination, presence of diarrheal and respiratory diseases, early stimulation practices, disposal of excreta and garbage, crops and breeding, used in other studies under similar conditions [10,12,16]. The use of questionnaires in nutritional studies has the advantages of speed, moderate cost, and covers a wide variety of aspects and facilitates the analysis of the data [18].
Anthropometric data was taken from children under 5 years old, using 02 height meters and 02 SECA-Unicef scales, following standardized protocols [14,19,20]. Figure 2 shows the sequence of the research process followed.
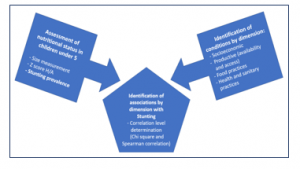
Figure 2. Sequence of the research procedure
2.5. Statistical analysis
The information was tabulated in the SPSS 23 program. The WHO-Anthro 3.2.2 program [14,19,20] was used to determine the Z scores and the nutritional status of the children.
Univariate analysis determines the distribution of data and relative frequencies of each variable studied. The bivariate analysis processed contingency tables with X2 test and Spearman correlation with 95% confidence.
3. Results
3.1. Socio-economic status of the study families
51.9% of children are male and 48.1% female, aged between 1 and 60 months; 36.5% is the first child. The average age of the mothers is 33 years. The families on average have 5 members, with a range of 2 to 10 members. The weekly economic income of the families on average is S/. 157 soles, with a range of 60 to 250 soles. The average weekly expenditure on food is S/. 106 soles, with a range between 35 and 180 soles; the daily per capita expenditure on food is S/. 3.50 soles (Range: 1.40 to 8.50 soles; Change US dollar = 3.30 soles).
2.1% of parents have no studies, 14.6% have primary, and 72.9% secondary and 10.4% have higher education. In moms, 1.9% have no studies, 42.3% have primary, 51.9% secondary and only 3.8% have higher education. 21.2% of the mothers are single, 23.1% married, 51.9% are living together with the husband and 3.8% are divorced or widowed.
57.7% of families own their homes, 7.7% are renters, and 5.9% are caregivers and 28.8% live in their parents’ house. The predominant material of the walls is adobe (84.6%), the rest is concrete and brick. The floor is dirt (88.5%), concrete / ceramic (11.5%) and tile roofs (77%); all homes have electric power. 57.7% of families use firewood for cooking, 5.8% use kerosene and 40.4% use propane gas. 42.3% use only one sleeping room and 48.1% use 2 rooms. 59.6% do not have a place to store firewood and 84.5% do not have a place to store their agricultural tools. 47.7% of kitchens do not have an adequate smoke vent. 53.8% have an exclusive place to store kitchen utensils. In 64% of families, they have animals in the kitchen (guinea pigs, dogs, chickens and cats). 78.8% of families are beneficiaries of some government social support program. In the last 15 days, 40.8% of the parents carried out agricultural work, 32.7% are workers, 16.3% are public / private employees, 8.2% were unemployed and 2% perform outpatient sales. 55.8% of the mothers are engaged in household chores, 32.7% in agriculture and the rest in other independent activities.
3.2. Child malnutrition
7.7% of acute malnutrition (weigh / height) was recorded and in parallel 5.8% overweight, the double burden of malnutrition, due to deficit and excess is observed, which confirms the period of nutritional transition in this community. 9.6% of children have global malnutrition (weight / age).
The stunting prevalence (height / age) determined in the study is 44.2%, including 7.7% of severe stunting (Figure 3), a very critical situation, since the national average is 12% [15]. This result is similar to that reported in Jauja and Janjaillo [11,12], and specifically at the district of Tunamarca, 30.4% of stunting is reported in children under 5 years old [11]. In this study, the prevalence of childhood anemia is 82.7%, an extremely high value associated with conditions of poverty and food insecurity [21].
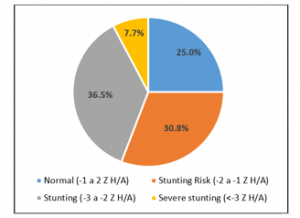
Figure 3. Nutritional status based on Z scores height for age
3.3. Food practices
Of the 52 children under 5-year-old, 88.5% drank breast milk; 65% received before 6 months of age, herbal water, evaporated milk or fresh milk (40%), porridge (30%), juices (5%), family food (5%) and broths (5%). The prevalence of exclusive breastfeeding was 35%.
37% of children consume solid foods more than twice a day and 63% between 3 and 5 times. The most frequently consumed foods are sugar (98%), oil (87.8%), potato (84%), rice (80%), vegetables (57%), fresh milk (47%) and bread (43%). Once a week, they consume olluco (73.5%), beans / lentils (73%), chicken meat (69%), fish (65%), egg (65%), corn (63%), noodles (61 , 2%), broad beans / peas (59%), bananas (59%), barley moron (57%), viscera / tripe (55%), quinoa (51%), citrus fruits (51%), guinea pig meat (42.9%). Less frequently, kiwicha, tarwi, maca and red meat are consumed.
3.4. Health practices, early stimulation and sanitation
86.5% of children have ever been vaccinated, but only 75% have all vaccines for their age. The prevalence of diarrhea and acute respiratory diseases was 28.8 and 32.7%, which are attended in the health facility (92.3%), the rest go to the healer or pharmacy. 75% of children are affiliated with the Sistema Integral de Salud del Ministerio de Salud or Seguro Social and 25% do not have any type of health insurance.
63.5, 55.8, 55.8, 46.2 and 38.5% of the mothers to stimulate the development of their children talk to them, caress them, make them play, sing or tell them stories. 55.8, 46.2, 40.4, 32.7, 30.8% of parents make handmade or buy toys, talk to them, play with them, tell them stories or caress them.
48% of families eliminate their feces in the farm / garden and 52% use a bathroom, latrine or pit. 46% throw trash into the farm and 54% burn it or bury it in the farm. 100% of families use previously treated piped water. 75% drink cold boiled water. 73% have a cleanliness place. 55.8% of mothers wash their hands before eating, 57.7% before preparing food, 48.1% after using the bathroom, 40% before breastfeeding and 21.2% after changing the diaper of babies; 71.2% use soap and water and 28.8% use only water.
3.5. Agro-food production
82.7% of families have farmland. 88.4% grow potatoes, 65% board beans, 55.8% barley, 47.6% grow other products. 44.2% of the families reach what is stored for the whole year; at 48.4% for 6 months and 7% for a maximum of 3 months. 23% have a vegetable garden with more than 3 crops (83.3%), including cabbage, lettuce, board beans, onion, carrot, radish, beet, squash, coriander / parsley, caigua, celery, cauliflower, chard, among others. 53.8% have pastures grown for their livestock, the rest only use natural pastures. 92.3% breed some domestic species, including cattle (43%), poultry (61.2%), pigs (47%), guinea pigs (46%) and sheep (41%), all traditionally raised with poor technological level, whose production is generally sold and serves as a family piggy bank.
3.6. Factors associated with stunting
Tables 1, 2 and 3, and figures 4, 5, 6, 7, 8 and 9, show the socioeconomic factors, food and health practices, early stimulation and productive aspects associated with stunting.
Table 1 Socio-economic factors associated with stunting
| Factor |
X2: P-value |
Spearman’s Correlation (r) | P-value of r |
| Children <30 months of age | 0,048 | -0,274 | 0,050 |
| Mother without education or primary | 0,001 | 0,454 | 0,001 |
| Absence of the father in the home | 0,017 | 0,332 | 0,016 |
| Not having own home | 0,003 | 0,413 | 0,002 |
| They use kerosene for cooking | 0,045 | 0,278 | 0,046 |
| They use gas for cooking | 0,000 | 0,530 | 0,000 |
| Mothers do not participate in social support | 0,032 | 0,297 | 0,032 |
| Weekly family income <50 dollars | 0,000 | 0,503 | 0,000 |
| Weekly food expenditure <31 dollars | 0,000 | 0,648 | 0,000 |
| Spending per capita / day in food. <.1.10 dollars | 0,000 | 0,591 | 0,000 |
| Food expenditure <65% of income | 0,008 | 0,370 | 0,007 |
P <0,05 demonstrates significant association and correlation
r = Spearman’s correlation
Table 2 Food practices, and health and early stimulation factors associated with stunting
| Factor | X2: P-value | Spearman’s Correlation (r) | P-value of r |
| Do not drink breast milk | 0,040 | 0,284 | 0,041 |
| Eating food before 6 months of age | 0,003 | 0,410 | 0,003 |
| Not having had exclusive breastfeeding | 0,042 | 0,290 | 0,043 |
| Low quinoa consumption frequency | 0,003 | 0,423 | 0,002 |
| Low frequency of maca consumption | 0,010 | 0,366 | 0,010 |
| Low frequency of red meat consumption | 0,008 | 0,382 | 0,007 |
| Low frequency of guinea pig consumption | 0,015 | 0,347 | 0,014 |
| Low frequency of fish consumption | 0,003 | 0,421 | 0,003 |
| Presence of childhood anemia | 0,003 | 0,407 | 0,003 |
| Presence of global malnutrition | 0,008 | 0,366 | 0,008 |
| Not having all vaccines / age | 0,036 | 0,291 | 0,037 |
| Presence of diarrhea | 0,038 | 0,288 | 0,039 |
| Presence of acute respiratory infections | 0,038 | 0,287 | 0,039 |
| Child without health insurance | 0,036 | 0,291 | 0,037 |
| Unboiled water consumption | 0,036 | 0,291 | 0,037 |
| Excreta deposition in open field | 0,028 | 0,306 | 0,028 |
| Not having a cleanliness place | 0,035 | 0,292 | 0,035 |
| Mothers do not hands wash, before eating | 0,031 | 0,298 | 0,032 |
| Mother do not hands wash, after using the bathroom | 0,023 | 0,314 | 0,023 |
| Washing only with water, without soap | 0,038 | 0,288 | 0,039 |
| There is no adequate smoke vent in the kitchen | 0,000 | 0,491 | 0,000 |
| Mother speaks to the child | 0,037 | 0,289 | 0,038 |
| Mother tells stories to the child | 0,027 | 0,306 | 0,027 |
| Mother sings to the child | 0,043 | 0,281 | 0,044 |
| Mother cares for the child | 0,031 | 0,298 | 0,032 |
| Mother plays with the child | 0,031 | 0,298 | 0,032 |
| Father speaks to the child | 0,043 | 0,281 | 0,044 |
P <0.05 demonstrates significant association and correlation
r = Spearman’s correlation
Table 3 Productive factors associated with stunting
| Factor |
X2: P-valor |
Spearman’s Correlation (r) | P-value of r |
| Not have bio-farm | 0,028 | 0,304 | 0,028 |
| Do not grow board beans | 0,005 | 0,430 | 0,004 |
| Do not raise guinea pigs | 0,035 | 0,298 | 0,036 |
P <0.05 demonstrates significant association and correlation
r = Spearman’s correlation
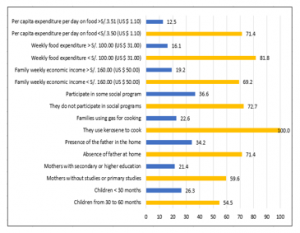
Figure 4. Stunting by socioeconomic variables (%)
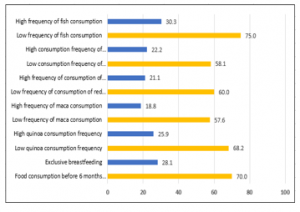
Figure 5. Stunting by food practices (%)
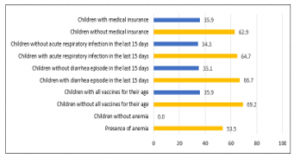
Figure 6. Stunting by health variables (%)
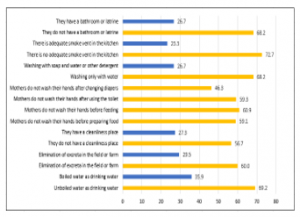
Figure 7. Stunting by health practices (%)
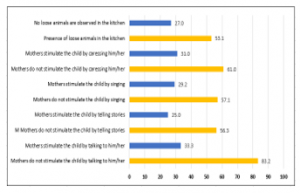
Figure 8. Stunting by development stimulation (%)
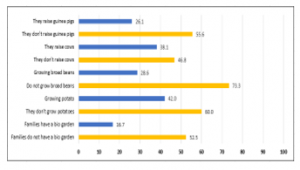
Figure 9. Stunting by agro-food production (%)
4. Discussion
The results of the study are similar to the report of the baseline of the district of Janjaillo-Jauja and other districts of the central highlands of Peru [11], where families produce for self-consumption, the productive yield of nutrient-rich crops necessary for nutrition Healthy is very low [22]. Agricultural communities need to find innovative ways to increase the production and consumption of protective foods to meet their health needs. Similar results were observed in the districts of Pancán, Masma, Masma Chiche, Huamalí, Apata, Janjaillo, all from the province of Jauja [12], where the food production of families does not cover their food needs throughout the year and their diet is eminently energetic, being the Main food the potato.
44.2% of children have stunting and were inversely associated with maternal education, immediate consumption of colostrum, increased frequency of protein food consumption, adequate dietary practices, complete vaccination, and early stimulation, boiled water consumption, adequate elimination of excreta, adequate hygiene practices, receiving food support and for raising minor animals. Similarly, in a study carried out in communities in the province of Concepción, Junín, it is observed that agro-food production does not cover the family’s food needs, due to the use of inadequate agricultural technologies, with the consumption of eminently energetic diets prevailing; 36.9% of the children had stunting and report that it had an inverse association with the maternal educational level, adequately constituted households, noble material of the walls of the house, drinking water consumption, higher frequency of potato consumption, broad beans, beans, guinea pig, viscera, egg, milk, green vegetables and citrus [1].
In Ricrán-Jauja (community adjacent to the study), the stunting prevalence in children under 5 years old was 49% and was associated with the possession of arable land, technological capacity, educational level and parental employment, food and care of health practices and some aspects related to environmental and sanitation conditions. Children of mothers with higher education do not present a risk of stunting or stunting; with a high stunting prevalence and severe stunting in children whose mothers had only primary or secondary education. In families not properly constituted, the stunting prevalence was higher. The highest prevalence of stunting was recorded in those that have a dirt floor and those that consume well water. The main agro-food variables inversely associated with the high stunting prevalence were the frequency of consumption of chicken meat, eggs, the possession of bio-vegetables with vegetables and the period of food storage, since they store, the stunting percentage for one year was lower compared to those that store for a short time and suffer from marked food insecurity [16].
In our study, the factors that are inversely related to the stunting prevalence are those directly linked to the availability, access, consumption and use of food; as possession of farmland, of bio-gardens and farms that partially cover food needs, under family production systems for self-consumption and sale.
Among the socio-economic factors that show an inverse association with stunting in children under 5 years old in Tunanmarca, there is the maternal educational level, hand washing practices at appropriate times because it reduces the prevalence of diarrheal diseases [23], having homes properly constituted, be homeowners and not depend on rent.
Among other factors associated with a better nutritional status of children in Tunanmarca is the consumption of breast milk, which protects them against the main causes of infant morbidity and mortality due to their contribution of immunological, nutritional and hormonal factors [24]; reducing the risk of enteric bacterial infections, mainly from Escherichia coli, which causes severe diarrhea with increased mortality in the newborn [25] and respiratory diseases such as pharyngitis, a disease that according to one study, it was reduced such as 40% in children who received exclusive breastfeeding [26].
This study recorded a lower prevalence of stunting when the house had adequate smoke vent; smoke exposure is strongly associated with acute respiratory infections in children under five years old [27], reporting that the burden of disease associated with solid fuel use is much more significant in communities with inadequate access to clean fuels, particularly in homes poor and rural areas of developing countries, where it constitutes 2.7% of health risks [28]. In our study, an association was also found between stunting and properly conserving the food produced, since the main factor involved in the origin and prevention of foodborne diseases is food hygiene, ensuring adequate hygiene and conservation [29].
A limitation of the study is the temporal bias that cross-sectional studies have; however, the research shows several strengths, such as the fact of studying several factors simultaneously and providing information that serves as a guide and basis for further studies and for decision-making in comprehensive nutritional interventions [18].
5. Conclusion
The stunting prevalence in children under 5 years old in the high Andean community of Tunanmarca, located in the central Andes of Peru was 44.2% and the factors that are directly associated with the prevalence of stunting were: Do not use gas for cooking, economic income weekly <50.00 dollars, weekly expenditure on family feeding <31.00 dollars, daily expenditure per capita on food <1.10 dolars, low maternal education level, no home ownership, consumption of food before 6 months of exclusive breastfeeding, low frequency of consumption of quinoa and fish, the presence of childhood anemia, inadequate venting of smoke in the kitchen, not having soap for hand washing and personal hygiene, and not having a bathroom.
Stunting is associated with various socioeconomic factors, availability and access to food and some food and health and hygiene practices.
These results demonstrate socio-economic and productive disparities for stunting in rural high Andean areas of central Peru, taking as a model the community of Tunanmarca in Jauja.
Acknowledgments
This study was funded by the Develop Special Fund for the Universidad Nacional del Centro del Perú.
To the mothers and their respective children who voluntarily participated in this study are thanked. To the authorities of the Tunanmarca district.
Conflict of interest
All the authors declare that there is no conflict of interests regarding the publication of this manuscript.
- Castro J, Chirinos D, Zenteno F, Situación agroalimentaria y estado nutricional infantil en comunidades de la provincia de Concepción, Junín-Perú. Libro de Resúmenes del XVIII CLN-SALN. 12-14,628. https://www.slaninternacional.org/congreso2018/avisos/libro-resumenes-congreso.php (2019).
- Tilman D, Clark M Global diets link environmental sustainability and human health. Nature 11/27; 515(7528), 518–522, 2014.
- Gómez MI, Barrett CB, Raney T et al Post-green revolution food systems and the triple burden of malnutrition. Food Policy 42, 129–138, 2013.
- Gross R, Schoeneberger H, Pfeifer H et al The Four Dimensions of Food and Nutrition Security: Definitions and Concepts. SCN News 2000 No.20 pp.20-25 ref.13. http://www.fao.org/elearning/course/fa/en/pdf/p-01_rg_concept.pdf (2019).
- Oenema S (2001) La Seguridad Alimentaria en los Hogares. FAO-RLC, Chile. http://www.fao.org/tempref/GI/Reserved/FTP_FaoRlc/old/prior/segalim/nutri/pdf/segalihog.pdf (2019).
- United Nations Transforming our world: the 2030 Agenda for Sustain Dev General Assembly Resolution 70/1, 25. September 2015. https://sustainabledevelopment.un.org/post2015/transformingourworld (accessed September 2019).
- Belahsen R Nutrition transition and food sustainability. Proc Nutr Soc. 2014, 385–8, 2014.
- Allen LN, Feigl AB Reframing non-communicable diseases as socially transmitted conditions. Lancet Glob Health. 2017;5, e644–6, 2017.
- Burchi F, De Muro P From food availability to nutritional capabilities: Advancing food security analysis. Food Policy 60, 10-19. DOI: https://doi.org/10.1016/j.foodpol.2015.03.008, 2016.
- Castro J, Chirinos D Impact of a Comprehensive Intervention on Food Security in Poor Families of Central Highlands of Peru. Food and Public Health 2015, 5(6), 213-219. doi: 10.5923/j.fph.20150506.02.
- Chirinos D Seguridad Alimentaria Nutricional en Poblaciones Vulnerables de la Región Central del Perú. Gráfica JOSIMPRESORES S.A.C. Huancayo, Perú. 270 pp 2015.
- Chirinos D, Castro J Situación agroalimentaria y desnutrición crónica en comunidades de la provincia de Jauja, Junín-Perú. Libro de Resúmenes del XVIII CLN-SALN. 12-14 noviembre 2018, 581-582. https://www.slaninternacional.org/congreso2018/avisos/libro-resumenes-congreso.php (2019).
- Gibson RS (2005) Principles of Nutritional Assessment. 2nd ed. Oxford University Press. 908 pp.
- Castro J, Chirinos D Z-Score Anthropometric Indicators Derived from NCHS-1977, CDC-2000 and WHO-2006 in Children Under 5 Years in Central Area of Peru. Universal Journal of Public Health 2(2), 73-81, 2014.
- Unicef Estado Mundial de la Infancia 2019 incluye a Perú entre las experiencias exitosas de lucha contra la desnutrición crónica infantil. https://www.unicef.org/peru/nota-de-prensa/estado-mundial-infancia-nutricion-alimentos-derechos-peru-experiencias-exitosas-desnutricion-cronica-infantil-reporte (2019).
- Castro J, Chirinos D, Zenteno F Relación entre la producción agroalimentaria y estado nutricional infantil en el distrito de Ricrán-Jauja. Instituto de Investigación de la Universidad Nacional del Centro del Perú, Huancayo 2013.
- DIRESA JUNIN Boletín estadístico de información de salud DIRESA JUNÍN-2017. Dirección Regional de Salud Junín (OITE-2017-RV: 1.0) 2017.
- Gross R, Kielmann A, Korte R et al Guidelines for Nutrition Baseline Surveys in Communities. The Southeast Asian Ministers of Education Organization and GTZ, Jakarta, Bangkok, Thailand, 28p 1997.
- WHO Child growth standards, WHO Anthro (version 3.2.2, 2011) and macros. World Health Organization. https://www.who.int/childgrowth/software/es/ (2019).
- Chirinos D, Castro J Comparison of NCHS-1977, CDC-2000 and WHO-2006 Nutritional Classification in 32 to 60-Month-old Children in the Central Higlansd of Peru. Universal Journal of Public Health 1(3), 143-149, 2013.
- Castro J, Chirinos D Prevalencia de anemia infantil y su asociación con factores socioeconómicos y productivos en una comunidad altoandina del Perú. Rev Esp Nutr Comunitaria, 25(3) 2019.
- Siegel KR, Ali MK, Srinivasiah A et al Do We Produce Enough Fruits and Vegetables to Meet Global Health Need. PLoS One, 9, Article e104059, 10.1371/joutnal.pone.0104059, 2014.
- Ejemot-Nwadiaro RI, Ehiri JE, Meremikwu MM et al. Hand washing for preventing diarrhoea. Cochrane Databaseof Systematic Reviews 2008 (1), Art. No: CD004265. doi: 10.1002/14651858.CD004265.pub2.
- González de Cosío-Martínez T, Hernández-Cordero S, Rivera-Dommarco J et al Recomendaciones para una política nacional de promoción de la lactancia materna en México: postura de la Academia Nacional de Medicina. Salud Pública de México, 59(1), 106-13, 2017.
- Manthey CF, Autran CA, Eckmann L et al. Human milk oligosaccharides protect against enteropathogenic Escherichia coli attachment in vitro and EPEC colonization in suckling mice. Journal Pediatric Gastroenterilogy Nutrition. 58(2), 165-8, 2014.
- Henkle E, Steinhoff M, Omer S et al. The Effect of Exclusive Breast-feeding on Respiratory Illness in Young Infants in a Maternal Immunization Trial in Bangladesh. Pediatric Infectious Disease Journal, 2(5), 431-5) 2013.
- Alvis N, De la Hoz F Contaminación del aire domiciliario y enfermedades respiratorias (infección respiratoria aguda baja, EPOC, cáncer de pulmón y asma) evidencias de asociación. Fac.Med. 56, 54-64, 2008.
- Bruce N, Perez-Padilla R, Albalak R Indoor air pollution in developing countries: a major environmental and public health challenge. Bulletin of the World Health Organization. 78, 1067-1071, 2008.
- Moreno MG, Alarcón A Higiene alimentaria para la prevención de trastornos digestivos infecciosos y por toxinas. Rev. Med. Clin. Condes, 21(5), 749-755, 2010.