Type 2 Diabetes Risk and Physical Activity in outpatients treated in Health Centers in a District of North Lima, 2020
Type 2 Diabetes Risk and Physical Activity in outpatients treated in Health Centers in a District of North Lima, 2020
Volume 5, Issue 6, Page No 1651-1656, 2020
Author’s Name: Deisy Chipana-Collahua1, Mariluz Chipana-Collahua1, Rosa Villegas-Ortiz1, Brian Meneses-Claudio2,a), Hernan Matta-Solis1
View Affiliations
1Faculty of Health Sciences, Universidad de Ciencias y Humanidades, 15314, Lima-Perú
2Image Processing Research Laboratory (INTI-Lab), Universidad de Ciencias y Humanidades, 15314, Lima-Perú
a)Author to whom correspondence should be addressed. E-mail: bmeneses@uch.edu.pe
Adv. Sci. Technol. Eng. Syst. J. 5(6), 1651-1656 (2020); ![]() DOI: 10.25046/aj0506196
DOI: 10.25046/aj0506196
Keywords: Diabetes risk, Lifestyle, Outpatients, Physical activity, Risk factors

Export Citations
Diabetes Mellitus Type 2 is a chronic disorder that affects the way the body metabolizes sugar (glucose) in the blood and depends on a combination of risk factors, such as genes and lifestyle. Although certain risk factors such as family history, age, or ethnicity cannot be changed, those related to diet, physical activity, and weight can be changed. These lifestyle changes can affect the probability of developing type 2 diabetes and its complications. In this research work, the prevention of the patient to develop type 2 diabetes with the option of leading a healthy lifestyle is proposed and reinforcing the population of each establishment with health education. It is a quantitative approach, a non-experimental, descriptive, and correlational study, with a population of 300 outpatients from a district of North Lima, who answered a questionnaire with sociodemographic data and the instruments of the level of physical activity IPAQ and risk of FINDRISK type 2 diabetes mellitus. In the results with respect to the level of physical activity, low 125 (41.7%) predominated and at risk of type 2 diabetes mellitus, 113 (27.7%) predominated. In conclusion, the population should be educated to have an adequate lifestyle by improving physical activity to prevent the risk of contracting diabetes.
Received: 31 August 2020, Accepted: 09 December 2020, Published Online: 25 December 2020
1. Introduction
Type 2 diabetes is currently considered one of the non-communicable diseases with the greatest negative impact and projection on the quality of life of the world population and represents a world health problem [1]; it is diagnosed in 85-95% of all those who suffer from it, with a higher percentage in less developed regions (one in 14 adults will have diabetes mellitus). It is estimated that nearly four million deaths a year are directly related to this condition, based on changes in the lifestyle of the population, associated with sedentary lifestyle, obesity, high blood pressure and other cardiovascular risk factors [2]. For these reasons, it is the fourth cause of death in the entire universe [3].
Globally, the number of patients diagnosed with type 2 diabetes mellitus has exceeded the references by more than 100% increase in the last 20 years [4]. In its development, it is related to lifestyle, age, sex, ethnicity/race and family history of Diabetes Mellitus Type 2 (DMT2) [5]. The Body Mass Index (BMI) increased means the probability of developing DMT2, to a greater extent in individuals with a Normal BMI compared to the obese, identified physical activity as a fundamental strategy in its prevention [6].
In Peru, the number of people with diabetes mellitus is increasing very rapidly and the main cause of its rapid increase is the important change in the lifestyle of the Peruvian population, whose current characteristics represent an excessive intake of high-calorie foods (junk food and sugary drinks), and what is equally worrisome: a reduction in physical activity that directly leads to a high morbidity of overweight and obesity [7].
Regular physical activity is essential for disease prevention, particularly chronic non-communicable diseases; Health promotion; quality of life; and reduction of mortality [8].
In [9], the study prevalence and incidence of type 2 diabetes mellitus in the general adult population of Peru, they define the prevalence of type 2 diabetes mellitus nationwide according to the National Survey of Nutritional, Biochemical, Socioeconomic and Cultural Indicators study was 5.1% in 2004-2005, and it increased to 7.0% in 2010-12, Perú Diabetes (PERUDIAB, national study). The Risk Factors of Non-communicable Diseases study in Lima and Callao reported a prevalence of 3.9% in 2006, and in 2010-2012 the Centre of Excellence in Chronic Diseases (CRONICAS) study also in Lima found this indicator at 5.5%. Regarding the incidence, three of the nine studies analyzed PERUDIAB estimated the incidence of diabetes in 19.5 new cases per 1,000 person-years. The CRONICAS study, in selected populations of Lima, Puno and Tumbes, found the same result. The Perú’s Rural to Urban Migrants (PERU MIGRANT) study estimated a 50% lower incidence than the previous two studies, although more than half of the population in this study lived in rural areas or were migrants from rural to urban areas.
In [10], the author studied physical activity in outpatients with diabetes mellitus type 2 concluded that 88% of diabetic patients had inactivity or minimal physical activity, estimating that patients with diabetes have a higher level of inactivity than the general population.
In [11], the author indicates that leading a healthy lifestyle pattern could lead to a lower risk of diabetes mellitus type 2, which identifies 142 associations related to the risk of developing DMT2. In which, they pointed out that Eleven associations (8%) presented evidence for the risk of DMT2 (low consumption of whole grains, metabolically healthy obesity, increased sedentary time). Thirty-four associations (24%) were associated with an increased risk of DMT2 and presented highly suggestive evidence, they were the following: high BMI, low educational level, gestational diabetes, increased consumption of processed meat, high level of total physical activity. Twenty-nine associations had suggestive evidence (20%), and 42 associations had weak evidence (30%) of DMT2 risk. All but six associations with convincing or highly suggestive evidence were based exclusively on prospective cohort studies.
The main objective of the study is to determine the risk of developing diabetes mellitus type 2 in relation to its level of physical activity in adults treated in health centers in a district of North Lima. It is important the need to modify the lifestyles of the population, associated with sedentary lifestyle, obesity, high blood pressure and other cardiovascular risk factors and thus identify physical activity as a fundamental strategy in its prevention.
Diabetes mellitus risk is understood as the probability of presenting or suffering from type 2 diabetes in adults attended in District-Rímac health centers, which can be evaluated by the presence of indicators such as age, body mass index, anthropometry waist, physical activity, consumption of vegetables or fruits, blood pressure medication, diagnosis of high glucose values and a history of diabetes mellitus [12].
The technique to be used in the research work will be the survey, which a significant amount of data will be obtained optimally and effectively. To measure the risk of type 2 diabetes mellitus, the data collection instrument will be used, the Finnish Diabetes Risk Score (FINDRISK) test that considers eight items grouped into eight dimensions and the level of physical activity will also be evaluated using the International Physical Activity Questionnaire (IPAQ), which considers 27 items grouped into three dimensions.
The data collection process will be carried out during the month of June through surveys, after the data will initially be entered into a data matrix designed in the Microsoft Excel 2013 program, then will be exported to the IBM SPSS Statistics version 24.0 program. It will apply descriptive statistical tests such as absolute frequencies, relative frequencies, and measures of central tendency, determining the risk of developing diabetes and the level of physical activity.
The following research work is structured as follows: In section II, the methodology that will determine the research work will be presented, with emphasis on the instrument, techniques to be used, scope of the study, valid inclusion, and exclusion criteria for the estimated population, among others. In section III, the results will show the tables and graphs obtained after data processing with an emphasis on determining the risk of developing type 2 diabetes mellitus and the level of physical activity of the studied population. In section IV, it will present the discussions of the research work and finally in section V, the conclusions obtained through the present research work, as well as the future work that leads to the timely detection of type 2 diabetes mellitus and the adoption of healthy styles.
2. Methods
The steps to carry out the survey as the population and sample were obtained, type of study, inclusion and exclusion criteria, analysis of the variables, data collection, location and application of the IPAQ and Finnish Diabetes Risk Score (FINDRISK) instruments. The paper before its application went through an ethics committee in which it was approved.
2.1. Population and Sample
It was applied to 300 outpatients at risk of developing diabetes, in the nine Health Centers of the Rimac district, considering the total distribution of patients who participated in the study, the sample corresponds to 35 participants from each center: H.C. Rímac, H.C. Caquetá and H.C. Flor de Amancaes. Likewise, 34 participants from Leoncio Prado, San Juan de Amancaes, Mariscal Castilla, Ciudad y Campo and Villa Los Ángeles.
2.2. Inclusion and Exclusion Criteria
Inclusion criterion is that all patients who receive regular care and wish to collaborate voluntarily in being evaluated to obtain a risk diagnosis participate and exclusion criteria; Patients who did not wish to participate in the study are excluded.
2.3. Type of study
The present work, due to its data collection characteristics and the measurement of the variables, has a quantitative approach, a non-experimental, descriptive and correlational study.
2.4. Analysis of the variables
The present study presents a main variable that is the risk of diabetes, the data collection instrument was used, the FINDRISK test that comprises eight items grouped into eight dimensions and also can be evaluated through the presence of indicators such as age, body mass index, anthropometry of the waist, physical activity, consumption of vegetables or fruits, medication for blood pressure, diagnosis of high glucose values and a history of diabetes mellitus [13].
The level of physical activity will be evaluated using the IPAQ questionnaire. The short version evaluates three specific characteristics of activity: intensity (mild, moderate or vigorous), frequency (measured in days per week) and duration (time per day). Activity of moderate intensity is considered as which produces a moderate increase in respiration, heart rate and sweating for at least 10 continuous minutes, and vigorous activity, such as which produces a greater increase in the same variables, for 10 minutes or more [14].
2.5. Instruments
The data collection technique was the survey and the selected instruments were the FINDRISK test and the short version IPAQ questionnaire to measure the level of physical activity.
The data collection process will be carried out during the month of June through the surveys, later the data will be initially entered into a data matrix designed in the Microsoft Excel 2013 program, and then they will be exported to the IBM SPSS Statistics version 24.0 program. And the data analysis will apply descriptive statistical tests such as absolute frequencies, relative frequencies and measures of central tendency, determining the risk of developing diabetes and the level of physical activity.
The instrument was applied in the nine establishments of the Rímac district. The respective permission was requested from Directorate of Integrated Health Networks (DIRIS) Lima Norte, to have access to health centers, for this purpose an enrollment was made in the ethics committee to approve the instrument to apply; After approval, it was presented to the head of each establishment and permission was given to the triage health personnel in charge of the area to develop the questionnaire.

Figure 1: The patient is triage taking anthropometric measurements, before going to the external office to be evaluated
As shown in Figure 1, the instructions on how to carry out the respective filling in of the questionnaires are explained to the patients, they were informed to mark a single alternative in the questions avoiding smearing, and the patients were also consulted to ask before any doubt that they would not understand, to obtain real data.
Figure 2 considers the distribution according to sex of the total number of people who participated in the study, segmented by each health center in the Rímac district, an analysis that considers 35 HC respondents: Rímac, Caquetá and Flor de Amancaes; the second block considers the HC with 34 respondents: Leoncio Prado, San Juan de Amancaes, Mariscal Castilla, Ciudad y Campo and Villa Los Angeles; and finally the block of 25 respondents the HC Piedra Liza, an activity that was carried out according to schedule and considered the minimum established quota.

Figure 2: Filling out the survey of outpatients treated in the health center of a district of North Lima – 2019 (N = 300)
2.6. Developing the surveys
The patients were interested in reading the questionnaire; some patients were hesitant to answer because of their advanced age they did not understand the questions, they did not interpret it in the health field.
Based on good data collection in most of the patients with good attitude and with consent, they collaborated in the survey. In some patients, they did not give their consent because of the time or they had another meeting, the discomfort of the patient and/or relatives when waiting for care was also observed, so they arrived before the mentioned time and were not treated, since that this has an impact on answering the survey.
It is important in the data collection, the technical staff of the triage service since their function is to take the anthropometric measurements (weight, height) and the abdominal perimeter of all the patients before entering the medical office and thus be diagnosed and evaluated.
3. Result
After collecting the data, graphic tables were generated where it will synthesize the information and graphics so that the results obtained are easier to understand.
Table 1: Sociodemographic data on the risk of type 2 diabetes and physical activity in outpatients treated at health centers in a district of North Lima, 2019 (n=300)
| Sex of hospitalized patient | Frequency (f) | Percentage (%) |
| Female | 214 | 71.3 |
| Male | 86 | 28.7 |
| Health Center | Frequency (f) | Percentage (%) |
| CMI Rímac | 35 | 11.7 |
| Caquetá | 35 | 11.7 |
| Flor de Amancaes | 35 | 11.7 |
| Leoncio Prado | 34 | 11.3 |
| San Juan de Amancaes | 34 | 11.3 |
| Mariscal Castilla | 34 | 11.3 |
| Ciudad y Campo | 34 | 11.3 |
| Villa los Ángeles | 34 | 11.3 |
| Piedra Liza | 25 | 8.3 |
| Degree of Study | Frequency (f) | Percentage (%) |
| No studies | 2 | 0.7 |
| Primary Incomplete | 2 | 0.7 |
| Primary Complete | 4 | 1.3 |
| High School Incomplete | 18 | 6.0 |
| High School Complete | 91 | 30.3 |
| University study Incomplete | 41 | 13.7 |
| University study Complete | 142 | 47.3 |
| Marital Status | Frequency (f) | Percentage (%) |
| Single | 121 | 40.3 |
| Cohabitant | 87 | 29.0 |
| Married | 65 | 21.7 |
| Separated | 7 | 2.3 |
| Divorced | 6 | 2.0 |
| Widowed | 14 | 4.7 |
| Type of Family | Frequency (f) | Percentage (%) |
| Nuclear | 111 | 37.0 |
| Single parent | 36 | 12.0 |
| Extended | 71 | 23.7 |
| Expanded | 40 | 13.3 |
| Reconstituted | 7 | 2.3 |
| Equivalent | 9 | 3.0 |
| Single Person | 26 | 8.7 |
| Mental health disorder | Frequency (f) | Percentage (%) |
| Depression | 3 | 1.0 |
| Family violence | 3 | 1.0 |
| Not have | 294 | 98.0 |
Table 1 considers the socio-demographic data regarding the sex of the participants, most of the surveyed sample, equivalent to 71.3%, is female. There are nine health centers in North Lima that were part of the study, which between 34 and 35 patients (11.7% and 11.3% respectively) for each health center made up the study sample, except for Piedra Liza Center, which had 25 patients (8.3%). Likewise, the data of the surveyed sample (47.3%) has completed higher education, followed as a percentage of those with complete secondary education (30.3%). Regarding marital status, most respondents (40.3%) were “single”. In a similar way, 37% of the surveyed patients denied having a mental health disorder.
Figure 3 considers the history of diabetes, which the risk is considered considering direct affinity, in which 108 patients are observed, representing 36% have no history, that is, relatives with a diagnosis of diabetes, followed by 104 patients representing 34.7% consider that there is a history of diabetes (grandparents, aunt, uncle, cousin, brother) and lastly 88 patients representing 29.3% consider that there is a history of diabetes (parents, siblings, children), they consider the line Transmissible with higher prevalence.
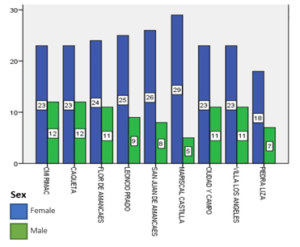
Figure 3: History of diabetes mellitus in outpatients attended in different health centers of a district of North Lima – 2019 (N = 300)
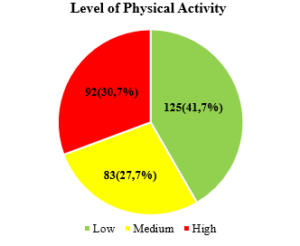
Figure 4: Patients surveyed who perform physical activity, cared for in the establishments of a District of North Lima – 2019 (n=300)
In Figure 4 regarding the level of physical activity, it is observed that 92 (30,7%) of the patients present a high level of physical activity, 83 (27,7%) a medium level of physical activity and 125 (41,7%) low level of physical activity.
In Figure 5 regarding the risk of type 2 diabetes mellitus, it is observed that 79 (26,3%) of the patients present a low risk, 113 (27,7%) present a slightly high risk, 46 (15,3%) present a moderate risk, 52 (17,3%) present a high risk and 10 (3,3%) of the patients present an extremely high risk.
Table 2: Relationship between the Risk of type 2 diabetes mellitus and Level of physical activity in outpatients attended in health centers of a district of North Lima, 2019 (n = 300) based on the Pearson’s Chi-square statistical test (X2)
| Level of physical activity | Total | |||||||
| Low | Moderate | High | ||||||
| Risk of type 2 diabetes mellitus | Low | Count | 30 | 27 | 22 | 79 | ||
| % of total | 10,0% | 9,0% | 7,3% | 26,3% | ||||
| Slightly high | Count | 55 | 28 | 30 | 113 | |||
| % of total | 18,3% | 9,3% | 10,0% | 37,7% | ||||
| Moderate | Count | 17 | 10 | 19 | 46 | |||
| % of total | 5,7% | 3,3% | 6,3% | 15,3% | ||||
| High | Count | 19 | 17 | 16 | 52 | |||
| % of total | 6,3% | 5,7% | 5,3% | 17,3% | ||||
| Very High | Count | 4 | 1 | 5 | 10 | |||
| % of total | 1,3% | 0,3% | 1,7% | 3,3% | ||||
| Total | Count | 125 | 83 | 92 | 300 | |||
| % of total | 41,7% | 27,7% | 30,7% | 100,0% | ||||
| Chi-square tests |
Value |
gl |
Sig. (p) |
|||||
| 9,653 | 8 | 0,290 | ||||||
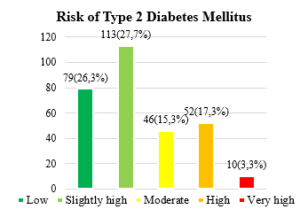
Figure 5: Risk of type 2 diabetes mellitus in patients treated in establishments in a District of North Lima – 2019 (n = 300)
Table 2 shows the relationship between risk of type 2 diabetes mellitus and level of physical activity in outpatients treated in health centers in a district of North Lima, where the significance value of the chi-square test is of 0,290 (p> 0.05) (X2 = 9,653; g.l. = 8), therefore, there is insufficient evidence to deny the dissociation hypothesis. Given the above, it is concluded that there is no significant relationship between the risk of type 2 diabetes and physical activity in outpatients in health facilities in a district of northern Lima, 2019 with a confidence level of 0,05 (95%).
The importance of obtaining data allows us to identify the relationship between physical activity and the risk of T2DM and which factors are risk factors, which we can carry out prevention strategies that allow maintaining the well-being of the person, also serves for future research with studies that allow evaluating the relationship between physical activity and risk of T2DM in which they can look for the effectiveness of the strategies applied in this research work.
4. Discussion
For the present research work, the focus was given to the patient on their physical health, although we can affirm that the risk of having type 2 diabetes mellitus today is one of the problems in our country due to the sedentary lifestyle that people present due to physical inactivity.
In the results on the level of physical activity, the patients present a low level of physical activity 125 (41,7%), this is since the patients have an inappropriate lifestyle, where sedentary lifestyle is the first factor present when physical activities are not performed, therefore patients tend to have an increased risk of non-communicable diseases that can compromise their health throughout their lives. In [15], the author argues that sedentary lifestyle is a predisposing factor for metabolic diseases where long hours spent at a computer, being on the phone and the eating of fast-food foods that provides a high caloric index, that is not waste by not performing any physical activity, compromises the health of the person generating health problems.
In the risk results for T2DM, patients present a slight risk of having this disease 113 (27,7%), this is since the prevalence of morbidity for contracting T2DM is increasingly considered higher, because people nowadays they manage an inadequate lifestyle, a poor diet, diminished family activities, also family history, where the person who has a relative with this disease if it does not have an adequate lifestyle can develop the disease. Therefore, adopting prevention and control strategies will reduce the risk of contracting T2DM. In [16], the author argue that family history of diabetes risk tends to increase the degree of susceptibility to the disease and that it is not possible to modify it, but also changes in the lifestyle of the person as a preventive measure by modifying food consumption, increasing physical activity and reducing body weight, are actions that allow the person to increase the benefits in their own health, ensuring well-being and trying to maintain a healthy life. Likewise, in [17], they argue that the self-care that patients with diabetes mellitus should exercise in themselves is important because it is related to the actions that each person take for their own benefit of their health including physical activity, proper nutrition, and self-control.
5. Conclusion
It is concluded that the population should be educated about the importance of increasing physical activity and of a healthy lifestyle where the well-being of health in the person is balanced.
It is concluded that nutritional counseling should be provided when making home visits to patients with diabetes mellitus.
It is concluded that the strengthening and control of prevention programs in primary care related to chronic diseases, including type 2 diabetes mellitus, should be considered.
It is concluded that preventive actions should be taken in the patient with diabetes mellitus such as a healthy lifestyle, a diet program that suits the patient and physical activity.
The main limitations in this research is the understanding that patients had about filling out the surveys, also, the time they had to fill out the surveys was also limited because the patients were waiting to be attended in the health centers and some did not want to fill out the survey; most of the patients voluntarily agreed to participate in the research work to find out if they had any risk of contracting T2DM.
Conflict of Interest
The authors declare no conflict of interest.
- A. Olokoba, O. Obateru, L. Olokoba, “Type 2 diabetes mellitus: A review of current trends.,” Oman Medical Journal, 27(4), 269–273, 2012, doi:10.5001/omj.2012.68.
- M. Mazidi, P. Toth, M. Banach, “C-reactive Protein Is Associated With Prevalence of the Metabolic Syndrome, Hypertension, and Diabetes Mellitus in US Adults.,” Angiology, 69(5), 438–442, 2018, doi:10.1177/0003319717729288.
- L. Slater, S. Stuckey, R. Chandra, “Tratamiento actual de la diabetes mellitus tipo 2.,” Neuroimaging Pharmacopoeia, 20(1), 289–292, 2016, doi:10.1007/978-3-319-12715-6_40.
- A. Koopman, J. Beulens, E. Voerman, P. Simone, A. Heijden, T. McDonald, M. Langendoen, F. Rutters, “The association between GAD65 antibody levels and incident Type 2 Diabetes Mellitus in an adult population: A meta-analysis.,” Metabolism: Clinical and Experimental, 95, 1–7, 2019, doi:10.1016/j.metabol.2019.03.001.
- A. Sharma, L. Sikora, S. Bush, “Management of Diabetes Mellitus in Adults at the End of Life: A Review of Recent Literature and Guidelines.,” Journal of Palliative Medicine, 22(9), 1133–1138, 2019, doi:10.1089/jpm.2018.0614.
- F. Petermann, X. Díaz, Á. Garrido, A. Leiva, M. Martínez, C. Salas, F. Poblete, C. Celis, “Association between type 2 diabetes and physical activity in individuals with family history of diabetes.,” Gaceta Sanitaria, 32(3), 230–235, 2018, doi:10.1016/j.gaceta.2017.09.008.
- A. Pinilla, M. Barrera, “Prevención en diabetes mellitus y riesgo cardiovascular: enfoque médico y nutricional.,” Revista Facultad de Medicina, 66(3), 459–468, 2018, doi:10.15446/revfacmed.v66n3.60060.
- S. Seclén, “Diabetes Mellitus en el Perú: hacia dónde vamos.,” Revista Medica Herediana, 26, 3–4, 2015, doi:10.20453/rmh.2015.2340.
- R. Carrillo, A. Bernabé, “DIABETES MELLITUS TIPO 2 EN PERÚ: UNA REVISIÓN SISTEMÁTICA SOBRE LA PREVALENCIA E INCIDENCIA EN POBLACIÓN GENERAL.,” Rev. Perú Med. Exp. Salud Publica, 36(1), 26–36, 2019, doi:10.17843/rpmesp.2019.361.4027.26.
- A. Manzaneda, M. Lazo, G. Málaga, “Physical activity in outpatients with type 2 diabetes in a national hospital of Perú.,” Rev. Perú Med. Exp. Salud Pública, 32(2), 311–315, 2015.
- V. Bellou, L. Belbais, L. Tzoulaki, E. Evangelou, “Risk factors for type 2 diabetes mellitus: An exposure-wide umbrella review of meta-analyses.,” PLoS ONE, 13(3), 1–27, 2018.
- Å. Bjørn, K. Midthjell, S. Krokstad, V. Rangul, A. Bauman, “Prolonged sitting may increase diabetes risk in physically inactive individuals: an 11 year follow-up of the HUNT Study, Norway.,” Diabetologia, 60(5), 830–835, 2017, doi:10.1007/s00125-016-4193-z.
- I. Mendiola, I. Urbina, A. Muñoz, G. Juanico, G. López, “Evaluación del desempeño del Finnish Diabetes Risk Score (findrisc) como prueba de tamizaje para diabetes mellitus tipo 2.,” Atención Familiar, 25(1), 22–26, 2017, doi:10.22201/facmed.14058871p.2018.1.62925.
- R. Barrera, “Cuestionario Internacional de actividad física (IPAQ),” Revista Enfermería Del Trabajo, 7(2), 49–54, 2017.
- B. Pérez, “Salud: entre la actividad física y el sedentarismo.,” An Venez Nutr, 27(1), 119–128, 2014.
- Y. Llorente, P. Soca, D. Rivas, Y. Borrego, “Factores de riesgo asociados con la aparición de diabetes mellitus tipo 2 en personas adultas.,” Revista Cubana de Endocrinología, 27(2), 123–133, 2016.
- M. Soler, E. Pérez, M. López, D. Quezada, “Conocimientos y autocuidado en pacientes con diabetes mellitus tipo 2.,” Archivo Médico de Camagüey, 20(3), 244–252, 2016.