
Mnemonic Discrimination Performance in a Memory Clinic: A Pilot Study
Abstract
Background:
Mnemonic discrimination is the behavioral ability stemming from pattern separation, which is the neural process of establishing independent and non-overlapping new memories. Over the past two decades, its assessment in various populations has contributed to a better conceptual understanding of age-related memory decline.
Objective:
To assess the clinical relevance of mnemonic discrimination in the memory clinics setting.
Methods:
This retrospective study was performed in 90 patients with a Mini-Mental State Examination (MMSE)>18 who consulted our memory clinic for the first time. All patients were tested with the Mnemonic Similarity Task, a freely available computerized test. Global cognitive function, executive function, visuoconstructional abilities, and verbal and visual episodic memory were also collected, together with the diagnosis after the initial clinical assessment (subjective cognitive complaint [SCC], mild cognitive impairment [MCI], or mild dementia).
Results:
Mnemonic discrimination performance was correlated with global cognitive function, executive function, and visual and verbal episodic memory scores, independent of age. It discriminated patients with SCC from those with MCI (amnestic or non-amnestic) with moderate accuracy (AUC = 0.77-0.78), similar to MMSE and the Frontal Assessment Battery (AUC = 0.74-0.84). Mnemonic discrimination performance did not distinguish between amnestic and non-amnestic MCI and the variability of the measure was important within groups.
Conclusion:
Mnemonic discrimination performance involves many cognitive domains and discriminates between patients with SCC and MCI with performance equivalent to “paper-and-pencil” screening tests. Further dedicated prospective studies will determine whether this task is of interest beyond research purposes, as a diagnostic or screening tool in primary care.
INTRODUCTION
Early detection of Alzheimer’s disease (AD) and related pathologies is crucial for future therapeutic interventions, such as disease-modifying therapies specifically targeting prodromal AD. However, early AD diagnosis remains challenging in primary care because memory complaints can be associated with many non-neurological conditions. One of the first essential steps in the diagnosis of early typical AD consists of carrying out a complete neuropsychological assessment to confirm an amnestic syndrome of the hippocampal type [1, 2]. However, clinical expertise for such assessments is sometimes difficult to access for many patients, and evaluations are laborious. Therefore, screening tools for memory complaints would be particularly useful to identify patients most at risk of developing typical AD in memory clinics, and to reassure other patients.
A fundamental physiological role of the hippocampus is to allow the formation of new episodic memories as individual representations [3, 4]. We can define each memory as the sum of co-occurring relevant contextual elements, some of which are shared among distinct memories. In this conceptual model, the hippocampus orthogonalizes a set of details to encode similar information as non-overlapping new memories, to avoid interference between long-term memory and new sensory inputs. This computational role of the hippocampus is named pattern separation [5] and is associated mainly with the function of the dentate gyrus, a hippocampal subfield involved in processing information derived from the entorhinal cortex via the perforant pathway [6]. The role of the dentate gyrus in pattern separation has been established over the past two decades by behavioral, electrophysiological, gene knock-out, and specific subfields lesions experiments in rodents, as well as by functional MRI studies in humans [7–11]. Mnemonic discrimination is the behavioral phenomenon stemming from an individual’s ability to perform pattern separation.
Age-related memory decline is characterized by a shift in hippocampal network dynamics with lower pattern separation performance [12–16]. In older people, new sensory inputs that are similar (but not identical) to previous inputs will fail to induce new memories due to impaired discrimination and representational rigidity [13, 14, 16, 17]. This age-related disability to discriminate among similar experiences is exacerbated in AD, even at the prodromal stage (amnestic mild cognitive impairment, MCI) [14, 18–20]. Conceptually, evaluating mnemonic discrimination performance could help identify the initiation of an amnestic syndrome of the hippocampal type because the entorhinal cortex is among the earliest brain areas affected by typical AD pathology [21, 22]. In this vein, it has been proposed to test mnemonic discrimination performance as part of a cognitive composite score in clinical trials of anti-amyloid drugs in asymptomatic AD (A4 study) [23].
Interestingly, mnemonic discrimination performance can be assessed quickly with freely available computerized tests, such as the Mnemonic Similarity Task (also known as Behavioral Pattern Separation Task) [7, 11, 19]. This task is easy, requiring very little supervision, can be performed rapidly (∼13 min), and the results are provided automatically by a computer. Therefore, the Mnemonic Similarity Task appears suitable for screening in primary care or at the first visit in memory clinics. Although there are differences in performance in this task between healthy older people and select patients with amnestic MCI or AD dementia [14, 18–20], this task has not been evaluated in unselected patients consulting in memory clinics. This study was performed to compare the performance of the Mnemonic Similarity Task with that of neuropsychological tests typically performed in memory clinics and to assess the ability of the Mnemonic Similarity Task to discriminate patients with a final diagnosis of subjective cognitive complaints (SCC), amnestic MCI, non-amnestic MCI, or mild AD dementia at the first visit.
MATERIALS AND METHODS
Participants, neuropsychological, and clinical assessments
Patients presenting to the Memory Clinic of Bordeaux University Hospital for their first neuropsychological and clinical assessment between 1 November 2021 and 31 April 2022 were included in this retrospective study. All patients with a memory complaint, complete available Mnemonic Similarity Test results (see below), and a Mini-Mental State Examination (MMSE) score > 18/30 were included in the analyses. Patients with decreased visual acuity based on history or neurological examination were excluded and participants were required to carry their glasses or contact lenses as normal. This study was performed in accordance with the Bordeaux University Hospital guidelines regarding retrospective studies of anonymized data and was authorized by the Direction de la Recherche Clinique et de l’Innovation, in accordance with the reference methodology (MR004).
As a routine procedure on the first visit to our memory clinic, patients were assessed using the MMSE and Montreal Cognitive Assessment (MoCA) for global cognitive function, Frontal Assessment Battery (FAB) for global executive function, Rey–Osterrieth Complex Figure (ROCF) for visuoconstructional abilities and visual memory (copy and immediate recall after 3 min), Free and Cued Selective Reminding test (FCSRT) for verbal episodic memory (total recall = free and cued recalls), Trail-Making test (TMT) A and B for attention, information processing speed, and executive function.
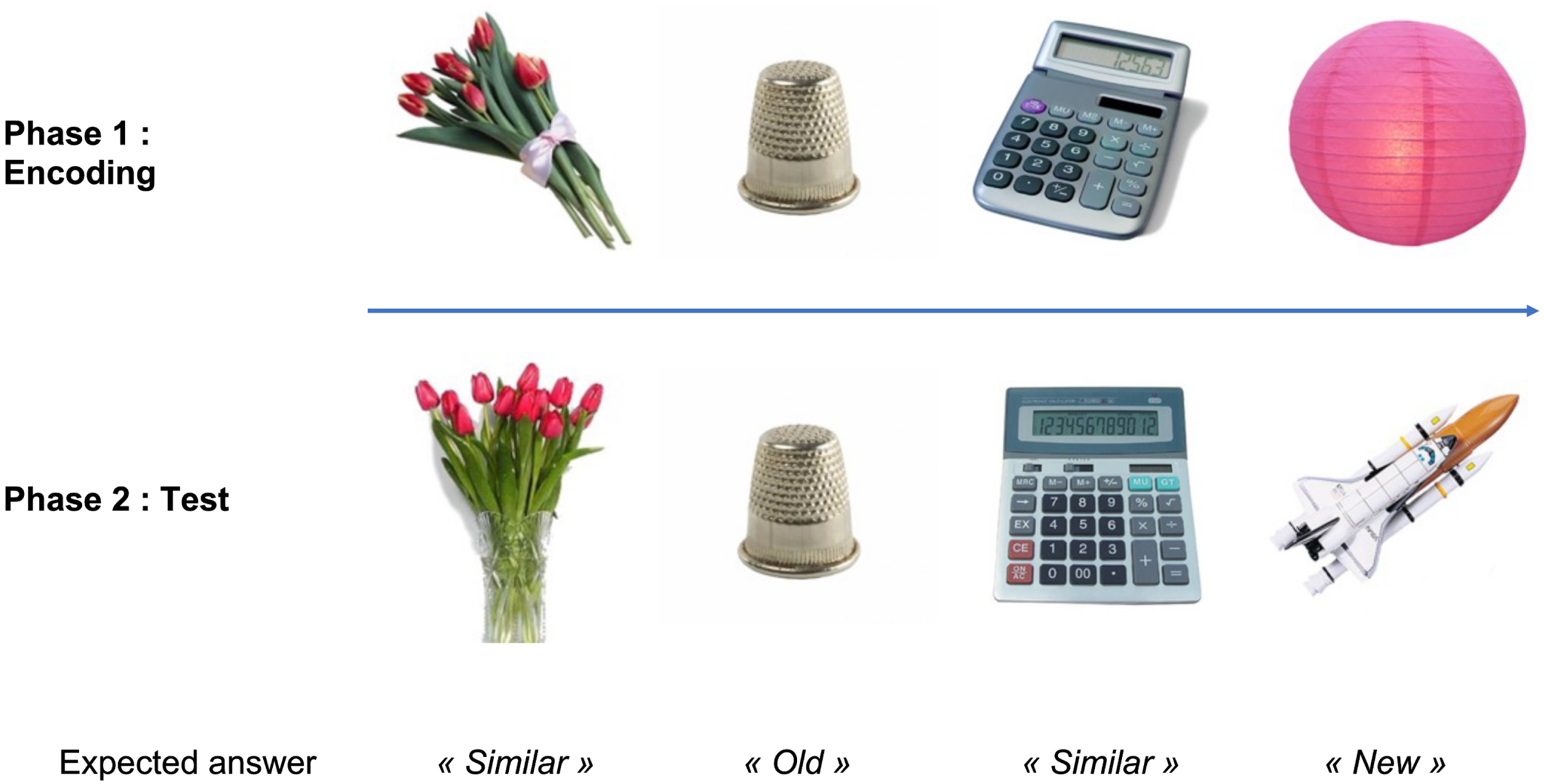
Fig. 1
Design of the Mnemonic Similarity Task (MST) and pictures examples. First, participants encode a set of pictures. In the second phase (surprise recognition memory test), participants should identify “old”, “new”, or “similar” objects as exactly the same pictures, novel foils, or lures related but not identical to previous pictures, respectively. Mnemonic discrimination performance is measured by the lure discrimination index: the rate of “similar” responses to the lure minus the rate of “similar” responses to the foils. (Pictures are from the MST, freely available at http://faculty.sites.uci.edu/starklab).
For each patient, the final stage diagnosis was made by an expert neurologist in accordance with the DSM-V [24] and Petersen criteria for MCI [25]. Age-appropriate normative scores were used for neuropsychological tests, except for the FCSRT for which we used the cut-off scores defining the amnestic syndrome of the hippocampal type [1]. Patients with a normal neuropsychological assessment, but who expressed a personal cognitive complaint that motivated their visit to the memory clinic, were classified as having SCC.
The Mnemonic Similarity Task
Mnemonic discrimination performance was assessed by the Mnemonic Similarity Test (BPS-O for Mac OS X, version 0.96, http://faculty.sites.uci.edu/starklab/mnemonicsimilarity-task-mst) [7, 26]. This computerized test consists of two phases. The first phase is an incidental encoding phase during which participants are presented with 128 pictures shown for 2 s with an interstimulus interval of 0.5 s. During this phase, participants must identify “indoor” and “outdoor” objects via a button press to maintain their attention. This encoding phase is followed immediately by an unexpected test phase during which participants are presented with 192 pictures with similar fixed exposition time (2 s) and interstimulus interval (0.5 s). One third of the pictures are exact repetitions of pictures shown in phase 1 (“targets”), one third are completely new objects (“foils”), and one third are similar but slightly different objects (“lures”). Participants are asked to identify “old”, “new” or “similar” pictures via a button press (Fig. 1).
Mnemonic discrimination performance was measured with the lure discrimination index, which was calculated as the rate of “similar” responses to the “lure” items minus the rate of “similar” responses to the “foils”, to correct for response bias. As an internal comparison for the task, we also measured the corrected recognition memory score, as the rate of “old” responses to the “target” items minus the rate of “old” responses to the “foils”.
Statistical analyses
Statistical analyses were performed using the XLstat 24.2.1 and Prism 9 software. Although the distribution of our neuropsychological data were predominantly Gaussian according to the Shapiro-Wilk normality test, we preferred to use nonparametric statistics given the small sample size of some of our subgroups. Quantitative data were thus represented as the median and range and qualitative data as percentages. Relationships between mnemonic discrimination performance and other neuropsychological scores were assessed using Spearman correlation coefficients. We used a Bonferroni-adjusted significance threshold of p < 0.0035 to adjust for multiple comparisons (n = 14). We also adjusted for age using appropriate regression models. Cognitive performances were compared among groups (patients with SCC, MCI or mild dementia) using the Kruskall-Wallis test followed by post-hoc Dunn’s multiple comparisons test. Receiver operating characteristic (ROC) analyses were performed to determine the cognitive scores that discriminated the patient groups. The optimal cutoffs in the ROC analyses were defined as the values maximizing the sum of sensitivity and specificity.
RESULTS
Demographic and clinical characteristics of patients
Ninety patients were included in our analyses. Among them, 33 were finally diagnosed with SCC, 21 with non-amnestic MCI (naMCI), 30 with amnestic MCI (aMCI) and 6 with mild dementia. The patients’ characteristics are summarized in Table 1.
Table 1
Demographic and clinical data for all patients and patients subgroups according to the final syndromic diagnosis. The lure discrimination index measures mnemonic discrimination performance. aMCI, amnestic mild cognitive impairment; naMCI, non-amnestic mild cognitive impairment; FAB, Frontal Assessment Battery; FCSRT, Free and Cued Selective Reminding Test, MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; ROCF, Rey–Osterrieth Complex Figure; SCC, subjective cognitive complaint; TMT, Trail Making Test
| Whole sample (n = 90) | SCC (n = 33) | NaMCI (n = 21) | AMCI (n = 30) | Mild dementia (n = 6) | |
| Gender (M/F, %) | 43.4 / 56.6 | 42.4 / 57.6 | 33.3 / 66.7 | 53.3 / 46.7 | 33.3 / 66.7 |
| Age (y) median [range] | 66.5 [42; 80] | 60 [42;78] | 71 [54;80] | 67 [49;76] | 70.5 [66; 74] |
| Education level (y) median [range] | 13 [5; 22] | 14 [9; 20] | 12 [9; 22] | 12 [5; 22] | 10 [5; 17] |
| FCSRT (total recall) median [range] | 45 [13; 48] | 47 [27; 48] | 45 [13; 48] | 36 [16; 48] | 41 [37; 44] |
| ROCF (copy) median [range] | 34 [4; 36] | 34 [24; 36] | 32 [4; 36] | 33 [5; 36] | 34 [26; 36] |
| ROCF (recall) median [range] | 15 [0; 30] | 19.5 [3.5; 30] | 17 [9.5; 25.5] | 10.5 [0; 27] | 4.25 [3; 5.5] |
| TMT-A s/correct move median [range] | 2.0 [0.7; 6.2] | 1.6 [0.7; 2.5] | 2.5 [1.3; 6.2] | 2.0 [1.1; 5.5] | 1.7 [0.9; 2.5] |
| TMT-B s/correct move median [range] | 4.2 [1.7; 14.4] | 3.1 [1.7; 9.7] | 5,5 [2,6; 14.4] | 4.1 [2.6; 12.6] | 6.1 [2.4; 9.9] |
| MoCA median [range] | 24 [19; 29] | 26 [22; 29] | 24 [19; 27] | 23 [19; 26] | 20 [20; 20] |
| MMSE median [range] | 26 [19; 30] | 29 [24; 30] | 26 [22; 29] | 25 [20; 29] | 21 [19; 26] |
| FAB median [range] | 15 [8; 18] | 18 [12; 18] | 14 [9; 18] | 15 [10; 17] | 11 [8; 11] |
| Lure discrimination Index median [range] | 5.5 [-18; 50] | 18 [-11; 50] | 0 [-9;43] | 2 [-18; 42] | 0 [-13; 15] |
| Recognition memory score median [range] | 67 [-47; 97] | 85 [23; 97] | 70 [2; 91] | 44 [-47; 84] | 14 [-17; 46] |
Associations between usual neuropsychological scores and mnemonic discrimination performance
Mnemonic discrimination performance was correlated with all neuropsychological test scores except the MoCA and the copy of the Rey–Osterrieth Complex Figure. The strongest correlation was found with TMT-B. While mnemonic discrimination performance was negatively correlated with age in our sample (r=-0.29, p = 0.0056), all correlations remained significant after adjustment for age (Table 2).
Table 2
Associations between neuropsychological tests and mnemonic discrimination performance, in the whole cohort and in the subgroup of patients with subjective cognitive complaint. Data represent the Spearman correlation coefficients (#significant correlation after Bonferroni correction for multiple comparisons, p < 0.0035) and in brackets the beta coefficients after adjustment for age in the regression models (*p < 0.05; **p < 0.01). The lure discrimination index measure mnemonic discrimination performance. FAB, Frontal Assessment Battery; FCSRT, Free and Cued Selective Reminding Test, MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; ROCF, Rey–Osterrieth Complex Figure; SCC, subjective cognitive complaint; TMT, Trail Making Test
| FCSRT (total recall) | ROCF (copy) | ROCF (recall) | TMT-A | TMT-B | MoCA | MMSE | FAB | |
| Lure discrimination Index (whole cohort, n = 90) | 0.38# (0.30**) | 0.09 (0.15) | 0.26 (0.27*) | -0.43# (-0.27*) | -0.48# (-0.30*) | 0.06 (0.009) | 0.45# (0.34**) | 0.44# (0.29*) |
| Lure discrimination Index (patients with SCC, n = 33) | 0.37# (0.16) | 0.11 (0.09) | 0.76# (0.73**) | -0.38 (-0.27) | -0.42# (-0.35) | -0.17 (-0.19) | 0.59# (0.52*) | 0.67# (0.66**) |
As a sensitivity analysis, we also tested the correlations in the subgroup of patients with SCC and obtained quite similar results (Table 2).
Association of mnemonic discrimination performance with the final diagnosis
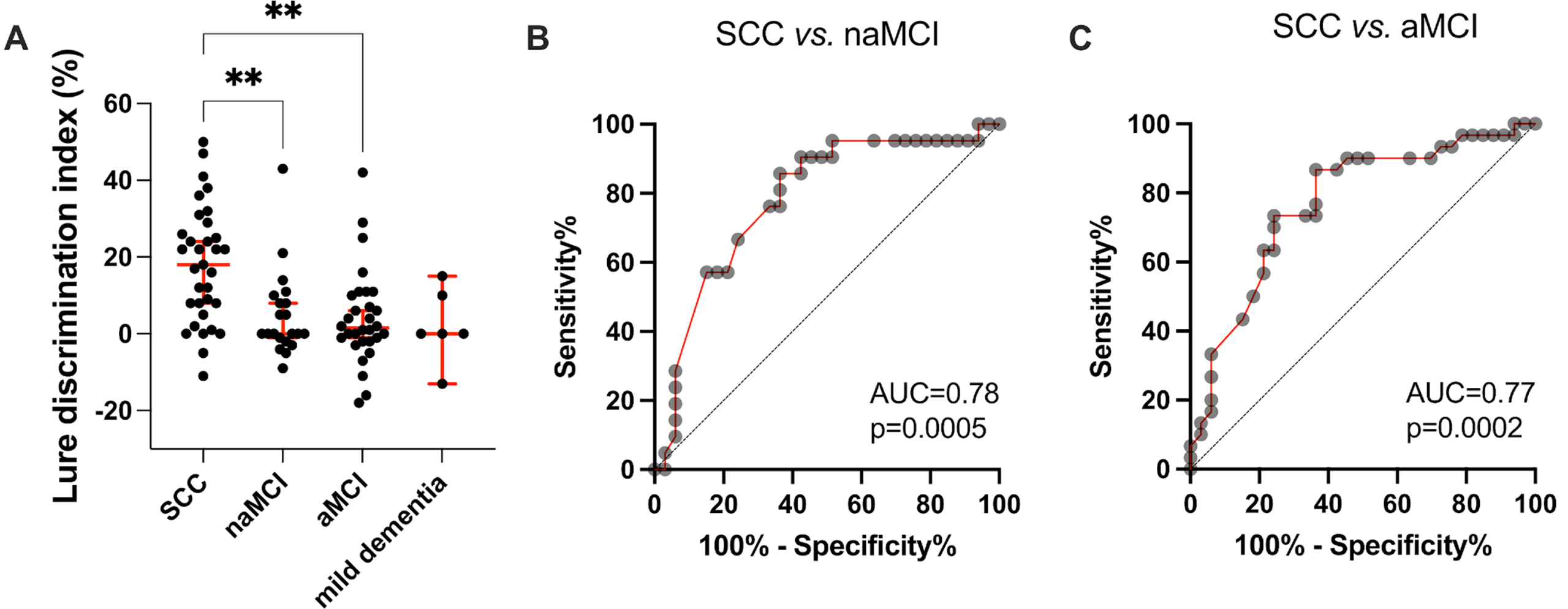
Mnemonic discrimination performance was significantly lower in patients with naMCI and aMCI compared to patients with SCC (median score = 18 [95% CI=8 to 24] in SCC patients versus 0 [95% CI=-1 to 8] and 2 [95% CI=-1 to 6] in naMCI and aMCI respectively, p < 0.01 for both comparisons). Patients with mild dementia (n = 6) had lower but not significantly different performance compared to SCC (median score = 0 [95% CI=-13 to 15] versus 18 [95% CI=8 to 24]; p = 0.11) (Fig. 2A). ROC analyses showed that the mnemonic discrimination performance significantly discriminated between SCC patients and naMCI or aMCI patients with moderate accuracy (Area Under the Curve [AUC] = 0.78, p = 0.0005 and AUC = 0.77, p = 0.0002 respectively, Fig. 2B, C). A lure discrimination index of 12 was considered an optimal cutoff to discriminate SCC from naMCI patients (86% sensitivity, 64% specificity) and from aMCI patients (87% sensitivity, 64% specificity).
Fig. 2
Association of mnemonic discrimination performance with final diagnoses. A) Lure discrimination index in patients according to their final diagnosis after full neuropsychological and clinical assessments. Each dot represents a single participant. The results are presented (in red) as the median±95% confidence interval. (**p<0.01, Dunn’s multiple comparison test). B, C) Receiver Operating Characteristic (ROC) curves analyses showing the ability of the lure discrimination index to discriminate among the final diagnoses (ROC analysis was performed only when the association in A was significant). aMCI, amnestic mild cognitive impairment; naMCI, non-amnestic mild cognitive impairment; AUC, area under the curve; SCC, subjective cognitive complaint.
In order to compare mnemonic discrimination performance to the standard “paper-and-pencil” screening tests used in primary care, we performed the same ROC analyses with MMSE and FAB scores. These tests also significantly discriminated between SCC and MCI patients with moderate to good accuracy (MMSE: AUC = 0.74, p = 0.0015 and AUC = 0.77, p = 0.0044 for SCC versus. naMCI and SCC versus aMCI respectively; FAB: AUC = 0.83, p = 0.0036 and AUC = 0.84, p = 0.0019 for SCC versus naMCI and SCC versus aMCI respectively).
DISCUSSION
In this study, we evaluated the clinical routine use of the Mnemonic Similarity Task. The results showed that mnemonic discrimination performance was correlated with global cognitive function (MMSE) and executive function (FAB). The strongest correlation was found with cognitive flexibility measured with the TMT-B, consistent with previous findings suggesting that the TMT-B score may explain much of the variance in mnemonic discrimination performance during aging [27]. Furthermore, the lure discrimination index was correlated with the total (free and cued) recall of FCSRT, a neuropsychological gold-standard to determine the amnestic syndrome of the hippocampal type [1] and to predict future AD dementia in elderly people [28]. It was also correlated with visual episodic memory, specifically correlating with the recall score of the Rey–Osterrieth Complex Figure, but not with the accuracy of the initial copy. The lack of correlation with the accuracy of the Rey–Osterrieth Complex Figure copy suggests there is no association between mnemonic discrimination and visuoconstructional abilities, while an association with visual perception was previously documented in older adults [29].
Our findings were consistent with previous studies using the Mnemonic Similarity Task. First, the lure discrimination index was correlated with age in our sample of patients, as usually described. Second, although collected in the context of a memory clinic, the mean lure discrimination index of participants with SCC (∼20%) was equivalent to those in previous studies in more selected experimental population of the same age (∼22% in 40-59 years old and ∼12% in 60-74). Third, patients with SCC had a better mnemonic discrimination performance than did patients with MCI and mild dementia, in whom mean lure discrimination index decreased to ∼0% [18, 19].
Mnemonic discrimination performance discriminated between SCC and MCI (amnestic or non-amnestic) patients with moderate to good accuracy (AUC = 0.76-0.86). Although the Mnemonic Similarity Task was designed to assess pattern separation, a neural function mediated by the entorhinal cortex and the hippocampus, it did not discriminate between aMCI and naMCI, probably because of the weight of executive functions (processing speed, inhibition and mental flexibility) in this test [27, 30]. Our results confirm the lack of specificity of the Mnemonic Similarity Task with respect to hippocampal function [31].
The Mnemonic Similarity Task is an easy-to-use, fast, and free test. We have shown here that it reflects the memory and executive impairments of patients consulting in memory clinics, and that the mnemonic discrimination performance had good sensitivity for discriminating SCC from MCI patients requiring further clinical investigation. Compared to the MMSE or the FAB, the Mnemonic Similarity Task use images as stimuli, which can be useful in cases of language impairment or if the patient does not speak the same language as the examiner. However, this task was designed for research purposes and not for clinical applications and it has many limitations. First, the variability in the measure, even in healthy subjects of the same age, is very important, and values largely overlap with those of patients with MCI or mild dementia. Therefore, the results can be challenging to interpret at the individual level. Second, to our knowledge, there is no normative value currently available and there have been no studies in the general population. Third, we showed that as a “screening” procedure, the lure discrimination index was not more accurate than MMSE or FAB in distinguishing patient with SCC or MCI.
The present pilot study had some limitations, including its retrospective nature and its small sample size. We acknowledge the lack of data concerning anxiety, depression and the characteristics and duration of cognitive complaint. Therefore, further studies involving prospectively collected data and larger cohorts both in the general population and in memory clinics are required to confirm our findings. Ideally, future longitudinal studies will also investigate whether mnemonic discrimination performance can predict the conversion from SCC to amnestic MCI, and from MCI to dementia. Indeed, the Mnemonic Similarity Task has been shown to be more sensitive than other widely used memory tests in detecting subtle memory changes which makes it worth investigating longitudinally in the context of subjective memory complaints [26]. Future studies may also use the recently optimized version of the Mnemonic Similarity Task [32], which is shorter and has shown a low impact of repeat-testing, which is of major interest in clinical practice.
In conclusion, we showed in this study that mnemonic discrimination performance involves many cognitive domains and is able to discriminate between patients with SCC and MCI at their first visit to a memory clinic but with performance equivalent to the usual “paper-and-pencil” screening tests. Mnemonic discrimination performance did not distinguish between amnestic and non-amnestic MCI and the variability of the measure was important within groups. It suggests that the Mnemonic Similarity Task provides little additional clinical information for assessment and/or screening of patients in the context of memory complaints and may be restricted to research purposes. Further dedicated prospective and longitudinal studies are required to complete and confirm these findings.
ACKNOWLEDGMENTS
The authors would like to thank the team of the Memory Clinic at Bordeaux University Hospital for their help in acquiring the data.
FUNDING
This work was supported by Bordeaux University Hospital.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
Anonymized data will be shared by request from any qualified investigator as long as data transfer is in agreement with EU legislation on the general data protection regulation.
REFERENCES
[1] | Sarazin M , Berr C , De Rotrou J , Fabrigoule C , Pasquier F , Legrain S , Michel B , Puel M , Volteau M , Touchon J , Verny M , Dubois B ((2007) ) Amnestic syndrome of the medial temporal type identifies prodromal AD: A longitudinal study. Neurology 69: , 1859–1867. |
[2] | Dubois B , Feldman HH , Jacova C , Cummings JL , Dekosky ST , Barberger-Gateau P , Delacourte A , Frisoni G , Fox NC , Galasko D , Gauthier S , Hampel H , Jicha GA , Meguro K , O’Brien J , Pasquier F , Robert P , Rossor M , Salloway S , Sarazin M , de Souza LC , Stern Y , Visser PJ , Scheltens P ((2010) ) Revising the definition of Alzheimer’s disease: A new lexicon. Lancet Neurol 9: , 1118–1127. |
[3] | Squire LR , Stark CEL , Clark RE ((2004) ) The medial temporal lobe. Annu Rev Neurosci 27: , 279–306. |
[4] | Milner B , Squire LR , Kandel ER ((1998) ) Cognitive neuroscience and the study of memory. Neuron 20: , 445–468. |
[5] | Yassa MA , Stark CEL ((2011) ) Pattern separation in the hippocampus. Trends Neurosci 34: , 515–525. |
[6] | Rolls ET ((2013) ) The mechanisms for pattern completion and pattern separation in the hippocampus. Front Syst Neurosci 7: , 74. |
[7] | Kirwan CB , Stark CEL ((2007) ) Overcoming interference: An fMRI investigation of pattern separation in the medial temporal lobe. Learn Mem Cold Spring Harb N 14: , 625–633. |
[8] | Leutgeb JK , Leutgeb S , Moser M-B , Moser EI ((2007) ) Pattern separation in the dentate gyrus and CA3 of the hippocampus. Science 315: , 961–966. |
[9] | Neunuebel JP , Knierim JJ ((2014) ) CA3 retrieves coherent representations from degraded input: Direct evidence for CA3 pattern completion and dentate gyrus pattern separation. Neuron 81: , 416–427. |
[10] | Bakker A , Kirwan CB , Miller M , Stark CEL ((2008) ) Pattern separation in the human hippocampal CA3 and dentate gyrus. Science 319: , 1640–1642. |
[11] | Lacy JW , Yassa MA , Stark SM , Muftuler LT , Stark CEL ((2011) ) Distinct pattern separation related transfer functions in human CA3/dentate and CA1 revealed using high-resolution fMRI and variable mnemonic similarity. Learn Mem 18: , 15–18. |
[12] | Maurer AP , Johnson SA , Hernandez AR , Reasor J , Cossio DM , Fertal KE , Mizell JM , Lubke KN , Clark BJ , Burke SN ((2017) ) Age-related changes in lateral entorhinal and CA3 neuron allocation predict poor performance on object discrimination. Front Syst Neurosci 11: , 49. |
[13] | Wilson IA , Gallagher M , Eichenbaum H , Tanila H ((2006) ) Neurocognitive aging: Prior memories hinder new hippocampal encoding. Trends Neurosci 29: , 662–670. |
[14] | Yassa MA , Lacy JW , Stark SM , Albert MS , Gallagher M , Stark CEL ((2011) ) Pattern separation deficits associated with increased hippocampal CA3 and dentate gyrus activity in nondemented older adults. Hippocampus 21: , 968–979. |
[15] | Gallagher M , Colantuoni C , Eichenbaum H , Haberman RP , Rapp PR , Tanila H , Wilson IA ((2006) ) Individual differences in neurocognitive aging of the medial temporal lobe. Age (Dordr) 28: , 221–233. |
[16] | Wilson IA , Ikonen S , Gallagher M , Eichenbaum H , Tanila H ((2005) ) Age-associated alterations of hippocampal place cells are subregion specific. J Neurosci 25: , 6877–6886. |
[17] | Wilson IA , Ikonen S , Gureviciene I , McMahan RW , Gallagher M , Eichenbaum H , Tanila H ((2004) ) Cognitive aging and the hippocampus: How old rats represent new environments. J Neurosci 24: , 3870–3878. |
[18] | Ally BA , Hussey EP , Ko PC , Molitor RJ ((2013) ) Pattern separation and pattern completion in Alzheimer’s disease: Evidence of rapid forgetting in amnestic mild cognitive impairment. Hippocampus 23: , 1246–1258. |
[19] | Stark SM , Yassa MA , Lacy JW , Stark CEL ((2013) ) A task to assess behavioral pattern separation (BPS) in humans: Data from healthy aging and mild cognitive impairment. Neuropsychologia 51: , 2442–2449. |
[20] | Toner CK , Pirogovsky E , Kirwan CB , Gilbert PE ((2009) ) Visual object pattern separation deficits in nondemented older adults. Learn Mem 16: , 338–342. |
[21] | Planche V , Bouteloup V , Mangin J-F , Dubois B , Delrieu J , Pasquier F , Blanc F , Paquet C , Hanon O , Gabelle A , Ceccaldi M , Annweiler C , Krolak-Salmon P , Habert M-O , Fischer C , Chupin M , Béjot Y , Godefroy O , Wallon D , Sauvée M , Bourdel-Marchasson I , Jalenques I , Tison F , Chêne G , Dufouil C , the MEMENTO Study group ((2021) ) Clinical relevance of brain atrophy subtypes categorization in memory clinics. Alzheimers Dement 17: , 641–652. |
[22] | Planche V , Manjon JV , Mansencal B , Lanuza E , Tourdias T , Catheline G , Coupé P ((2022) ) Structural progression of Alzheimer’s disease over decades: The MRI staging scheme. Brain Commun 4: , fcac109. |
[23] | Papp KV , Rentz DM , Maruff P , Sun C-K , Raman R , Donohue MC , Schembri A , Stark C , Yassa MA , Wessels AM , Yaari R , Holdridge KC , Aisen PS , Sperling RA ((2021) ) The Computerized Cognitive Composite (C3) in an Alzheimer’s Disease Secondary Prevention Trial. J Prev Alzheimers Dis 8: , 59–67. |
[24] | American Psychiatric Association ((2013) ) DSM-5: Diagnostic and statistical manual of mental disorders. American Psychiatric Association, Washington DC. |
[25] | Petersen RC ((2004) ) Mild cognitive impairment as a diagnostic entity. J Intern Med 256: , 183–194. |
[26] | Planche V , Ruet A , Charré-Morin J , Deloire M , Brochet B , Tourdias T ((2017) ) Pattern separation performance is decreased in patients with early multiple sclerosis. Brain Behav 7: , e00739. |
[27] | Gellersen HM , Trelle AN , Henson RN , Simons JS ((2021) ) Executive function and high ambiguity perceptual discrimination contribute to individual differences in mnemonic discrimination in older adults. Cognition 209: , 104556. |
[28] | Auriacombe S , Helmer C , Amieva H , Berr C , Dubois B , Dartigues J-F ((2010) ) Validity of the free and cued selective reminding test in predicting dementia: The 3C study. Neurology 74: , 1760–1767. |
[29] | Davidson PSR , Vidjen P , Trincao-Batra S , Collin CA ((2019) ) Older adults’ lure discrimination difficulties on the mnemonic similarity task are significantly correlated with their visual perception. J Gerontol B Psychol Sci Soc Sci 74: , 1298–1307. |
[30] | Foster CM , Giovanello KS ((2020) ) Domain general processes moderate age-related performance differences on the mnemonic similarity task. Memory 28: , 528–536. |
[31] | Pishdadian S , Hoang NV , Baker S , Moscovitch M , Rosenbaum RS ((2020) ) Not only memory: Investigating the sensitivity and specificity of the Mnemonic Similarity Task in older adults. Neuropsychologia 149: , 107670. |
[32] | Stark CEL , Noche JA , Ebersberger JR , Mayer L , Stark SM ((2023) ) Optimizing the mnemonic similarity task for efficient, widespread use. Front Behav Neurosci 17: , 1080366. |

