
Facing the Realities of Pragmatic Design Choices in Environmental Health Studies: Experiences from the Household Air Pollution Intervention Network Trial

 ,
,  , , , , , and
, , , , , and 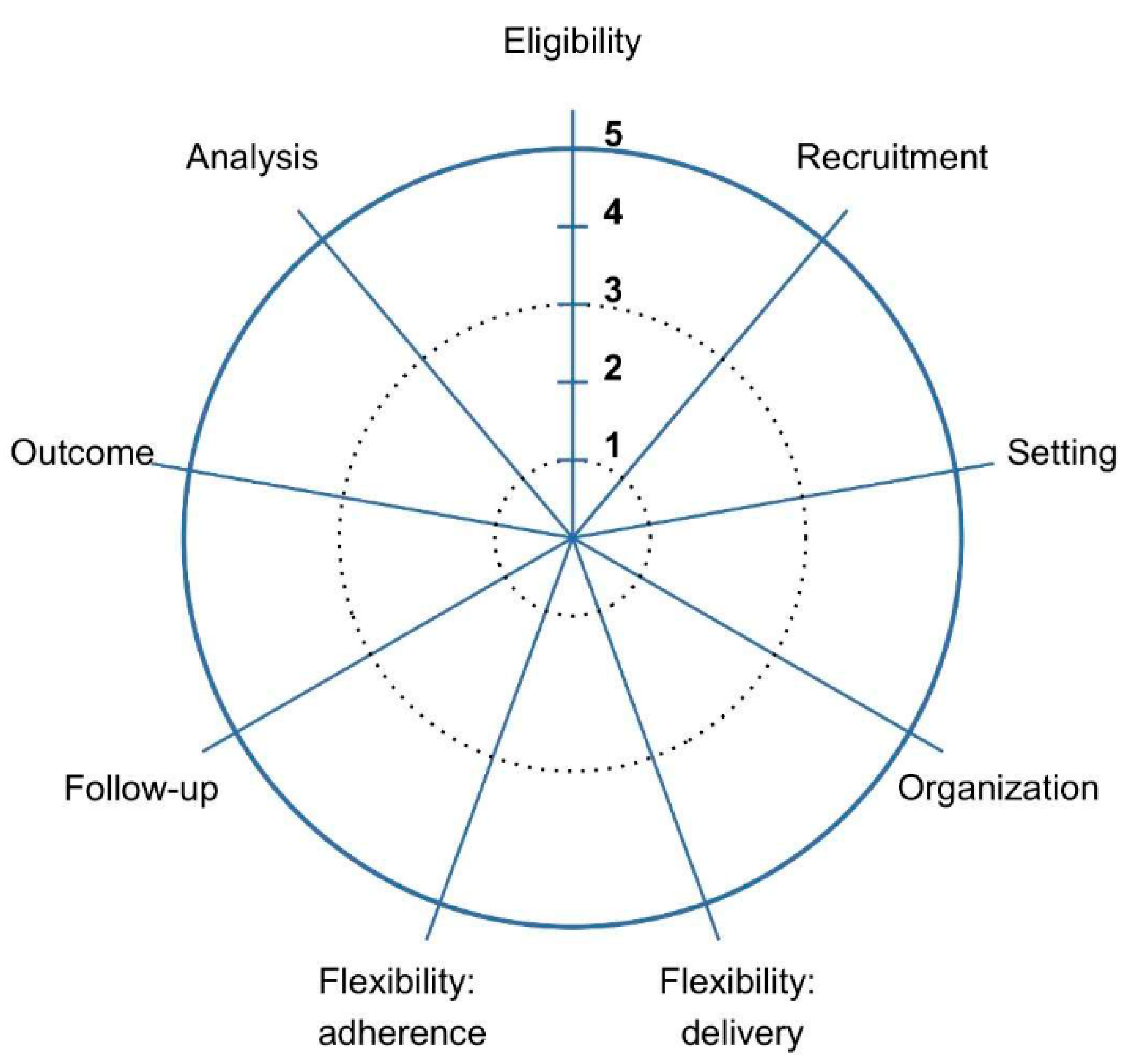{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Design
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
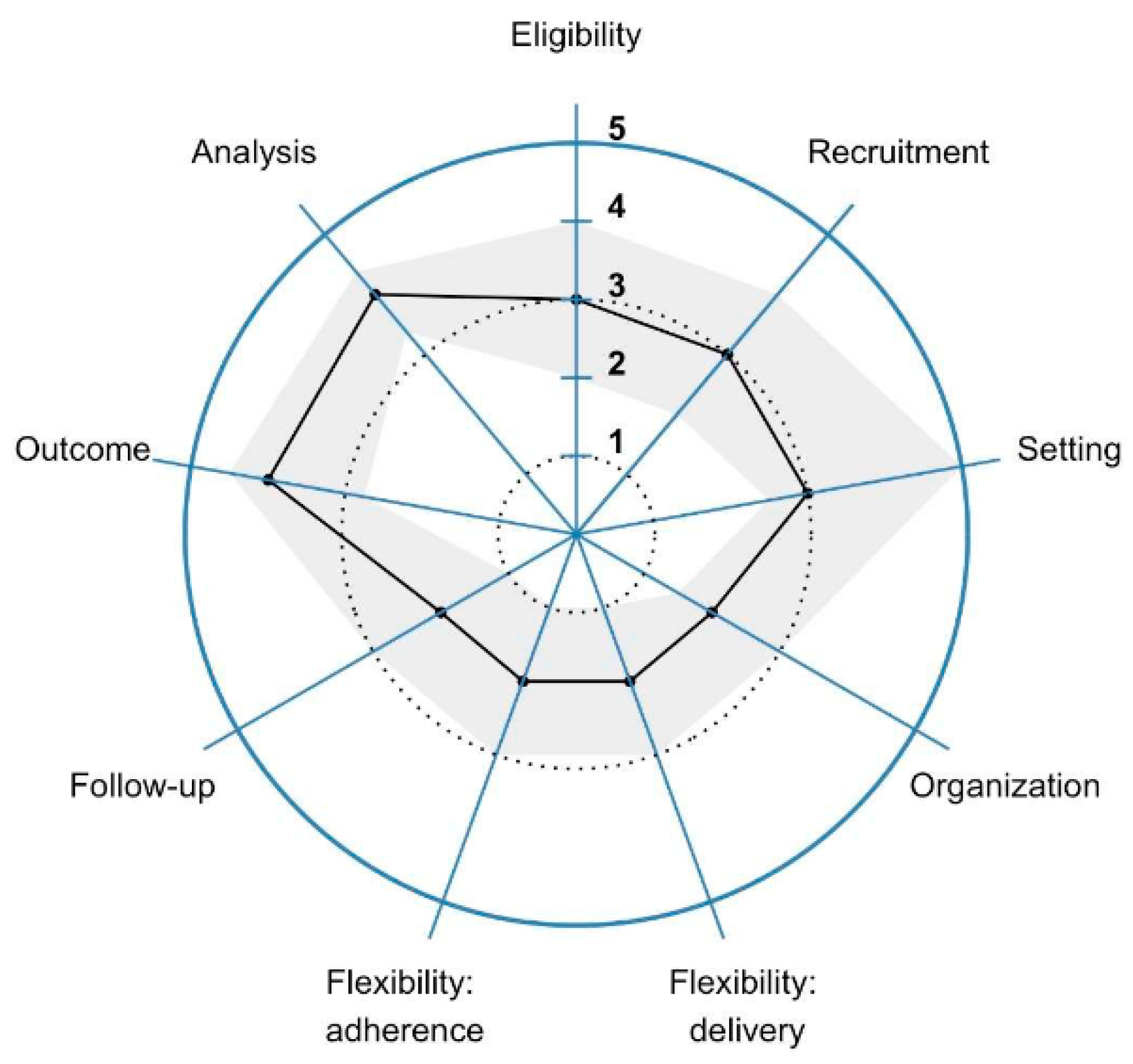
3.2. Ranking of the Nine PRECIS-2 Domains
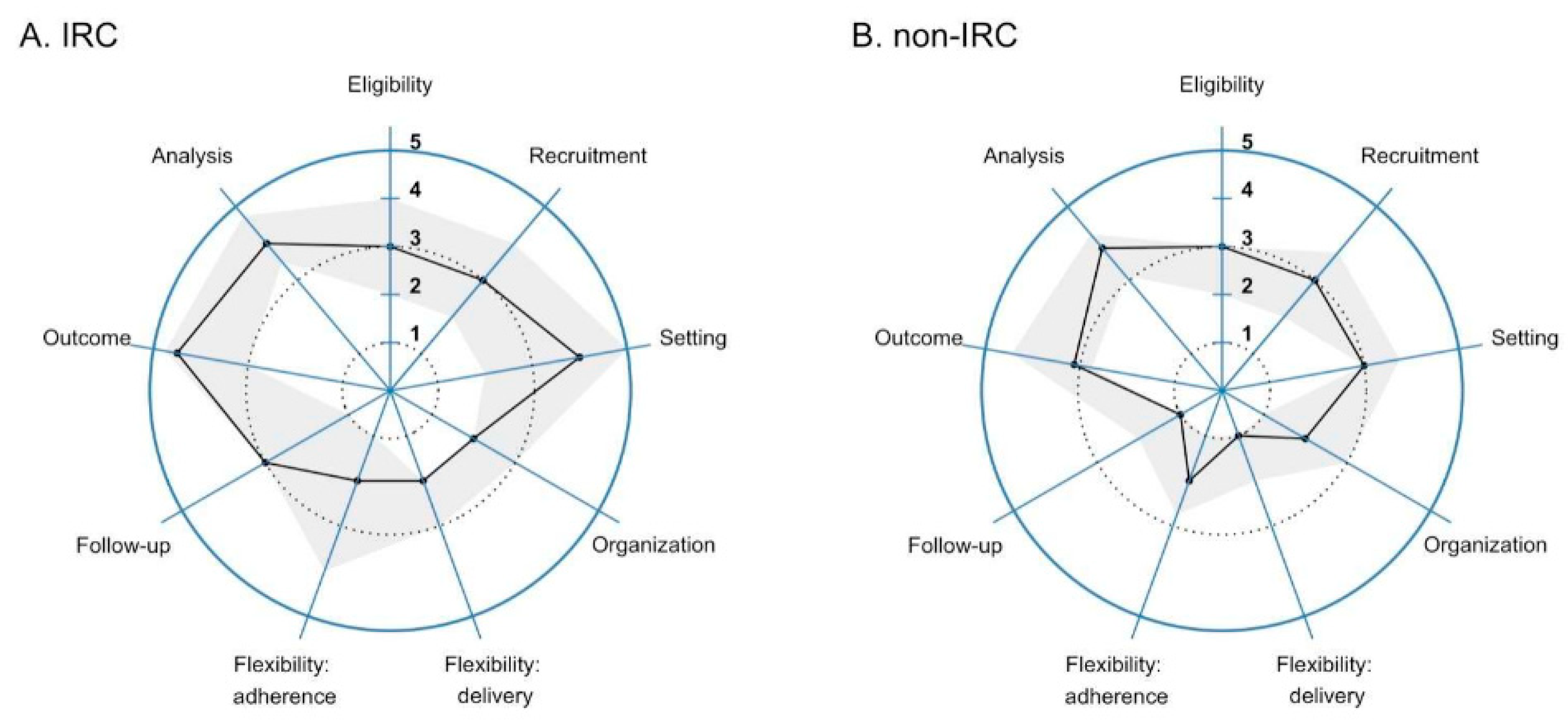
3.3. Ranking According to Where Investigators Worked
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harbour, R.; Miller, J. A new system for grading recommendations in evidence based guidelines. BMJ 2001, 323, 334–336. [Google Scholar] [CrossRef] [PubMed]
- Peel, J.L.; Baumgartner, J.; Wellenius, G.A.; Clark, M.L.; Smith, K.R. Are Randomized Trials Necessary to Advance Epidemiologic Research on Household Air Pollution? Curr. Epidemiol. Rep. 2015, 2, 263–270. [Google Scholar] [CrossRef]
- Allen, R.W.; Barn, P.K.; Lanphear, B.P. Randomized controlled trials in environmental health research: Unethical or underutilized? PLoS Med. 2015, 12, e1001775. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.R.; McCracken, J.P.; Weber, M.W.; Hubbard, A.; Jenny, A.; Thompson, L.M.; Balmes, J.; Diaz, A.; Arana, B.; Bruce, N. Effect of reduction in household air pollution on childhood pneumonia in Guatemala (RESPIRE): A randomised controlled trial. Lancet 2011, 378, 1717–1726. [Google Scholar] [CrossRef]
- Gupta, S.K. Intention-to-treat concept: A review. Perspect. Clin. Res. 2011, 2, 109–112. [Google Scholar] [CrossRef]
- Ranganathan, P.; Pramesh, C.S.; Aggarwal, R. Common pitfalls in statistical analysis: Intention-to-treat versus per-protocol analysis. Perspect. Clin. Res. 2016, 7, 144–146. [Google Scholar] [CrossRef]
- Kent, D.M.; Kitsios, G. Against pragmatism: On efficacy, effectiveness and the real world. Trials 2009, 10, 48. [Google Scholar] [CrossRef]
- Treweek, S.; Zwarenstein, M. Making trials matter: Pragmatic and explanatory trials and the problem of applicability. Trials 2009, 10, 37. [Google Scholar] [CrossRef]
- Loudon, K.; Treweek, S.; Sullivan, F.; Donnan, P.; Thorpe, K.E.; Zwarenstein, M. The PRECIS-2 tool: Designing trials that are fit for purpose. BMJ 2015, 350, 2147. [Google Scholar] [CrossRef]
- Clasen, T.; Checkley, W.; Peel, J.L.; Balakrishnan, K.; McCracken, J.P.; Rosa, G.; Thompson, L.M.; Barr, D.B.; Clark, M.L.; Johnson, M.A.; et al. Design and Rationale of the HAPIN Study: A Multicountry Randomized Controlled Trial to Assess the Effect of Liquefied Petroleum Gas Stove and Continuous Fuel Distribution. Environ. Health Perspect. 2020, 128, 47008. [Google Scholar] [CrossRef]
- Johnson, M.A.; Steenland, K.; Piedrahita, R.; Clark, M.L.; Pillarisetti, A.; Balakrishnan, K.; Peel, J.L.; Naeher, L.P.; Liao, J.; Wilson, D.; et al. Air Pollutant Exposure and Stove Use Assessment Methods for the Household Air Pollution Intervention Network (HAPIN) Trial. Environ. Health Perspect. 2020, 128, 47009. [Google Scholar] [CrossRef]
- Quinn, A.K.; Williams, K.N.; Thompson, L.M.; Harvey, S.A.; Piedrahita, R.; Wang, J.; Quinn, C.; Pillarisetti, A.; McCracken, J.P.; Rosenthal, J.P.; et al. Fidelity and Adherence to a Liquefied Petroleum Gas Stove and Fuel Intervention during Gestation: The Multi-Country Household Air Pollution Intervention Network (HAPIN) Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 12592. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.N.; Thompson, L.M.; Sakas, Z.; Hengstermann, M.; Quinn, A.; Díaz-Artiga, A.; Thangavel, G.; Puzzolo, E.; Rosa, G.; Balakrishnan, K.; et al. Designing a comprehensive behaviour change intervention to promote and monitor exclusive use of liquefied petroleum gas stoves for the Household Air Pollution Intervention Network (HAPIN) trial. BMJ Open 2020, 10, e037761. [Google Scholar] [CrossRef] [PubMed]
- Gong, M.N.; Schenk, L.; Gajic, O.; Mirhaji, P.; Sloan, J.; Dong, Y.; Festic, E.; Herasevich, V. Early intervention of patients at risk for acute respiratory failure and prolonged mechanical ventilation with a checklist aimed at the prevention of organ failure: Protocol for a pragmatic stepped-wedged cluster trial of PROOFCheck. BMJ Open 2016, 6, e011347. [Google Scholar] [CrossRef]
- Wang, H.E.; Prince, D.K.; Stephens, S.W.; Herren, H.; Daya, M.; Richmond, N.; Carlson, J.; Warden, C.; Colella, M.R.; Brienza, A.; et al. Design and implementation of the Resuscitation Outcomes Consortium Pragmatic Airway Resuscitation Trial (PART). Resuscitation 2016, 101, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Wildes, T.S.; Winter, A.C.; Maybrier, H.R.; Mickle, A.M.; Lenze, E.J.; Stark, S.; Lin, N.; Inouye, S.K.; Schmitt, E.M.; McKinnon, S.L.; et al. Protocol for the Electroencephalography Guidance of Anesthesia to Alleviate Geriatric Syndromes (ENGAGES) study: A pragmatic, randomised clinical trial. BMJ Open 2016, 6, e011505. [Google Scholar] [CrossRef] [PubMed]
- Levenson, J.C.; Rollman, B.L.; Ritterband, L.M.; Strollo, P.J.; Smith, K.J.; Yabes, J.G.; Moore, C.G.; Harvey, A.G.; Buysse, D.J. Hypertension with unsatisfactory sleep health (HUSH): Study protocol for a randomized controlled trial. Trials 2017, 18, 256. [Google Scholar] [CrossRef] [PubMed]
- Norman, G. Likert scales, levels of measurement and the “laws” of statistics. Adv. Health Sci. Educ. Theory Pract. 2010, 15, 625–632. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna. Available online: https://www.R-project.org/ (accessed on 7 November 2021).
- Goodman, D.; Crocker, M.E.; Pervaiz, F.; McCollum, E.D.; Steenland, K.; Simkovich, S.M.; Miele, C.H.; Hammitt, L.L.; Herrera, P.; Zar, H.J.; et al. Challenges in the diagnosis of paediatric pneumonia in intervention field trials: Recommendations from a pneumonia field trial working group. Lancet Respir. Med. 2019, 7, 1068–1083. [Google Scholar] [CrossRef]
- Crocker, M.E.; Hossen, S.; Goodman, D.; Simkovich, S.M.; Kirby, M.; Thompson, L.M.; Rosa, G.; Garg, S.S.; Thangavel, G.; McCollum, E.D.; et al. Effects of high altitude on respiratory rate and oxygen saturation reference values in healthy infants and children younger than 2 years in four countries: A cross-sectional study. Lancet Glob. Health 2020, 8, e362–e373. [Google Scholar] [CrossRef]
- Sambandam, S.; Mukhopadhyay, K.; Sendhil, S.; Ye, W.; Pillarisetti, A.; Thangavel, G.; Natesan, D.; Ramasamy, R.; Natarajan, A.; Aravindalochanan, V.; et al. Exposure contrasts associated with a liquefied petroleum gas (LPG) intervention at potential field sites for the multi-country household air pollution intervention network (HAPIN) trial in India: Results from pilot phase activities in rural Tamil Nadu. BMC Public Health 2020, 20, 1799. [Google Scholar] [CrossRef] [PubMed]
- Liao, J.; Kirby, M.A.; Pillarisetti, A.; Piedrahita, R.; Balakrishnan, K.; Sambandam, S.; Mukhopadhyay, K.; Ye, W.; Rosa, G.; Majorin, F.; et al. LPG stove and fuel intervention among pregnant women reduce fine particle air pollution exposures in three countries: Pilot results from the HAPIN trial. Environ. Pollut. 2021, 291, 118198. [Google Scholar] [CrossRef]
- Simkovich, S.M.; Underhill, L.J.; Kirby, M.A.; Crocker, M.E.; Goodman, D.; McCracken, J.P.; Thompson, L.M.; Diaz-Artiga, A.; Castañaza-Gonzalez, A.; Garg, S.S.; et al. Resources and Geographic Access to Care for Severe Pediatric Pneumonia in Four Resource-limited Settings. Am. J. Respir. Crit. Care Med. 2022, 205, 183–197. [Google Scholar] [CrossRef] [PubMed]
- Checkley, W.; Williams, K.N.; Kephart, J.L.; Fandiño-Del-Rio, M.; Steenland, N.K.; Gonzales, G.F.; Naeher, L.P.; Harvey, S.A.; Moulton, L.H.; Davila-Roman, V.G.; et al. Effects of a Household Air Pollution Intervention with Liquefied Petroleum Gas on Cardiopulmonary Outcomes in Peru. A Randomized Controlled Trial. Am. J. Respir. Crit. Care Med. 2021, 203, 1386–1397. [Google Scholar] [CrossRef] [PubMed]
- Dávila-Román, V.G.; Toenjes, A.K.; Meyers, R.M.; Lenzen, P.M.; Simkovich, S.M.; Herrera, P.; Fung, E.; Papageorghiou, A.T.; Craik, R.; McCracken, J.P.; et al. Ultrasound Core Laboratory for the Household Air Pollution Intervention Network Trial: Standardized Training and Image Management for Field Studies Using Portable Ultrasound in Fetal, Lung, and Vascular Evaluations. Ultrasound Med. Biol. 2021, 47, 1506–1513. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide: Global Update 2005; World Health Organization: Geneva, Switzerland, 2006; Available online: https://apps.who.int/iris/bitstream/handle/10665/69477/WHO_SDE_PHE_OEH_06.02_eng.pdf;jsessionid=85D78412EA2EF5886F9B58BEA3D2FE56?sequence=1 (accessed on 7 November 2021).
- Thompson, B.T.; Schoenfeld, D. Usual care as the control group in clinical trials of nonpharmacologic interventions. Proc. Am. Thorac. Soc. 2007, 4, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Smelt, A.F.; van der Weele, G.M.; Blom, J.W.; Gussekloo, J.; Assendelft, W.J. How usual is usual care in pragmatic intervention studies in primary care? An overview of recent trials. Br. J. Gen. Pract. 2010, 60, e305–e318. [Google Scholar] [CrossRef]
- Lipman, P.D.; Loudon, K.; Dluzak, L.; Moloney, R.; Messner, D.; Stoney, C.M. Framing the conversation: Use of PRECIS-2 ratings to advance understanding of pragmatic trial design domains. Trials 2017, 18, 532. [Google Scholar] [CrossRef]
- Loudon, K.; Zwarenstein, M.; Sullivan, F.M.; Donnan, P.T.; Gágyor, I.; Hobbelen, H.J.S.M.; Althabe, F.; Krishnan, J.A.; Treweek, S. The PRECIS-2 tool has good interrater reliability and modest discriminant validity. J. Clin. Epidemiol. 2017, 88, 113–121. [Google Scholar] [CrossRef]
- Zwarenstein, M.; Thorpe, K.; Treweek, S.; Loudon, K. PRECIS-2 for retrospective assessment of RCTs in systematic reviews. J. Clin. Epidemiol. 2020, 126, 202–206. [Google Scholar] [CrossRef]
- Schouten, B.; Cobben, F.; Bethlehem, J. Indicators for the representativeness of survey response. Surv. Methodol. 2009, 35, L101–L113. [Google Scholar]
- Rindfuss, R.R.; Choe, M.K.; Tsuya, N.O.; Bumpass, L.L.; Tamaki, E. Do Low Survey Response Rates Bias Results? Evidence from Japan. Demogr. Res. 2015, 32, 797–828. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Checkley, W.; Hossen, S.; Rosa, G.; Thompson, L.M.; McCracken, J.P.; Diaz-Artiga, A.; Balakrishnan, K.; Simkovich, S.M.; Underhill, L.J.; Nicolaou, L.; et al. Facing the Realities of Pragmatic Design Choices in Environmental Health Studies: Experiences from the Household Air Pollution Intervention Network Trial. Int. J. Environ. Res. Public Health 2022, 19, 3790. https://doi.org/10.3390/ijerph19073790
Checkley W, Hossen S, Rosa G, Thompson LM, McCracken JP, Diaz-Artiga A, Balakrishnan K, Simkovich SM, Underhill LJ, Nicolaou L, et al. Facing the Realities of Pragmatic Design Choices in Environmental Health Studies: Experiences from the Household Air Pollution Intervention Network Trial. International Journal of Environmental Research and Public Health. 2022; 19(7):3790. https://doi.org/10.3390/ijerph19073790
Chicago/Turabian StyleCheckley, William, Shakir Hossen, Ghislaine Rosa, Lisa M. Thompson, John P. McCracken, Anaite Diaz-Artiga, Kalpana Balakrishnan, Suzanne M. Simkovich, Lindsay J. Underhill, Laura Nicolaou, and et al. 2022. "Facing the Realities of Pragmatic Design Choices in Environmental Health Studies: Experiences from the Household Air Pollution Intervention Network Trial" International Journal of Environmental Research and Public Health 19, no. 7: 3790. https://doi.org/10.3390/ijerph19073790