
Factors Associated with Mental Health Outcomes in Hospital Workers during the COVID-19 Pandemic: A Mixed-Methods Study

 ,
,  , and
, and
Abstract
:1. Introduction
1.1. Mental Health in Healthcare Workers of COVID-19 Patients
1.2. Factors Associated with Mental Health in Healthcare Workers
1.3. Aims of the Investigation
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Participants
2.4. Procedures
2.5. Instruments
2.5.1. Perceived Stress
2.5.2. Depressive Symptoms
2.5.3. Anxiety Symptoms
2.5.4. Other Variables
2.6. Analysis
2.7. Qualitative Analysis
2.8. Ethics
3. Results
3.1. Quantitative Results
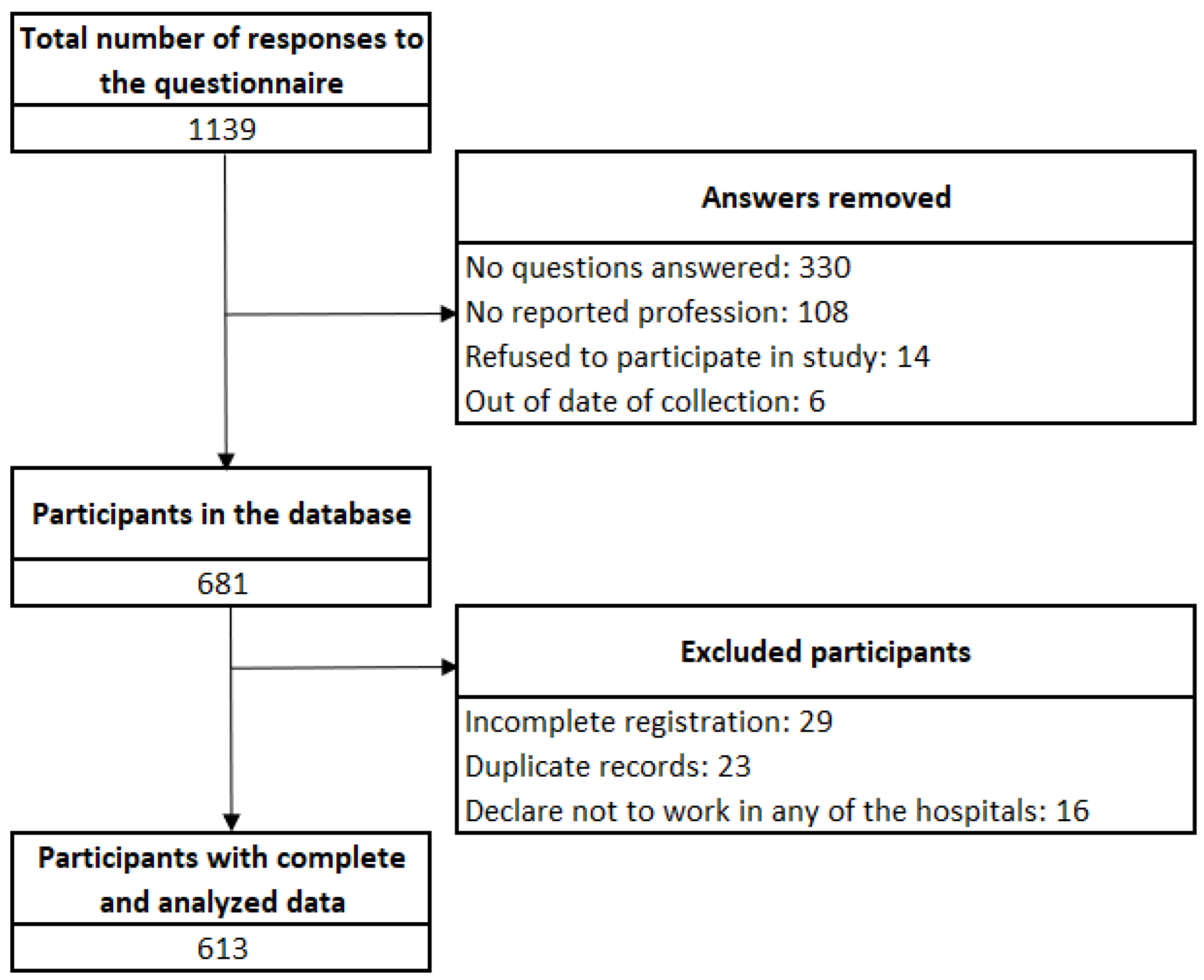
3.1.1. Participants
3.1.2. Bivariate Association
3.1.3. Regression Model
3.2. Qualitative Results
3.2.1. Emotional Distress Linked to Hospital Experiences of Suffering and Death
“It was shocking; it was really difficult to see 15 patients die every day. I don’t know if you have seen the rubbish packages in the streets, in black bags, that’s how the corpses were. Containers full. In truth it was like that in all [hospital] shifts.”(SR.03.09.10)
3.2.2. Fear of Contracting COVID-19
“I don’t really want to go to work. I’m scared, I’m scared, I pray all the time from here [hospital] to my house. I go praying and I say God please take care of me.”(AV.04.10.10)
“In those months that all this began [COVID-19 pandemic], in April, May, until June I felt terrible fear; and I think most of my colleagues too. It was a terror to come and work and when they told me “Yes, the patient you treated came out positive” we were terrified, we were in panic, I really did not know what to do.”(AV.05.10.10)
3.2.3. Modification of Life Routines
“Since I have restarted the work in July [2020], it is no longer the same. For example, I have to take a private mobility to go to work. Until now, I have not gotten on a bus because of the fear of getting infected.”(AV.01.07.10)
3.2.4. Exacerbation of Mental Disorders
“The change I feel is very marked… I feel affected with a depression that has become more and more profound. And the little tolerance for hospital work. So, I imagine that, like me, there are many colleagues, or many people close to the health system who have had this type of condition as well.”(SR.04.11.10)
“On a personal level, there is more anxiety, more fear, now for example I am medicated, I am on alprazolam at night because it was not my circadian rhythm to sleep every day at the same time.”(SR.03.11.10)
3.2.5. Physical Problems Associated with Emotional Distress
“At least in my case, I have anxiety attacks. At first, it started giving me like… episodes of sinus tachycardia and I went to the cardiologist. That had never happened to me, never in my life that had happened to me. The cardiologist did an ultrasound on me, did pertinent tests and everything and said: “You’re fine. I think you have to start regulating the work issue a bit, lower the intensity with what you do because that is affecting you.” And up to now I am still on medications.”(AV.03.10.10).
4. Discussion
4.1. Main Findings and Significance of the Results
4.2. Clinical Relevance
4.3. Limitations and Future Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hamid, S.; Mir, M.Y.; Rohela, G.K. Novel coronavirus disease (COVID-19): A pandemic (epidemiology, pathogenesis and potential therapeutics). New Microbes New Infect. 2020, 35, 100679. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease (COVID-19) Dashboard|WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/?gclid=CjwKCAiAqJn9BRB0EiwAJ1Sztem0DuIa_N2Ks2YpcEOGgyyvJIIuRLQTimQ0xkrfjR-OY0sfiF9l1BoC1sQQAvD_BwE (accessed on 1 April 2022).
- Gobierno del Perú. Sala Situacional COVID-19 Perú. Available online: https://covid19.minsa.gob.pe/sala_situacional.asp (accessed on 1 April 2022).
- Duan, L.; Zhu, G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 2020, 7, 300–302. [Google Scholar] [CrossRef]
- Zhou, X. Psychological crisis interventions in Sichuan Province during the 2019 novel coronavirus outbreak. Psychiatry Res. 2020, 286, 112895. [Google Scholar] [CrossRef] [PubMed]
- Kira, I.A.; Shuwiekh, H.A.M.; Ashby, J.S.; Elwakeel, S.A.; Alhuwailah, A.; Sous, M.S.F.; Baali, S.B.A.; Azdaou, C.; Oliemat, E.M.; Jamil, H.J. The Impact of COVID-19 Traumatic Stressors on Mental Health: Is COVID-19 a New Trauma Type. Int. J. Ment. Health Addict. 2021, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Bridgland, V.M.E.; Moeck, E.K.; Green, D.M.; Swain, T.L.; Nayda, D.M.; Matson, L.A.; Hutchison, N.P.; Takarangi, M.K.T. Why the COVID-19 pandemic is a traumatic stressor. PLoS ONE 2021, 16, e0240146. [Google Scholar] [CrossRef]
- Uphoff, E.P.; Lombardo, C.; Johnston, G.; Weeks, L.; Rodgers, M.; Dawson, S.; Seymour, C.; Kousoulis, A.A.; Churchill, R. Mental health among healthcare workers and other vulnerable groups during the COVID-19 pandemic and other coronavirus outbreaks: A rapid systematic review. PLoS ONE 2021, 16, e0254821. [Google Scholar] [CrossRef]
- Hamaideh, S.H.; Al-Modallal, H.; Tanash, M.; Hamdan-Mansour, A. Depression, anxiety and stress among undergraduate students during COVID-19 outbreak and “home-quarantine”. Nurs. Open 2022, 9, 1423–1431. [Google Scholar] [CrossRef]
- Antiporta, D.A.; Cutipé, Y.L.; Mendoza, M.; Celentano, D.D.; Stuart, E.A.; Bruni, A. Depressive symptoms among Peruvian adult residents amidst a National Lockdown during the COVID-19 pandemic. BMC Psychiatry 2021, 21, 111. [Google Scholar] [CrossRef]
- CISA Cyber Infrastructure. Guidance on the Essential Critical Infrastructure Workforce: Ensuring Community and National Resilience in COVID-19 Response. Available online: https://www.cisa.gov/sites/default/files/publications/Version_3.0_CISA_Guidance_on_Essential_Critical_Infrastructure_Workers_1.pdf (accessed on 10 January 2021).
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated with Mental Health Outcomes among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Kang, L.; Li, Y.; Hu, S.; Chen, M.; Yang, C.; Yang, B.X.; Wang, Y.; Hu, J.; Lai, J.; Ma, X.; et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. Lancet Psychiatry 2020, 7, e14. [Google Scholar] [CrossRef] [Green Version]
- Dutta, A.; Sharma, A.; Torres-Castro, R.; Pachori, H.; Mishra, S. Mental health outcomes among health-care workers dealing with COVID-19/severe acute respiratory syndrome coronavirus 2 pandemic: A systematic review and meta-analysis. Indian J. Psychiatry 2021, 63, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Nashwan, A.J.; Al-Fayyadh, S.; Al-Hadrawi, H.; Al-Jubouri, M.B.; Jaafar, S.A.; Hussein, S.M.; Nashwan, A.J.; Alharahsheh, M.A.; Kader, N.; Alabdulla, M. Development and Initial Validation of Stigma Towards Healthcare Providers Working with COVID-19 Patients Scale (S19-HCPs). J. Multidiscip. Healthc. 2021, 14, 3125–3134. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, S.P.; Rawal, N.; Shrestha, D.B.; Budhathoki, P.; Banmala, S.; Awal, S.; Bhandari, G.; Poudel, R.; Parajuli, A.R. Prevalence of Anxiety, Depression, and Perceived Stigma in Healthcare Workers in Nepal during Later Phase of First Wave of COVID-19 Pandemic: A Web-Based Cross-Sectional Survey. Cureus 2021, 13, e16037. [Google Scholar] [CrossRef] [PubMed]
- Gasparro, R.; Scandurra, C.; Maldonato, N.M.; Dolce, P.; Bochicchio, V.; Valletta, A.; Sammartino, G.; Sammartino, P.; Mariniello, M.; di Lauro, A.E.; et al. Perceived Job Insecurity and Depressive Symptoms among Italian Dentists: The Moderating Role of Fear of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 5338. [Google Scholar] [CrossRef] [PubMed]
- Khudaykulov, A.; Changjun, Z.; Obrenovic, B.; Godinic, D.; Alsharif, H.Z.H.; Jakhongirov, I. The fear of COVID-19 and job insecurity impact on depression and anxiety: An empirical study in China in the COVID-19 pandemic aftermath. Curr. Psychol. 2022, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Obrenovic, B.; Du, J.; Godinic, D.; Baslom, M.M.M.; Tsoy, D. The Threat of COVID-19 and Job Insecurity Impact on Depression and Anxiety: An Empirical Study in the USA. Front. Psychol. 2021, 12, 648572. [Google Scholar] [CrossRef]
- Rafi, M.A.; Mamun, M.A.; Hsan, K.; Hossain, M.; Gozal, D. Psychological Implications of Unemployment among Bangladesh Civil Service Job Seekers: A Pilot Study. Front. Psychiatry 2019, 10, 578. [Google Scholar] [CrossRef] [Green Version]
- Zafar, N.; Jamal, Z.; Mujeeb Khan, M. Preparedness of the Healthcare Personnel against the Coronavirus Disease 2019 (COVID-19) Outbreak: An Audit Cycle. Front. Public Health 2020, 8, 502. [Google Scholar] [CrossRef]
- The Lancet. The plight of essential workers during the COVID-19 pandemic. Lancet 2020, 395, 1587. [Google Scholar] [CrossRef]
- Ho, C.S.; Chee, C.Y.; Ho, R.C. Mental Health Strategies to Combat the Psychological Impact of COVID-19 Beyond Paranoia and Panic. Ann. Acad. Med. Singap. 2020, 49, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Abraham, A.; Chaabna, K.; Doraiswamy, S.; Bhagat, S.; Sheikh, J.; Mamtani, R.; Cheema, S. Depression among healthcare workers in the Eastern Mediterranean Region: A systematic review and meta-analysis. Hum. Resour. Health 2021, 19, 81. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.C.; Chen, P.F.; Lee, T.H.; Lin, C.C.; Chiang, K.T.; Tsai, M.F.; Kuo, H.F.; Lung, F.W. The Effect of Religion on Psychological Resilience in Healthcare Workers during the Coronavirus Disease 2019 Pandemic. Front. Psychol. 2021, 12, 628894. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Copeland, W.E.; McGinnis, E.; Bai, Y.; Adams, Z.; Nardone, H.; Devadanam, V.; Rettew, J.; Hudziak, J.J. Impact of COVID-19 Pandemic on College Student Mental Health and Wellness. J. Am. Acad. Child. Adolesc. Psychiatry 2021, 60, 134–141.e132. [Google Scholar] [CrossRef]
- Carter, S.M.; Shih, P.; Williams, J.; Degeling, C.; Mooney-Somers, J. Conducting Qualitative Research Online: Challenges and Solutions. Patient 2021, 14, 711–718. [Google Scholar] [CrossRef]
- Alcalde-Rabanal, J.E.; Lazo-González, O.; Nigenda, G. Sistema de salud de Perú. Salud Publica Méx 2011, 53, s243–s254. [Google Scholar]
- Centers for Disease Control and Prevention. Appendix 2. Terminology. Available online: https://www.cdc.gov/infectioncontrol/guidelines/healthcare-personnel/appendix/terminology.html (accessed on 10 January 2021).
- Campo-Arias, A.; Oviedo, H.C.; Herazo, E. Escala de Estrés Percibido-10: Desempeño psicométrico en estudiantes de medicina de Bucaramanga, Colombia. Rev. Fac. Med. 2014, 62, 1–24. [Google Scholar] [CrossRef]
- Seedhom, A.E.; Kamel, E.G.; Mohammed, E.S.; Raouf, N.R. Predictors of Perceived Stress among Medical and Nonmedical College Students, Minia, Egypt. Int. J. Prev. Med. 2019, 10, 107. [Google Scholar] [CrossRef]
- Manea, L.; Gilbody, S.; McMillan, D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): A meta-analysis. Can. Med. Assoc. J. 2012, 184, E191–E196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassiani-Miranda, C.A.; Vargas-Hernández, M.C.; Pérez-Aníbal, E.; Herazo-Bustos, M.I.; Hernández-Carrillo, M. Confiabilidad y dimensión del cuestionario de salud del paciente (PHQ-9) para la detección de síntomas de depresión en estudiantes de ciencias de la salud en Cartagena, 2014. Biomédica 2017, 37, 112–120. [Google Scholar] [PubMed] [Green Version]
- Saldivia, S.; Aslan, J.; Cova, F.; Vicente, B.; Inostroza, C.; Rincón, P. Propiedades psicométricas del PHQ-9 (Patient Health Questionnaire) en centros de atención primaria de Chile. Rev. Méd. Chile 2019, 147, 53–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villarreal-Zegarra, D.; Copez-Lonzoy, A.; Bernabe-Ortiz, A.; Melendez-Torres, G.J.; Bazo-Alvarez, J.C. Valid group comparisons can be made with the Patient Health Questionnaire (PHQ-9): A measurement invariance study across groups by demographic characteristics. PLoS ONE 2019, 14, e0221717. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- García-Campayo, J.; Zamorano, E.; Ruiz, M.A.; Pardo, A.; Pérez-Páramo, M.; López-Gómez, V.; Freire, O.; Rejas, J. Cultural adaptation into Spanish of the generalized anxiety disorder-7 (GAD-7) scale as a screening tool. Health Qual. Life Outcomes 2010, 8, 8. [Google Scholar] [CrossRef] [Green Version]
- Yáñez, J.A.; Afshar Jahanshahi, A.; Alvarez-Risco, A.; Li, J.; Zhang, S.X. Anxiety, Distress, and Turnover Intention of Healthcare Workers in Peru by Their Distance to the Epicenter during the COVID-19 Crisis. Am. J. Trop. Med. Hyg. 2020, 103, 1614–1620. [Google Scholar] [CrossRef]
- Huang, J.Z.; Han, M.F.; Luo, T.D.; Ren, A.K.; Zhou, X.P. Mental health survey of 230 medical staff in a tertiary infectious disease hospital for COVID-19. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 2020, 38, E001. [Google Scholar] [CrossRef]
- Riecher-Rössler, A. Sex and gender differences in mental disorders. Lancet Psychiatry 2017, 4, 8–9. [Google Scholar] [CrossRef]
- Jacob, L.; Haro, J.M.; Koyanagi, A. Relationship between living alone and common mental disorders in the 1993, 2000 and 2007 National Psychiatric Morbidity Surveys. PLoS ONE 2019, 14, e0215182. [Google Scholar] [CrossRef] [Green Version]
- Stahl, S.T.; Beach, S.R.; Musa, D.; Schulz, R. Living alone and depression: The modifying role of the perceived neighborhood environment. Aging Ment. Health 2017, 21, 1065–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revicki, D.A.; Whitley, T.W.; Gallery, M.E. Organizational characteristics, perceived work stress, and depression in emergency medicine residents. Behav. Med. 1993, 19, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Archer, L.R.; Keever, R.R.; Gordon, R.A.; Archer, R.P. The relationship between residents’ characteristics, their stress experiences, and their psychosocial adjustment at one medical school. Acad. Med. 1991, 66, 301–303. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.; Chen, J.H.; Xu, Y.F. Patients with mental health disorders in the COVID-19 epidemic. Lancet Psychiatry 2020, 7, e21. [Google Scholar] [CrossRef]
- Zandifar, A.; Badrfam, R.; Mohammadian Khonsari, N.; Mohammadi, M.R.; Asayesh, H.; Qorbani, M. Prevalence and Associated Factors of Posttraumatic Stress Symptoms and Stigma among Health Care Workers in Contact with COVID-19 Patients. Iran. J. Psychiatry 2020, 15, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Lee, E.H.; Park, N.R.; Choi, Y.H. Mental Health of Nurses Working at a Government-designated Hospital during a MERS-CoV Outbreak: A Cross-sectional Study. Arch. Psychiatr. Nurs. 2018, 32, 2–6. [Google Scholar] [CrossRef] [Green Version]
- Wilson, J.M.; Lee, J.; Fitzgerald, H.N.; Oosterhoff, B.; Sevi, B.; Shook, N.J. Job Insecurity and Financial Concern during the COVID-19 Pandemic Are Associated with Worse Mental Health. J. Occup. Env. Med. 2020, 62, 686–691. [Google Scholar] [CrossRef]
- Del Carmen, M. Peru Embarks on a Comprenhensive Approach to COVID-19. Available online: https://www.undp.org/content/undp/en/home/blog/2020/peru-embarks-on-a-comprehensive-approach-to-covid-19.html (accessed on 26 July 2020).
- Jimenez, M.M.; Bui, A.L.; Mantilla, E.; Miranda, J.J. Human resources for health in Peru: Recent trends (2007-2013) in the labour market for physicians, nurses and midwives. Hum. Resour. Health 2017, 15, 69. [Google Scholar] [CrossRef] [Green Version]
- Carrasco-Cortez, V. Los trabajadores de salud, los actores olvidados de las reformas. Acta. Méd. Peru. 2014, 31, 50–56. [Google Scholar]
- Blustein, D.L.; Duffy, R.; Ferreira, J.A.; Cohen-Scali, V.; Cinamon, R.G.; Allan, B.A. Unemployment in the time of COVID-19: A research agenda. J. Vocat. Behav. 2020, 119, 103436. [Google Scholar] [CrossRef]
- Liberati, E.; Richards, N.; Willars, J.; Scott, D.; Boydell, N.; Parker, J.; Pinfold, V.; Martin, G.; Dixon-Woods, M.; Jones, P.B. A qualitative study of experiences of NHS mental healthcare workers during the Covid-19 pandemic. BMC Psychiatry 2021, 21, 250. [Google Scholar] [CrossRef] [PubMed]
- Kotera, Y.; Ozaki, A.; Miyatake, H.; Tsunetoshi, C.; Nishikawa, Y.; Kosaka, M.; Tanimoto, T. Qualitative Investigation into the Mental Health of Healthcare Workers in Japan during the COVID-19 Pandemic. Int. J. Env. Res. Public Health 2022, 19, 568. [Google Scholar] [CrossRef] [PubMed]
- Koontalay, A.; Suksatan, W.; Prabsangob, K.; Sadang, J.M. Healthcare Workers’ Burdens During the COVID-19 Pandemic: A Qualitative Systematic Review. J. Multidiscip. Healthc. 2021, 14, 3015–3025. [Google Scholar] [CrossRef] [PubMed]
- Neto, M.L.R.; Almeida, H.G.; Esmeraldo, J.D.a.; Nobre, C.B.; Pinheiro, W.R.; de Oliveira, C.R.T.; Sousa, I.d.C.; Lima, O.M.M.L.; Lima, N.N.R.; Moreira, M.M.; et al. When health professionals look death in the eye: The mental health of professionals who deal daily with the 2019 coronavirus outbreak. Psychiatry Res. 2020, 288, 112972. [Google Scholar] [CrossRef]
- Barello, S.; Palamenghi, L.L.; Graffigna, G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. 2020, 290, 113129. [Google Scholar] [CrossRef]
- Villarreal-Zegarra, D.; Copez-Lonzoy, A.; Vilela-Estrada, A.L.; Huarcaya-Victoria, J. Depression, post-traumatic stress, anxiety, and fear of COVID-19 in the general population and health-care workers: Prevalence, relationship, and explicative model in Peru. BMC Psychiatry 2021, 21, 455. [Google Scholar] [CrossRef]
- Chan, M.F.; Al-Shekaili, M.; Al-Adawi, S.; Hassan, W.; Al-Said, N.; Al-Sulaimani, F.; Jayapal, S.K.; Al-Mawali, A. Mental health outcomes among health-care workers in Oman during COVID-19: A cluster analysis. Int. J. Nurs. Pract. 2021, 27, e12998. [Google Scholar] [CrossRef]
- Chen, Q.; Liang, M.; Li, Y.; Guo, J.; Fei, D.; Wang, L.; He, L.; Sheng, C.; Cai, Y.; Li, X.; et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e15–e16. [Google Scholar] [CrossRef]
- Huarcaya-Victoria, J. Consideraciones sobre la salud mental en la pandemia de COVID-19. Rev. Peru Med. Exp. Salud Publica 2020, 37, 327–334. [Google Scholar] [CrossRef]
- Imai, H. Trust is a key factor in the willingness of health professionals to work during the COVID-19 outbreak: Experience from the H1N1 pandemic in Japan 2009. Psychiatry Clin. Neurosci. 2020, 74, 329–330. [Google Scholar] [CrossRef] [Green Version]
- Gobierno del Perú. Guía Técnica para el Cuidado de la Salud Mental del Personal de Salud en el contexto del COVID-19. Available online: https://www.gob.pe/institucion/minsa/informes-publicaciones/473389-guia-tecnica-para-el-cuidado-de-la-salud-mental-del-personal-de-la-salud-en-el-contexto-del-covid-19 (accessed on 18 March 2021).
- Vizheh, M.; Qorbani, M.; Arzaghi, S.M.; Muhidin, S.; Javanmard, Z.; Esmaeili, M. The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. J. Diabetes Metab. Disord. 2020, 19, 1967–1978. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | n (%) | |
|---|---|---|
| Sex | Female | 379 (61.8) |
| Male | 234 (38.2) | |
| Age (years) * | 39 (30–47) | |
| Civil status | Single | 308 (50.2) |
| Married or living together | 265 (43.2) | |
| Divorced | 28 (4.6) | |
| Widowed | 12 (2.0) | |
| Hospital | Guillermo Almenara Irigoyen NH. | 384 (62.6) |
| Edgardo Rebagliati Martins NH. | 229 (37.4) | |
| Type of healthcare worker | Physicians | 87 (14.2) |
| Nurses | 122 (19.9) | |
| Other clinical workers | 96 (15.7) | |
| Non-clinical workers | 308 (50.2) | |
| Professed religion | 412 (67.2) | |
| Living alone | 85 (13.9) | |
| Living with a person at risk | 267 (43.6) | |
| Mental health history | 42 (6.9) | |
| Anxiety | Normal | 440 (71.8) |
| Mild | 120 (19.6) | |
| Moderated | 40 (6.5) | |
| Severe | 13 (2.1) | |
| Depression | Normal | 434 (70.8) |
| Mild | 124 (20.2) | |
| Moderated | 30 (4.9) | |
| Moderately severe or Severe | 25 (4.1) | |
| Stress | Mild | 132 (21.5) |
| Moderated | 459 (74.9) | |
| Severe | 22 (3.6) |
| Characteristics | Anxiety, n (%) | p Value * | Stress, n (%) | p Value * | Depression, n (%) | p Value * | |||
|---|---|---|---|---|---|---|---|---|---|
| Normal-to-Mild | Moderate-to-Severe | Mild | Moderate-to-Severe | Normal-to-Mild | Moderate-to-Severe | ||||
| Sex | 0.211 | 0.002 | 0.772 | ||||||
| Female | 342 (90.2) | 37 (9.8) | 66 (17.4) | 313 (82.6) | 344 (90.8) | 35 (9.2) | |||
| Male | 218 (93.2) | 16 (6.8) | 66 (28.2) | 168 (71.8) | 214 (91.5) | 20 (8.6) | |||
| Age | 0.437 | 0.009 | 0.432 | ||||||
| 18 to 29 years old | 120 (90.9) | 12 (9.1) | 41 (31.1) | 91 (68.9) | 116 (87.9) | 16 (12.1) | |||
| 30 to 39 years old | 181 (91.4) | 17 (8.6) | 43 (21.7) | 155 (78.3) | 183 (92.4) | 15 (7.6) | |||
| 40 to 49 years old | 153 (93.9) | 10 (6.1) | 31 (19.0) | 132 (81.0) | 151 (92.6) | 12 (7.4) | |||
| 50 years or more | 106 (88.3) | 14 (11.7) | 17 (14.2) | 103 (85.8) | 108 (90.0) | 12 (10.0) | |||
| Civil status | 0.752 | 0.543 | 0.825 | ||||||
| Single, divorced, or widowed | 319 (91.7) | 29 (8.3) | 78 (22.4) | 270 (77.6) | 316 (90.8) | 32 (9.2) | |||
| Married or cohabiting | 241 (90.9) | 24 (9.1) | 54 (20.4) | 211 (79.6) | 242 (91.3) | 23 (8.7) | |||
| Type of healthcare worker | 0.297 | <0.001 | 0.061 | ||||||
| Nonclinical workers | 285 (92.5) | 23 (7.5) | 91 (29.6) | 217 (70.5) | 287 (93.2) | 21 (6.8) | |||
| Clinical workers | 275 (90.2) | 30 (9.8) | 41 (13.4) | 264 (86.6) | 271 (88.9) | 34 (11.2) | |||
| Professed religion | 0.180 | <0.001 | 0.130 | ||||||
| No | 188 (93.5) | 13 (6.5) | 60 (29.9) | 141 (70.2) | 188 (93.5) | 13 (6.5) | |||
| Yes | 372 (90.3) | 40 (9.7) | 72 (17.5) | 340 (82.5) | 370 (89.8) | 42 (10.2) | |||
| Live alone | 0.329 | 0.630 | 0.138 | ||||||
| No | 480 (90.9) | 48 (9.1) | 112 (21.2) | 416 (78.8) | 477 (90.3) | 51 (9.7) | |||
| Yes | 80 (94.1) | 5 (5.9) | 20 (23.5) | 65 (76.5) | 81 (95.3) | 4 (4.7) | |||
| Live with a person at risk | 0.022 | 0.023 | 0.002 | ||||||
| No | 324 (93.6) | 22 (6.4) | 86 (24.9) | 260 (75.1) | 326 (94.2) | 20 (5.8) | |||
| Yes | 236 (88.4) | 31 (11.6) | 46 (17.2) | 221 (82.8) | 232 (86.9) | 35 (13.1) | |||
| Mental health history | <0.001 | 0.006 | <0.001 | ||||||
| No | 534 (93.5) | 37 (6.5) | 130 (22.8) | 441 (77.2) | 532 (93.2) | 39 (6.8) | |||
| Yes | 26 (61.9) | 16 (38.1) | 2 (4.8) | 40 (95.2) | 26 (61.9) | 16 (38.1) | |||
| Feeling stigma for working in the hospital | <0.001 | 0.018 | <0.001 | ||||||
| Less than half the days | 525 (93.1) | 39 (6.9) | 128 (22.7) | 436 (77.3) | 521 (92.4) | 43 (7.6) | |||
| More than half of the days | 35 (71.4) | 14 (28.6) | 4 (8.2) | 45 (91.8) | 37 (75.5) | 12 (24.5) | |||
| Fear of infecting family members | <0.001 | <0.001 | <0.001 | ||||||
| Less than half the days | 337 (96.6) | 12 (3.4) | 94 (26.9) | 255 (73.1) | 336 (96.3) | 13 (3.7) | |||
| More than half of the days | 223 (84.5) | 41 (15.5) | 38 (14.4) | 226 (85.6) | 222 (84.1) | 42 (15.9) | |||
| Thinking about losing your job | <0.001 | 0.001 | <0.001 | ||||||
| Less than half the days | 514 (94.7) | 29 (5.3) | 128 (23.6) | 415 (76.4) | 511 (94.1) | 32 (5.9) | |||
| More than half of the days | 46 (65.7) | 24 (34.3) | 4 (5.7) | 66 (94.3) | 47 (67.1) | 23 (32.9) | |||
| Having two or more symptoms of COVID-19 in the last few weeks | <0.001 | 0.002 | <0.001 | ||||||
| No | 428 (93.9) | 28 (6.1) | 112 (24.6) | 344 (75.4) | 434 (95.2) | 22 (4.8) | |||
| Yes | 132 (84.1) | 25 (15.9) | 20 (12.7) | 137 (87.3) | 124 (79.0) | 33 (21.0) | |||
| Characteristics | Moderate-to-Severe Anxiety | Moderate-to-Severe Stress | Moderate-to-Severe Depression | ||
|---|---|---|---|---|---|
| rPR (95% CI) | aRP (95%CI) * | rPR (95% CI) ** | rPR (95% CI) | aRP (95%CI) *** | |
| Sex | |||||
| Male | Ref. | – | Ref. | Ref. | – |
| Female | 1.43 (0.62–3.29) | 1.15 (1.07–1.24) | 1.08 (1.00–1.17) | ||
| Age | |||||
| 18 to 29 years old | Ref. | – | Ref. | Ref. | Ref. |
| 30 to 39 years old | 0.94 (0.65–1.36) | 1.14 (0.94–1.37) | 0.63 (0.42–0.93) | 0.34 (0.15–0.77) | |
| 40 to 49 years old | 0.67 (0.23–2.01) | 1.17 (1.08–1.27) | 0.61 (0.37–0.99) | 0.63 (0.47–0.85) | |
| 50 years or more | 1.28 (1.18–1.40) | 1.25 (1.20–1.29) | 0.83 (0.31–2.19) | 0.70 (0.17–2.88) | |
| Civil status | |||||
| Single, divorced, or widowed | Ref. | – | Ref. | Ref. | – |
| Married or cohabiting | 1.09 (1.08–1.10) | 1.03 (1.03–1.03) | 0.94 (0.69–1.28) | ||
| Type of healthcare worker | |||||
| Nonclinical workers | Ref. | – | Ref. | Ref. | – |
| Clinical workers | 1.32 (0.76–2.28) | 1.23 (1.13–1.34) | 1.63 (1.11–2.42) | ||
| Professed religion | |||||
| No | Ref. | – | Ref. | Ref. | – |
| Yes | 1.50 (1.39–1.62) | 1.18 (1.04–1.33) | 1.58 (0.73–3.42) | ||
| Living alone | |||||
| No | Ref. | – | Ref. | Ref. | – |
| Yes | 0.65 (0.59–0.70) | 0.97 (0.85–1.10) | 0.49 (0.38–0.63) | ||
| Living with a person at risk of COVID-19 | |||||
| No | Ref. | – | Ref. | Ref. | – |
| Yes | 1.83 (1.09–3.06) | 1.10 (1.03–1.17) | 2.27 (1.53–3.36) | ||
| Mental health history | |||||
| No | Ref. | Ref. | Ref. | Ref. | Ref. |
| Yes | 5.88 (4.84–7.14) | 3.42 (2.97–3.94) | 1.23 (1.23–1.24) | 5.58 (4.71–6.61) | 3.34 (2.90–3.84) |
| Feeling stigma for working in the hospital | |||||
| Less than half the days | Ref. | – | Ref. | Ref. | – |
| More than half of the days | 4.13 (1.80–9.50) | 1.19 (1.12–1.25) | 3.21 (2.75–3.75) | ||
| Fear of infecting family members | |||||
| Less than half the days | Ref. | Ref. | Ref. | Ref. | Ref. |
| More than half of the days | 4.52 (4.18–4.89) | 2.91 (2.75–3.08) | 1.17 (1.11–1.23) | 4.27 (2.90–6.28) | 2.51 (1.31–4.80) |
| Thinking about losing their job | |||||
| Less than half the days | Ref. | Ref. | Ref. | Ref. | Ref. |
| More than half of the days | 6.42 (4.23–9.75) | 3.62 (2.04–6.43) | 1.23 (1.15–1.32) | 5.58 (4.92–6.32) | 3.39 (2.62–4.27) |
| Having two or more symptoms of COVID-19 in the last few weeks | |||||
| No | Ref. | – | Ref. | Ref. | Ref. |
| Yes | 2.59 (1.62–4.15) | 1.16 (1.16–1.16) | 4.36 (3.70–5.13) | 3.59 (2.11–6.09) | |
| Age | Sex | Work Area | Symptoms |
|---|---|---|---|
| Clinical Workers | |||
| 32 | Female | Hospitalization | Moderate anxiety |
| 29 | Female | Hospitalization | Severe depression |
| 53 | Male | Emergency | Moderate stress |
| 28 | Female | ICU | Severe stress |
| 47 | Female | Hospitalization | Moderate anxiety |
| 34 | Male | ICU | Severe depression |
| 60 | Female | Hospitalization | Severe stress |
| 37 | Female | Hospitalization | Severe stress |
| Nonclinical workers | |||
| 39 | Male | Administrative | Moderate anxiety |
| 40 | Female | Administrative | Moderate-to-severe depression |
| 58 | Female | Administrative | Severe stress |
| 30 | Male | Administrative | Moderate-to-severe depression |
| 47 | Female | Cleaning | Moderate anxiety |
| 51 | Female | Cleaning | Moderate-to-severe depression |
| 38 | Female | Cleaning | Severe stress |
| 23 | Male | Cleaning | Severe stress |
| 26 | Male | Security | Severe anxiety |
| 54 | Female | Security | Moderate-to-severe depression |
| 40 | Male | Security | Moderate stress |
| 40 | Male | Security | Moderate stress |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huarcaya-Victoria, J.; Villarreal-Rao, B.; Luna, M.; Rojas-Mendoza, W.; Alarcon-Ruiz, C.A.; Villarreal-Zegarra, D.; Vilela-Estrada, A.L.; Ramírez, S. Factors Associated with Mental Health Outcomes in Hospital Workers during the COVID-19 Pandemic: A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2022, 19, 5346. https://doi.org/10.3390/ijerph19095346
Huarcaya-Victoria J, Villarreal-Rao B, Luna M, Rojas-Mendoza W, Alarcon-Ruiz CA, Villarreal-Zegarra D, Vilela-Estrada AL, Ramírez S. Factors Associated with Mental Health Outcomes in Hospital Workers during the COVID-19 Pandemic: A Mixed-Methods Study. International Journal of Environmental Research and Public Health. 2022; 19(9):5346. https://doi.org/10.3390/ijerph19095346
Chicago/Turabian StyleHuarcaya-Victoria, Jeff, Beltran Villarreal-Rao, Matilde Luna, Wendoline Rojas-Mendoza, Christoper A. Alarcon-Ruiz, David Villarreal-Zegarra, Ana L. Vilela-Estrada, and Samantha Ramírez. 2022. "Factors Associated with Mental Health Outcomes in Hospital Workers during the COVID-19 Pandemic: A Mixed-Methods Study" International Journal of Environmental Research and Public Health 19, no. 9: 5346. https://doi.org/10.3390/ijerph19095346