
Epidemiological, Clinical, and Virological Investigation of the First Four Cases of Monkeypox in Cartagena during the 2022 Outbreak

Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Definition and Identification
2.2. Molecular Detection
2.3. Sequencing and Bioinformatics Processing
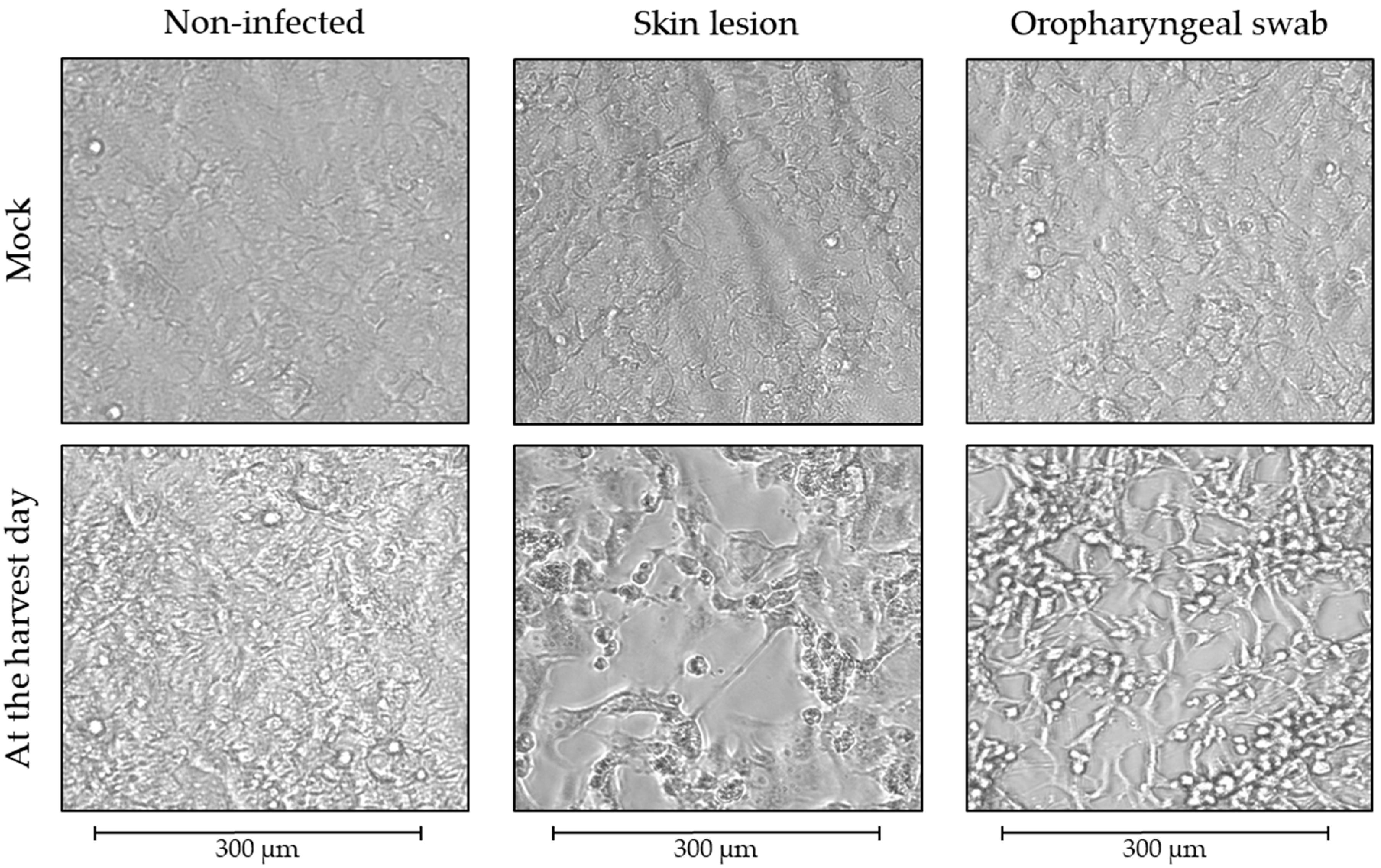
2.4. Viral Isolation and Plaque Assay
3. Results
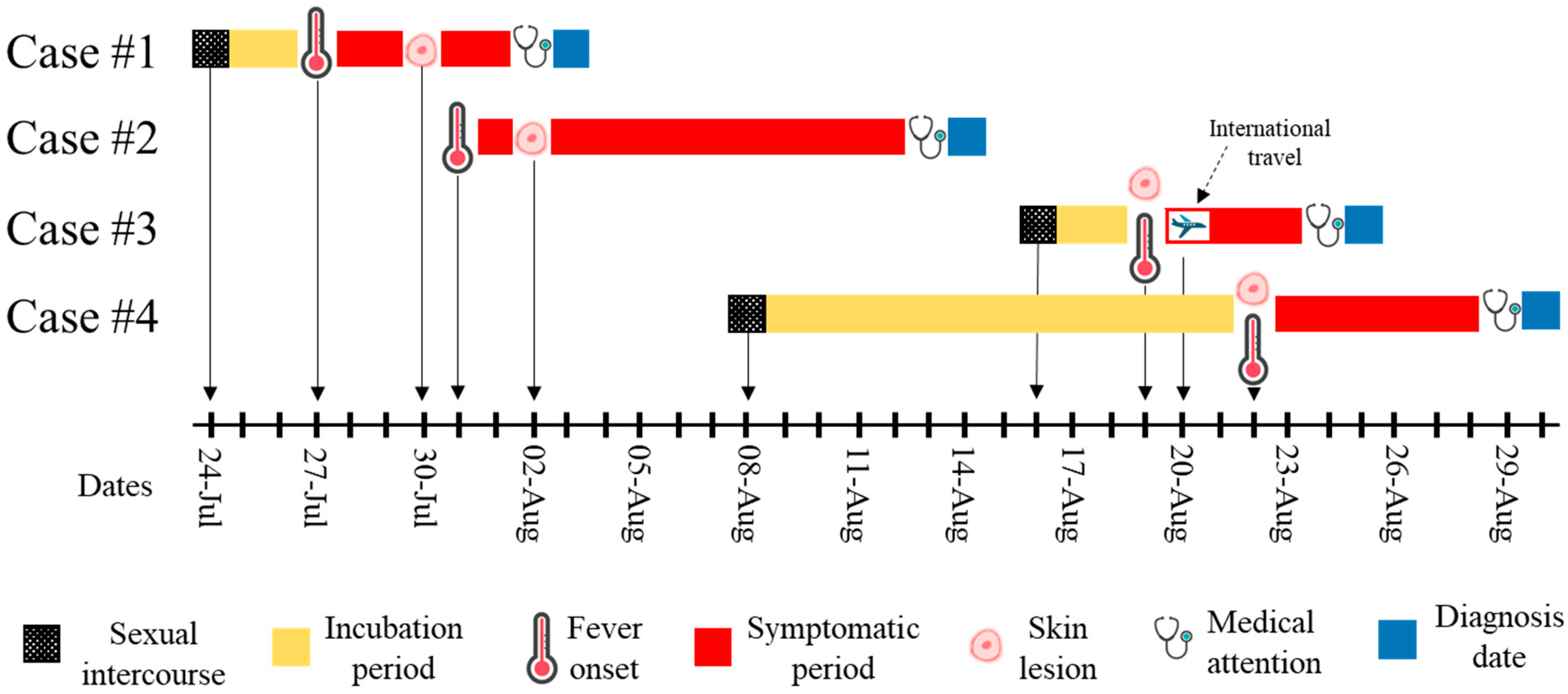
3.1. Case #1
3.2. Case #2
3.3. Case #3
3.4. Case #4
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Breman, J.G.; Kalisa-Ruti; Steniowski, M.V.; Zanotto, E.; Gromyko, A.I.; Arita, I. Human monkeypox, 1970–1979. Bull. World Health Organ. 1980, 58, 165–182. [Google Scholar] [PubMed]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The changing epidemiology of human monkeypox—A potential threat? A systematic review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef]
- Ghazy, R.M.; Hammad, E.M.; Hall, M.A.; Mahboob, A.; Zeina, S.; Elbanna, E.H.; Fadl, N.; Abdelmoneim, S.A.; ElMakhzangy, R.; Hammad, H.M.; et al. How can imported monkeypox break the borders? A rapid systematic review. Comp. Immunol. Microbiol. Infect. Dis. 2022, 92, 101923. [Google Scholar] [CrossRef]
- Bhattacharya, M.; Dhama, K.; Chakraborty, C. Recently spreading human monkeypox virus infection and its transmission during COVID-19 pandemic period: A travelers’ prospective. Travel Med. Infect. Dis. 2022, 49, 102398. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Multi-Country Monkeypox Outbreak: Situation Update—17 June 2022. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON393 (accessed on 7 September 2022).
- World Health Organization. WHO Director-General Declares the Ongoing Monkeypox Outbreak a Public Health Emergency of International Concern. Available online: https://www.who.int/europe/news/item/23-07-2022-who-director-general-declares-the-ongoing-monkeypox-outbreak-a-public-health-event-of-international-concern (accessed on 7 September 2022).
- Centers for Disease Control and Prevention. 2022 Monkeypox Outbreak Global Map. Available online: https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html (accessed on 1 December 2022).
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, I.; Habibi, M.S.; et al. Monkeypox Virus Infection in Humans across 16 Countries—April–June 2022. N. Engl. J. Med. 2022, 387, 679–691. [Google Scholar] [CrossRef]
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C.; et al. Clinical presentation and virological assessment of confirmed human monkeypox virus cases in Spain: A prospective observational cohort study. Lancet 2022, 400, 661–669. [Google Scholar] [CrossRef]
- Ministerio de Salud y Protección Social de Colombia. Minsalud e INS Confirman Tres Casos de Viruela Símica en Colombia. Available online: https://www.minsalud.gov.co/Paginas/Minsalud-e-INS-confirman-tres-casos-de-viruela-simica-en-Colombia.aspx (accessed on 7 September 2022).
- Instituto Nacional de Salud de Colombia. Enfermedades Emergentes—Viruela Símica. Available online: https://www.ins.gov.co/Noticias/Paginas/Enfermedades-emergentes.aspx#hepatitis (accessed on 19 December 2022).
- Li, Y.; Zhao, H.; Wilkins, K.; Hughes, C.; Damon, I.K. Real-time PCR assays for the specific detection of monkeypox virus West African and Congo Basin strain DNA. J. Virol. Methods 2010, 169, 223–227. [Google Scholar] [CrossRef]
- Matthijs, W.; Jonges, M.; van den Ouden, A. Monkeypox Virus Whole Genome Sequencing Using Combination of NextGenPCR and Oxford Nanopore. Available online: https://www.protocols.io/view/monkeypox-virus-whole-genome-sequencing-using-comb-n2bvj6155lk5/v1 (accessed on 7 September 2022).
- Laiton-Donato, K.; Álvarez-Díaz, D.A.; Franco-Muñoz, C.; Ruiz-Moreno, H.A.; Rojas-Estévez, P.; Prada, A.; Rosales, A.; Ospina, M.L.; Mercado-Reyes, M. Monkeypox virus genome sequence from an imported human case in Colombia. Biomedica 2022, 42, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Lapa, D.; Carletti, F.; Mazzotta, V.; Matusali, G.; Pinnetti, C.; Meschi, S.; Gagliardini, R.; Colavita, F.; Mondi, A.; Minosse, C.; et al. Monkeypox virus isolation from a semen sample collected in the early phase of infection in a patient with prolonged seminal viral shedding. Lancet Infect. Dis. 2022, 22, 1267–1269. [Google Scholar] [CrossRef]
- Kim, J.-W.; Lee, M.; Shin, H.; Choi, C.-H.; Choi, M.-M.; Kim, J.W.; Yi, H.; Yoo, C.-K.; Rhie, G.-E. Isolation and identification of monkeypox virus MPXV-ROK-P1-2022 from the first case in the Republic of Korea. Osong Public Health Res. Perspect. 2022, 13, 308–311. [Google Scholar] [CrossRef]
- Noe, S.; Zange, S.; Seilmaier, M.; Antwerpen, M.H.; Fenzl, T.; Schneider, J.; Spinner, C.D.; Bugert, J.J.; Wendtner, C.-M.; Wölfel, R. Clinical and virological features of first human monkeypox cases in Germany. Infection 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Juarez, D.; Long, K.C.; Aguilar, P.; Kochel, T.J.; Halsey, E.S. Assessment of plaque assay methods for alphaviruses. J. Virol. Methods 2013, 187, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Salud y Protección Social—Instituto Nacional de Salud de Colombia. Viruela Símica (Monkepox). Available online: https://app.powerbi.com/view?r=eyJrIjoiNjQzZGQ0ZjAtODRhMi00MzFhLWFmODctOWMxNGVkNGFjMDhkIiwidCI6ImE2MmQ2YzdiLTlmNTktNDQ2OS05MzU5LTM1MzcxNDc1OTRiYiIsImMiOjR9 (accessed on 19 December 2022).
- Núñez, I.; García-Grimshaw, M.; Ceballos-Liceaga, S.E.; Toledo-Salinas, C.; Carbajal-Sandoval, G.; Sosa-Laso, L.; García-Rodríguez, G.; Cortés-Alcalá, R.; de la Torre, A.; Fragoso-Saavedra, S.; et al. Epidemiological and clinical characteristics of patients with human monkeypox infection in Mexico: A nationwide observational study. Lancet Reg. Health Am. 2022, 100392. [Google Scholar] [CrossRef] [PubMed]
- Miura, F.; van Ewijk, C.E.; Backer, J.A.; Xiridou, M.; Franz, E.; Op de Coul, E.; Brandwagt, D.; van Cleef, B.; van Rijckevorsel, G.; Swaan, C.; et al. Estimated incubation period for monkeypox cases confirmed in the Netherlands, May 2022. Eurosurveillance 2022, 27, 2200448. [Google Scholar] [CrossRef] [PubMed]
- Brites, C.; Deminco, F.; Sá, M.S.; Brito, J.T.; Luz, E.; Stocker, A. The First Two Cases of Monkeypox Infection in MSM in Bahia, Brazil, and Viral Sequencing. Viruses 2022, 14, 1841. [Google Scholar] [CrossRef] [PubMed]
- Paran, N.; Yahalom-Ronen, Y.; Shifman, O.; Lazar, S.; Ben-Ami, R.; Yakubovsky, M.; Levy, I.; Wieder-Feinsod, A.; Amit, S.; Katzir, M.; et al. Monkeypox DNA levels correlate with virus infectivity in clinical samples, Israel, 2022. Eurosurveillance 2022, 27, 2200636. [Google Scholar] [CrossRef] [PubMed]
- Suñer, C.; Ubals, M.; Tarín-Vicente, E.J.; Mendoza, A.; Alemany, A.; Hernández-Rodríguez, Á.; Casañ, C.; Descalzo, V.; Ouchi, D.; Marc, A.; et al. Viral dynamics in patients with monkeypox infection: A prospective cohort study in Spain. Lancet Infect. Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative on Sharing Avian Influenza Data (GISAID)—Submission Tracker Global hMpxV. Available online: https://gisaid.org/submission-tracker-global-hmpxv/ (accessed on 20 December 2022).
- Global Initiative on Sharing Avian Influenza Data (GISAID)—hMpxV Phylogeny. Available online: https://gisaid.org/hmpxv-phylogeny/ (accessed on 19 December 2022).
- Scarpa, F.; Sanna, D.; Azzena, I.; Cossu, P.; Locci, C.; Angeletti, S.; Maruotti, A.; Ceccarelli, G.; Casu, M.; Fiori, P.L.; et al. Genetic Variability of the Monkeypox Virus Clade IIb B.1. J. Clin. Med. 2022, 11, 6388. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Case | Source of Infection a | Skin Lesion Swab | Oropharyngeal Swab | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| G2RG/G2RWA b | NCBI Accession Number | Genome Coverage/Average Depth | Day Post Infection/CPE c | Day Post Infection/G2RG b | PFU/mL | G2RG b | Day Post Infection/CPE c | Day Post Infection/G2RG b | PFU/mL | ||
| #1 | Unknown | 21.5/18.2 | OP390175 | 88.0%/315.7X | 2/1+; 3/2+ 4/3+ | 0/18.5; 4/16.1 | 1.5 × 103 | 38.6 | 6/1+; 7/2+; 8/3+ | 0/37.0; 8/Negative | 0 |
| #2 | Unknown | 19.1/17.0 | Not deposited d | 53.3%/96.8X | 7/1+ 8/2+ 9/3+ | 0/21.9; 8/30.8 | 1.0 × 101 | 35.3 | 6/1+; 7/2+; 8/3+ | 0/36.5 8/Negative | 0 |
| #3 | Imported | 20.3/18.5 | OP390179 | 88.8%/347.4X | 1/1+; 2/2+; 3/3+ | 0/19.4; 1/24.6; 2/22.4; 3/17.3 | 6.0 × 103 | 24.4 | 2/1+; 3/2+; 4/3+ | 0/24.4; 4/16.5 | 5.0 × 101 |
| #4 | Unknown | 22.2/21.9 | OP390180 | 78.5%/247.6X | 2/2+; 3/3+ | 0/21.8; 3/20.1 | 5.0 × 102 | 28.4 | 6/1+; 7/2+; 8/3+ | 0/30.9; 8/31.7 | 3.0 × 101 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loyola, S.; Fernández-Ruiz, M.; Gómez-Camargo, D. Epidemiological, Clinical, and Virological Investigation of the First Four Cases of Monkeypox in Cartagena during the 2022 Outbreak. Pathogens 2023, 12, 159. https://doi.org/10.3390/pathogens12020159
Loyola S, Fernández-Ruiz M, Gómez-Camargo D. Epidemiological, Clinical, and Virological Investigation of the First Four Cases of Monkeypox in Cartagena during the 2022 Outbreak. Pathogens. 2023; 12(2):159. https://doi.org/10.3390/pathogens12020159
Chicago/Turabian StyleLoyola, Steev, Mashiel Fernández-Ruiz, and Doris Gómez-Camargo. 2023. "Epidemiological, Clinical, and Virological Investigation of the First Four Cases of Monkeypox in Cartagena during the 2022 Outbreak" Pathogens 12, no. 2: 159. https://doi.org/10.3390/pathogens12020159