
Intrauterine and Extrauterine Environmental PM2.5 Exposure Is Associated with Overweight/Obesity (O/O) in Children Aged 6 to 59 Months from Lima, Peru: A Case-Control Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
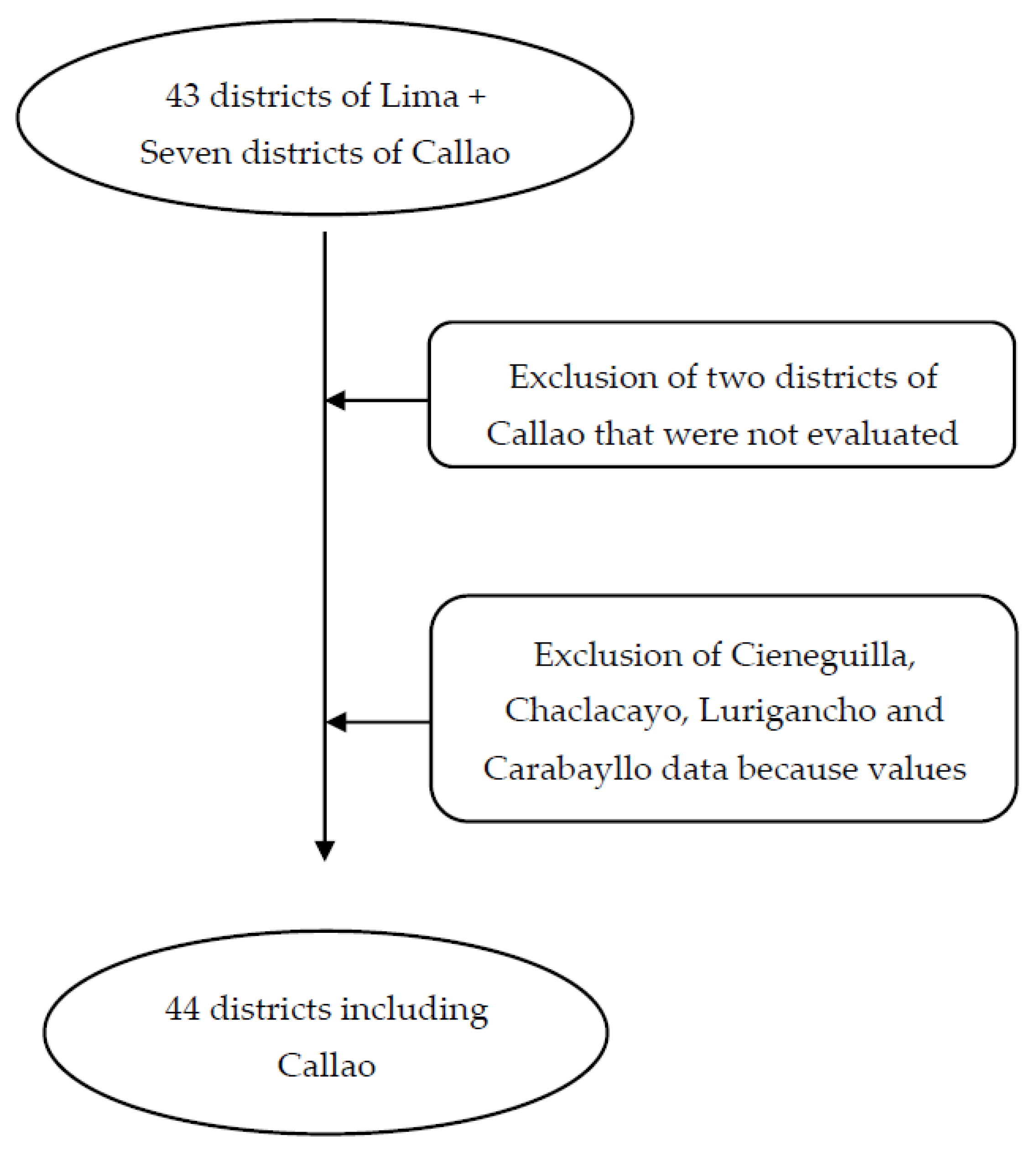
2.1. Study Area
2.2. PM2.5 Exposure
2.3. Study Population
2.4. Definition of Cases and Controls
2.5. Variable Definitions
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Air Pollution [Internet]. WHO. 2020. Available online: https://www.who.int/health-topics/air-pollution#tab=tab_1 (accessed on 6 November 2021).
- Feng, S.; Gao, D.; Liao, F.; Zhou, F.; Wang, X. The health effects of ambient PM2.5 and potential mechanisms. Ecotoxicol. Environ. Saf. 2016, 128, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Vasquez-Apestegui, B.V.; Parras-Garrido, E.; Tapia, V.; Paz-Aparicio, V.M.; Rojas, J.P.; Sanchez-Ccoyllo, O.R.; Gonzales, G.F. Association between air pollution in Lima and the high incidence of COVID-19: Findings from a post hoc analysis. BMC Public Health 2021, 21, 1161. [Google Scholar] [CrossRef] [PubMed]
- Gurnani, M.; Birken, C.; Hamilton, J. Childhood Obesity. Pediatr. Clin. N. Am. 2015, 62, 821–840. [Google Scholar] [CrossRef] [PubMed]
- Malecka-Tendera, E.; Mazur, A. Childhood obesity: A pandemic of the twenty-first century. Int. J. Obes. 2006, 30, S1–S3. [Google Scholar] [CrossRef] [Green Version]
- An, R.; Ji, M.; Yan, H.; Guan, C. Impact of ambient air pollution on obesity: A systematic review. Int. J. Obes. 2018, 42, 1112–1126. [Google Scholar] [CrossRef]
- Furlong, M.A.; Klimentidis, Y.C. Associations of air pollution with obesity and body fat percentage, and modification by polygenic risk score for BMI in the UK Biobank. Environ. Res. 2020, 185, 109364. [Google Scholar] [CrossRef]
- Zheng, H.; Xu, Z.; Wang, Q.; Ding, Z.; Zhou, L.; Xu, Y.; Su, H.; Li, X.; Zhang, L.; Cheng, J. Long-term exposure to ambient air pollution and obesity in school-aged children and adolescents in Jiangsu province of China. Environ. Res. 2021, 195, 110804. [Google Scholar] [CrossRef]
- Zhang, N.; Wang, L.; Zhang, M.; Nazroo, J. Air quality and obesity at older ages in China: The role of duration, severity and pollutants. PLoS ONE 2019, 14, e0226279. [Google Scholar] [CrossRef] [Green Version]
- Barrea, L.; Savastano, S.; Di Somma, C.; Savanelli, M.C.; Nappi, F.; Albanese, L.; Orio, F.; Colao, A. Low serum vitamin D-status, air pollution and obesity: A dangerous liaison. Rev. Endocr. Metab. Disord. 2017, 18, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Darbre, P.D. Overview of air pollution and endocrine disorders. Int. J. Gen. Med. 2018, 11, 191–207. [Google Scholar]
- Chen, M.; Wang, X.; Hu, Z.; Zhou, H.; Xu, Y.; Qiu, L.; Qin, X.; Zhang, Y.; Ying, Z. Programming of mouse obesity by maternal exposure to concentrated ambient fine particles. Part. Fibre Toxicol. 2017, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.-X.; Ge, C.-X.; Qin, Y.-T.; Gu, T.-T.; Lou, D.-S.; Li, Q.; Hu, F.-H.; Feng, J.; Huang, P.; Tan, J. Prolonged PM2.5 exposure elevates risk of oxidative stress-driven nonalcoholic fatty liver disease by triggering increase of dyslipidemia. Free Radic. Biol. Med. 2019, 130, 542–556. [Google Scholar] [CrossRef]
- Izaola, O.; de Luis, D.; Sajoux, I.; Domingo, J.C.; Vidal, M. Inflammation, and obesity (lipoinflammation). Nutr. Hosp. 2015, 31, 2352–2358. [Google Scholar] [PubMed] [Green Version]
- Yang, B.-Y.; Guo, Y.; Markevych, I.; Qian, Z.M.; Bloom, M.S.; Heinrich, J.; Dharmage, S.C.; Rolling, C.A.; Jordan, S.S.; Komppula, M.; et al. Association of Long-term Exposure to Ambient Air Pollutants With Risk Factors for Cardiovascular Disease in China. JAMA Netw. Open 2019, 2, e190318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IQAir. World Air Quality Report [Internet]. 2021. Available online: https://www.iqair.com/world-air-quality-report (accessed on 14 June 2022).
- Echevarría-Castro, N.; Matayoshi-Pérez, A.; Alvarado, G. Association between Maternal Depressive Symptoms with Overweight/Obesity among Children Aged 0–5 Years According to the 2016 Demographic and Family Health Survey. Child. Obes. 2020, 16, 307–315. [Google Scholar] [CrossRef]
- Dorsey, A.F.; Penny, M.E.; Thompson, A.L. Adiposity, and pathogen exposure: An investigation of response to iron supplementation and hypothesized predictors in anemic pre-school-aged children living in a dual burden environment. Am. J. Phys. Anthropol. 2021, 176, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Morales-Ancajima, V.C.; Tapia, V.; Vu, B.N.; Liu, Y.; Alarcón-Yaquetto, D.E.; Gonzales, G.F. Increased Outdoor PM2.5 Concentration Is Associated with Moderate/Severe Anemia in Children Aged 6–59 Months in Lima, Peru. J. Environ. Public Health 2019, 2019, 6127845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vu, B.; Sánchez, O.; Bi, J.; Xiao, Q.; Hansel, N.; Checkley, W.; Gonzales, G.F.; Steenland, K.; Liu, Y. Developing an advanced PM2.5 exposure model in Lima, Peru. Remote Sens. 2019, 11, 641. [Google Scholar] [CrossRef] [Green Version]
- Tapia, V.; Steenland, K.; Sarnat, S.E.; Vu, B.; Liu, Y.; Sánchez-Ccoyllo, O.; Vásquez, V.; Gonzales, G.F. Time-series analysis of ambient PM2.5 and cardiorespiratory emergency room visits in Lima, Peru during 2010–2016. J. Expo. Sci. Environ. Epidemiol. 2020, 30, 680–688. [Google Scholar] [CrossRef]
- WHO. Child Growth Standards. 2014. Available online: https://www.who.int/tools/child-growth-standards/standards/weight-for-length-height (accessed on 9 May 2020).
- Instituto de Estadística e Informática. Mapa de Pobreza Monetaria Provincial y Distrital, Lima. 2018. Available online: https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1718/Libro.pdf (accessed on 15 May 2020).
- Fleisch, A.F.; Rifas-Shiman, S.L.; Koutrakis, P.; Schwartz, J.D.; Kloog, I.; Melly, S.; Coull, B.A.; Zanobetti, A.; Gillman, M.W.; Gold, D.R.; et al. Prenatal Exposure to Traffic Pollution: Associations with Reduced Fetal Growth and Rapid Infant Weight Gain. Epidemiology 2015, 26, 43–50. [Google Scholar] [CrossRef]
- Zordão, O.P.; Claro, L.W.; Saldiva, P.; Donato, J.; Veras, M.; Prada, P.O. Air Pollution Exposure during Pregnancy and Lactation Induces Obesity and Glucose Intolerance in the Offspring. Diabetes 2018, 67 (Suppl. 1), 223-OR. [Google Scholar] [CrossRef]
- Patterson, W.B.; Glasson, J.; Naik, N.; Jones, R.B.; Berger, P.K.; Plows, J.F.; Minor, H.A.; Lurmann, F.; Gornan, M.I.; Alderete, T.L. Prenatal exposure to ambient air pollutants and early infant growth and adiposity in the Southern California Mother’s Milk Study. Environ. Health 2021, 20, 67. [Google Scholar] [CrossRef] [PubMed]
- Bloemsma, L.D.; Dabelea, D.; Thomas, D.S.K.; Peel, J.L.; Adgate, J.L.; Allshouse, W.B.; Martenies, S.E.; Magzamen, S.; Starling, A.P. Prenatal exposure to ambient air pollution and traffic and indicators of adiposity in early childhood: The Healthy Start study. Int. J. Obes. 2022, 46, 494–501. [Google Scholar] [CrossRef]
- Fleisch, A.F.; Aris, I.M.; Rifas-Shiman, S.L.; Coull, B.A.; Luttmann-Gibson, H.; Koutrakis, P.; Schwartz, J.D.; Kloog, I.; Gold, D.R.; Oken, E. Prenatal Exposure to Traffic Pollution and Childhood Body Mass Index Trajectory. Front. Endocrinol. 2019, 9, 771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanoli, J.; Coull, B.A.; de Cuba, S.E.; Fabian, P.M.; Carnes, F.; Massaro, M.A.; Poblacion, A.; Bellocco, R.; Kloog, I.; Schwartz, J.; et al. Postnatal exposure to PM2.5 and weight trajectories in early childhood. Environ. Epidemiol. 2021, 6, E181. [Google Scholar] [CrossRef] [PubMed]
- Rolland-Cachera, M.F.; Deheeger, M.; Bellisle, F.; Sempé, M.; Guilloud-Bataille, M.; Patois, E. Adiposity rebound in children: A simple indicator for predicting obesity. Am. J. Clin. Nutr. 1984, 39, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Rolland-Cachera, M.F.; Deheeger, M.; Guilloud-Bataille, M.; Avons, P.; Patois, E.; Sempé, M. Tracking the development of adiposity from one month of age to adulthood. Ann. Hum. Biol. 1987, 14, 219–229. [Google Scholar] [CrossRef]
- Vrijkotte, T.G.M.; Oostvogels, A.J.J.M.; Stronks, K.; Roseboom, T.J.; Hof, M.H.P. Growth patterns from birth to overweight at age 5–6 years of children with various backgrounds in socioeconomic status and country of origin: The ABCD study. Pediatr. Obes. 2020, 15, 12635. [Google Scholar] [CrossRef] [Green Version]
- Cole, T.J. Children grow and horses race: Is the adiposity rebound a critical period for later obesity? BMC Pediatr. 2004, 4, 6. [Google Scholar] [CrossRef] [Green Version]
- Goh, E.K.; Kim, O.Y.; Yoon, S.R.; Jeon, H.J. Timing of Adiposity Rebound and Determinants of Early Adiposity Rebound in Korean Infants and Children Based on Data from the National Health Insurance Service. Nutrients 2022, 14, 929. [Google Scholar] [CrossRef]
- Ip, E.H.; Marshall, S.A.; Saldana, S.; Skelton, J.A.; Suerken, C.K.; Arcury, T.A.; Quandt, S.A. Determinants of Adiposity Rebound Timing in Children. J. Pediatr. 2017, 184, 151–156.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banjari, I.; Martinović, M.; Belojević, G.; Ašanin, B.; Kovačević, N.D.; Kenjerić, D.; Miskulin, M.; Patovic, S.; Sokolic, D.; Buljan, V.; et al. Poverty and other correlates of obesity and underweight among 7-year-olds from Croatia and Montenegro. Public Health 2020, 182, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Gamboa-Gamboa, T.; Fantin, R.; Cordoba, J.; Caravaca, I.; Gómez-Duarte, I. Relationship between childhood obesity and socio-economic status among primary school children in Costa Rica. Public Health Nutr. 2021, 24, 3825–3833. [Google Scholar] [CrossRef] [PubMed]
- Wallwork, R.S.; Colicino, E.; Zhong, J.; Kloog, I.; Coull, B.A.; Vokonas, P.; Schwartz, J.D.; Baccarelli, A.A. Ambient Fine Particulate Matter, Outdoor Temperature, and Risk of Metabolic Syndrome. Am. J. Epidemiol. 2017, 185, 30–39. [Google Scholar] [CrossRef]
- Eriksson, J.G.; Forsén, T.; Tuomilehto, J.; Osmond, C.; Barker, D.J.P. Early adiposity rebound in childhood and risk of Type 2 diabetes in adult life. Diabetologia 2003, 46, 190–194. [Google Scholar] [CrossRef]
- Farro-Maldonado, M.Y.; Gutierrez-Perez, G.; Hernandez-Vásquez, A.; Barrenechea-Pulache, A.; Santero, M.; Rojas-Roque, C.; Azanedo, D. Socioeconomic inequalities in abdominal obesity among Peruvian adults. PLoS ONE 2021, 16, e0254365. [Google Scholar] [CrossRef]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, M.H.; Silverstein, J.H.; Yanovski, J.A. Pediatric Obesity-Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 709–757. [Google Scholar] [CrossRef] [Green Version]
- Paes, S.T.; Marins, J.C.B.; Andreazzi, A.E. Metabolic effects of exercise on childhood obesity: A current vision. Rev. Paul. Pediatr. 2015, 33, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.Y.; Qi, S.J. Childhood obesity and food intake. World J. Pediatrics 2015, 11, 101–107. [Google Scholar] [CrossRef]
- Andriani, H. Birth weight and childhood obesity: Effect modification by residence and household wealth. Emerg. Themes Epidemiol. 2022, 18, 6. [Google Scholar] [CrossRef]
- Reilly, J.J.; Armstrong, J.; Dorosty, A.R.; Emmett, P.M.; Ness, A.; Rogers, I.; Steer, C.; Sherriff, A. Avon Longitudinal Study of Parents and Children Study Team. Early life risk factors for obesity in childhood: Cohort study. BMJ 2005, 11, 1357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzales, G.F.; Steenland, K. Environmental Health in Peru: Outdoor and Indoor Air Contamination. Rev. Panam. Salud. Pub. 2014, 36, 141. [Google Scholar]



{kind=link}
{kind=link}
| O/O Aged 6 to 11 | O/O Aged 12 to 35 | O/O Aged 36 to 59 |
|---|---|---|
| PM2.5 (μg/m3) Quartiles | PM2.5 Quartiles | PM2.5 Quartiles |
| Q1 (14.36–18.63) | Q1 (14.38–18.77) | Q1 (14.91–18.35) |
| Q2 (18.64–20.40) | Q2 (18.78–20.76) | Q2 (18.36–20.19) |
| Q3 (20.41–26.85) | Q3 (20.77–27.64) | Q3 (20.20–27.53) |
| Q4 (26.86–46.05) | Q4 (27.65–46.07) | Q4 (27.54–46.05) |
| Relative Humidity (%) | ||
| Q1 (54.37–66.90) | Q1 (54.20–66.44) | Q1 (54.46–66.79) |
| Q2 (66.91–73.16) | Q2 (66.45–71.88) | Q2 (66.80–73.37) |
| Q3 (73.17–80.67) | Q3 (71.89–79.61) | Q3 (73.38–80.04) |
| Q4 (80.68–89.90) | Q4 (79.62–89.70) | Q4 (80.05–89.69) |
| Temperature (°C) | ||
| Q1 (17.09–21.55) | Q1 (17.10–21.57) | Q1 (17.11–21.63) |
| Q2 (21.56–23.29) | Q2 (21.58–23.16) | Q2 (21.64–23.41) |
| Q3 (23.30–25.56) | Q3 (23.17–25.41) | Q3 (23.42–25.52) |
| Q4 (25.57–30.35) | Q4 (25.42–30.35) | Q4 (25.53–30.36) |
| Poverty (%) | ||
| Q1 (0.17–10.48) | Q1 (0.17–10.48) | Q1 (0.17–10.04) |
| Q2 (10.49–16.84) | Q2 (10.49–16.84) | Q2 (10.05–15.99) |
| Q3 (16.85–22.80) | Q3 (16.85–22.04) | Q3 (16.00–22.04) |
| Q4 (22.81–29.09) | Q4 (22.05–29.09) | Q4 (22.05–29.09) |
| Exposure | Extrauterine | Intrauterine | ||
|---|---|---|---|---|
| Variables | Cases n = 32,616 | Control n = 32,616 | Cases n = 20,433 | Control n = 20,433 |
| (Mean ± SD) | (Mean ± SD) | (Mean ± SD) | (Mean ± SD) | |
| Weight (kg) | 14.23 ± 4.36 a | 11.45 ± 3.23 | 12.29 ± 2.71 | 10.04 ± 2.09 a |
| Height (cm) | 82.52 ± 12.98 a | 81.59 ± 12.37 | 76.62 ± 8.86 | 75.89 ± 8.33 a |
| WHZ * | 2.67 ± 0.66 a | 0.51 ± 0.89 | 2.62 ± 0.61 | 0.54 ± 0.87 a |
| PM2.5 (μg/m3) | 23.67 ± 6.05 b | 22.68 ± 5.27 | 23.24 ± 5.40 | 21.80 ± 4.61 b |
| Temperature (°C) | 23.53 ± 2.49 | 23.43 ± 2.52 | 23.80 ± 2.13 | 23.46 ± 1.88 |
| Relative Humidity (%) | 73.10 ± 8.08 | 73.18 ± 8.07 | 72.89 ± 4.60 | 72.97 ± 4.65 |
| Poverty (%) | 16.10 ± 7.06 | 16.20 ± 6.83 | 16.50 ± 6.96 | 16.35 ± 6.67 |
| Exposure | Overweight/Obesity n = 65,232 or (95% CI) | Exposure | Overweight/Obesity n = 40,866 or (95% CI) |
|---|---|---|---|
| Extrauterine PM2.5 | 1.57 (1.51–1.63) | Intrauterine PM2.5 | 1.99 (1.88–2.12) |
| Relative Humidity (%) | Relative Humidity (%) | ||
| Q1 (54.20–66.67) | 1.0 | Q1 (61.18–69.54) | 1.0 |
| Q2 (66.68–72.63) | 0.89 (0.83–0.95) | Q2 (69.55–73.13) | 0.967 (0.89–1.05) |
| Q3 (72.64–80.06) | 0.79 (0.71–0.89) | Q3 (73.14–75.71) | 0.90 (0.81–0.99) |
| Q4 (80.07–89.90) | 0.82 (0.70–0.96) | Q4 (75.72–86.38) | 0.86 (0.77–0.97) |
| Temperature (°C) | Temperature (°C) | ||
| Q1 (17.09–21.58) | 1.0 | Q1 (18.53–22.35) | 1.0 |
| Q2 (21.59–23.26) | 0.95 (0.90–1.00) | Q2 (22.36–23.59) | 0.79 (0.75–0.85) |
| Q3 (23.27–25.49) | 0.85 (0.79–0.91) | Q3 (23.60–24.80) | 0.83 (0.77–0.89) |
| Q4 (25.50–30.36) | 0.77 (0.71–0.84) | Q4 (24.81–29.41) | 0.93 (0.85–1.01) |
| Poverty (%) | Poverty (%) | ||
| Q1 (0.17–10.48) | 1.0 | Q1 (0.17–10.48) | 1.0 |
| Q2 (10.49–16.84) | 0.80 (0.77–0.84) | Q2 (10.49–16.84) | 0.81 (0.76–0.86) |
| Q3 (16.85–22.04) | 0.74 (0.70–0.77) | Q3 (16.85–22.80) | 0.68 (0.64–0.72) |
| Q4 (22.05–29.09) | 0.75 (0.71–0.79) | Q4 (22.81–29.09) | 0.73 (0.69–0.78) |
| PM2.5 Quartiles | PM2.5 Quartiles | ||
| Q1 (14.36–18.63) | 1.0 | Q1 (15.73–18.61) | 1.0 |
| Q2 (18.64–20.49) | 0.83 (0.79–0.87) | Q2 (18.62–19.82) | 0.86 (0.81–0.92) |
| Q3 (20.50–27.37) | 0.97 (0.92–1.03) | Q3 (19.83–26.88) | 1.24 (1.15–1.33) |
| Q4 (27.38–46.07) | 1.52 (1.43–1.62) | Q4 (26.89–40.44) | 1.99 (1.84–2.16) |
| Exposure | Male n = 34,514 or (95% CI) | Exposure | Female n = 30,718 or (95% CI) |
|---|---|---|---|
| PM2.5 | 1.58 (1.50–1.67) | PM2.5 | 1.56 (1.47–1.64) |
| Relative Humidity (%) | Relative Humidity (%) | ||
| Q1 (54.37–66.67) | 1.0 | Q1 (54.20–66.66) | 1.0 |
| Q2 (66.68–72.64) | 0.86 (0.78–0.94) | Q2 (66.67–72.60) | 0.92 (0.84–1.02) |
| Q3 (72.65–80.07) | 0.79 (0.68–0.92) | Q3 (72.61–80.06) | 0.79 (0.67–0.93) |
| Q4 (80.08–89.70) | 0.84 (0.68–1.04) | Q4 (80.07–89.90) | 0.79 (0.63–0.99) |
| Temperature (°C) | Temperature (°C) | ||
| Q1 (17.10–21.58) | 1.0 | Q1 (17.09–21.59) | 1.0 |
| Q2 (21.59–23.26) | 0.94 (0.87–1.01) | Q2 (21.60–23.25) | 0.96 (0.88–1.04) |
| Q3 (23.27–25.49) | 0.83 (0.753–0.92) | Q3 (23.26–25.47) | 0.87 (0.79–0.97) |
| Q4 (25.50–30.35) | 0.76 (0.67–0.86) | Q4 (25.48–30.36) | 0.79 (0.69–0.90) |
| Poverty (%) | Poverty (%) | ||
| Q1 (0.17–10.48) | 1.0 | Q1 (0.17–10.48) | 1.0 |
| Q2 (10.49–16.84) | 0.83 (0.78–0.88) | Q2 (10.49–16.84) | 0.78 (0.72–0.83) |
| Q3 (16.85–22.04) | 0.76 (0.71–0.82) | Q3 (16.85–22.04) | 0.71 (0.66–0.76) |
| Q4 (22.05–29.09) | 0.77 (0.72–0.83) | Q4 (22.05–29.09) | 0.72 (0.67–0.78) |
| Exposure | O/O Aged 6 to 11 | O/O Aged 12 to 35 | O/O Aged 36 to 59 |
|---|---|---|---|
| n = 21,918 or (95% CI) | n = 29,146 or (95% CI) | n = 14,174 or (95% CI) | |
| Extrauterine PM2.5 | 3.07 (2.84–3.31) | 1.31 (1.24–1.38) | 0.98 (0.91–1.01) |
| Relative Humidity (%) | |||
| Q1 | 1.0 | 1.0 | 1.0 |
| Q2 | 0.87 (0.77–0.99) | 0.81 (0.73–0.89) | 1.07 (0.91–1.25) |
| Q3 | 0.72 (0.59–0.89) | 0.71 (0.60–0.84) | 1.00 (0.79–1.27) |
| Q4 | 0.75 (0.56–1.00) | 0.79 (0.63–1.00) | 0.89 (0.65–1.23) |
| Temperature (°C) | |||
| Q1 | 1.0 | 1.0 | 1.0 |
| Q2 | 0.97 (0.88–1.07) | 0.94 (0.87–1.02) | 0.94 (0.84–1.07) |
| Q3 | 0.83 (0.73–0.94) | 0.81 (0.73–0.90) | 0.94 (0.81–1.09) |
| Q4 | 0.71 (0.60–0.83) | 0.72 (0.63–0.82) | 0.94 (0.78–1.14) |
| Poverty (%) | |||
| Q1 | 1.0 | 1.0 | 1.0 |
| Q2 | 0.72 (0.66–0.78) | 0.84 (0.79–0.91) | 0.88 (0.80–0.98) |
| Q3 | 0.58 (0.53–0.64) | 0.76 (0.70–0.81) | 0.96 (0.86–1.07) |
| Q4 | 0.70 (0.64–0.77) | 0.74 (0.69–0.80) | 0.95 (0.85 -1.06) |
| PM2.5 Quartiles | |||
| Q1 | 1.0 | 1.0 | 1.0 |
| Q2 | 0.79 (0.72–0.86) | 0.78 (0.73–0.84) | 1.03 (0.92–1.14) |
| Q3 | 1.27 (1.16–1.40) | 0.78 (0.72–0.85) | 0.98 (0.87–1.11) |
| Q4 | 3.33 (2.98–3.72) | 1.11 (1.01–1.21) | 0.99 (0.87–1.12) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paz-Aparicio, V.M.; Tapia, V.; Vasquez-Apestegui, B.V.; Steenland, K.; Gonzales, G.F. Intrauterine and Extrauterine Environmental PM2.5 Exposure Is Associated with Overweight/Obesity (O/O) in Children Aged 6 to 59 Months from Lima, Peru: A Case-Control Study. Toxics 2022, 10, 487. https://doi.org/10.3390/toxics10080487
Paz-Aparicio VM, Tapia V, Vasquez-Apestegui BV, Steenland K, Gonzales GF. Intrauterine and Extrauterine Environmental PM2.5 Exposure Is Associated with Overweight/Obesity (O/O) in Children Aged 6 to 59 Months from Lima, Peru: A Case-Control Study. Toxics. 2022; 10(8):487. https://doi.org/10.3390/toxics10080487
Chicago/Turabian StylePaz-Aparicio, Valeria M., Vilma Tapia, Bertha Vanessa Vasquez-Apestegui, Kyle Steenland, and Gustavo F. Gonzales. 2022. "Intrauterine and Extrauterine Environmental PM2.5 Exposure Is Associated with Overweight/Obesity (O/O) in Children Aged 6 to 59 Months from Lima, Peru: A Case-Control Study" Toxics 10, no. 8: 487. https://doi.org/10.3390/toxics10080487