
Factors Associated with Not Receiving a Booster Dose of COVID-19 Vaccine in Peru

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
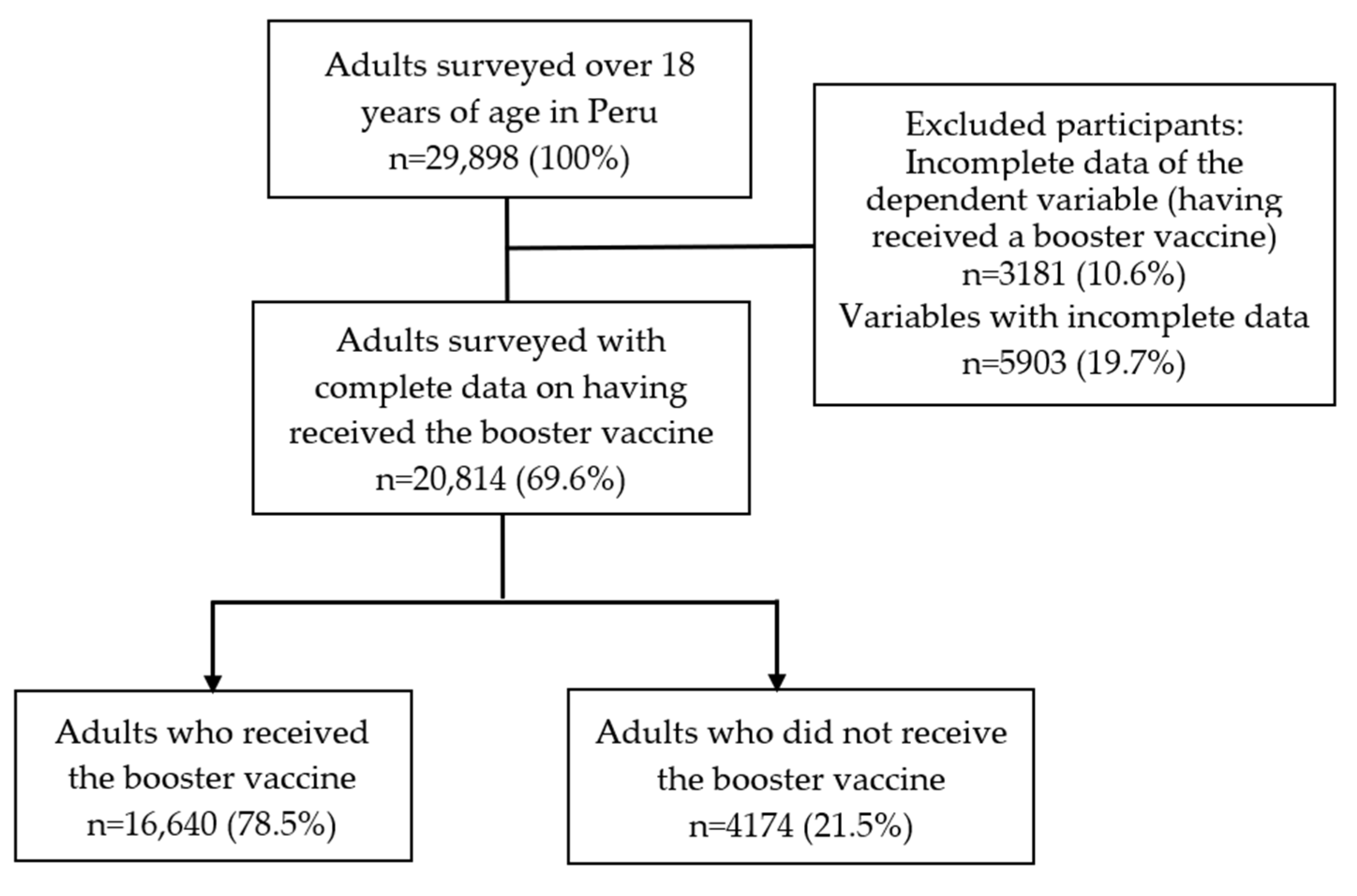
2.2. Population, Sample, and Sampling
2.3. Sample and Sampling
2.4. Questionnaire
2.5. Variables
2.5.1. Outcome Variable: Not Receiving a Booster Dose against COVID-19
2.5.2. Independent Variables
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Characteristics of the Study Sample
3.2. Bivariate Analysis according to Not Having Received the Booster Vaccine against COVID-19
3.3. Factors Associated with Not Having Received the Booster Vaccine against COVID-19
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johns Hopkins University. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 2 May 2022).
- World Health Organization. Vaccines and Immunization. Available online: https://www.who.int/health-topics/vaccines-and-immunization#tab=tab_1 (accessed on 27 April 2022).
- Li, X.; Mukandavire, C.; Cucunubá, Z.M.; Londono, S.E.; Abbas, K.; Clapham, H.E.; Jit, M.; Johnson, H.L.; Papadopoulos, T.; Vynnycky, E.; et al. Estimating the Health Impact of Vaccination against Ten Pathogens in 98 Low-Income and Middle-Income Countries from 2000 to 2030: A Modelling Study. Lancet 2021, 397, 398–408. [Google Scholar] [CrossRef]
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global Impact of the First Year of COVID-19 Vaccination: A Mathematical Modelling Study. Lancet Infect. Dis. 2022, 22, 174–175. [Google Scholar] [CrossRef]
- Krause, P.R.; Fleming, T.R.; Peto, R.; Longini, I.M.; Figueroa, J.P.; Sterne, J.A.C.; Cravioto, A.; Rees, H.; Higgins, J.P.T.; Boutron, I.; et al. Considerations in Boosting COVID-19 Vaccine Immune Responses. Lancet 2021, 398, 1377–1380. [Google Scholar] [CrossRef]
- World Health Organization. Interim Statement on Booster Doses for COVID-19 Vaccination—Update 4 October 2021. Available online: https://www.who.int/news/item/04-10-2021-interim-statement-on-booster-doses-for-covid-19-vaccination (accessed on 2 May 2022).
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of Effectiveness of Vaccines against SARS-CoV-2 Infection and COVID-19 Disease: Results of a Systematic Review and Meta-Regression. Lancet 2022, 399, 924–944. [Google Scholar] [CrossRef]
- Mbaeyi, S.; Oliver, S.E.; Collins, J.P.; Godfrey, M.; Goswami, N.D.; Hadler, S.C.; Jones, J.; Moline, H.; Moulia, D.; Reddy, S.; et al. The Advisory Committee on Immunization Practices’ Interim Recommendations for Additional Primary and Booster Doses of COVID-19 Vaccines—United States, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1545–1552. [Google Scholar] [CrossRef]
- Moreira, E.D.; Kitchin, N.; Xu, X.; Dychter, S.S.; Lockhart, S.; Gurtman, A.; Perez, J.L.; Zerbini, C.; Dever, M.E.; Jennings, T.W.; et al. Safety and Efficacy of a Third Dose of BNT162b2 COVID-19 Vaccine. N. Engl. J. Med. 2022, 386, 1910–1921. [Google Scholar] [CrossRef]
- Jara, A.; Undurraga, E.A.; Zubizarreta, J.R.; González, C.; Pizarro, A.; Acevedo, J.; Leo, K.; Paredes, F.; Bralic, T.; Vergara, V.; et al. Effectiveness of Homologous and Heterologous Booster Doses for an Inactivated SARS-CoV-2 Vaccine: A Large-Scale Prospective Cohort Study. Lancet Glob. Health 2022, 10, e798–e806. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against COVID-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Sachdeva, R.; Gower, C.; Ramsay, M.; Lopez Bernal, J. Effectiveness of COVID-19 Booster Vaccines against COVID-19-Related Symptoms, Hospitalization and Death in England. Nat. Med. 2022, 28, 831–837. [Google Scholar] [CrossRef]
- Ministerio de Salud. Sala Situacional COVID-19 Perú. Available online: https://covid19.minsa.gob.pe/sala_situacional.asp (accessed on 24 August 2020).
- Ministerio de Salud. Vacuna COVID-19 En El Peru. Available online: https://www.minsa.gob.pe/reunis/data/vacunas-covid19.asp (accessed on 27 April 2022).
- El Peruano COVID-19: Dosis de Refuerzo Se Aplicará Desde Este Viernes 26 a Personas de 18 Años o Más. Available online: https://elperuano.pe/noticia/134142-covid-19-dosis-de-refuerzo-se-aplicara-desde-este-viernes-26-a-personas-de-18-anos-o-mas (accessed on 27 June 2022).
- Barkay, N.; Cobb, C.; Eilat, R.; Galili, T.; Haimovich, D.; LaRocca, S.; Morris, K.; Sarig, T. Weights and Methodology Brief for the COVID-19 Symptom Survey by University of Maryland and Carnegie Mellon University, in Partnership with Facebook. arXiv 2020, arXiv:2009.14675. [Google Scholar]
- Herrera-Añazco, P.; Urrunaga-Pastor, D.; Benites-Zapata, V.A.; Bendezu-Quispe, G.; Toro-Huamanchumo, C.J.; Hernandez, A.V. Gender Differences in Depressive and Anxiety Symptoms During the First Stage of the COVID-19 Pandemic: A Cross-Sectional Study in Latin America and the Caribbean. Front. Psychiatry 2022, 13, 727034. [Google Scholar]
- Riehm, K.E.; Badillo Goicoechea, E.; Wang, F.M.; Kim, E.; Aldridge, L.R.; Lupton-Smith, C.P.; Presskreischer, R.; Chang, T.-H.; LaRocca, S.; Kreuter, F.; et al. Association of Non-Pharmaceutical Interventions to Reduce the Spread of SARS-CoV-2 With Anxiety and Depressive Symptoms: A Multi-National Study of 43 Countries. Int. J. Public Health 2022, 67, 1604430. [Google Scholar] [CrossRef]
- Herrera-Añazco, P.; Uyen-Cateriano, Á.; Urrunaga-Pastor, D.; Bendezu-Quispe, G.; Toro-Huamanchumo, C.J.; Rodríguez-Morales, A.J.; Hernández, A.V.; Benites-Zapata, V.A. Prevalence and factors associated with the intention to be vaccinated against COVID-19 in Peru. Rev. Peru. Med. Exp. Salud Publica 2021, 38, 381–390. [Google Scholar] [CrossRef]
- Herrera-Añazco, P.; Urrunaga-Pastor, D.; Benites-Zapata, V.A.; Bendezu-Quispe, G.; Toro-Huamanchumo, C.J.; Hernandez, A.V. COVID-19 Symptomatology and Compliance with Community Mitigation Strategies in Latin America Early during the COVID-19 Pandemic. Prev. Med. Rep. 2022, 25, 101665. [Google Scholar] [CrossRef]
- Urrunaga-Pastor, D.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Toro-Huamanchumo, C.J.; Rodriguez-Morales, A.J.; Hernandez, A.V.; Benites-Zapata, V.A.; Bendezu-Quispe, G. Prevalence and Factors Associated with Parents’ Non-Intention to Vaccinate Their Children and Adolescents against COVID-19 in Latin America and the Caribbean. Vaccines 2021, 9, 1303. [Google Scholar] [CrossRef]
- Benites-Zapata, V.A.; Urrunaga-Pastor, D.; Solorzano-Vargas, M.L.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Bendezu-Quispe, G.; Toro-Huamanchumo, C.J.; Hernandez, A.V. Prevalence and Factors Associated with Food Insecurity in Latin America and the Caribbean during the First Wave of the COVID-19 Pandemic. Heliyon 2021, 7, e08091. [Google Scholar] [CrossRef]
- Statista Research Department América Latina: Dosis y Pauta de Tercera Vacunación Contra La COVID-19 Por País 2022. Available online: https://es.statista.com/estadisticas/1282619/dosis-y-pauta-de-tercera-vacunacion-contra-la-covid-19-por-pais-america-latina/ (accessed on 27 April 2022).
- BBC News Mundo Vacuna Contra La COVID-19: Los Países de América Latina Que Administran Una Tercera Dosis de Refuerzo. Available online: https://www.bbc.com/mundo/noticias-america-latina-58152738 (accessed on 27 April 2022).
- Horwitz, L.; Zissis, C. Graficando La Vacunación Contra El COVID-19 En América Latina. Available online: https://www.as-coa.org/articles/graficando-la-vacunacion-contra-el-covid-19 (accessed on 27 April 2022).
- The Lancet Infectious Diseases. COVID-19 Vaccine Equity and Booster Doses. Lancet Infect. Dis. 2021, 21, 1193. [Google Scholar] [CrossRef]
- March Cerdà, J.C. Pacientes empoderados para una mayor confianza en el sistema sanitario. Rev. Calid. Asist. 2015, 30, 1–3. [Google Scholar] [CrossRef]
- Ministerio de Salud. Campaña Nacional de Vacunación Contra La COVID-19. Available online: https://www.gob.pe/institucion/pcm/campa%C3%B1as/3451-campana-nacional-de-vacunacion-contra-la-covid-19 (accessed on 4 May 2022).
- Ministerio de Salud. Protocolo de Aplicación de Dosis de Refuerzo de La Vacuna Contra La COVID-19 Para Personas de 60 Años a Más. Available online: https://cdn.www.gob.pe/uploads/document/file/2332692/Protocolo.pdf (accessed on 4 May 2022).
- Ministerio de Salud. Dosis de Refuerzo En La Campaña de Vacunación Contra SARS-Cov-2 En Chile. Available online: https://www.minsal.cl/wp-content/uploads/2021/08/Dosis-de-refuerzo-en-la-campa%C3%B1a-de-vacunaci%C3%B3n-contra-SARS-CoV-2-en-Chile.pdf (accessed on 27 April 2022).
- Lossio, J. COVID-19 en el Perú: Respuestas estatales y sociales. Hist. Ciênc. Saúde 2021, 28, 581–585. [Google Scholar] [CrossRef]
- Herrera-Añazco, P.; Uyen-Cateriano, A.; Mezones-Holguin, E.; Taype-Rondan, A.; Mayta-Tristan, P.; Malaga, G.; Hernandez, A.V. Some Lessons That Peru Did Not Learn before the Second Wave of COVID-19. Int. J. Health Plann. Manag. 2021, 36, 995–998. [Google Scholar] [CrossRef]
- López, M.G.F.; Tarazona, A.S.; Cruz-Vargas, J.A.D.L.; López, M.G.F.; Tarazona, A.S.; Cruz-Vargas, J.A.D.L. Distribución Regional de Mortalidad Por COVID-19 En Perú. Rev. Fac. Med. Hum. 2021, 21, 326–334. [Google Scholar] [CrossRef]
- Ramírez-Soto, M.C.; Ortega-Cáceres, G.; Arroyo-Hernández, H. Excess All-Cause Deaths Stratified by Sex and Age in Peru: A Time Series Analysis during the COVID-19 Pandemic. BMJ Open 2022, 12, e057056. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística e Informática. Características de La Población. Available online: https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1539/cap01.pdf (accessed on 27 April 2022).
- Instituto Nacional de Estadística e Informática. Perú: Indicadores de Educación Por Departamento 2009–2019. Available online: https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1751/libro.pdf (accessed on 27 April 2022).
- Instituto Nacional de Estadística e Informática. Indicadores de Empleo Ingreso Por Departamento 2007–2017. Available online: https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1537/libro.pdf (accessed on 27 April 2022).
- Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef]
- Haktanir, A.; Can, N.; Seki, T.; Kurnaz, M.F.; Dilmaç, B. Do We Experience Pandemic Fatigue? Current State, Predictors, and Prevention. Curr. Psychol. 2021, 1–12. [Google Scholar] [CrossRef]
- Meacci, L.; Primicerio, M. Pandemic Fatigue Impact on COVID-19 Spread: A Mathematical Modelling Answer to the Italian Scenario. Results Phys. 2021, 31, 104895. [Google Scholar] [CrossRef]
- Martinez-Garcia, M.; Rabasa, A.; Barber, X.; Polotskaya, K.; Roomp, K.; Oliver, N. Key Factors Affecting People’s Unwillingness to Be Confined during the COVID-19 Pandemic in Spain: A Large-Scale Population Study. Sci. Rep. 2021, 11, 18626. [Google Scholar] [CrossRef]
- The COCONEL Group. A Future Vaccination Campaign against COVID-19 at Risk of Vaccine Hesitancy and Politicisation. Lancet Infect. Dis. 2020, 20, 769–770. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.-F.; Lee, H.Y.; AbuBakar, S. The Use of the Health Belief Model to Assess Predictors of Intent to Receive the COVID-19 Vaccine and Willingness to Pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Ministerio de Salud. Protocolo de Aplicación de Tercera y Cuarta Dosis Para La Vacunación Contra La COVID-19. Available online: https://www.gob.pe/institucion/minsa/informes-publicaciones/2888984-protocolo-de-aplicacion-de-tercera-y-cuarta-dosis-para-la-vacunacion-contra-la-covid-19 (accessed on 27 April 2022).


{kind=link}
| Characteristics | n | % * | 95%CI * |
|---|---|---|---|
| Gender | |||
| Male | 10,914 | 48.7 | 44.8–52.7 |
| Female | 9900 | 51.3 | 47.3–55.2 |
| Age (years) | |||
| 18–24 | 3458 | 15.8 | 13.8–18.1 |
| 25–34 | 4455 | 22.1 | 21.2–23.0 |
| 35–44 | 4175 | 20.0 | 19.1–20.9 |
| 45–54 | 3933 | 18.6 | 18.0–19.3 |
| 55–64 | 3070 | 12.2 | 11.4–13.1 |
| 65–74 | 1478 | 9.9 | 8.5–11.5 |
| 75 years or older | 245 | 1.4 | 0.9–2.1 |
| Area of residence | |||
| City | 17,991 | 83.2 | 73.0–90.1 |
| Town | 1721 | 10.0 | 5.8–16.7 |
| Village or rural area | 1102 | 6.8 | 4.2–10.8 |
| Educational level | |||
| Primary school or less | 341 | 2.1 | 1.7–2.7 |
| Secondary school—pre-university | 7713 | 39.1 | 37.0–41.3 |
| University | 9784 | 45.8 | 44.2–47.4 |
| Postgraduate | 2976 | 12.9 | 12.0–13.9 |
| Employment | |||
| No | 8159 | 41.5 | 40.4–42.6 |
| Yes | 12,655 | 58.5 | 57.4–59.6 |
| Comorbidities | |||
| None | 16,694 | 81.1 | 78.8–83.2 |
| 1 to 2 | 3785 | 17.2 | 15.4–19.2 |
| Greater than or equal to 3 | 335 | 1.6 | 1.3–2.1 |
| History of COVID-19 | |||
| No | 10,304 | 49.8 | 48.5–51.1 |
| Yes | 10,510 | 50.2 | 48.9–51.5 |
| Having received a booster | |||
| Yes | 16,640 | 78.5 | 74.8–81.7 |
| No | 4174 | 21.5 | 18.3–25.2 |
| Characteristics | Not having Received Booster | ||||||
|---|---|---|---|---|---|---|---|
| Yes | No | p-Value ** | |||||
| n | % * | 95%CI * | n | % * | 95%CI * | ||
| Gender | 0.006 | ||||||
| Male | 8785 | 77.1 | 73.0–80.7 | 2129 | 22.9 | 19.3–27.0 | |
| Female | 7855 | 79.7 | 76.3–82.8 | 2045 | 20.3 | 17.2–23.7 | |
| Age (years) | <0.001 | ||||||
| 18–24 | 2018 | 56.9 | 54.8–58.9 | 1440 | 43.1 | 41.1–45.2 | |
| 25–34 | 3262 | 70.2 | 64.3–75.6 | 1193 | 29.8 | 24.4–35.7 | |
| 35–44 | 3411 | 79.9 | 76.0–83.2 | 764 | 20.1 | 16.8–24.0 | |
| 45–54 | 3459 | 86.6 | 83.8–88.9 | 474 | 13.4 | 11.1–16.2 | |
| 55–64 | 2850 | 91.5 | 88.3–93.8 | 220 | 8.5 | 6.2–11.7 | |
| 65–74 | 1402 | 94.5 | 92.5–95.9 | 76 | 5.5 | 4.1–7.5 | |
| 75 years or older | 238 | 97.7 | 93.9–99.2 | 7 | 2.3 | 0.8–6.1 | |
| Area of residence | <0.001 | ||||||
| City | 14,628 | 80.2 | 77.1–82.9 | 3363 | 19.8 | 17.1–22.9 | |
| Town | 1230 | 70.3 | 67.3–73.1 | 491 | 29.7 | 26.9–32.7 | |
| Village or rural area | 782 | 69.5 | 63.6–74.8 | 320 | 30.5 | 25.2–36.4 | |
| Educational level | <0.001 | ||||||
| Primary school or less | 229 | 70.1 | 64.8–74.9 | 112 | 29.9 | 25.1–35.2 | |
| Secondary school—pre-university | 5747 | 73.1 | 69.5–76.5 | 1966 | 26.9 | 23.5–30.5 | |
| University | 7967 | 80.3 | 76.1–83.9 | 1817 | 19.7 | 16.1–23.9 | |
| Postgraduate | 2697 | 89.5 | 85.5–92.6 | 279 | 10.5 | 7.4–14.5 | |
| Employment | 0.002 | ||||||
| No | 6362 | 77.1 | 72.9–80.9 | 1797 | 22.9 | 19.1–27.1 | |
| Yes | 10,278 | 79.4 | 75.9–82.4 | 2377 | 20.6 | 17.6–24.1 | |
| Comorbidities | <0.001 | ||||||
| None | 13,181 | 77.5 | 73.6–80.9 | 3513 | 22.5 | 19.1–26.4 | |
| 1 to 2 | 3164 | 82.3 | 79.4–84.8 | 621 | 17.7 | 15.2–20.6 | |
| Greater than or equal to 3 | 295 | 87.5 | 83.5–90.6 | 40 | 12.5 | 9.4–16.5 | |
| History of COVID-19 | <0.001 | ||||||
| No | 8515 | 80.8 | 76.8–84.2 | 1789 | 19.2 | 15.8–23.2 | |
| Yes | 8125 | 76.1 | 72.5–79.4 | 2385 | 23.9 | 20.6–27.5 | |
| Characteristics | Crude Model | Adjusted Model | ||||
|---|---|---|---|---|---|---|
| cPR | 95%CI | p-Value | aPR | 95%CI | p-Value | |
| Gender | ||||||
| Male | Ref. | Ref. | ||||
| Female | 0.98 | 0.96–0.99 | 0.008 | 0.97 | 0.96–0.99 | 0.001 |
| Non-binary | ||||||
| Age (years) | Ref. | Ref. | ||||
| 75 years or older | 1.03 | 1.01–1.05 | 0.004 | 1.04 | 1.01–1.06 | 0.002 |
| 65–74 | 1.06 | 1.03–1.09 | <0.001 | 1.06 | 1.03–1.08 | <0.001 |
| 55–64 | 1.11 | 1.09–1.13 | <0.001 | 1.10 | 1.08–1.13 | <0.001 |
| 45–54 | 1.17 | 1.15–1.20 | <0.001 | 1.16 | 1.14–1.19 | <0.001 |
| 35–44 | 1.27 | 1.22–1.31 | <0.001 | 1.26 | 1.21–1.30 | <0.001 |
| 25–34 | 1.40 | 1.36–1.44 | <0.001 | 1.37 | 1.33–1.41 | <0.001 |
| Area of residence | ||||||
| City | Ref. | Ref. | ||||
| Town | 1.08 | 1.05–1.11 | <0.001 | 1.05 | 1.02–1.07 | 0.001 |
| Village or rural area | 1.09 | 1.05–1.12 | <0.001 | 1.06 | 1.03–1.10 | 0.001 |
| Educational level | ||||||
| Postgraduate | Ref. | Ref. | ||||
| University | 1.08 | 1.07–1.10 | <0.001 | 1.03 | 1.02–1.05 | <0.001 |
| Secondary school—pre-university | 1.15 | 1.13–1.17 | <0.001 | 1.07 | 1.05–1.09 | <0.001 |
| Primary school or less | 1.18 | 1.12–1.24 | <0.001 | 1.11 | 1.05–1.18 | <0.001 |
| Employment | ||||||
| Yes | Ref. | Ref. | ||||
| No | 1.02 | 1.01–1.03 | 0.004 | 1.01 | 1.00–1.02 | 0.022 |
| Comorbidities | ||||||
| Greater than or equal to 3 | Ref. | Ref. | ||||
| 1 to 2 | 1.05 | 1.02–1.08 | 0.004 | 1.01 | 0.97–1.05 | 0.562 |
| None | 1.09 | 1.06–1.12 | <0.001 | 1.02 | 0.98–1.06 | 0.327 |
| History of COVID-19 | ||||||
| No | Ref. | Ref. | ||||
| Yes | 1.04 | 1.03–1.05 | <0.001 | 1.03 | 1.01–1.04 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bendezu-Quispe, G.; Caira-Chuquineyra, B.; Fernandez-Guzman, D.; Urrunaga-Pastor, D.; Herrera-Añazco, P.; Benites-Zapata, V.A. Factors Associated with Not Receiving a Booster Dose of COVID-19 Vaccine in Peru. Vaccines 2022, 10, 1183. https://doi.org/10.3390/vaccines10081183
Bendezu-Quispe G, Caira-Chuquineyra B, Fernandez-Guzman D, Urrunaga-Pastor D, Herrera-Añazco P, Benites-Zapata VA. Factors Associated with Not Receiving a Booster Dose of COVID-19 Vaccine in Peru. Vaccines. 2022; 10(8):1183. https://doi.org/10.3390/vaccines10081183
Chicago/Turabian StyleBendezu-Quispe, Guido, Brenda Caira-Chuquineyra, Daniel Fernandez-Guzman, Diego Urrunaga-Pastor, Percy Herrera-Añazco, and Vicente A. Benites-Zapata. 2022. "Factors Associated with Not Receiving a Booster Dose of COVID-19 Vaccine in Peru" Vaccines 10, no. 8: 1183. https://doi.org/10.3390/vaccines10081183