3.1. Main Results
The segmented regression methods revealed a significant effect of the SARS-CoV-2 pandemic on the infectious episodes registered in the primary care clinical histories of a pediatric population. In parallel, a significant decrease was evident in the prescription of antibiotics, especially penicillins, cephalosporins, and macrolides. As for the diseases of Chapter A, seven change points were observed, with a significant jump in September 2020 at the beginning of the school year when diagnostic tests for SARS-CoV-2 became available. Respiratory and otorhinolaryngologic episodes presented six change points, and the segmented regression corresponding with the period of confinement in the first months of 2020 shows a marked downward trend, followed by a more horizontal one.
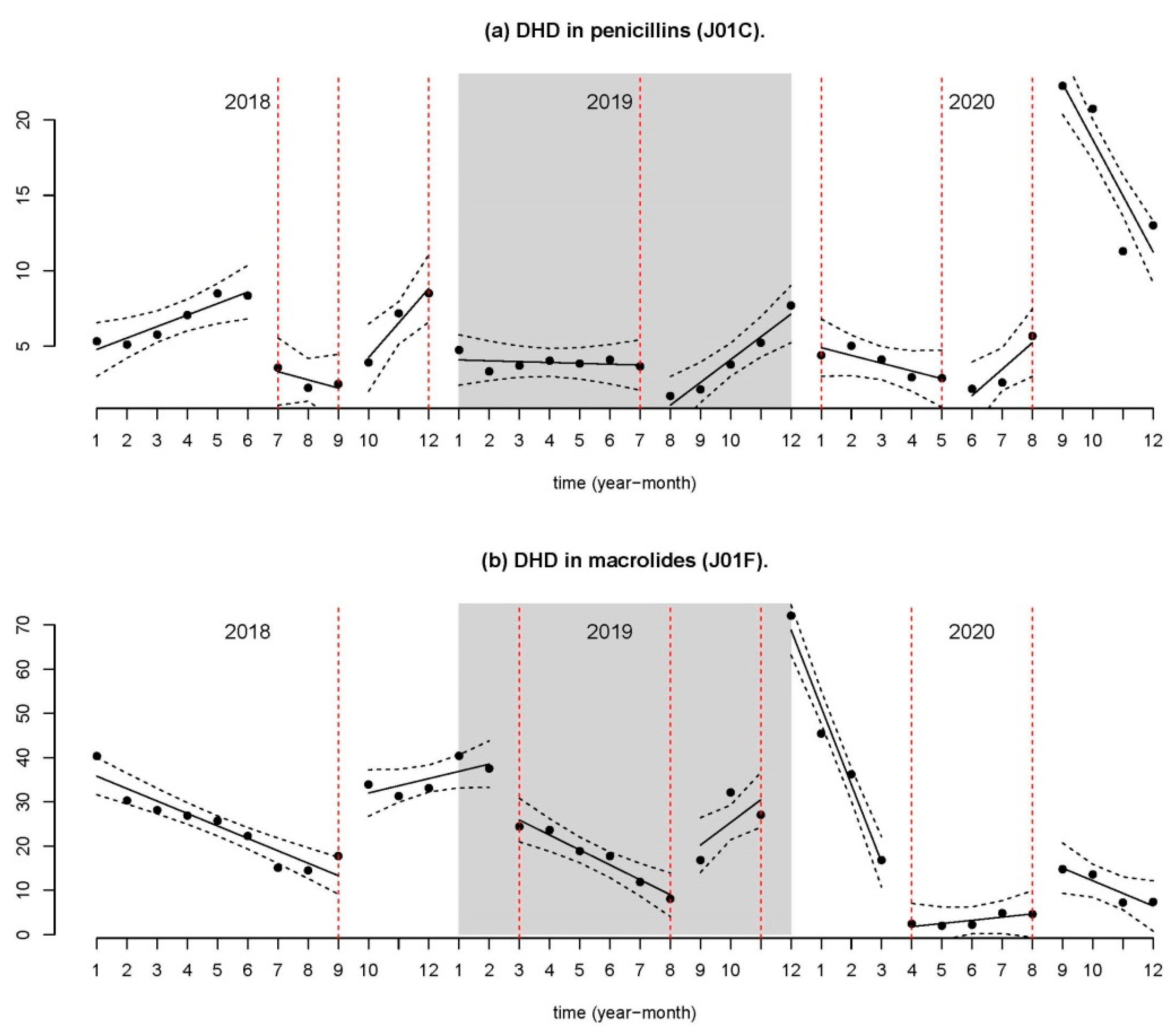
Regarding the consumption of antibiotics (penicillins, cephalosporins, and macrolides), five significant change points were identified. The changes in constants and slopes for the identified segmented regressions followed a similar evolution to that observed in respiratory and otorhinolaryngologic diseases, with a very marked downward trend at the beginning of 2020, followed by a small change in the following months.
3.2. Impact on Infectious Diseases
In the pediatric population under study, a significant decrease was observed in respiratory infections starting in February of 2020 and reaching the largest decline between April and June of the same year (both included), coinciding with the implementation of harsher restriction measures to contain the SARS-CoV-2 pandemic (lockdown, school closing, and restricted mobility), and the resulting social isolation. In September of 2020, a slight increase was noted; this is likely to be related to the return to school activity. However, the levels remained considerably below those of 2018 and 2019.
Respiratory infections are the most common infections occurring during childhood, with children suffering from an average of three to eight upper respiratory infections per year, rates which may be twice as high in infants attending nursery school. Generally speaking, these infections tend to be caused by rhinoviruses, parainfluenza viruses, respiratory syncytial viruses, other coronaviruses, adenoviruses, enteroviruses, and influenza viruses [
12]. The data collected here do not permit the analysis of the etiological agents in most of these infections. Therefore, we are unaware of the individual behavior of each of these viruses in our population. We can, however, infer that a global decline took place in these pathogens, given the major decrease observed in all types of respiratory infections, both upper (upper respiratory viruses, sinusitis, amygdalitis, laryngitis), as well as lower (bronchitis, pneumonia) for all age groups, as compared to the two prior years. One exception is influenza, which maintained a similar incidence as that of the two years prior to the period of study.
As for the other viral infections, the aggregate study of diagnoses from Chapter A of the ICPC (exanthematous viral diseases and SARS-CoV-2) reveals an increase in these illnesses in February of 2020, coinciding with the arrival and initial diagnoses of the SARS-CoV-2 virus in Spain. As of April 2020, this initial increase was followed by a progressive decline, which continued until June of the same year. As of this moment, a notable increase took place in these infections, which continued until the end of the studied period. This pattern is not normal for this group of illnesses, which tend to reveal two seasonal peaks, one in the spring and another in the fall, as observed in the data from 2018 and 2019.
As for the other infections examined, gastrointestinal and urinary tract infections are noteworthy. The former experienced a pronounced decrease as compared to the years prior to the pandemic, while the latter did not undergo any substantial changes, with only a minor decrease being noted in their incidence following the application of the restrictions.
These results are similar to those published by other authors, who have noted that the measures taken to contain the transmission of SARS-CoV-2 led to a global decline in the incidence of transmissible respiratory or contact infections, although they did not affect other infections that are unaffected by social contacts, such as urinary tract infections [
27,
28]. For these other infections, only a mild decline was observed, perhaps due to the lack of physician visits in response to mild and self-treatable symptoms.
The major decline in respiratory infections found in the study population has also been revealed by Haddadin [
29], who noted intense drops in the incidence of acute respiratory infections, including those caused by the respiratory syncytial virus (RSV) and influenza. This latter infection has not been observed in our study. The incidence of influenza remained stable in 2020 as compared to the prior two seasons. This may be due to the fact that the pandemic in Spain took place in March of 2020, after the end of the annual flu epidemic, which took place during the months of January and February. WHO also notes that current influenza surveillance data should be interpreted with caution, as the ongoing SARS-CoV-2 pandemic has influenced the ability to seek medical assistance, affected staffing, and led to changes in priorities, as well as the ability to perform tests. This distortion continued at the beginning of the 2020–2021 flu season, forcing a rethinking and adaptation of influenza surveillance, following the international recommendations of the European Center for Disease Prevention and Control (ECDC) and the World Health Organization (WHO) [
17].
Rius-Peris and Britton [
30,
31] reported a notable decline in admittance and assistance to urgent care due to bronchiolitis (caused by RSV) and a change in seasonality [
29,
30], which was also seen in other respiratory viruses [
32]. Rhinovirus, however, which does not have a lipid coating, and therefore does not respond as well to hand hygiene for its prevention, continued to circulate atypically and was the agent responsible for most of the bronchiolitis cases in the 2020–2021 season [
30].
Another factor influencing the decline in the registration of infections may be the significant decrease in demand for pediatric care. Numerous authors [
28,
33,
34] have expressed their concern due to a noted hesitancy in the seeking of healthcare assistance by parents and caregivers, which was most likely due to a fear of exposure to coronavirus and limited access to primary care services, potentially delaying the diagnosis of other illnesses.
In addition to the reduced number of respiratory and other viral infections, this study demonstrated a major global decline in the prescription of antibiotics in primary care. This decrease continued throughout the study period and increased during the second quarter of 2020, coinciding with the at-home lockdown and stricter containment measures implemented during the pandemic. The most affected antibiotics are those typically used to treat respiratory infections, especially broad-spectrum penicillins, mainly amoxicillin, and combinations of penicillins and beta-lactamase inhibitors. It is interesting to note that the prescription of macrolides, especially azithromycin, despite being a treatment used in SARS-CoV-2 infections during the initial phase of the pandemic, revealed a significant reduction in use. Numerous studies have revealed that many COVID-19 patients received antibiotics, especially early on in the pandemic, and that these were mainly adults with comorbidities (75%). Children received lower rates (57%) [
18,
23,
35,
36].
Most bacterial infections occurring during pediatric ages can be treated in an outpatient manner through the prescription of oral antibiotics. These prescriptions tend to be written in primary and urgent care services, mainly for respiratory infections. This is the main cause of the inappropriate use of antibiotics [
18,
23,
35,
36,
37]. In Spain, the age group that consumes the most antibiotics is that of 0 to 4 years, with an exposure rate of 58.8%, generally associated with inappropriate indication. The most commonly used antibiotics are amoxicillin and amoxicillin with clavulanic acid, with a tendency to increase the use of amoxicillin on its own. The second most commonly prescribed antibiotics are first- and second-generation macrolides and cephalosporins, with both of these experiencing a major decline in the rate of their prescription [
32].
3.3. Impact on the Dispensing of Antibiotics
Data from this study on the consumption of antibiotics reveal that those from the J1C group (penicillins) are the most frequently used in all of the study years, followed by macrolides. This coincides with prior research [
38].
A significant decline was not seen in the prescription of other antibiotics that are commonly used in non-respiratory infections (i.e., urinary tract infections), such as third-generation cotrimoxazole or cephalosporins, such as cefixime.
On the other hand, a minor increase was found in the use of tetracyclines, despite the fact that their use is quite limited in pediatrics, given their contraindication in children under the age of 8, their secondary effects, and the infrequency of the pathologies for which they are used.
Our data were compared with those published by the Spanish Agency of Medicines, on a national level (PRAN) [
7], to verify whether or not there was support for the hypothesis regarding the declined use of antibiotics in 2020, secondary to the decrease in respiratory infections, as occurred in the Vigo health area. The data collected on a national level include adult and pediatric patients, as well as prescriptions from hospitals and private healthcare services. Therefore, the figures in our context are lower for all groups. The decrease in the use of antibiotics is clear for all groups, both on a national and local level, except for the J01E (trimethoprim and combinations) and J01X groups, which did not vary. This is consistent with the stability of the incidence of urinary infections and subsidiary pathologies treated with these therapeutic groups.
Divergence is evident in the use of antibiotics from group J01A (tetracyclines). The increased use of tetracyclines in the age group of 10 to 14 has been seen in our health area, but has not been observed on a national level. This may be related to the mandatory use of face masks by children over the age of 6, resulting in an increased number of cases of acne (the so-called maskne) [
39]. The term maskne is used to refer to the acne resulting from the use of face masks by patients who did not previously suffer from this condition, since an area of heat, humidity, and friction is created, occluding the hair follicles and favoring the appearance of acne. This may have resulted in an increase in the prescription of tetracyclines for its treatment.
It is also necessary to consider the influence of telephone consultations in the prescription profiles, as compared to the face-to-face consultations. Studies comparing telephone care and in-person visits indicate that the former increases the number of follow-up consultations and the inappropriate prescription of antibiotics; however, additional studies are necessary in order to confirm the influence of telemedicine on this these types of prescriptions [
40,
41,
42].
This decreased use of antibiotics has also been found in 25 other European countries [
43], with the exception of Bulgaria, in which an increase took place in 2020. As noted in our study, the largest decrease took place in the use of penicillins and beta-lactams, drugs prescribed for respiratory infections, which is in line with the decline in the rate of these infections in the European Union (European Centre for Disease Prevention and Control) [
44]. The theory of the ecological niche of viruses, according to which a dynamic variation of the ecosystem would be produced by being replaced by other viruses through the phenomena of competition or cooperation between them, would also have affected the circulation of SARS-CoV-2 in the year 2020, and would have caused the replacement of infections by other respiratory viruses [
45].
In the infant and youth populations, there was a decreased circulation of viruses and bacteria as a result of the SARS-CoV-2 pandemic. There was also a decline in the consumption of antibiotics and a decrease in flare-ups of asthma in 2020 [
27]. On the other hand, a significant increase was seen in psychosocial issues, such as anxiety, self-destructive behaviors, eating disorders, substance abuse, and new technology addictions. It should also be noted that restriction measures may cause increased susceptibility to other infective agents, which may result in more intense future or unexpected outbreaks [
30]. Therefore, specific studies should assess which measures are more appropriate in a similar situation and which should be continued from the current practices (such as handwashing, staying at home when having symptoms of illness, and following clinical practice guidelines to ensure the rational use of antibiotics).
3.4. Limitations and Strengths
All of the primary care professionals used the same electronic clinical history and its use is universal in all visits. Furthermore, it may be considered representative of the infective episodes and the consumption of J01, given that 93.31% of the population has a digital clinical history on the National Healthcare System.
The main limitation of this study is the variability in the coding used by professionals and the lack of individual validation of the study events. However, we can assess its integrity and validity by comparing the rates obtained with those of the medical literature, or from their integration in the computerized system of primary care and public health. Thus, in the case of diseases of mandatory declaration (EDO, based on their initials in Spanish), in Galicia, the inclusion of episodes that have been recorded in the primary care clinical history of the epidemiological surveillance system of the EDO is standardized.
The data used in this study correspond to the outpatient use of J01 medications, not considering the consumption derived from hospital use, in admitted patients, or those dispensed to outpatients and in socio-healthcare establishments from hospital pharmacy services. It also excludes consumption via private prescriptions and mutual insurance agencies that is not invoiced through the SNS. It should also be noted that invoicing data do not correspond precisely with the data on the prescriptions, since said prescriptions may not be dispensed. Furthermore, not all medications dispensed by the pharmacies are actually taken by the patients.
ITS are increasingly recognized as designs that, when properly designed and analyzed, can provide reliable effect estimates on the impact of interventions in situations where randomization is not feasible [
24]. Despite recent publications containing detailed guidance on how to conduct ITS studies [
46], reporting on the design features and results of ITS studies is still lacking [
47]. Among other noteworthy aspects, the specification of the time interval (months), the outcome (ratio or DHD), shape model (level change and slope change), autocorrelation application, and effect measures (level change and slope change, including
p and confidence intervals) are specified. It was not possible to analyze a control group, as recommended in the literature. This was not available anywhere, on a global level.


 ,
, 

{kind=link}
{kind=link}
{kind=link}


