
A Systematic Review of Sleep–Wake Disorder Diagnostic Criteria Reliability Studies

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
- Evaluation of sleep–wake disorder diagnosis criteria of the different versions of the DSM, ICSD, and ICD.
- Evaluation of diagnostic criteria based on clinical interviews or on clinical data recording.
- Reliability, defined as the degree of agreement among raters, measured by the Cohen’s kappa coefficient.
- Full original research papers, published in a peer-reviewed journal, suitable for inclusion in a systematic review and meta-analysis.
- Absence of restriction made on the date of articles included in this review.
- Structured interview containing a single question on which reliability was assessed.
- Self-rated questionnaires developed for the patient to complete by him/herself to assess the presence of sleep symptoms.
- Absence of assessment of Cohen’s kappa coefficient.
- Studies not published in English.
- Studies investigating reliability only of polysomnography scoring.
- Single case studies, conference posters, reviews, meta-analyses, unpublished studies, opinions, and comments.
2.2. Search Strategy and Selection Process
2.3. Data Extraction and Collection
- First Author/Year/Countries of evaluation/Journal;
- Monocentric/Multicentric studies;
- Type and number of different sleep–wake disorders evaluated;
- Classification(s) used for diagnostic criteria and year of publication (ICSD, DSM, ICD).
- 5.
- Number of clinical interviews performed with a patient, i.e., number of times a patient has been interviewed;
- 6.
- Characteristics and number of raters, i.e., type of clinical profession and level of expertise in sleep medicine;
- 7.
- Types of clinical interviews (structured, semi-structured, and unstructured) based on face-to-face or telephone interviews;
- 8.
- Modality of diagnostic conclusion, with the interviewer clinical judgment (i.e., by the interviewer conducting the clinical interview or by the clinician based on clinical data recording) or without the interviewer clinical judgment (i.e., automatically);
- 9.
- Reliability study quality standard criteria, i.e., reliability guidelines (e.g., Guidelines for Reporting Reliability and Agreement Studies (GRRAS)) [22].
- 10.
- Modality of diagnosis comparisons between raters, number of patients interviewed, and number of clinical judgment conclusions given;
- 11.
- Number of Cohen’s kappa coefficients calculated;
- 12.
- Cohen’s kappa coefficient of each of the different sleep–wake disorders studied and number of patients with the diagnosis.
2.4. Synthesis of Results
3. Results
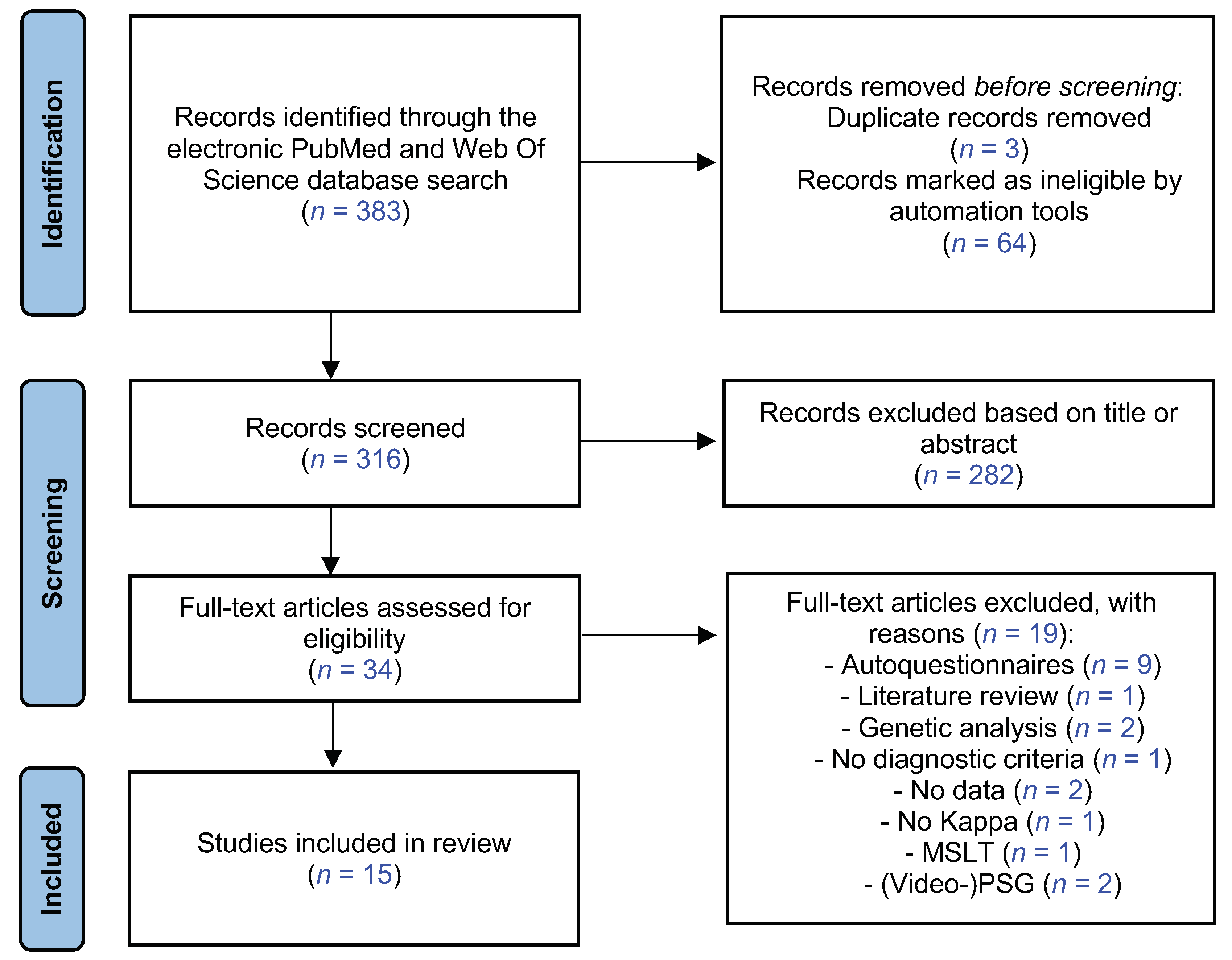
3.1. Results of the Literature Search
3.2. General Description
3.2.1. Description of the Selected Studies
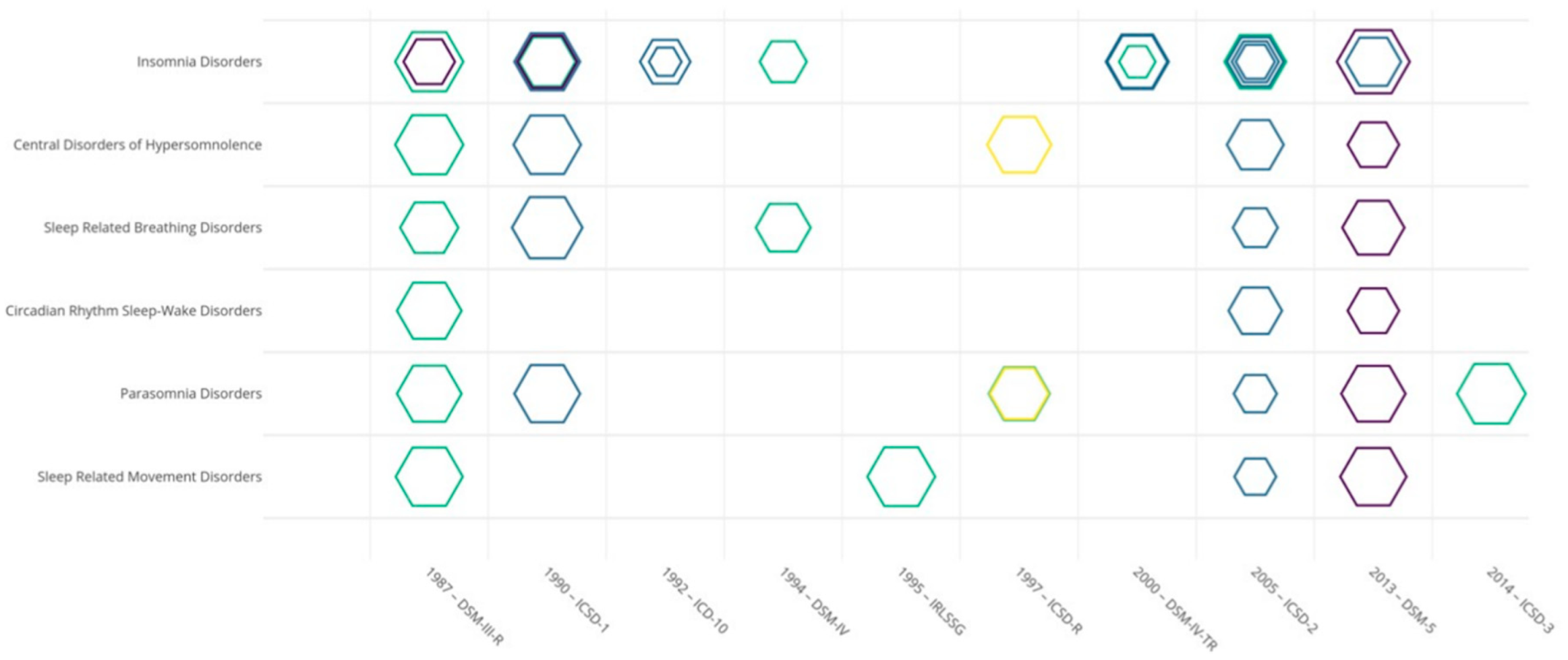
3.2.2. Main Sleep–Wake Disorders Categories and Principal Classifications
3.2.3. Modality of Diagnostic Comparisons among Raters
- The first group of methods (11/15 studies) involved interviewing a patient several times with a specific maximal time interval. These methods have been designed as “test–retest reliability” methods.
- ○
- In seven studies, the patient was interviewed by two interviewers (generally with a good level of expertise in sleep medicine), and reliability was calculated by comparing the sleep–wake disorders diagnosis reached independently by different interviewers (in green in Figure 2 and Table S2) [18,24,26,28,30,31,32]. Types of clinical interviews varied (structured, semi-structured, or unstructured), but all were based on face-to-face interviews performed at two different times. In this methodology to study reliability, the number of clinical interviews performed with a patient corresponds to the number of diagnosis conclusions given by the interviewer, and the modality of diagnostic conclusion was done by the interviewer [18,24,26,30,31] and/or automatically based on the clinical data collected during the interviews [28,32].
- ○
- In four studies, a patient was interviewed independently at two different times by a clinician and an interviewer with a structured questionnaire (in blue in Figure 2 and Table S2). The clinician (sleep specialist) conducted an unstructured face-to-face interview [13,14] or semi-structured telephone interview [25,29]. The structured questionnaire was a standardized assessment based on DISP (n = 1) [14] or the Brief Insomnia Questionnaire (BIQ) (n = 2) [25,29] for telephone interviews and based on Sleep-EVAL (n = 1) for face-to-face interviews [13], conducted by a non-sleep specialist and non-clinician [14]. Reliability was calculated by comparing the sleep–wake disorder diagnosis reached by the clinician conducting the interview and the diagnosis reached automatically based on the questionnaire responses (in blue in Table S2). In this methodology to study reliability, the number of interviews performed with a patient corresponds to the number of diagnosis conclusions given by the clinician conducting the interview and given automatically.
- In the second group of methods (4/15 studies), diagnostic criteria by different clinicians were applied based on previous clinical data recordings. “Clinical data recordings” refer to the collection of data from video (n = 2), audio (n = 1), and medical records (n = 1). These methods have been designed as “joint interrater reliability” methods.
- ○
- Two studies evaluated a single recording of a clinical interview between a patient and a sleep specialist (raters for Vignatelli et al., 2003 [33], and 17 raters for Vignatelli et al., 2022 [34]), which was subsequently evaluated by several clinicians to estimate reliability (in yellow in Figure 2 and Table S2) [33,34]. All recordings were videotapes of semi-structured face-to-face interviews. Reliability was calculated by comparing the sleep–wake disorder diagnosis done by a different clinician watching the same videotapes. In this methodology to study reliability, the number of clinical interviews performed with a patient was inferior to the number of diagnosis conclusions given by the clinician based on videotapes. The methodology of Vignatelli et al., 2002 [34] followed the GRRAS [22].
- ○
- Two studies were based on a patient being interviewed by an interviewer, which was subsequently evaluated by a clinician based on the recordings of the previous clinical interview [20,27] (in purple in Figure 2 and Table S2). The recordings constituted the clinical data of the medical records following an unstructured face-to-face clinical interview conducted by a sleep specialist [27] or the audio recording of a structured interview following a clinical telephone interview conducted by a non-sleep specialist and non-clinician [20]. Reliability was calculated by comparing the sleep–wake disorder diagnosis reached by the clinician conducting the interview [27] or automatically [20], and by the clinician based on the recording clinical data [20,27]. In this methodology to study reliability, the number of clinical interviews performed with a patient was two times inferior to the number of diagnosis conclusions given.
3.3. Cohen’s Kappa Coefficients of the Main Sleep–Wake Disorder Categories
- -
- -
- -
- -
- -
- -
3.4. Reliability Methods for the Main Sleep–Wake Disorder Categories
4. Discussion
4.1. Study of Reliability of Sleep–Wake Disorder Diagnosis Criteria
4.2. Methodology of Sleep–Wake Disorder Reliability Studies
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Kales, A.; Kales, J.D. Sleep Disorders. N. Engl. J. Med. 1974, 290, 487–499. [Google Scholar] [CrossRef]
- Association of Sleep Disorders Centers. Diagnostic Classification of the Sleep and Arousal Disorders; Association of Sleep Disorders Centers: New York, NY, USA, 1979. [Google Scholar]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. International Classification of Diseases 11th Edition (ICD-11). In Encyclopedia of Personality and Individual Differences; Springer International Publishing: Cham, Switzerland, 2017; pp. 1–6. ISBN 978-3-319-28099-8. [Google Scholar]
- Chmielewski, M.; Clark, L.A.; Bagby, R.M.; Watson, D. Method Matters: Understanding Diagnostic Reliability in DSM-IV and DSM-5. J. Abnorm. Psychol. 2015, 124, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.E.; Narrow, W.E.; Regier, D.A.; Kuramoto, S.J.; Kupfer, D.J.; Kuhl, E.A.; Greiner, L.; Kraemer, H.C. DSM-5 Field Trials in the United States and Canada, Part I: Study Design, Sampling Strategy, Implementation, and Analytic Approaches. Am. J. Psychiatry 2013, 170, 43–58. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Forman, J.B.; Nee, J. DSM-III Field Trials: I. Initial Interrater Diagnostic Reliability. Am. J. Psychiatry 1979, 136, 815–817. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, M.; Brooke, E.M.; Cooper, J.E. An Experimental Approach to Psychiatric Diagnosis. An International Study. Acta Psychiatr. Scand. Suppl. 1968, 201, 7–89. [Google Scholar] [PubMed]
- Kraemer, H.C.; Kupfer, D.J.; Clarke, D.E.; Narrow, W.E.; Regier, D.A. DSM-5: How Reliable Is Reliable Enough? AJP 2012, 169, 13–15. [Google Scholar] [CrossRef]
- Becker, G. Creating Comparability among Reliability Coefficients: The Case of Cronbach Alpha and Cohen Kappa. Psychol. Rep. 2000, 87, 1171–1182E. [Google Scholar] [CrossRef]
- Morin, C.M.; Edinger, J. The Oxford Handbook of Sleep and Sleep Disorders; Oxford University Press: Oxford, UK, 2011; ISBN 978-0-19-970442-2. [Google Scholar]
- Ohayon, M.M.; Guilleminault, C.; Zulley, J.; Palombini, L.; Raab, H. Validation of the Sleep-EVAL System Against Clinical Assessments of Sleep Disorders and Polysomnographic Data. Sleep 1999, 22, 925–930. [Google Scholar] [CrossRef]
- Merikangas, K.R.; Zhang, J.; Emsellem, H.; Swanson, S.A.; Vgontzas, A.; Belouad, F.; Blank, M.M.; Chen, W.; Einen, M.; He, J.P.; et al. The Structured Diagnostic Interview for Sleep Patterns and Disorders: Rationale and Initial Evaluation. Sleep Med. 2014, 15, 530–535. [Google Scholar] [CrossRef]
- Hamilton, C.M.; Strader, L.C.; Pratt, J.G.; Maiese, D.; Hendershot, T.; Kwok, R.K.; Hammond, J.A.; Huggins, W.; Jackman, D.; Pan, H.; et al. The PhenX Toolkit: Get the Most from Your Measures. Am. J. Epidemiol. 2011, 174, 253–260. [Google Scholar] [CrossRef]
- Jones, K.D. A Critique of the DSM-5 Field Trials. J. Nerv. Ment. Dis. 2012, 200, 517–519. [Google Scholar] [CrossRef] [PubMed]
- Regier, D.A.; Narrow, W.E.; Clarke, D.E.; Kraemer, H.C.; Kuramoto, S.J.; Kuhl, E.A.; Kupfer, D.J. DSM-5 Field Trials in the United States and Canada, Part II: Test-Retest Reliability of Selected Categorical Diagnoses. Am. J. Psychiatry 2013, 170, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Schramm, E.; Hohagen, F.; Grasshoff, U.; Riemann, D.; Hajak, G.; Weess, H.G.; Berger, M. Test-Retest Reliability and Validity of the Structured Interview for Sleep Disorders According to DSM-III—R. Am. J. Psychiatry 1993, 150, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Edinger, J.D.; Kirby, A.C.; Lineberger, M.D.; Loiselle, M.M.; Wohlgemuth, W.K.; Means, M.K. Duke Structured Interview Schedule for DSM-IV-TR and International Classification of Sleep Disorders, Second Edition, Sleep Disorders Diagnoses; Veterans Affairs and Duke University Medical Centers: New York, NY, USA, 2006. [Google Scholar]
- Taylor, D.J.; Wilkerson, A.K.; Pruiksma, K.E.; Williams, J.M.; Ruggero, C.J.; Hale, W.; Mintz, J.; Organek, K.M.; Nicholson, K.L.; Litz, B.T.; et al. Reliability of the Structured Clinical Interview for DSM-5 Sleep Disorders Module. J. Clin. Sleep Med. 2018, 14, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Kottner, J.; Audige, L.; Brorson, S.; Donner, A.; Gajewski, B.J.; Hróbjartsson, A.; Roberts, C.; Shoukri, M.; Streiner, D.L. Guidelines for Reporting Reliability and Agreement Studies (GRRAS) Were Proposed. Int. J. Nurs. Stud. 2011, 48, 661–671. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Hauri, P.J.; Roth, T.; Stepanski, E.J.; Thorpy, M.J.; Bixler, E.O.; Kales, A.; Manfredi, R.L.; Vgontzas, A.N.; et al. Diagnostic Concordance for DSM-IV Sleep Disorders: A Report from the APA/NIMH DSM-IV Field Trial. Am. J. Psychiatry 1994, 151, 1351–1360. [Google Scholar] [CrossRef]
- Chung, K.-F.; Yeung, W.-F.; Ho, F.Y.-Y.; Ho, L.-M.; Yung, K.-P.; Yu, Y.-M.; Kwok, C.-W. Validity and Reliability of the Brief Insomnia Questionnaire in the General Population in Hong Kong. J. Psychosom. Res. 2014, 76, 374–379. [Google Scholar] [CrossRef]
- Edinger, J.D.; Wyatt, J.K.; Stepanski, E.J.; Olsen, M.K.; Stechuchak, K.M.; Carney, C.E.; Chiang, A.; Crisostomo, M.I.; Lineberger, M.D.; Means, M.K.; et al. Testing the Reliability and Validity of DSM-IV-TR and ICSD-2 Insomnia Diagnoses: Results of a Multitrait-Multimethod Analysis. Arch. Gen. Psychiatry 2011, 68, 992–1002. [Google Scholar] [CrossRef] [Green Version]
- Edinger, J.D.; Fins, A.I.; Goeke, J.M.; McMillan, D.K.; Gersh, T.L.; Krystal, A.D.; McCall, W.V. The Empirical Identification of Insomnia Subtypes: A Cluster Analytic Approach. Sleep 1996, 19, 398–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hening, W.A.; Allen, R.P.; Washburn, M.; Lesage, S.; Earley, C.J. Validation of the Hopkins Telephone Diagnostic Interview for Restless Legs Syndrome. Sleep Med. 2008, 9, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Coulouvrat, C.; Hajak, G.; Lakoma, M.D.; Roth, T.; Sampson, N.; Shahly, V.; Shillington, A.; Stephenson, J.J.; Walsh, J.K.; et al. Reliability and Validity of the Brief Insomnia Questionnaire in the America Insomnia Survey. Sleep 2010, 33, 1539–1549. [Google Scholar] [CrossRef]
- Loddo, G.; Vignatelli, L.; Zenesini, C.; Lusa, F.; Sambati, L.; Baldelli, L.; Favoni, V.; Pisani, L.R.; Pierangeli, G.; Cevoli, S.; et al. Interobserver Reliability of ICSD-3 Diagnostic Criteria for Disorders of Arousal in Adults. Sleep Breath. 2019, 23, 1309–1314. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Stone, J.; McDonald, K.; Jones, S. Psychological Management of Insomnia: A Clinical Replication Series with 100 Patients. Behav. Ther. 1994, 25, 291–309. [Google Scholar] [CrossRef]
- Vignatelli, L.; Bisulli, F.; Zaniboni, A.; Naldi, I.; Fares, J.E.; Provini, F.; Vetrugno, R.; Plazzi, G.; Tinuper, P.; Montagna, P. Interobserver Reliability of ICSD-R Minimal Diagnostic Criteria for the Parasomnias. J. Neurol. 2005, 252, 712–717. [Google Scholar] [CrossRef]
- Vignatelli, L.; Scaglione, C.; Grassi, C.; Minguzzi, E.; Provini, F.; Plazzi, G.; Bernardini, G.; Negrotti, A.; Maestri, M.; Marchese, R. Interobserver Reliability of ICSD-R Criteria for REM Sleep Behaviour Disorder. J. Sleep Res. 2003, 12, 255–257. [Google Scholar] [CrossRef]
- Vignatelli, L.; Plazzi, G.; Bassein, L.; Barbato, A.; De Vincentiis, A.; Lugaresi, E.; D’Alessandro, R.; GIN-SEN. Gruppo Italiano Narcolessia-Studio Epidemiologico Nazionale ICSD Diagnostic Criteria for Narcolepsy: Interobserver Reliability. International Classification of Sleep Disorders. Sleep 2002, 25, 193–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, R.P.; Picchietti, D.; Hening, W.A.; Trenkwalder, C.; Walters, A.S.; Montplaisi, J. Restless Legs Syndrome: Diagnostic Criteria, Special Considerations, and Epidemiology: A Report from the Restless Legs Syndrome Diagnosis and Epidemiology Workshop at the National Institutes of Health. Sleep Med. 2003, 4, 101–119. [Google Scholar] [CrossRef]
- Edinger, J.D.; Bonnet, M.H.; Bootzin, R.R.; Doghramji, K.; Dorsey, C.M.; Espie, C.A.; Jamieson, A.O.; McCall, W.V.; Morin, C.M.; Stepanski, E.J. Derivation of Research Diagnostic Criteria for Insomnia: Report of an American Academy of Sleep Medicine Work Group. Sleep 2004, 27, 1567–1596. [Google Scholar] [CrossRef]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision; World Health Organization: Geneva, Switzerland, 1990; ISBN 978-92-4-154649-2. [Google Scholar]
- Buysse, D.J.; Ancoli-Israel, S.; Edinger, J.D.; Lichstein, K.L.; Morin, C.M. Recommendations for a Standard Research Assessment of Insomnia. Sleep 2006, 29, 1155–1173. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F., III; Kupfer, D.J.; Thorpy, M.J.; Bixler, E.; Manfredi, R.; Kales, A.; Vgontzas, A.; Stepanski, E.; Roth, T.; et al. Clinical Diagnoses in 216 Insomnia Patients Using the International Classification of Sleep Disorders (ICSD), DSM-IV and ICD-10 Categories: A Report From the APA/NIMH DSM-IV Field Trial. Sleep 1994, 17, 630–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohayon, M.M.; Roberts, R.E. Comparability of Sleep Disorders Diagnoses Using DSM-IV and ICSD Classifications with Adolescents. Sleep 2001, 24, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F., III; Kupfer, D.J.; Thorpy, M.J.; Bixler, E.; Kales, A.; Manfredi, R.; Vgontzas, A.; Stepanski, E.; Roth, T.; et al. Effects of Diagnosis on Treatment Recommendations in Chronic Insomnia—A Report from the APA/NIMH DSM-IV Field Trial. Sleep 1997, 20, 542–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, D.T.; Fiske, D.W. Convergent and Discriminant Validation by the Multitrait-Multimethod Matrix. Psychol. Bull. 1959, 56, 81–105. [Google Scholar] [CrossRef] [Green Version]
- Kendell, R.; Jablensky, A. Distinguishing between the Validity and Utility of Psychiatric Diagnoses. Am. J. Psychiatry 2003, 160, 4–12. [Google Scholar] [CrossRef]
- Castelnovo, A.; Lopez, R.; Proserpio, P.; Nobili, L.; Dauvilliers, Y. NREM Sleep Parasomnias as Disorders of Sleep-State Dissociation. Nat. Rev. Neurol. 2018, 14, 470–481. [Google Scholar] [CrossRef]
- Loddo, G.; Lopez, R.; Cilea, R.; Dauvilliers, Y.; Provini, F. Disorders of Arousal in Adults: New Diagnostic Tools for Clinical Practice. Sleep Sci. Pract. 2019, 3, 5. [Google Scholar] [CrossRef] [Green Version]
- Lopez, R.; Shen, Y.; Chenini, S.; Rassu, A.L.; Evangelista, E.; Barateau, L.; Jaussent, I.; Dauvilliers, Y. Diagnostic Criteria for Disorders of Arousal: A Video-Polysomnographic Assessment. Ann. Neurol. 2018, 83, 341–351. [Google Scholar] [CrossRef]
- Lopez, R.; Lefevre, L.; Barateau, L.; Micoulaud-Franchi, J.-A.; Dauvilliers, Y.; Schenck, C.H. A Series of 8 Cases of Sleep-Related Psychogenic Dissociative Disorders and Proposed Updated Diagnostic Criteria. J. Clin. Sleep Med. 2022, 18, 563–573. [Google Scholar] [CrossRef]
- American Academy of Sleep Medicine Task Force Sleep-Related Breathing Disorders in Adults: Recommendations for Syndrome Definition and Measurement Techniques in Clinical Research. The Report of an American Academy of Sleep Medicine Task Force. Sleep 1999, 22, 667–689.
- Berry, A.; Brooks, R.; Gamaldo, C.; Harding, S.; Lloyd, R.; Marcus, C.; Vaughn, B. AASM Scoring Manual Version 2.2; American Academy of Sleep Medicine: Darien, IL, USA, 2015; p. 7. [Google Scholar]
- Ruehland, W.R.; Rochford, P.D.; O’Donoghue, F.J.; Pierce, R.J.; Singh, P.; Thornton, A.T. The New Aasm Criteria for Scoring Hypopneas: Impact on the Apnea Hypopnea Index. Sleep 2009, 32, 150–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenberg, R.S.; Van Hout, S. The American Academy of Sleep Medicine Inter-Scorer Reliability Program: Respiratory Events. J. Clin. Sleep Med. 2014, 10, 447–454. [Google Scholar] [CrossRef] [Green Version]
- Stepnowsky, C.J., Jr.; Berry, C.; Dimsdale, J.E. The Effect of Measurement Unreliability on Sleep and Respiratory Variables. Sleep 2004, 27, 990–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitney, C.W.; Gottlieb, D.J.; Redline, S.; Norman, R.G.; Dodge, R.R.; Shahar, E.; Surovec, S.; Nieto, F.J. Reliability of Scoring Respiratory Disturbance Indices and Sleep Staging. Sleep 1998, 21, 749–757. [Google Scholar] [CrossRef] [Green Version]
- D’Incau, E.; Gauld, C.; Philip, P.; Micoulaud-Franchi, J.-A. Sleep Bruxism Pulled between Two Worlds. J. Sleep Res. 2021, 30, e13351. [Google Scholar] [CrossRef]
- Malhotra, A.; Ayappa, I.; Ayas, N.; Collop, N.; Kirsch, D.; Mcardle, N.; Mehra, R.; Pack, A.I.; Punjabi, N.; White, D.P.; et al. Metrics of Sleep Apnea Severity: Beyond the Apnea-Hypopnea Index. Sleep 2021, 44, zsab030. [Google Scholar] [CrossRef]
- McNicholas, W.T.; Levy, P. Sleep-Related Breathing Disorders: Definitions and Measurements. Eur. Respir. J. 2000, 15, 988–989. [Google Scholar] [CrossRef] [Green Version]
- Pevernagie, D.A.; Gnidovec-Strazisar, B.; Grote, L.; Heinzer, R.; McNicholas, W.T.; Penzel, T.; Randerath, W.; Schiza, S.; Verbraecken, J.; Arnardottir, E.S. On the Rise and Fall of the Apnea-Hypopnea Index: A Historical Review and Critical Appraisal. J. Sleep Res. 2020, 29, e13066. [Google Scholar] [CrossRef]
- Randerath, W.; Bassetti, C.L.; Bonsignore, M.R.; Farre, R.; Ferini-Strambi, L.; Grote, L.; Hedner, J.; Kohler, M.; Martinez-Garcia, M.; Mihaicuta, S.; et al. Challenges and Perspectives in Obstructive Sleep Apnoea: Report by an Ad Hoc Working Group of the Sleep Disordered Breathing Group of the European Respiratory Society and the European Sleep Research Society. Eur. Respir. J. 2018, 52. [Google Scholar] [CrossRef]
- Randerath, W.J.; Herkenrath, S.; Treml, M.; Grote, L.; Hedner, J.; Bonsignore, M.R.; Pépin, J.L.; Ryan, S.; Schiza, S.; Verbraecken, J.; et al. Evaluation of a Multicomponent Grading System for Obstructive Sleep Apnoea: The Baveno Classification. ERJ Open Res. 2021, 7, 928–2020. [Google Scholar] [CrossRef] [PubMed]
- Silber, M.H.; Krahn, L.E.; Olson, E.J. Diagnosing Narcolepsy: Validity and Reliability of New Diagnostic Criteria. Sleep Med. 2002, 3, 109–113. [Google Scholar] [CrossRef]
- Folkerts, M.; Rosenthal, L.; Roehrs, T.; Krstevska, S.; Murlidhar, A.; Zorick, F.; Wittig, R.; Roth, T. The Reliability of the Diagnostic Features in Patients with Narcolepsy. Biol. Psychiatry 1996, 40, 208–214. [Google Scholar] [CrossRef]
- Lopez, R.; Doukkali, A.; Barateau, L.; Evangelista, E.; Chenini, S.; Jaussent, I.; Dauvilliers, Y. Test–Retest Reliability of the Multiple Sleep Latency Test in Central Disorders of Hypersomnolence. Sleep 2017, 40, zsx164. [Google Scholar] [CrossRef] [PubMed]
- Lammers, G.J.; Bassetti, C.L.A.; Dolenc-Groselj, L.; Jennum, P.J.; Kallweit, U.; Khatami, R.; Lecendreux, M.; Manconi, M.; Mayer, G.; Partinen, M.; et al. Diagnosis of Central Disorders of Hypersomnolence: A Reappraisal by European Experts. Sleep Med. Rev. 2020, 52, 101306. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M.; Dauvilliers, Y.; Reynolds, C.F. Operational Definitions and Algorithms for Excessive Sleepiness in the General Population: Implications for DSM-5 Nosology. Arch. Gen. Psychiatry 2012, 69, 71–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruoff, C.; Pizza, F.; Trotti, L.M.; Sonka, K.; Vandi, S.; Cheung, J.; Pinto, S.; Einen, M.; Simakajornboon, N.; Han, F.; et al. The MSLT Is Repeatable in Narcolepsy Type 1 But Not Narcolepsy Type 2: A Retrospective Patient Study. J. Clin. Sleep Med. 2018, 14, 65–74. [Google Scholar] [CrossRef]
- Marelli, S.; Galbiati, A.; Rinaldi, F.; Giora, E.; Oldani, A.; Strambi, L.F.; Zucconi, M. Restless Legs Syndrome/Willis Ekbom Disease: New Diagnostic Criteria According to Different Nosology. Arch. Ital. Biol. 2015, 153, 184–193. [Google Scholar] [CrossRef]
- Walters, A.S.; Aldrich, M.S.; Allen, R.; Ancoli-Israel, S.; Buchholz, D.; Chokroverty, S.; Coccagna, G.; Earley, C.; Ehrenberg, B.; Feest, T.G.; et al. Toward a Better Definition of the Restless Legs Syndrome. Mov. Disord. 1995, 10, 634–642. [Google Scholar] [CrossRef]
- Lavigne, G.J.; Rompre, P.H.; Montplaisir, J.Y. Sleep Bruxism: Validity of Clinical Research Diagnostic Criteria in a Controlled Polysomnographic Study. J. Dent. Res. 1996, 75, 546–552. [Google Scholar] [CrossRef]
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; Laat, A.D.; Leeuw, R.D.; et al. International Consensus on the Assessment of Bruxism: Report of a Work in Progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Lobbezoo, F.; Ahlberg, J.; Glaros, A.G.; Kato, T.; Koyano, K.; Lavigne, G.J.; De Leeuw, R.; Manfredini, D.; Svensson, P.; Winocur, E. Bruxism Defined and Graded: An International Consensus. J. Oral Rehabil. 2013, 40, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Carney, C.E.; Buysse, D.J.; Ancoli-Israel, S.; Edinger, J.D.; Krystal, A.D.; Lichstein, K.L.; Morin, C.M. The Consensus Sleep Diary: Standardizing Prospective Sleep Self-Monitoring. Sleep 2012, 35, 287–302. [Google Scholar] [CrossRef] [Green Version]
- Morgenthaler, T.I.; Lee-Chiong, T.; Alessi, C.; Friedman, L.; Aurora, R.N.; Boehlecke, B.; Brown, T.; Chesson, A.L., Jr.; Kapur, V.; Maganti, R.; et al. Practice Parameters for the Clinical Evaluation and Treatment of Circadian Rhythm Sleep Disorders. Sleep 2007, 30, 1445–1459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cottler, L. The DSM-IV Field Trial for Substance Use Disorders: Major Results. Drug Alcohol Depend. 1995, 38, 59–69. [Google Scholar] [CrossRef]
- Keller, M.B.; Klein, D.N.; Hirschfeld, R.M.A.; Kocsis, J.H.; McCullough, J.P.; Miller, I.; First, M.B.; Holzer, C.P.; Keitner, G.I.; Marin, D.B. Results of the DSM-IV Mood Disorders Field Trial. Am. J. Psychiatry 1995, 152, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Zinbarg, R.E.; Barlow, D.H.; Liebowitz, M.; Street, L. The DSM-IV Field Trial for Mixed Anxiety-Depression. Am. J. Psychiatry 1994, 151, 1153–1162. [Google Scholar] [CrossRef]
- Schenck, C.H.; Montplaisir, J.Y.; Frauscher, B.; Hogl, B.; Gagnon, J.-F.; Postuma, R.; Sonka, K.; Jennum, P.; Partinen, M.; Arnulf, I.; et al. Rapid Eye Movement Sleep Behavior Disorder: Devising Controlled Active Treatment Studies for Symptomatic and Neuroprotective Therapy—A Consensus Statement from the International Rapid Eye Movement Sleep Behavior Disorder Study Group. Sleep Med. 2013, 14, 795–806. [Google Scholar] [CrossRef]
- Gauld, C.; Lopez, R.; Geoffroy, P.A.; Morin, C.M.; Guichard, K.; Giroux, É.; Dauvilliers, Y.; Dumas, G.; Philip, P.; Micoulaud-Franchi, J.-A. A Systematic Analysis of ICSD-3 Diagnostic Criteria and Proposal for Further Structured Iteration. Sleep Med. Rev. 2021, 58, 101439. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Wakefield, J.C. DSM-IV Diagnostic Criterion for Clinical Significance: Does It Help Solve the False Positives Problem? Am. J. Psychiatry 1999, 156, 1856–1864. [Google Scholar] [CrossRef]
- Buysse, D.J.; Yu, L.; Moul, D.E.; Germain, A.; Stover, A.; Dodds, N.E.; Johnston, K.L.; Shablesky-Cade, M.A.; Pilkonis, P.A. Development and Validation of Patient-Reported Outcome Measures for Sleep Disturbance and Sleep-Related Impairments. Sleep 2010, 33, 781–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wieczorek, T.; Wieckiewicz, M.; Smardz, J.; Wojakowska, A.; Michalek-Zrabkowska, M.; Mazur, G.; Martynowicz, H. Sleep Structure in Sleep Bruxism: A Polysomnographic Study Including Bruxism Activity Phenotypes across Sleep Stages. J. Sleep Res. 2020, 29, e13028. [Google Scholar] [CrossRef] [PubMed]
- Lavigne, G.; Kato, T.; Herrero Babiloni, A.; Huynh, N.; Dal Fabbro, C.; Svensson, P.; Aarab, G.; Ahlberg, J.; Baba, K.; Carra, M.C.; et al. Research Routes on Improved Sleep Bruxism Metrics: Toward a Standardised Approach. J. Sleep Res. 2021, 30, e13320. [Google Scholar] [CrossRef]
- Shepherd, M. A Study of the Major Psychoses in an English County [Maudsley Monographs, Number Three], 1st ed.; Chapman & Hall: London, UK, 1957. [Google Scholar]
- Hening, W.A.; Allen, R.P.; Thanner, S.; Washburn, T.; Heckler, D.; Walters, A.S.; Earley, C.J. The Johns Hopkins Telephone Diagnostic Interview for the Restless Legs Syndrome: Preliminary Investigation for Validation in a Multi-Center Patient and Control Population. Sleep Med. 2003, 4, 137–141. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Methods 1 and 2 “Test–Retest Reliability” | Methods 3 and 4 “Joint Interrater Reliability” | Total | |
|---|---|---|---|
| DSMs | n = 3 (18% *) (kappa mean = 0.67) | n = 16 (75% *) (kappa mean = 0.70) | 19 |
| ICSDs | n = 14 (82% *) (kappa mean = 0.72) | n = 5 (25% *) (kappa mean = 0.67) | 19 |
| Total | 17 | 21 | 38 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gauld, C.; Lopez, R.; Philip, P.; Taillard, J.; Morin, C.M.; Geoffroy, P.A.; Micoulaud-Franchi, J.-A. A Systematic Review of Sleep–Wake Disorder Diagnostic Criteria Reliability Studies. Biomedicines 2022, 10, 1616. https://doi.org/10.3390/biomedicines10071616
Gauld C, Lopez R, Philip P, Taillard J, Morin CM, Geoffroy PA, Micoulaud-Franchi J-A. A Systematic Review of Sleep–Wake Disorder Diagnostic Criteria Reliability Studies. Biomedicines. 2022; 10(7):1616. https://doi.org/10.3390/biomedicines10071616
Chicago/Turabian StyleGauld, Christophe, Régis Lopez, Pierre Philip, Jacques Taillard, Charles M. Morin, Pierre Alexis Geoffroy, and Jean-Arthur Micoulaud-Franchi. 2022. "A Systematic Review of Sleep–Wake Disorder Diagnostic Criteria Reliability Studies" Biomedicines 10, no. 7: 1616. https://doi.org/10.3390/biomedicines10071616