
Cognitive Impairment in Secondary Progressive Multiple Sclerosis: Effect of Disease Duration, Age, and Progressive Phenotype

 , ,
, ,
Abstract
:1. Introduction
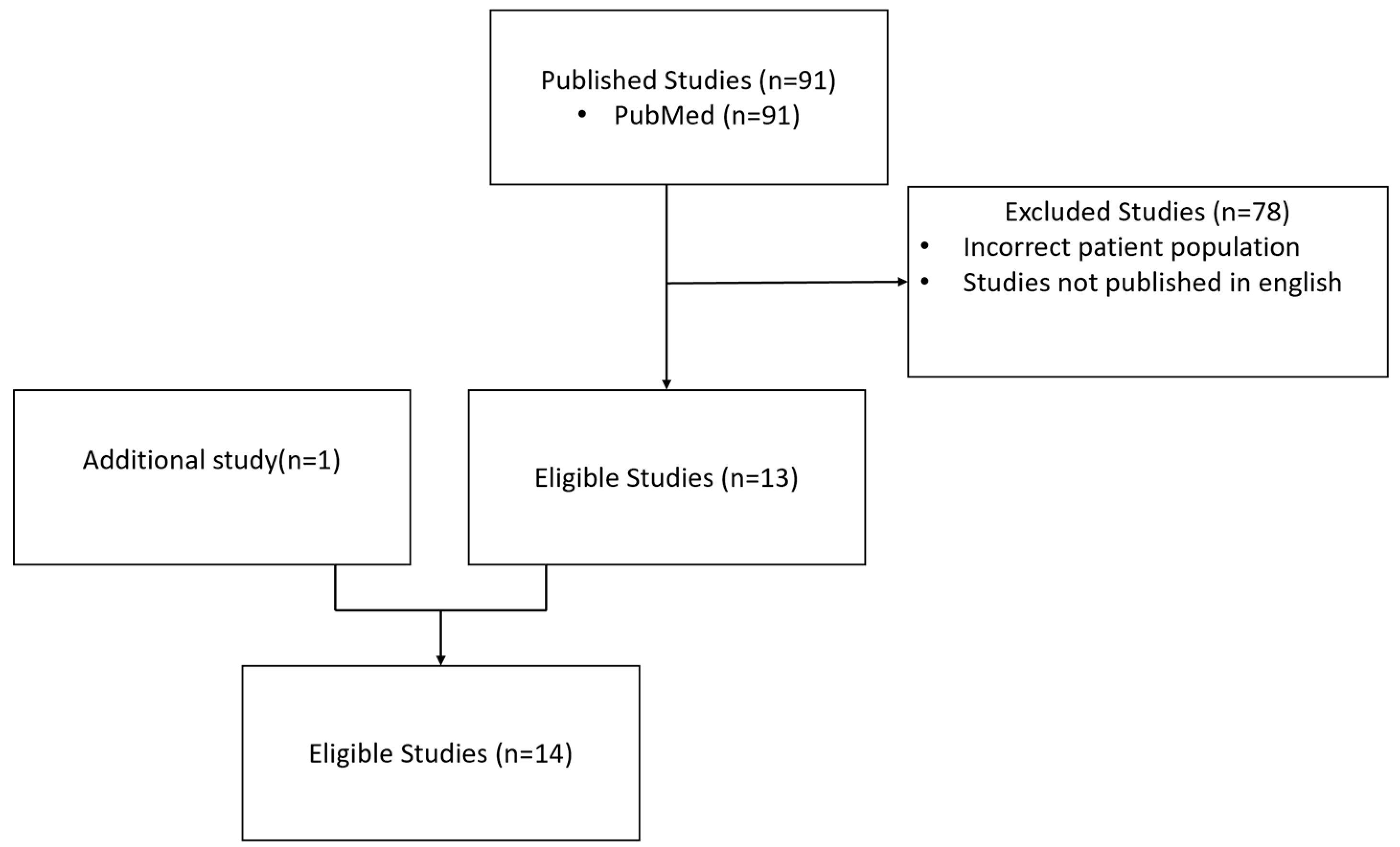
2. Methods
3. Results
3.1. Associations between Cognitive Disorders and Disease Duration
3.2. Associations between Cognitive Disorders and MS Phenotypes
3.3. Association between Cognitive Impairment Profile and MS Phenotype
3.4. The Evolution of Cognitive Disorders over Disease Course
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deloire, M.S.A. Cognitive impairment as marker of diffuse brain abnormalities in early relapsing remitting multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2005, 76, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Brochet, B.; Ruet, A. Cognitive Impairment in Multiple Sclerosis with Regards to Disease Duration and Clinical Phenotypes. Front Neurol. 2019, 10, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruet, A.; Deloire, M.; Charré-Morin, J.; Hamel, D.; Brochet, B. Cognitive impairment differs between primary progressive and relapsing-remitting MS. Neurology 2013, 80, 1501–1508. [Google Scholar] [CrossRef] [PubMed]
- Eijlers, A.J.; van Geest, Q.; Dekker, I.; Steenwijk, M.D.; Meijer, K.A.; Hulst, H.E.; Barkhof, F.; Uitdehaag, B.M.; Schoonheim, M.M.; Geurts, J.J. Predicting cognitive decline in multiple sclerosis: A 5-year follow-up study. Brain 2018, 141, 2605–2618. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.P.; Ponziani, G.; Siracusa, G.; Sorbi, S. Cognitive Dysfunction in Early-Onset Multiple Sclerosis: A Reappraisal after 10 Years. Arch Neurol. 2001, 58, 1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damasceno, A.; Pimentel-Silva, L.R.; Damasceno, B.P.; Cendes, F. Cognitive trajectories in relapsing–remitting multiple sclerosis: A longitudinal 6-year study. Mult. Scler. J. 2020, 26, 1740–1751. [Google Scholar] [CrossRef] [PubMed]
- Achiron, A.; Chapman, J.; Magalashvili, D.; Dolev, M.; Lavie, M.; Bercovich, E.; Polliack, M.; Doniger, G.M.; Stern, Y.; Khilkevich, O.; et al. Modeling of Cognitive Impairment by Disease Duration in Multiple Sclerosis: A Cross-Sectional Study. PLoS ONE 2013, 8, e71058. [Google Scholar] [CrossRef] [Green Version]
- Ruano, L.; Portaccio, E.; Goretti, B.; Niccolai, C.; Severo, M.; Patti, F.; Cilia, S.; Gallo, P.; Grossi, P.; Ghezzi, A.; et al. Age and disability drive cognitive impairment in multiple sclerosis across disease subtypes. Mult. Scler. J. 2017, 23, 1258–1267. [Google Scholar] [CrossRef] [Green Version]
- Dackovic, J.; Pekmezovic, T.; Mesaros, S.; Dujmovic, I.; Stojsavljevic, N.; Martinovic, V.; Drulovic, J. The Rao’s Brief Repeatable Battery in the study of cognition in different multiple sclerosis phenotypes: Application of normative data in a Serbian population. Neurol. Sci. 2016, 37, 1475–1481. [Google Scholar] [CrossRef]
- Smestad, C.; Sandvik, L.; Landrø, N.I.; Celius, E.G. Cognitive impairment after three decades of multiple sclerosis: Cognitive impairment in MS. Eur. J. Neurol. 2010, 17, 499–505. [Google Scholar] [CrossRef]
- Planche, V.; Gibelin, M.; Cregut, D.; Pereira, B.; Clavelou, P. Cognitive impairment in a population-based study of patients with multiple sclerosis: Differences between late relapsing−remitting, secondary progressive and primary progressive multiple sclerosis. Eur. J. Neurol. 2016, 23, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Maubeuge, N.; Deloire, M.S.; Brochet, B.; Ehrlé, N.; Charré-Morin, J.; Saubusse, A.; Ruet, A.; BICAFMS Study Investigators. Validation of the French version of the minimal assessment of cognitive function in multiple sclerosis (MACFIMS). Mult. Scler. Relat. Disord. 2021, 48, 102692. [Google Scholar] [CrossRef] [PubMed]
- Brissart, H.; Morele, E.; Baumann, C.; Perf, M.L.; Leininger, M.; Taillemite, L.; Dillier, C.; Pittion, S.; Spitz, E.; Debouverie, M. Cognitive impairment among different clinical courses of multiple sclerosis. Neurol. Res. 2013, 35, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Huijbregts, S.C.J.; Kalkers, N.F.; de Sonneville, L.M.J.; de Groot, V.; Reuling, I.E.W.; Polman, C.H. Differences in cognitive impairment of relapsing remitting, secondary, and primary progressive MS. Neurology 2004, 63, 335–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosti-Otajärvi, E.; Ruutiainen, J.; Huhtala, H.; Hämäläinen, P. Cognitive performance profile in different phenotypes of MS with cognitive complaints. Mult. Scler. Relat. Disord. 2014, 3, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Renner, A.; Baetge, S.J.; Filser, M.; Ullrich, S.; Lassek, C.; Penner, I. Characterizing cognitive deficits and potential predictors in multiple sclerosis: A large nationwide study applying Brief International Cognitive Assessment for Multiple Sclerosis in standard clinical care. J. Neuropsychol. 2020, 14, 347–369. [Google Scholar] [CrossRef]
- Benedict, R.H.; Cookfair, D.; Gavett, R.; Gunther, M.; Munschauer, F.; Garg, N.; Weinstock-Guttman, B. Validity of the minimal assessment of cognitive function in multiple sclerosis (MACFIMS). J. Int. Neuropsychol. Soc. 2006, 12, 549–558. [Google Scholar] [CrossRef]
- Kizlaitienė, R.; Kaubrys, G.; Giedraitienė, N.; Ramanauskas, N.; Dementavičienė, J. Composite Marker of Cognitive Dysfunction and Brain Atrophy is Highly Accurate in Discriminating between Relapsing-Remitting and Secondary Progressive Multiple Sclerosis. Med. Sci. Monit. 2017, 23, 588–597. [Google Scholar] [CrossRef] [Green Version]
- Matias-Guiu, J.A.; Cortés-Martínez, A.; Valles-Salgado, M.; Oreja-Guevara, C.; Pytel, V.; Montero, P.; Moreno-Ramos, T.; Matias-Guiu, J. Functional Components of Cognitive Impairment in Multiple Sclerosis: A Cross-Sectional Investigation. Front Neurol. 2017, 8, 643. [Google Scholar] [CrossRef]
- Huijbregts, S.C.J.; Kalkers, N.F.; de Sonneville, L.M.J.; de Groot, V.; Polman, C.H. Cognitive impairment and decline in different MS subtypes. J. Neurol. Sci. 2006, 245, 187–194. [Google Scholar] [CrossRef]
- Cree, B.A.C.; Arnold, D.L.; Chataway, J.; Chitnis, T.; Fox, R.J.; Ramajo, A.P.; Murphy, N.; Lassmann, H. Secondary Progressive Multiple Sclerosis: New Insights. Neurology 2021, 97, 378–388. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Number of Centres | Number of Patients | Comments and Main Evaluation Criteria | Primary Results | |||
|---|---|---|---|---|---|---|---|
| SPMS (N) | PPMS (N) | RRMS (N) | Control Subjects (N) | ||||
| Benedict, 2006 | 1 | 78 | 7 | 200 | 56 | +6 patients with PPMS (primary progressive) The aim of the study was to assess the validity of MACFIMS as a tool for detecting cognitive impairment in patients with MS. | The 7 neuropsychological evaluation tests used by the MACFIMS enabled identification of healthy individuals and patients with MS and to distinguish patients with the RR form from those with SP form, with an effect size varying from medium to very high. |
| Brissart, 2013 | 1 | 36 | 24 | 78 | 63 | The main objective was to describe cognitive impairment in the early stages of MS; the secondary objective was to compare cognitive performance according to MS phenotypes. | Compared to RR forms, patients with SP forms had more severe involvement on SDMT and RAVLT. There was no significant difference between the PP and SP forms. |
| Eijlers, 2018 | 1 | 33 | 19 | 182 | 60 | The aim of the study was to identify MRI parameters and demographic and/or clinical data that could be predictive of cognitive decline during 5-year follow-up with BRB. | 66/234 patients (28%) presented a cognitive decline during follow-up, particularly in the progressive forms: 18/33 patients with SPMS (55%), 10/19 patients with PPMS (53%), and 38/182 patients with RRMS (21%). |
| Huijbregt, 2004 & 2006 | 1 | 71 | 55 | 108 | 67 | The aim of the study was to explore the cognitive functions of patients with MS and to assess the impact of the different phenotypes of the disease. The 2-year follow-up is presented in the 2006 study. Assessment by BRB. | The severity of the impairment was greater in the SPMS than in the RRMS forms for memory tests (SRT and SPART) for information processing speed (SDMT) and for working memory (PASAT). The severity of the impairment was greater in the SPMS forms than in the RRMS forms for memory tests (SRT, Selective Reminding Test; and SPART) for the speed of information processing (SDMT, Symbol Digit Modalities Test) and for working memory (PASAT, Paced Auditory Serial Addition Task). |
| Maubeuge, 2020 | 15 | 46 | 45 | 43 | 276 | The aim of the study was to validate the French version of the MACFIMS. | The cognitive deficit concerned 33.7% of patients with MS: 42.9% in the SPMS group, 35.3% in the PPMS group, and 18.8% in the RRMS group. |
| Author | Number of Centres | Number of Patients | Comments and Main Evaluation Criteria | Primary Results | |||
|---|---|---|---|---|---|---|---|
| SPMS (N) | PPMS (N) | RRMR (N) | Control Subjects (N) | ||||
| Achiron, 2013 | 1 | 100 | 27 | 1173 | Controls (1569 healthy subjects) | +200 patients with CIS The objective of the study was to evaluate the evolution of cognitive capacities in patients with MS via a battery of computerized tests evaluating verbal and non-verbal memory, executive functions, visuospatial perception, verbal function, attention, speed of information processing, and motor skills. | 5 years after disease onset, 20.9% of patients had a cognitive decline of one standard deviation and 6% a severe cognitive decline of two standard deviations. The 10-year rates were 29.3% and 9.0%. The severity of the overall cognitive score was greater for the group of patients with SPMS than in the group of patients with CIS or RRMS (81.3 versus 92.1, p < 0.0001 and 90.6, p < 0.0001). |
| Dackovic, 2016 | 1 | 31 | 35 | 65 | 0 | +37 patients with CIS. The aim of the study was to assess cognitive performance based on MS phenotypes using BRB. | 58.9% of patients presented with cognitive impairment: 40.5% in the CIS group, 36.9% in the RRMS group, 96.8% in the SPMS group, and 85.7% in the PPMS group (before adjustment, percentages not specified after adjustment). |
| Kizlaitiené, 2017 | 1 | 45 | - | 43 | 0 | The objective of the study was to identify a simple way to discriminate between RRMS and SPMS forms that is applicable in clinical practice, based on MRI data and evaluation of cognitive performance using a specific battery. | The study proposed a composite marker based on imagery and cognitive testing to discriminate between RRMS and SPMS. |
| Matias-Guiu 2017 | 1 | 52 | 23 | 236 | Norms | The aim was to determine the frequency of cognitive deficits and the main cognitive domains affected and to identify the factors associated. The neuropsychological evaluation was carried out using a specific battery. | Cognitive decline identified in 41.5% of patients, significantly more frequent in patients with forms of SP and PP (p = 0.002). The mean scores for the items verbal memory and superior executive functions were higher in patients with RRMS than in patients with a progressive form. |
| Planche, 2015 | 1 + network | 37 | 23 | 41 | 0 | Retrospective analysis of cognitive tests (BRB or others) from a MS patient database to explore the distribution and frequency of different phenotypes. | 63% of the patients had a significant cognitive decline (36.6% in the RRMS group, 86.1% in the SPMS group, and 73.9% in the PPMS group). Patients with SPMS had double the risk of cognitive decline compared with RRMS patients. |
| Renner, 2020 | 65 | 87 | 29 | 978 | 0 | Multicentre study to characterize cognitive deficits and to identify predictive markers of cognitive decline using in particular the BICAMS battery. | Cognitive disorders were present in 28% of patients and more frequent in the progressive forms (SP: 45.9%, PP: 44.8%) than in the RR form (25.8%). |
| Rosti-Otajarvi, 2014 | 1 | 32 | 26 | 138 | 0 | The aim of the study was to assess the extent to which cognitive complaints by patients with different MS phenotypes were associated with specific cognitive deficit profiles using the BRB. | A significant difference was noted between the progressive forms and the RR forms using the SDMT (37.7 vs. 44.9, p = 0.001). |
| Ruano, 2017 | 6 | 74 | 40 | 759 | 0 | +167 patients with CIS. The aim of the study was to compare the prevalence and characteristics of cognitive impairment in a population of patients with MS, based on the BRB and the Stroop test. | The percentage of cognitively impaired patients was significantly higher in the SP form (79.4%) versus the CIS (34.5%) and the RR (44.5%) forms.In multivariate analysis, the determinants of cognitive decline were age and physical disability. |
| Smestad, 2010 | 1 + region | 72 | 14 | 36 | 0 | The aim of the study was to assess the evolution of cognitive abilities over 3 decades in patients with MS via a battery of specific neuropsychological tests. | After 30 years of MS, 48% of patients presented with cognitive decline. Logistic regression analysis with cognitive deficit as the dependent variable showed a significant association with the phenotype, the risk being higher in SPMS forms than in RRMS forms with an odds ratio of 2.74 (p = 0.049). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brochet, B.; Clavelou, P.; Defer, G.; De Seze, J.; Louapre, C.; Magnin, E.; Ruet, A.; Thomas-Anterion, C.; Vermersch, P. Cognitive Impairment in Secondary Progressive Multiple Sclerosis: Effect of Disease Duration, Age, and Progressive Phenotype. Brain Sci. 2022, 12, 183. https://doi.org/10.3390/brainsci12020183
Brochet B, Clavelou P, Defer G, De Seze J, Louapre C, Magnin E, Ruet A, Thomas-Anterion C, Vermersch P. Cognitive Impairment in Secondary Progressive Multiple Sclerosis: Effect of Disease Duration, Age, and Progressive Phenotype. Brain Sciences. 2022; 12(2):183. https://doi.org/10.3390/brainsci12020183
Chicago/Turabian StyleBrochet, Bruno, Pierre Clavelou, Gilles Defer, Jérôme De Seze, Céline Louapre, Eloi Magnin, Aurélie Ruet, Catherine Thomas-Anterion, and Patrick Vermersch. 2022. "Cognitive Impairment in Secondary Progressive Multiple Sclerosis: Effect of Disease Duration, Age, and Progressive Phenotype" Brain Sciences 12, no. 2: 183. https://doi.org/10.3390/brainsci12020183