Lymphotropic Viruses EBV, KSHV and HTLV in Latin America: Epidemiology and Associated Malignancies. A Literature-Based Study by the RIAL-CYTED

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Epstein–Barr Virus
2.1. EBV-Associated Lymphoid Neoplasms in Latin America
2.1.1. Hodgkin Lymphoma
2.1.2. Burkitt Lymphoma
2.1.3. Diffuse Large B Cell Lymphoma
2.1.4. T and NK Lymphoproliferative Disorders
3. Kaposi Sarcoma Human Herpesvirus
KSHV Prevalence and Morbidity in Latin America
4. Human T-Cell Lymphotropic Virus
HTLV Prevalence and Morbidity in Latin America
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Schottenfeld, D.; Beebe-Dimmer, J. The cancer burden attributable to biologic agents. Ann Epidemiol. 2015, 25, 183–187. [Google Scholar] [CrossRef]
- Morales-Sanchez, A.; Fuentes-Panana, E.M. Human viruses and cancer. Viruses 2014, 6, 4047–4079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biological Agents. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; 100B (Eipstein Barr Virus); Internactional Agency for Research on Cancer: Lyon, France, 2012; pp. 49–92.
- Casulo, C.; Friedberg, J.W. Burkitt lymphoma- a rare but challenging lymphoma. Best Pract. Res. Clin. Haematol. 2018, 31, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Shannon-Lowe, C.; Rickinson, A.B.; Bell, A.I. Epstein-Barr virus-associated lymphomas. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2017, 372, e20160271. [Google Scholar] [CrossRef] [PubMed]
- Higgins, C.D.; Swerdlow, A.J.; Macsween, K.F.; Harrison, N.; Williams, H.; McAulay, K.; Thomas, R.; Reid, S.; Conacher, M.; Britton, K.; et al. A study of risk factors for acquisition of Epstein-Barr virus and its subtypes. J. Infect. Dis. 2007, 195, 474–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odumade, O.A.; Hogquist, K.A.; Balfour, H.H., Jr. Progress and problems in understanding and managing primary Epstein-Barr virus infections. Clin. Microbiol. Rev. 2011, 24, 193–209. [Google Scholar] [CrossRef] [Green Version]
- Hsu, J.L.; Glaser, S.L. Epstein-barr virus-associated malignancies: Epidemiologic patterns and etiologic implications. Crit. Rev. Oncol. Hematol. 2000, 34, 27–53. [Google Scholar] [CrossRef]
- WHO Classification of Tumours of Hematopoietic and Lymphoid Tissues, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2017; Volume 2.
- Cohen, M.; De Matteo, E.; Narbaitz, M.; Carreno, F.A.; Preciado, M.V.; Chabay, P.A. Epstein-Barr virus presence in pediatric diffuse large B-cell lymphoma reveals a particular association and latency patterns: Analysis of viral role in tumor microenvironment. Int. J. Cancer 2013, 132, 1572–1580. [Google Scholar] [CrossRef]
- Cohen, M.; Narbaitz, M.; Metrebian, F.; De Matteo, E.; Preciado, M.V. Epstein-Barr virus-positive diffuse large B-cell lymphoma association is not only restricted to elderly patients. Int. J. Cancer 2014, 135, 2816–2824. [Google Scholar] [CrossRef]
- Cohen, M.; Vistarop, A.G.; Huaman, F.; Narbaitz, M.; Metrebian, F.; De Matteo, E.; Preciado, M.V.; Chabay, P.A. Cytotoxic response against Epstein Barr virus coexists with diffuse large B-cell lymphoma tolerogenic microenvironment: Clinical features and survival impact. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef]
- Corti, M.; Minue, G.; Campitelli, A.; Narbaitz, M.; Gilardi, L. An Aggressive Plasmablastic Lymphoma of the Oral Cavity as Primary Manifestation of Acquired Immunodeficiency Syndrome: Case Report and Literature Review. Int. Arch. Otorhinolaryngol. 2015, 19, 354–358. [Google Scholar] [PubMed] [Green Version]
- Lara, J.; Cohen, M.; De Matteo, E.; Aversa, L.; Preciado, M.V.; Chabay, P. Epstein-Barr virus (EBV) association and latency profile in pediatric Burkitt’s lymphoma: Experience of a single institution in Argentina. J. Med. Virol. 2014, 86, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Corti, M.; Villafane, M.F.; Bistmans, A.; Campitelli, A.; Narbaitz, M.; Bare, P. Oral cavity and extra-oral plasmablastic lymphomas in AIDS patients: Report of five cases and review of the literature. Int. J. STD AIDS 2011, 22, 759–763. [Google Scholar] [CrossRef]
- Chabay, P.; Lara, J.; Lorenzetti, M.; Cambra, P.; Acosta Haab, G.; Aversa, L.; De Matteo, E.; Preciado, M.V. Epstein Barr virus in relation to apoptosis markers and patients’ outcome in pediatric B-cell non-Hodgkin lymphoma. Cancer Lett. 2011, 307, 221–226. [Google Scholar] [CrossRef]
- Metta, H.; Corti, M.; Maranzana, A.; Schtirbu, R.; Narbaitz, M.; De Dios Soler, M. Unusual case of plasmablastic non-Hodgkin’s lymphoma located in the liver. First case reported in an AIDS patient. Ann. Hepatol. 2009, 8, 242–245. [Google Scholar] [CrossRef]
- Chabay, P.; De Matteo, E.; Lorenzetti, M.; Gutierrez, M.; Narbaitz, M.; Aversa, L.; Preciado, M.V. Vulvar plasmablastic lymphoma in a HIV-positive child: A novel extraoral localisation. J. Clin. Pathol. 2009, 62, 644–646. [Google Scholar] [CrossRef]
- Chabay, P.; De Matteo, E.; Lorenzetti, M.; Barón, A.V.; Valva, P.; Preciado, M.V. Low frequency of Epstein Barr virus association and high frequency of p53 overexpression in an Argentinean pediatric T-cell lymphoma series. Pediatr. Dev. Pathol. 2009, 12, 28–34. [Google Scholar] [CrossRef]
- Chabay, P.A.; Barros, M.H.; Hassan, R.; De Matteo, E.; Rey, G.; Carrico, M.K.; Renault, I.Z.; Preciado, M.V. Pediatric Hodgkin lymphoma in 2 South American series: A distinctive epidemiologic pattern and lack of association of Epstein-Barr virus with clinical outcome. J. Pediatr. Hematol. Oncol. 2008, 30, 285–291. [Google Scholar] [CrossRef]
- Fellner, M.D.; Durand, K.; Correa, R.M.; Redini, L.; Yampolsky, C.; Colobraro, A.; Sevlever, G.; Teyssié, A.R.; Benetucci, J.; Picconi, M.A. Circulating Epstein-Barr virus (EBV) in HIV-infected patients and its relation with primary brain lymphoma. Int. J. Infect. Dis. 2007, 11, 172–178. [Google Scholar] [CrossRef] [Green Version]
- De Matteo, E.; Baron, A.V.; Chabay, P.; Porta, J.; Dragosky, M.; Preciado, M.V. Comparison of Epstein-Barr virus presence in Hodgkin lymphoma in pediatric versus adult Argentine patients. Arch. Pathol. Lab. Med. 2003, 127, 1325–1329. [Google Scholar]
- Preciado, M.V.; Fallo, A.; Chabay, P.; Calcagno, L.; De Matteo, E. Epstein Barr virus-associated lymphoma in HIV-infected children. Pathol Res. Pract. 2002, 198, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Rao, C.R.; Gutierrez, M.I.; Bhatia, K.; Fend, F.; Franklin, J.; Appaji, L.; Gallo, G.; O’Conor, G.; Lalitha, N.; Magrath, I. Association of Burkitt’s lymphoma with the Epstein-Barr virus in two developing countries. Leuk. Lymphoma 2000, 39, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Preciado, M.V.; Cristobal, E.; Menarguez, J.; Martinez Montero, J.C.; Diez, B.; De Matteo, E.; Grinstein, S. Oncogene expression in tumour cells of pediatric Hodgkin’s disease in Argentina—Correlation with Epstein Barr virus presence. Pathol. Res. Pract. 1998, 194, 25–31. [Google Scholar] [CrossRef]
- Preciado, M.V.; De Matteo, E.; Diez, B.; Grinstein, S. Epstein-Barr virus (EBV) latent membrane protein (LMP) in tumor cells of Hodgkin’s disease in pediatric patients. Med. Pediatr. Oncol. 1995, 24, 1–5. [Google Scholar] [CrossRef]
- Preciado, M.V.; De Matteo, E.; Diez, B.; Menarguez, J.; Grinstein, S. Presence of Epstein-Barr virus and strain type assignment in Argentine childhood Hodgkin’s disease. Blood 1995, 86, 3922–3929. [Google Scholar] [CrossRef]
- Drut, R.M.; Day, S.; Drut, R.; Meisner, L. Demonstration of Epstein-Barr viral DNA in paraffin-embedded tissues of Burkitt’s lymphoma from Argentina using the polymerase chain reaction and in situ hybridization. Pediatr. Pathol. 1994, 14, 101–109. [Google Scholar] [CrossRef]
- Poles, W.A.; Nishi, E.E.; de Oliveira, M.B.; Eugenio, A.I.P.; de Andrade, T.A.; Campos, A.; de Campos, R.R., Jr.; Vassallo, J.; Alves, A.C.; Scapulatempo Neto, C.; et al. Targeting the polarization of tumor-associated macrophages and modulating mir-155 expression might be a new approach to treat diffuse large B-cell lymphoma of the elderly. Cancer Immunol. Immunother. 2019, 68, 269–282. [Google Scholar] [CrossRef]
- Guedes, J.C.R.; Cunha, K.; Machado, J.; Pinto, L.W. Nasal-type extranodal T-cell/NK lymphoma in association with hemophagocytic syndrome. An. Bras. Dermatol. 2018, 93, 422–425. [Google Scholar] [CrossRef] [Green Version]
- Miranda, M.F.R.; Santos, J.; Muller, S.F.R.; Bittencourt, M.J.S.; Brito, A.C.; Barros Junior, J.; Xerfan, E.M.S. Hydroa Vacciniforme-Like T-Cell Lymphoma: A Further Brazilian Case. Am. J. Dermatopathol. 2018, 40, 201–204. [Google Scholar] [CrossRef]
- Campos, A.; Moreira, A.; Ribeiro, K.B.; Paes, R.P.; Zerbini, M.C.; Aldred, V.; de Souza, C.A.; Neto, C.S.; Soares, F.A.; Vassallo, J. Frequency of EBV associated classical Hodgkin lymphoma decreases over a 54-year period in a Brazilian population. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Barros, M.H.; Leite, E.; Chabay, P.; Morais, V.; Stefanoff, G.; Hassan, R. Diagnosing lymphoma in a setting with a high burden of infection: A pediatric case of Epstein-Barr virus-associated aggressive B-cell lymphoma with t(8;14) (q23;q32) and extensive necrosis mimicking tuberculosis. Rev. Soc. Bras. Med. Trop. 2015, 48, 108–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, T.A.; Evangelista, A.F.; Campos, A.H.; Poles, W.A.; Borges, N.M.; Camillo, C.M.; Soares, F.A.; Vassallo, J.; Paes, R.P.; Zerbini, M.C.; et al. A microRNA signature profile in EBV+ diffuse large B-cell lymphoma of the elderly. Oncotarget 2014, 5, 11813–11826. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, C.R.; Felipe-Silva, A.; de Campos, F.P.F.; Zerbini, M.C.N. Nodal Epstein-Barr virus-positive T-cell/NK-cell lymphoma associated with immunodeficiency: A rare condition looking for recognition. Autops. Case Rep. 2014, 4, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Rebelo-Pontes, H.A.; Abreu, M.C.; Guimarães, D.M.; Fonseca, F.P.; Andrade, B.A.; Almeida, O.P.; Pinto Júnior, D.D.; Corrêa-Pontes, F.S. Burkitt’s lymphoma of the jaws in the Amazon region of Brazil. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e32–e37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minnicelli, C.; Barros, M.H.; Klumb, C.E.; Romano, S.O.; Zalcberg, I.R.; Hassan, R. Relationship of Epstein-Barr virus and interleukin 10 promoter polymorphisms with the risk and clinical outcome of childhood Burkitt lymphoma. PLoS ONE 2012, 7, e46005. [Google Scholar] [CrossRef]
- Assis, M.C.; Campos, A.H.; Oliveira, J.S.; Soares, F.A.; Silva, J.M.; Silva, P.B.; Penna, A.D.; Souza, E.M.; Baiocchi, O.C. Increased expression of CD4+CD25+FOXP3+ regulatory T cells correlates with Epstein-Barr virus and has no impact on survival in patients with classical Hodgkin lymphoma in Brazil. Med. Oncol. 2012, 29, 3614–3619. [Google Scholar] [CrossRef]
- Santos, M.; Nogueira, L.; Talahri, C.; Massone, C.; Cerroni, L.; Mira, M.T.; Talhari, S. Hydroa vacciniforme-like lymphoma in a patient from the Brazilian Amazon. Int. J. Dermatol. 2013, 52, 641–643. [Google Scholar] [CrossRef]
- Marques, M.; Luz, E.; Hummel, M.; Vieira, M.; Bahia, R.C.; Oliveira, M.C.; Netto, E.M.; Luz, I.; Araujo, I. Prognostic Biomarkers and EBV Infection Research in Diffuse Large B-Cell Lymphoma of the Palatine Tonsils. ISRN Oncol. 2012, 2012, 7. [Google Scholar] [CrossRef] [Green Version]
- Barros, M.H.; Hassan, R.; Niedobitek, G. Disease patterns in pediatric classical Hodgkin lymphoma: A report from a developing area in Brazil. Hematol. Oncol. 2011, 29, 190–195. [Google Scholar] [CrossRef]
- Barros, M.H.; Scheliga, A.; De Matteo, E.; Minnicelli, C.; Soares, F.A.; Zalcberg, I.R.; Hassan, R. Cell cycle characteristics and Epstein-Barr virus are differentially associated with aggressive and non-aggressive subsets of Hodgkin lymphoma in pediatric patients. Leuk. Lymphoma 2010, 51, 1513–1522. [Google Scholar] [CrossRef]
- Barros, M.H.; Vera-Lozada, G.; Soares, F.A.; Niedobitek, G.; Hassan, R. Tumor microenvironment composition in pediatric classical Hodgkin lymphoma is modulated by age and Epstein-Barr virus infection. Int. J. Cancer 2012, 131, 1142–1152. [Google Scholar] [CrossRef] [PubMed]
- Souza, E.M.; Baiocchi, O.C.; Zanichelli, M.A.; Alves, A.C.; Assis, M.G.; Eiras, D.P.; Dobo, C.; Oliveira, J.S. Impact of Epstein-Barr virus in the clinical evolution of patients with classical Hodgkin’s lymphoma in Brazil. Hematol. Oncol. 2010, 28, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Souza, E.M.; Baiocchi, O.C.; Zanichelli, M.A.; Alves, A.C.; Assis, M.G.; Silva, J.M.; Dobo, C.; Oliveira, J.S. Matrix metalloproteinase-9 is consistently expressed in Hodgkin/Reed-Sternberg cells and has no impact on survival in patients with Epstein-Barr virus (EBV)-related and non-related Hodgkin lymphoma in Brazil. Med. Oncol. 2012, 29, 2148–2152. [Google Scholar] [CrossRef] [PubMed]
- Gualco, G.; Domeny-Duarte, P.; Chioato, L.; Barber, G.; Natkunam, Y.; Bacchi, C.E. Clinicopathologic and molecular features of 122 Brazilian cases of nodal and extranodal NK/T-cell lymphoma, nasal type, with EBV subtyping analysis. Am. J. Surg. Pathol. 2011, 35, 1195–1203. [Google Scholar] [CrossRef]
- Gaiolla, R.D.; Domingues, M.A.; Niero-Melo, L.; de Oliveira, D.E. Serum levels of interleukins 6, 10, and 13 before and after treatment of classic Hodgkin lymphoma. Arch. Pathol. Lab. Med. 2011, 135, 483–489. [Google Scholar]
- Gualco, G.; Weiss, L.M.; Barber, G.N.; Bacchi, C.E. Diffuse large B-cell lymphoma involving the central nervous system. Int. J. Surg. Pathol. 2011, 19, 44–50. [Google Scholar] [CrossRef]
- Gualco, G.; Ortega, V.; Chioato, L.; Musto, M.L.; Bacchi, L.M.; Weiss, L.M.; Bacchi, C.E. Hodgkin’s Lymphoma Presenting as Dominant Gastric Lesion in Immunocompetent Patients: Report of 5 Cases With EBV Analysis. Int. J. Surg. Pathol. 2011, 19, 235–240. [Google Scholar] [CrossRef]
- Machado, A.S.; Da Silva Robaina, M.C.; Magalhães De Rezende, L.M.; Apa, A.G.; Amoêdo, N.D.; Bacchi, C.E.; Klumb, C.E. Circulating cell-free and Epstein-Barr virus DNA in pediatric B-non-Hodgkin lymphomas. Leuk. Lymphoma 2010, 51, 1020–1027. [Google Scholar] [CrossRef]
- Gualco, G.; Chioato, L.; Van Den Berg, A.; Weiss, L.M.; Bacchi, C.E. Composite lymphoma: EBV-positive classic Hodgkin lymphoma and peripheral T-cell lymphoma: A case report. Appl. Immunohistochem. Mol. Morphol. 2009, 17, 72–76. [Google Scholar] [CrossRef]
- Campos, A.H.; Aldred, V.L.; Ribeiro, K.C.; Vassallo, J.; Soares, F.A. Role of immunoexpression of nitric oxide synthases by Hodgkin and Reed-Sternberg cells on apoptosis deregulation and on clinical outcome of classical Hodgkin lymphoma. Mol. Cell. Biochem. 2009, 321, 95–102. [Google Scholar] [CrossRef]
- Queiroga, E.M.; Gualco, G.; Chioato, L.; Harrington, W.J.; Araujo, I.; Weiss, L.M.; Bacchi, C.E. Viral studies in burkitt lymphoma: Association with Epstein-Barr virus but not HHV-8. Am. J. Clin. Pathol. 2008, 130, 186–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Queiroga, E.M.; Gualco, G.; Weiss, L.M.; Dittmer, D.P.; Araujo, I.; Klumb, C.E.; Harrington, W.J., Jr.; Bacchi, C.E. Burkitt lymphoma in Brazil is characterized by geographically distinct clinicopathologic features. Am. J. Clin. Pathol. 2008, 130, 946–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pizza, M.; Bruniera, P.; Luporini, S.M.; Marcelino da Silva, H.R.; Borsato, M.L.; de Castro, H.C.; Soares, F.A.; Paes, R.A. Detection of Epstein-Barr virus in children and adolescents with Burkitt’s lymphoma by in situ hybridization using tissue microarrays. Hematology 2008, 13, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Hassan, R.; Klumb, C.E.; Felisbino, F.E.; Guiretti, D.M.; White, L.R.; Stefanoff, C.G.; Barros, M.H.; Seuanez, H.N.; Zalcberg, I.R. Clinical and demographic characteristics of Epstein-Barr virus-associated childhood Burkitt’s lymphoma in Southeastern Brazil: Epidemiological insights from an intermediate risk region. Haematologica 2008, 93, 780–783. [Google Scholar] [CrossRef] [PubMed]
- Ferrazzo, K.L.; Mesquita, R.A.; Aburad, A.T.; Nunes, F.D.; de Sousa, S.O. EBV detection in HIV-related oral plasmablastic lymphoma. Oral Dis. 2007, 13, 564–569. [Google Scholar] [CrossRef]
- Figueiredo, C.P.; Franz-Vasconcelos, H.C.; Giunta, G.; Mazzuco, T.L.; Caon, T.; Fernandes, A.L.; Simoes, C.M.; Antunes, V.L.; Niel, C.; Barardi, C.R. Detection of Torque teno virus in Epstein-Barr virus positive and negative lymph nodes of patients with Hodgkin lymphoma. Leuk. Lymphoma 2007, 48, 731–735. [Google Scholar] [CrossRef]
- Costa, H.; Franco, M.; Hahn, M.D. Primary lymphoma of the central nervous system: A clinical-pathological and immunohistochemical study of ten autopsy cases. Arq. Neuropsiquiatr. 2006, 64, 976–982. [Google Scholar] [CrossRef] [Green Version]
- Musacchio, J.G.; Carvalho Mda, G.; Morais, J.C.; Silva, N.H.; Scheliga, A.; Romano, S.; Spector, N. Detection of free circulating Epstein-Barr virus DNA in plasma of patients with Hodgkin’s disease. Sao Paulo Med. J. 2006, 124, 154–157. [Google Scholar] [CrossRef] [Green Version]
- Araujo, I.; Bittencourt, A.L.; Barbosa, H.S.; Netto, E.M.; Mendonca, N.; Foss, H.D.; Hummel, M.; Stein, H. The high frequency of EBV infection in pediatric Hodgkin lymphoma is related to the classical type in Bahia, Brazil. Virchows Arch. 2006, 449, 315. [Google Scholar] [CrossRef]
- Hassan, R.; White, L.R.; Stefanoff, C.G.; de Oliveira, D.E.; Felisbino, F.E.; Klumb, C.E.; Bacchi, C.E.; Seuanez, H.N.; Zalcberg, I.R. Epstein-Barr virus (EBV) detection and typing by PCR: A contribution to diagnostic screening of EBV-positive Burkitt’s lymphoma. Diagn. Pathol. 2006, 1, 17. [Google Scholar] [CrossRef] [Green Version]
- Klumb, C.E.; Hassan, R.; De Oliveira, D.E.; De Resende, L.M.; Carrico, M.K.; De Almeida Dobbin, J.; Pombo-De-Oliveira, M.S.; Bacchi, C.E.; Maia, R.C. Geographic variation in Epstein-Barr virus-associated Burkitt’s lymphoma in children from Brazil. Int. J. Cancer 2004, 108, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Klumb, C.E.; Hassan, R.; Zalcberg, I.R.; Resende, L.M.; Carrico, M.K.; Maia, R.C. p53 protein expression does not correlate with EBV status in childhood B non-Hodgkin lymphomas. Pediatr. Blood Cancer 2004, 43, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Pinto, M.T.; Ferreira, F.V.D.A.; Pitombeira, M.D.S.; Magalhães, S.M.M.; Costa, C.M.B.E.D.; Lima Filho, P.W.L.; Férrer, R.P.C.; Aguiar, A.L.P.D.; Rocha Filho, F.D. Analysis of the association between Epstein-Barr virus and classic Hodgkin s lymphoma in adult patients from Ceará (Brazil) by immunohistochemistry and in situ hybridization. J. Bras. Patol. Med. Lab. 2006, 42, 201–205. [Google Scholar] [CrossRef]
- Spector, N.; Milito, C.B.; Biasoli, I.; Luiz, R.R.; Pulcheri, W.; Morais, J.C. The prognostic value of the expression of Bcl-2, p53 and LMP-1 in patients with Hodgkin’s lymphoma. Leuk. Lymphoma 2005, 46, 1301–1306. [Google Scholar] [CrossRef] [PubMed]
- Loureiro, M.M.; Morais, J.C.; Milito, C.B.; Portugal, R.D.; Pulcheri, W.; Spector, N. Expression of Epstein-Barr virus in patients with Hodgkin’s disease: Report of 64 cases from Rio de Janeiro, Brazil. J. Bras. Patol. Med. Lab. 2004, 40, 37–40. [Google Scholar] [CrossRef] [Green Version]
- Vassallo, J.; Metze, K.; Traina, F.; de Souza, C.A.; Lorand-Metze, I. Expression of Epstein-Barr virus in classical Hodgkin’s lymphomas in Brazilian adult patients. Haematologica 2001, 86, 1227–1228. [Google Scholar]
- Vassallo, J.; Metze, K.; Traina, F.; de Souza, C.A.; Lorand-Metze, I. The prognostic relevance of apoptosis-related proteins in classical Hodgkin’s lymphomas. Leuk. Lymphoma 2003, 44, 483–488. [Google Scholar] [CrossRef]
- Elgui de Oliveira, D.; Bacchi, M.M.; Abreu, E.S.; Niero-Melo, L.; Bacchi, C.E. Hodgkin disease in adult and juvenile groups from two different geographic regions in Brazil: Characterization of clinicopathologic aspects and relationship with Epstein-Barr virus infection. Am. J. Clin. Pathol. 2002, 118, 25–30. [Google Scholar] [CrossRef]
- Altemani, A.; Barbosa, A.C.; Kulka, M.; Takahashi, T.; Endo, L.; Vassallo, J.; Lorand-Metze, I. Characteristics of nasal T/NK-cell lymphoma among Brazilians. Neoplasma 2002, 49, 55–60. [Google Scholar]
- Sandlund, J.T.; Fonseca, T.; Leimig, T.; Verissimo, L.; Ribeiro, R.; Lira, V.; Berard, C.W.; Sixbey, J.; Crist, W.M.; Mao, L.; et al. Predominance and characteristics of Burkitt lymphoma among children with non-Hodgkin lymphoma in northeastern Brazil. Leukemia 1997, 11, 743–746. [Google Scholar] [CrossRef] [Green Version]
- Razzouk, B.I.; Gan, Y.J.; Mendonca, C.; Jenkins, J.J.; Liu, Q.; Hudson, M.; Sixbey, J.W.; Ribeiro, R.C. Epstein-Barr virus in pediatric Hodgkin disease: Age and histiotype are more predictive than geographic region. Med. Pediatr. Oncol. 1997, 28, 248–254. [Google Scholar] [CrossRef]
- Araujo, I.; Foss, H.D.; Bittencourt, A.; Hummel, M.; Demel, G.; Mendonca, N.; Herbst, H.; Stein, H. Expression of Epstein-Barr virus-gene products in Burkitt’s lymphoma in Northeast Brazil. Blood 1996, 87, 5279–5286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bacchi, M.M.; Bacchi, C.E.; Alvarenga, M.; Miranda, R.; Chen, Y.Y.; Weiss, L.M. Burkitt’s lymphoma in Brazil: Strong association with Epstein-Barr virus. Mod. Pathol. 1996, 9, 63–67. [Google Scholar] [PubMed]
- Armstrong, A.; Alexander, F.; Paes, R.P.; Morad, N.; Gallagher, A.; Krajewski, A.; Jones, D.; Angus, B.; Adams, J.; Cartwright, R. Association of Epstein-Barr virus with pediatric Hodgkin’s disease. Am. J. Pathol. 1993, 142, 1683. [Google Scholar] [PubMed]
- Quintanilla-Martinez, L.; Ridaura, C.; Nagl, F.; Saez-de-Ocariz, M.; Duran-McKinster, C.; Ruiz-Maldonado, R.; Alderete, G.; Grube, P.; Lome-Maldonado, C.; Bonzheim, I.; et al. Hydroa vacciniforme-like lymphoma: A chronic EBV+ lymphoproliferative disorder with risk to develop a systemic lymphoma. Blood 2013, 122, 3101–3110. [Google Scholar] [CrossRef] [PubMed]
- Palma, I.; Sanchez, A.E.; Jimenez-Hernandez, E.; Alvarez-Rodriguez, F.; Nava-Frias, M.; Valencia-Mayoral, P.; Salinas-Lara, C.; Velazquez-Guadarrama, N.; Portilla-Aguilar, J.; Pena, R.Y.; et al. Detection of Epstein-Barr virus and genotyping based on EBNA2 protein in Mexican patients with hodgkin lymphoma: A comparative study in children and adults. Clin. Lymphoma Myeloma Leuk. 2013, 13, 266–272. [Google Scholar] [CrossRef]
- Garcéa-Álvarez, K.G.; Garibaldi-Covarrubias, R.; Flores-Márquez, M.R.; Ortiz-Hidalgo, C. Plasma cell myeloma associated with Epstein-Barr virus infection in an 11-year-old girl. Pediatr. Dev. Pathol. 2012, 15, 339–342. [Google Scholar] [CrossRef]
- Aviles-Salas, A.; Herrera-Goepfert, R.; Aguilar-Leon, D.; Candelaria-Hernandez, M.; Martinez-Cordero, E.; Corti, M. Plasmablastic lymphoma of the gastrointestinal tract in AIDS patients. Medicina 2011, 71, 536–541. [Google Scholar]
- Hofscheier, A.; Ponciano, A.; Bonzheim, I.; Adam, P.; Lome-Maldonado, C.; Vela, T.; Cortes, E.; Ortiz-Hidalgo, C.; Fend, F.; Quintanilla-Martinez, L. Geographic variation in the prevalence of Epstein-Barr virus-positive diffuse large B-cell lymphoma of the elderly: A comparative analysis of a Mexican and a German population. Mod. Pathol. 2011, 24, 1046–1054. [Google Scholar] [CrossRef] [Green Version]
- Dirnhofer, S.; Angeles-Angeles, A.; Ortiz-Hidalgo, C.; Reyes, E.; Gredler, E.; Krugmann, J.; Fend, F.; Quintanilla-Martinez, L. High prevalence of a 30-base pair deletion in the Epstein-Barr virus (EBV) latent membrane protein 1 gene and of strain type B EBV in Mexican classical Hodgkin’s disease and reactive lymphoid tissue. Hum. Pathol. 1999, 30, 781–787. [Google Scholar] [CrossRef]
- Elenitoba-Johnson, K.S.; Zarate-Osorno, A.; Meneses, A.; Krenacs, L.; Kingma, D.W.; Raffeld, M.; Jaffe, E.S. Cytotoxic granular protein expression, Epstein-Barr virus strain type, and latent membrane protein-1 oncogene deletions in nasal T-lymphocyte/natural killer cell lymphomas from Mexico. Mod. Pathol. 1998, 11, 754–761. [Google Scholar] [PubMed]
- Magana, M.; Sangueza, P.; Gil-Beristain, J.; Sanchez-Sosa, S.; Salgado, A.; Ramon, G.; Sangueza, O.P. Angiocentric cutaneous T-cell lymphoma of childhood (hydroa-like lymphoma): A distinctive type of cutaneous T-cell lymphoma. J. Am. Acad. Dermatol. 1998, 38, 574–579. [Google Scholar] [CrossRef]
- Quintanilla-Martinez, L.; Lome-Maldonado, C.; Schwarzmann, F.; Gredler, E.; Reyes, E.; Angeles-Angeles, A.; Fend, F. Post-transplantation lymphoproliferative disorders in Mexico: An aggressive clonal disease associated with Epstein-Barr virus type A. Mod. Pathol. 1998, 11, 200–208. [Google Scholar] [PubMed]
- Quintanilla-Martínez, L.; Lome-Maldonado, C.; Ott, G.; Gschwendtner, A.; Gredler, E.; Reyes, E.; Angeles-Angeles, A.; Fend, F. Primary non-Hodgkin’s lymphoma of the intestine: High prevalence of Epstein-Barr virus in Mexican lymphomas as compared with European cases. Blood J. Am. Soc. Hematol. 1997, 89, 644–651. [Google Scholar]
- Quintanilla-Martinez, L.; Gamboa-Dominguez, A.; Gamez-Ledesma, I.; Orozco-Estevez, H.; Angeles-Angeles, A. High prevalence of the Epstein-Barr virus in a Mexican population with Hodgkin’s disease. Rev. Investig. Clin. 1994, 46, 355–362. [Google Scholar]
- Quintanilla-Martinez, L.; Gamboa-Domnquez, A.; Gamez-Ledesma, I.; Angeles-Angeles, A.; Mohar, A. Association of Epstein-Barr virus latent membrane protein and Hodgkin’s disease in Mexico. Mod. Pathol. 1995, 8, 675–679. [Google Scholar]
- Zarate-Osorno, A.; Roman, L.N.; Kingma, D.W.; Meneses-Garcia, A.; Jaffe, E.S. Hodgkin’s disease in Mexico. Prevalence of Epstein-Barr virus sequences and correlations with histologic subtype. Cancer 1995, 75, 1360–1366. [Google Scholar] [CrossRef]
- Cordova Perez, F.J.; Gonzalez-Keelan, C.I.; Velez, R. Epstein-Barr virus in biopsies from patients with Hodgkin and non-Hodgkin lymphoma at the University of Puerto Rico immunohistochemistry laboratory. P. R. Health Sci. J. 2003, 22, 125–129. [Google Scholar]
- Aybar, A.; Krause, J.R. Coexpression of major histocompatibility complex class I and LMP1 in Epstein-Barr virus-positive Hodgkin’s lymphoma in a pediatric age group. Microsc. Res. Tech. 2005, 68, 247–249. [Google Scholar] [CrossRef]
- Riverend, E.; Rengifo, E.; Longchong, M.; Ruíz, R.; Tormo, B.; Garćia, J.; Portero, R.; Quintero, S.; Valdés, M.; Rodríguez, T.; et al. Burkitt’s lymphoma in Cuba. I. Clinical and morphological features and EBV association. Oncology 1984, 41, 13–18. [Google Scholar] [CrossRef]
- Quijano, S.; Saavedra, C.; Fiorentino, S.; Orozco, O.; Bravo, M.M. Epstein-Barr virus presence in Colombian Hodgkin lymphoma cases and its relation to treatment response. Biomedica 2004, 24, 163–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quijano, S.M.; Saavedra, C.; Bravo, M.M.; Fiorentino, S.; Orozco, O. Expression of heat shock proteins HSP72 and HSP73 in Colombian patients with Hodgkin lymphoma positive and negative for Epstein Barr virus. Rev. Med. Chile 2003, 131, 1375–1381. [Google Scholar] [CrossRef] [PubMed]
- Beltran, B.E.; Quinones, P.; Morales, D.; Malaga, J.M.; Chavez, J.C.; Sotomayor, E.M.; Castillo, J.J. Response and survival benefit with chemoimmunotherapy in Epstein-Barr virus-positive diffuse large B-cell lymphoma. Hematol. Oncol. 2018, 36, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, C.; Beltran, B.; Quiñones, P.; Carbajal, T.; Vilcapaza, J.; Yabar, A.; Segura, P.; Quintanilla-Martinez, L.; Miranda, R.N.; Castillo, J.J. Large B-cell lymphoma arising in cardiac myxoma or intracardiac fibrinous mass: A localized lymphoma usually associated with Epstein-Barr virus? Cardiovasc. Pathol. 2015, 24, 60–64. [Google Scholar] [CrossRef]
- Beltran, B.E.; Maza, I.; Moises-Alfaro, C.B.; Vasquez, L.; Quinones, P.; Morales, D.; Sanchez, G.; Paredes, G.; Oscanoa, M.; Geronimo, J.; et al. Thalidomide for the treatment of hydroa vacciniforme-like lymphoma: Report of four pediatric cases from Peru. Am. J. Hematol. 2014, 89, 1160–1161. [Google Scholar] [CrossRef]
- Ernesto Beltran, B.; Quinones Avila, P.; Morales Luna, D.; Cotrina Montenegro, E.; Gallo Lopez, A.; Lopez Ilasaca, M. Gastrointestinal Epstein Barr virus positive diffuse large B cell lymphoma in elderly: Report of five cases and review of literature. Rev. Gastroenterol. Peru 2011, 31, 285–288. [Google Scholar]
- Rodriguez-Pinilla, S.M.; Barrionuevo, C.; Garcia, J.; de los Angeles, M.; Pajares, R.; Casavilca, S.; Montes, J.; Martinez, A.; Montes-Moreno, S.; Sanchez, L.; et al. Epstein-Barr virus-positive systemic NK/T-cell lymphomas in children: Report of six cases. Histopathology 2011, 59, 1183–1193. [Google Scholar] [CrossRef]
- Beltran, B.E.; Castillo, J.J.; Morales, D.; de Mendoza, F.H.; Quinones, P.; Miranda, R.N.; Gallo, A.; Lopez-Ilasaca, M.; Butera, J.N.; Sotomayor, E.M. EBV-positive diffuse large B-cell lymphoma of the elderly: A case series from Peru. Am. J. Hematol. 2011, 86, 663–667. [Google Scholar] [CrossRef]
- Morales, D.; Beltran, B.; De Mendoza, F.H.; Riva, L.; Yabar, A.; Quinones, P.; Butera, J.N.; Castillo, J. Epstein-Barr virus as a prognostic factor in de novo nodal diffuse large B-cell lymphoma. Leuk. Lymphoma 2010, 51, 66–72. [Google Scholar] [CrossRef]
- Beltran, B.; Salas, R.; Quiñones, P.; Morales, D.; Hurtado, F.; Cotrina, E.; Riva, L.; Castillo, J. EBV-positive diffuse large B-cell lymphoma in a human T-lymphotropic virus type 1 carrier. Infect. Agent. Cancer 2009, 4, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Pinilla, S.M.; Barrionuevo, C.; Garcia, J.; Martinez, M.T.; Pajares, R.; Montes-Moreno, S.; Casavilca, S.; Montes, J.; Bravo, F.; Zaharia, M.; et al. EBV-associated cutaneous NK/T-cell lymphoma: Review of a series of 14 cases from peru in children and young adults. Am. J. Surg. Pathol. 2010, 34, 1773–1782. [Google Scholar] [CrossRef] [PubMed]
- Barrionuevo, C.; Zaharia, M.; Martinez, M.T.; Taxa, L.; Misad, O.; Moscol, A.; Sarria, G.; Guerrero, I.; Casanova, L.; Flores, C.; et al. Extranodal NK/T-cell lymphoma, nasal type: Study of clinicopathologic and prognosis factors in a series of 78 cases from Peru. Appl. Immunohistochem. Mol. Morphol. 2007, 15, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Barrionuevo, C.; Anderson, V.M.; Zevallos-Giampietri, E.; Zaharia, M.; Misad, O.; Bravo, F.; Caceres, H.; Taxa, L.; Martinez, M.T.; Wachtel, A.; et al. Hydroa-like cutaneous T-cell lymphoma: A clinicopathologic and molecular genetic study of 16 pediatric cases from Peru. Appl. Immunohistochem. Mol. Morphol. 2002, 10, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Quintanilla-Martinez, L.; Franklin, J.L.; Guerrero, I.; Krenacs, L.; Naresh, K.N.; Rama-Rao, C.; Bhatia, K.; Raffeld, M.; Magrath, I.T. Histological and immunophenotypic profile of nasal NK/T cell lymphomas from Peru: High prevalence of p53 overexpression. Hum. Pathol. 1999, 30, 849–855. [Google Scholar] [CrossRef]
- Arber, D.A.; Weiss, L.M.; Albújar, P.F.; Chen, Y.Y.; Jaffe, E.S. Nasal lymphomas in Peru. High incidence of T-cell immunophenotype and Epstein-Barr virus infection. Am. J. Surg. Pathol. 1993, 17, 392–399. [Google Scholar] [CrossRef]
- Chang, K.L.; Albujar, P.F.; Chen, Y.Y.; Johnson, R.M.; Weiss, L.M. High prevalence of Epstein-Barr virus in the Reed-Sternberg cells of Hodgkin’s disease occurring in Peru. Blood 1993, 81, 496–501. [Google Scholar] [CrossRef]
- Montalvo, N.; Redroban, L. Hydroa Vacciniforme-Like EBV-Positive Cutaneous T-Cell Lymphoma, First Report of 2 Cases in Ecuador. Am. J. Dermatopathol. 2016, 38, e57–e59. [Google Scholar] [CrossRef]
- Sánchez-Giler, S.; Herrera-Vásquez, A.; Castillo-Zambrano, C.; Solórzano-Alava, L.; Zambrano-Castro, D.; Kuon-Yeng, C.; Silva-Orellana, A.; Murillo-Zambrano, J.; Cucalón-González, G. Detección del Virus de Epstein-Barr en linfoma mediante qPCR//Detection of Epstein-Barr Virus (EBV) in lymphoma through qPCR. Ciencia Unemi 2018, 11, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Zoroquiain, P.; González, S.; Molgó, M.; Rodríguez, A.; Valbuena, J.R. Leukocytoclastic vasculitis as early manifestation of Epstein-Barr virus-positive diffuse large B-cell lymphoma of the elderly. Am. J. Dermatopathol. 2012, 34, 330–334. [Google Scholar] [CrossRef]
- Martin, C.; Carrasco, C.; Sotomayor, C.; Otth, C. Prevalence of Epstein-Barr virus associated with nasal lymphoma in patients attending the regional hospital of Valdivia, Chile, between 1987 and 2005. J. Med. Virol. 2010, 82, 825–828. [Google Scholar] [CrossRef]
- Cabrera, M.E.; Eizuru, Y.; Itoh, T.; Koriyama, C.; Tashiro, Y.; Ding, S.; Rey, S.; Akiba, S.; Corvalan, A. Nasal natural killer/T-cell lymphoma and its association with type “i”/XhoI loss strain Epstein-Barr virus in Chile. J. Clin. Pathol. 2007, 60, 656–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutierrez, M.I.; Bhatia, K.; Barriga, F.; Diez, B.; Muriel, F.S.; de Andreas, M.L.; Epelman, S.; Risueno, C.; Magrath, I.T. Molecular epidemiology of Burkitt’s lymphoma from South America: Differences in breakpoint location and Epstein-Barr virus association from tumors in other world regions. Blood 1992, 79, 3261–3266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambinder, R.F.; Browning, P.J.; Lorenzana, I.; Leventhal, B.G.; Cosenza, H.; Mann, R.B.; MacMahon, E.M.; Medina, R.; Cardona, V.; Grufferman, S.; et al. Epstein-Barr virus and childhood Hodgkin’s disease in Honduras and the United States. Blood 1993, 81, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Monterroso, V.; Zhou, Y.; Koo, S.; Glackin, C.; Bujan, W.; Medeiros, L.J. Hodgkin’s disease in Costa Rica: A report of 40 cases analyzed for Epstein-Barr virus. Am. J. Clin. Pathol. 1998, 109, 618–624. [Google Scholar] [CrossRef] [Green Version]
- Weinreb, M.; Day, P.J.; Niggli, F.; Powell, J.E.; Raafat, F.; Hesseling, P.B.; Schneider, J.W.; Hartley, P.S.; Tzortzatou-Stathopoulou, F.; Khalek, E.R.; et al. The role of Epstein-Barr virus in Hodgkin’s disease from different geographical areas. Arch. Dis. Child. 1996, 74, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Gulley, M.L.; Eagan, P.A.; Quintanilla-Martinez, L.; Picado, A.L.; Smir, B.N.; Childs, C.; Dunn, C.D.; Craig, F.E.; Williams, J.W., Jr.; Banks, P.M. Epstein-Barr virus DNA is abundant and monoclonal in the Reed-Sternberg cells of Hodgkin’s disease: Association with mixed cellularity subtype and Hispanic American ethnicity. Blood 1994, 83, 1595–1602. [Google Scholar] [CrossRef] [Green Version]
- Takano, Y.; Colanzi, R.P.; Siga, J. High incidence of Epstein-Barr virus associated non-Hodgkin’s lymphomas in the Bolivian mountains. Pathol. Int. 1994, 44, 237–240. [Google Scholar] [CrossRef]
- Schwartz, E.J.; Molina-Kirsch, H.; Zhao, S.; Marinelli, R.J.; Warnke, R.A.; Natkunam, Y. Immunohistochemical characterization of nasal-type extranodal NK/T-cell lymphoma using a tissue microarray: An analysis of 84 cases. Am. J. Clin. Pathol. 2008, 130, 343–351. [Google Scholar] [CrossRef]
- Grufferman, S.; Delzell, E. Epidemiology of Hodgkin’s disease. Epidemiol. Rev. 1984, 6, 76–106. [Google Scholar] [CrossRef]
- Howlader, N.N.A.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.L.D.; Chen, H.S.; Feuer, E.J.; et al. SEER Cancer Statistics Review, 1975–2016; National Cancer Institute: Bethesda, MD, USA, 2016.
- Macfarlane, G.J.; Evstifeeva, T.; Boyle, P.; Grufferman, S. International patterns in the occurrence of Hodgkin’s disease in children and young adult males. Int. J. Cancer 1995, 61, 165–169. [Google Scholar] [CrossRef]
- Kalisz, K.; Alessandrino, F.; Beck, R.; Smith, D.; Kikano, E.; Ramaiya, N.H.; Tirumani, S.H. An update on Burkitt lymphoma: A review of pathogenesis and multimodality imaging assessment of disease presentation, treatment response, and recurrence. Insights Imaging 2019, 10, 56. [Google Scholar] [CrossRef] [PubMed]
- Crawford, D.H. Biology and disease associations of Epstein-Barr virus. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2001, 356, 461–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, J.M.; Klumb, C.E.; de Souza Reis, R.; de Oliveira Santos, M.; Oliveira, J.F.; de Camargo, B.; Pombo-de-Oliveira, M.S. Lymphoma subtype incidence rates in children and adolescents: First report from Brazil. Cancer Epidemiol. 2012, 36, e221–e226. [Google Scholar] [CrossRef] [PubMed]
- Chabay, P.A.; Preciado, M.V. EBV primary infection in childhood and its relation to B-cell lymphoma development: A mini-review from a developing region. Int. J. Cancer 2013, 133, 1286–1292. [Google Scholar] [CrossRef] [PubMed]
- Pedraza, R.M.; Arboleda, L.P.A.; Sanchez-Romero, C.; Quinones, J.A.A.; Tovar, C.J.M.; Henao, J.R.; de Almeida, O.P. Intraoral EBV-positive sporadic Burkitt lymphoma in an elderly patient with bilateral presentation. Autops. Case Rep. 2019, 9, e2019117. [Google Scholar] [CrossRef]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues; IARC Press: Lyon, France, 2008.
- Shimoyama, Y.; Yamamoto, K.; Asano, N.; Oyama, T.; Kinoshita, T.; Nakamura, S. Age-related Epstein-Barr virus-associated B-cell lymphoproliferative disorders: Special references to lymphomas surrounding this newly recognized clinicopathologic disease. Cancer Sci. 2008, 99, 1085–1091. [Google Scholar] [CrossRef]
- Hoeller, S.; Tzankov, A.; Pileri, S.A.; Went, P.; Dirnhofer, S. Epstein-Barr virus-positive diffuse large B-cell lymphoma in elderly patients is rare in Western populations. Hum. Pathol. 2010, 41, 352–357. [Google Scholar] [CrossRef]
- Beltran, B.; Morales, D.; Quiñones, P.; Salas, R.; Carrasco-Yalan, A.A. Distribution and Pathology Characteristics of Non Hodgkin Lymphoma in Peru: A Study of 1014 Cases Using WHO Classification of Lymphoid Neoplasm. Blood 2007, 110, 4419. [Google Scholar] [CrossRef]
- Babcock, G.J.; Decker, L.L.; Volk, M.; Thorley-Lawson, D.A. EBV persistence in memory B cells in vivo. Immunity 1998, 9, 395–404. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.Y.; Montes-Mojarro, I.A.; Fend, F.; Quintanilla-Martinez, L. Epstein-Barr Virus-Associated T and NK-Cell Lymphoproliferative Diseases. Front. Pediatr. 2019, 7, 71. [Google Scholar] [CrossRef] [Green Version]
- Coleman, C.B.; Lang, J.; Sweet, L.A.; Smith, N.A.; Freed, B.M.; Pan, Z.; Haverkos, B.; Pelanda, R.; Rochford, R. Epstein-Barr Virus Type 2 Infects T Cells and Induces B Cell Lymphomagenesis in Humanized Mice. J. Virol. 2018, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coleman, C.B.; Wohlford, E.M.; Smith, N.A.; King, C.A.; Ritchie, J.A.; Baresel, P.C.; Kimura, H.; Rochford, R. Epstein-Barr virus type 2 latently infects T cells, inducing an atypical activation characterized by expression of lymphotactic cytokines. J. Virol. 2015, 89, 2301–2312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J.I.; Jaffe, E.S.; Dale, J.K.; Pittaluga, S.; Heslop, H.E.; Rooney, C.M.; Gottschalk, S.; Bollard, C.M.; Rao, V.K.; Marques, A.; et al. Characterization and treatment of chronic active Epstein-Barr virus disease: A 28-year experience in the United States. Blood 2011, 117, 5835–5849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engels, E.A.; Pfeiffer, R.M.; Goedert, J.J.; Virgo, P.; McNeel, T.S.; Scoppa, S.M.; Biggar, R.J. Trends in cancer risk among people with AIDS in the United States 1980–2002. Aids 2006, 20, 1645–1654. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Siegel, R.; Torre, L.; Jemal, A. Global and Regional Estimates of the Incidence and Mortality for 38 Cancers: GLOBOCAN 2018; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2018.
- Chadburn, A.; Said, J.; Gratzinger, D.; Chan, J.K.; de Jong, D.; Jaffe, E.S.; Natkunam, Y.; Goodlad, J.R. HHV8/KSHV-Positive Lymphoproliferative Disorders and the Spectrum of Plasmablastic and Plasma Cell Neoplasms: 2015 SH/EAHP Workshop Report-Part 3. Am. J. Clin. Pathol. 2017, 147, 171–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calabro, M.L.; Sarid, R. Human Herpesvirus 8 and Lymphoproliferative Disorders. Mediterr. J. Hematol. Infect. Dis. 2018, 10, e2018061. [Google Scholar] [CrossRef]
- Kapelushnik, J.; Ariad, S.; Benharroch, D.; Landau, D.; Moser, A.; Delsol, G.; Brousset, P. Post renal transplantation human herpesvirus 8-associated lymphoproliferative disorder and Kaposi’s sarcoma. Br. J. Haematol. 2001, 113, 425–428. [Google Scholar] [CrossRef]
- Di Minno, G.; Perno, C.F.; Tiede, A.; Navarro, D.; Canaro, M.; Guertler, L.; Ironside, J.W. Current concepts in the prevention of pathogen transmission via blood/plasma-derived products for bleeding disorders. Blood Rev. 2016, 30, 35–48. [Google Scholar] [CrossRef] [Green Version]
- Pellett, P.E.; Wright, D.J.; Engels, E.A.; Ablashi, D.V.; Dollard, S.C.; Forghani, B.; Glynn, S.A.; Goedert, J.J.; Jenkins, F.J.; Lee, T.H.; et al. Multicenter comparison of serologic assays and estimation of human herpesvirus 8 seroprevalence among US blood donors. Transfusion 2003, 43, 1260–1268. [Google Scholar] [CrossRef]
- Ferreira, S.; Sanabani, S.; Reis, A.D.; Chamone, D.F.; Sabino, E.C. Human herpesvirus type 8 among Brazilian blood donors. Transfusion 2003, 43, 1764–1765. [Google Scholar] [CrossRef]
- Perez, C.; Tous, M.; Gallego, S.; Zala, N.; Rabinovich, O.; Garbiero, S.; Martinez, M.J.; Cunha, A.M.; Camino, S.; Camara, A.; et al. Seroprevalence of human herpesvirus-8 in blood donors from different geographical regions of Argentina, Brazil, and Chile. J. Med. Virol. 2004, 72, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Zago, A.; Bourboulia, D.; Viana, M.C.; Collandre, H.; Dietze, R.; Boshoff, C.; Keller, R. Seroprevalence of human herpesvirus 8 and its association with Kaposi sarcoma in Brazil. Sex. Transm. Dis. 2000, 27, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, M.C.; de Souza, V.A.; Sumita, L.M.; Freire, W.; Weiss, H.A.; Sabino, E.C.; Franceschi, S.; Pannuti, C.S.; Mayaud, P. Prevalence of, and risk factors for Kaposi’s sarcoma-associated herpesvirus infection among blood donors in Brazil: A multi-center serosurvey. J. Med. Virol. 2008, 80, 1202–1210. [Google Scholar] [CrossRef] [PubMed]
- Magri, M.C.; Carbone, P.H.; de los Santos-Fortuna, E.; Caterino-de-Araujo, A. A comparative study of the frequency of antibody and titers against human herpesvirus 8 latent and lytic antigens in “at-risk” individuals and among patients with Kaposi’s sarcoma. J. Med. Virol. 2009, 81, 1292–1297. [Google Scholar] [CrossRef]
- Nascimento, M.C.; Sumita, L.M.; Souza, V.U.; Weiss, H.A.; Oliveira, J.; Mascheretti, M.; Quiroga, M.; Vela, R.A.; Sabino, E.; Pannuti, C.S.; et al. Seroprevalence of Kaposi sarcoma-associated herpesvirus and other serologic markers in the Brazilian Amazon. Emerg. Infect. Dis. 2009, 15, 663–667. [Google Scholar] [CrossRef]
- Avelleira, J.C.; Lupi, O.; Caterino-de-Araujo, A.; Santos-Fortuna Ede, L. Seroprevalence of HHV-8 infection in the pediatric population of two university hospitals in Rio de Janeiro, Brazil. Int. J. Dermatol. 2006, 45, 381–383. [Google Scholar] [CrossRef]
- Chagas, C.A.; Endo, L.H.; Sakano, E.; Pinto, G.A.; Brousset, P.; Vassallo, J. Detection of herpesvirus type 8 (HHV8) in children’s tonsils and adenoids by immunohistochemistry and in situ hybridization. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 65–72. [Google Scholar] [CrossRef]
- Freitas, R.B.; Freitas, M.R.; Linhares, A.C. Prevalence of human herpesvirus 8 antibodies in the population of Belém, Pará, Brazil. Rev. Inst. Med. Trop. São Paulo 2002, 44, 309–313. [Google Scholar] [CrossRef]
- Colleoni, G.W.; Duarte, L.C.; Kerbauy, F.R.; Lobão, M.; Yunis, M.P.; Alves, A.C.; de Souza, V.A.; Bordin, J.O.; de Oliveira, J.S. 2-Chloro-deoxyadenosine induces durable complete remission in Castleman’s disease but may accelerate its transformation to non-Hodgkin’s lymphoma. Acta Oncol. 2003, 42, 784–787. [Google Scholar] [CrossRef] [Green Version]
- Caroline Ribeiro Sales, A.; Romao de Souza Junior, V.; Iglis de Oliveira, M.; Azevedo Braga Albuquerque, C.; de Barros Campelo Junior, E.; Sergio Ramos de Araujo, P. Multicentric Castleman’s disease in human immunodeficiency virus infection: Two case reports. J. Med. Case Rep. 2018, 12, 1–4. [Google Scholar] [CrossRef]
- Naime Fde, F.; Fakhouri, F.; Martins, C.S.; Couto, W.J. HIV-associated multicentric Castleman’s disease. Rare Tumors 2012, 4, 127–129. [Google Scholar] [CrossRef] [PubMed]
- Pinto, L.W.; Nunes, E.P. Simultaneous lymph node involvement by Castleman disease and Kaposi sarcoma. Rev. Bras. Hematol. Hemoter. 2011, 33, 73–76. [Google Scholar] [PubMed] [Green Version]
- Sousa, V.; Carvalho, L. Mediastinal angiofolicular lymphoid hyperplasia—Castleman’s disease—Case report. Rev. Port. Pneumol. 2006, 12, 275–280. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, P.Y.; Atala, M.M.; Pereira, J.; Caterino-de-Araujo, A. Primary effusion lymphoma with cardiac involvement in HIV positive patient-complete response and long survival with chemotherapy and HAART. J. Clin. Virol. 2009, 44, 84–85. [Google Scholar] [CrossRef] [PubMed]
- Cunha, A.; Costa, S.C.; Lima, C.S.; Ortega, M.; Costa, F.F. Low incidence of human herpesvirus 8 in bone marrow samples from Brazilian patients with multiple myeloma. Acta Haematol. 2001, 105, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Hulaniuk, M.L.; Torres, O.; Bartoli, S.; Fortuny, L.; Burgos Pratx, L.; Nunez, F.; Salamone, H.; Corach, D.; Trinks, J.; Caputo, M. Increased prevalence of human herpesvirus type 8 (HHV-8) genome among blood donors from North-Western Argentina. J. Med. Virol. 2017, 89, 518–527. [Google Scholar] [CrossRef]
- Perez, C.L.; Tous, M.I.; Zala, N.; Camino, S. Human herpesvirus 8 in healthy blood donors, Argentina. Emerg. Infect. Dis. 2010, 16, 150–151. [Google Scholar] [CrossRef]
- De Sanjose, S.; Mbisa, G.; Perez-Alvarez, S.; Benavente, Y.; Sukvirach, S.; Hieu, N.T.; Shin, H.R.; Anh, P.T.; Thomas, J.; Lazcano, E.; et al. Geographic variation in the prevalence of Kaposi sarcoma-associated herpesvirus and risk factors for transmission. J. Infect. Dis. 2009, 199, 1449–1456. [Google Scholar] [CrossRef]
- Corti, M.; Villafañe, M.F.; Solari, R.; De Carolis, L.; Cangelosi, D.; Santoro, J.; Schtirbu, R.; Lewi, D.; Bistmans, A.; Narbaitz, M.; et al. Non-Hodgkin lymphomas of the oral cavity in AIDS patients in a reference hospital of infectious diseases in Argentina: Report of eleven cases and review of the literature. J. Gastrointest. Cancer 2011, 42, 143–148. [Google Scholar] [CrossRef]
- Cacciari, V.; Arra, A.; D’Alessandro, D.; Errea, S.; Kohan, D.; Elsner, B.; Benetucci, J. Enfermedad de Castleman e infección por HIV. Presentación de dos casos y revisión de la literatura. Actual. Sida Infectol. 2015, 23, 32–40. [Google Scholar]
- Perez, C.L.; Rudoy, S. Anti-CD20 monoclonal antibody treatment of human herpesvirus 8-associated, body cavity-based lymphoma with an unusual phenotype in a human immunodeficiency virus-negative patient. Clin. Diagn. Lab. Immunol. 2001, 8, 993–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez, C.L.; Tous, M.I. Diversity of human herpesvirus 8 genotypes in patients with AIDS and non-AIDS associated Kaposi’s sarcoma, Castleman’s disease and primary effusion lymphoma in Argentina. J. Med. Virol. 2017, 89, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Mohanna, S.; Portillo, J.A.; Carriquiry, G.; Vidal, J.; Ferrufino, J.C.; Sanchez, J.; Bravo, F.; Gotuzzo, E. Human herpesvirus-8 in Peruvian blood donors: A population with hyperendemic disease? Clin. Infect. Dis. 2007, 44, 558–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohanna, S.; Sanchez, J.; Ferrufino, J.C.; Bravo, F.; Gotuzzo, E. Characteristics of Castleman’s disease in Peru. Eur. J. Intern. Med. 2006, 17, 170–174. [Google Scholar] [CrossRef]
- Sevilla-Lizcano, D.B.; Frias-Soria, C.L.; Ortiz-Hidalgo, C. Castleman disease. Histopathological and immunohistochemical analysis of 39 cases. Gac. Med. Mex. 2017, 153, 550–558. [Google Scholar]
- Sobrevilla-Calvo Pde, J.; Avilés-Salas, A.; Cortés-Padilla, D.E.; Rivas-Vera, S. Clinical and pathological features of Castleman’s disease: Experience at the Instituto Nacional de Cancerología, Mexico City. Cir. Cir. 2009, 77, 187–192. [Google Scholar]
- Sanchez-Pena, P.; Romero-Guadarrama, M.B.; Aguirre-Garcia, J. Diseases associated with HIV infection: Study of biopsies and surgical resection specimens at a large general hospital in Mexico City. Ann. Diagn. Pathol. 2009, 13, 162–167. [Google Scholar] [CrossRef]
- Avilés-Salas, A.; Candelaria, M.; Sevilla-Lizcano, D.B.; Burgos, S. Large B-cell lymphoma coexisting with Castleman’s disease. Report of one case. Rev. Med. Chile 2017, 145, 945–949. [Google Scholar]
- Avilés-Salas, A.; Cornejo-Juárez, P.; Sobrevilla-Calvo Pde, J. Coexistence of plasmablastic lymphoma, Kaposi sarcoma and Castleman disease in a patient with HIV infection. Rev. Chil. Infectol. 2011, 28, 76–80. [Google Scholar] [CrossRef] [Green Version]
- Mayor, A.M.; Gómez, M.A.; Ríos-Olivares, E.; Hunter-Mellado, R.F. AIDS-defining neoplasm prevalence in a cohort of HIV-infected patients, before and after highly active antiretroviral therapy. Ethn. Dis. 2008, 18, S2-189-94. [Google Scholar]
- Kouri, V.; Eng, S.M.; Rodriguez, M.E.; Resik, S.; Orraca, O.; Moore, P.S.; Chang, Y. Seroprevalence of Kaposi’s sarcoma-associated herpesvirus in various populations in Cuba. Rev. Panam.Salud Pública 2004, 15, 320–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kouri, V.; Martinez, P.A.; Capo, V.; Blanco, O.; Rodriguez, M.E.; Jimenez, N.; Fleites, G.; Caballero, I.; Dovigny, M.C.; Aleman, Y.; et al. Kaposi’s Sarcoma and Human Herpesvirus 8 in Cuba: Evidence of subtype B expansion. Virology 2012, 432, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, L.; Serraino, D.; Rezza, G.; Lence, J.; Ortiz, R.M.; Cruz, T.; Vaccarella, S.; Sarmati, L.; Andreoni, M.; Franceschi, S. Infection with human herpesvirus type 8 and human T-cell leukaemia virus type 1 among individuals participating in a case-control study in Havana City, Cuba. Br. J. Cancer 2002, 87, 1253–1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez Silva, H.; Buchaca Faxas, E.; Machado Puerto, I.; Pérez Román, G.; Pérez Caballero, D. Castleman’s disease. Review of five cases. Anal. Med. Interna 2005, 22, 24–27. [Google Scholar]
- Orozco, B.; Gómez, L.M.; Estrada, S.; Restrepo, B.N.; Cataño, J.C. Relación entre el virus humano herpes 8 y el sarcoma de Kaposi en pacientes positivos y negativos para el VIH. Infectio 2011, 11, 111–116. [Google Scholar]
- Guanira, J.V.; Casper, C.; Lama, J.R.; Morrow, R.; Montano, S.M.; Caballero, P.; Suarez, L.; Whittington, W.L.; Wald, A.; Sanchez, J.; et al. Prevalence and correlates of human herpesvirus 8 infection among Peruvian men who have sex with men. J. Acquir. Immune Defic. Syndr. 2008, 49, 557–562. [Google Scholar] [CrossRef] [Green Version]
- Mohanna, S.; Maco, V.; Gown, A.; Morales, D.; Bravo, F.; Gotuzzo, E. Is classic Kaposi’s sarcoma endemic in Peru?: Report of a case in an indigenous patient. Am. J. Trop. Med. Hyg. 2006, 75, 324–326. [Google Scholar] [CrossRef]
- Revilla-Lopez, J.; Mendoza-Fabian, R.; Anampa-Guzman, A.; Rosales-Zuniga, J.; Chalco-Huaman, J. Endemic kaposi’s sarcoma in a HIV-Negative patient. Rev. Peru. Med. Exp. Salud Publica 2015, 32, 808–812. [Google Scholar]
- Mohanna, S.; Ferrufino, J.C.; Sanchez, J.; Bravo, F.; Gotuzzo, E. Epidemiological and clinical characteristics of classic Kaposi’s sarcoma in Peru. J. Am. Acad. Dermatol. 2005, 53, 435–441. [Google Scholar] [CrossRef]
- Jessurun, J.; Angeles-Angeles, A.; Gasman, N. Comparative demographic and autopsy findings in acquired immune deficiency syndrome in two Mexican populations. J. Acquir. Immune Defic. Syndr. 1990, 3, 579–583. [Google Scholar]
- Ramirez-Amador, V.; Esquivel-Pedraza, L.; Sierra-Madero, J.; Anaya-Saavedra, G.; Gonzalez-Ramirez, I.; Ponce-de-Leon, S. The Changing Clinical Spectrum of Human Immunodeficiency Virus (HIV)-Related Oral Lesions in 1,000 Consecutive Patients: A 12-Year Study in a Referral Center in Mexico. Medicine 2003, 82, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Kourí, V.; Martínez, P.A.; Blanco, O.; Capó, V.; Rodríguez, M.E.; Dovigny Mdel, C.; Cardellá, L.; Gala, A.; Jiménez, N.A.; Luzardo, C.; et al. Kaposi’s sarcoma-associated herpesvirus load in asymptomatic contacts of Cuban epidemic KS patients. Arch. Virol. 2010, 155, 1971–1976. [Google Scholar] [CrossRef] [PubMed]
- Braz-Silva, P.H.; Tozetto-Mendoza, T.R.; Sumita, L.M.; Freire, W.; Palmieri, M.; do Canto, A.M.; Avelino-Silva, V.I.; Gallottini, M.; Mayaud, P.; Pannuti, C.S. Prospective study of human herpesvirus 8 oral shedding, viremia, and serological status among human immunodeficiency virus seropositive and seronegative individuals in Sao Paulo, Brazil. J. Oral Microbiol. 2017, 9, 1384287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Oliveira Mendes Cahu, G.G.; Morais, V.M.; Lopes, T.R.; da Silva, D.M.; Tozetto-Mendoza, T.R.; Pannuti, C.S.; Cunha Duarte Coelho, M.R. Prevalence of human herpesvirus 8 infection in people living with HIV/AIDS in Pernambuco, Brazil. J. Med. Virol. 2016, 88, 2016–2020. [Google Scholar] [CrossRef] [PubMed]
- Ishak Mde, O.; Martins, R.N.; Machado, P.R.; de Souza, L.L.; Machado, L.F.; Azevedo, V.N.; Katano, H.; Sata, T.; Hasegawa, H.; Vallinoto, A.C.; et al. High diversity of HHV-8 molecular subtypes in the Amazon region of Brazil: Evidence of an ancient human infection. J. Med. Virol. 2007, 79, 1537–1544. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.R.; Farias, K.J.; Pereira, M.G.; Freitas, P.P.; Fonseca, B.A. Human herpesvirus 8 (HHV-8) detected by nested polymerase chain reaction (PCR) in HIV patients with or without Kaposi’s sarcoma. An analytic cross-sectional study. Sao Paulo Med. J. 2015, 134, 187–192. [Google Scholar] [CrossRef] [Green Version]
- Pierrotti, L.C.; Etzel, A.; Sumita, L.M.; Braga, P.E.; Eluf-Neto, J.; de Souza, V.A.; Segurado, A.A. Human herpesvirus 8 (HHV-8) infection in HIV/AIDS patients from Santos, Brazil: Seroprevalence and associated factors. Sex. Transm. Dis. 2005, 32, 57–63. [Google Scholar] [CrossRef]
- Sosa, C.; Klaskala, W.; Chandran, B.; Soto, R.; Sieczkowski, L.; Wu, M.H.; Baum, M.; Wood, C. Human herpesvirus 8 as a potential sexually transmitted agent in Honduras. J. Infect. Dis. 1998, 178, 547–551. [Google Scholar] [CrossRef] [Green Version]
- Sosa, C.; Benetucci, J.; Hanna, C.; Sieczkowski, L.; Deluchi, G.; Canizal, A.M.; Mantina, H.; Klaskala, W.; Baum, M.; Wood, C. Human herpesvirus 8 can be transmitted through blood in drug addicts. Medicina 2001, 61, 291–294. [Google Scholar]
- Whitby, D.; Marshall, V.A.; Bagni, R.K.; Wang, C.D.; Gamache, C.J.; Guzman, J.R.; Kron, M.; Ebbesen, P.; Biggar, R.J. Genotypic characterization of Kaposi’s sarcoma-associated herpesvirus in asymptomatic infected subjects from isolated populations. J. Gen. Virol. 2004, 85, 155–163. [Google Scholar] [CrossRef]
- Cunha, A.M.; Caterino-de-Araujo, A.; Costa, S.C.; Santos-Fortuna, E.; Boa-Sorte, N.C.; Goncalves, M.S.; Costa, F.F.; Galvao-Castro, B. Increasing seroprevalence of human herpesvirus 8 (HHV-8) with age confirms HHV-8 endemicity in Amazon Amerindians from Brazil. J. Gen. Virol. 2005, 86, 2433–2437. [Google Scholar] [CrossRef] [PubMed]
- De Souza, V.A.; Sumita, L.M.; Nascimento, M.C.; Oliveira, J.; Mascheretti, M.; Quiroga, M.; Freire, W.S.; Tateno, A.; Boulos, M.; Mayaud, P.; et al. Human herpesvirus-8 infection and oral shedding in Amerindian and non-Amerindian populations in the Brazilian Amazon region. J. Infect. Dis. 2007, 196, 844–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souza, V.A.; Salzano, F.M.; Petzl-Erler, M.L.; Nascimento, M.C.; Mayaud, P.; Borges, J.D.; Pannuti, C.S. Variations in human herpesvirus type 8 seroprevalence in Native Americans, South America. Emerg. Infect. Dis. 2010, 16, 1003–1006. [Google Scholar] [CrossRef] [PubMed]
- Corti, M.; de Dios Soler, M.; Bare, P.; Villafañe, M.F.; de Tezanos Pinto, M.; Pérez Bianco, R.; Narbaitz, M. Linfomas asociados con la infección por el virus de la inmunodeficiencia humana: Subtipos histológicos y asociación con los virus de Epstein Barr y Herpes-8. Medicina 2010, 70, 151–158. [Google Scholar] [PubMed]
- Hernàndez, D.E.; Masquelier, B.; Pèrez, O.; Oliver, M.; Fleury, H.J. Human herpesvirus 8 variants in Venezuelan patients with AIDS-related Kaposi sarcoma. Clin. Infect. Dis. 2003, 36, 385–386. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.X.; Sata, T.; Stamey, F.R.; Voevodin, A.; Katano, H.; Koizumi, H.; Deleon, M.; De Cristofano, M.A.; Galimberti, R.; Pellett, P.E. Molecular characterization of strains of Human herpesvirus 8 from Japan, Argentina and Kuwait. J. Gen. Virol. 2001, 82, 499–506. [Google Scholar] [CrossRef]
- Vassallo, J.; Rebouças, I.; Brousset, P. Detection of HHV-8 in reactive lymphoid tissue of patients from São Paulo state, Brazil. J. Clin. Pathol. 2002, 55, 78–79. [Google Scholar] [CrossRef] [Green Version]
- Biggar, R.J.; Whitby, D.; Marshall, V.; Linhares, A.C.; Black, F. Human herpesvirus 8 in Brazilian Amerindians: A hyperendemic population with a new subtype. J. Infect. Dis. 2000, 181, 1562–1568. [Google Scholar] [CrossRef] [Green Version]
- Cassar, O.; Blondot, M.L.; Mohanna, S.; Jouvion, G.; Bravo, F.; Maco, V.; Duprez, R.; Huerre, M.; Gotuzzo, E.; Gessain, A. Human herpesvirus 8 genotype E in patients with Kaposi sarcoma, Peru. Emerg. Infect. Dis. 2010, 16, 1459–1462. [Google Scholar] [CrossRef]
- Kazanji, M.; Dussart, P.; Duprez, R.; Tortevoye, P.; Pouliquen, J.F.; Vandekerkhove, J.; Couppié, P.; Morvan, J.; Talarmin, A.; Gessain, A. Serological and molecular evidence that human herpesvirus 8 is endemic among Amerindians in French Guiana. J. Infect. Dis. 2005, 192, 1525–1529. [Google Scholar] [CrossRef] [Green Version]
- Zong, J.; Ciufo, D.M.; Viscidi, R.; Alagiozoglou, L.; Tyring, S.; Rady, P.; Orenstein, J.; Boto, W.; Kalumbuja, H.; Romano, N.; et al. Genotypic analysis at multiple loci across Kaposi’s sarcoma herpesvirus (KSHV) DNA molecules: Clustering patterns, novel variants and chimerism. J. Clin. Virol. 2002, 23, 119–148. [Google Scholar] [CrossRef]
- Duong, Y.T.; Jia, H.; Lust, J.A.; Garcia, A.D.; Tiffany, A.J.; Heneine, W.; Switzer, W.M. Short communication: Absence of evidence of HTLV-3 and HTLV-4 in patients with large granular lymphocyte (LGL) leukemia. AIDS Res. Hum. Retrovir. 2008, 24, 1503–1505. [Google Scholar] [CrossRef] [PubMed]
- Gessain, A.; Cassar, O. Epidemiological Aspects and World Distribution of HTLV-1 Infection. Front. Microbiol. 2012, 3, e00388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowis, G.W.; Sheremata, W.A.; Minagar, A. Epidemiologic features of HTLV-II: Serologic and molecular evidence. Ann. Epidemiol. 2002, 12, 46–66. [Google Scholar] [CrossRef]
- Azran, I.; Schavinsky-Khrapunsky, Y.; Priel, E.; Huleihel, M.; Aboud, M. Implications of the evolution pattern of human T-cell leukemia retroviruses on their pathogenic virulence (Review). Int. J. Mol. Med. 2004, 14, 909–915. [Google Scholar] [CrossRef] [PubMed]
- Verdonck, K.; González, E.; Van Dooren, S.; Vandamme, A.M.; Vanham, G.; Gotuzzo, E. Human T-lymphotropic virus 1: Recent knowledge about an ancient infection. Lancet Infect. Dis. 2007, 7, 266–281. [Google Scholar] [CrossRef]
- Blattner, W.A.; Kalyanaraman, V.S.; Robert-Guroff, M.; Lister, T.A.; Galton, D.A.; Sarin, P.S.; Crawford, M.H.; Catovsky, D.; Greaves, M.; Gallo, R.C. The human type-C retrovirus, HTLV, in Blacks from the Caribbean region, and relationship to adult T-cell leukemia/lymphoma. Int. J. Cancer 1982, 30, 257–264. [Google Scholar] [CrossRef]
- Schüpbach, J.; Kalyanaraman, V.S.; Sarngadharan, M.G.; Blattner, W.A.; Gallo, R.C. Antibodies against three purified proteins of the human type C retrovirus, human T-cell leukemia-lymphoma virus, in adult T-cell leukemia-lymphoma patients and healthy Blacks from the Caribbean. Cancer Res. 1983, 43, 886–891. [Google Scholar]
- Hernandez Ramirez, P.; Rivero Jimenez, R.; Ballester Santovenia, M.; Navea Leyva, L.; Matutes, E.; Catovsky, D.; Yamaguchi, K.; Fukuyoshi, Y.; Nishimura, Y.; Kiyokawa, T.; et al. Very low seroprevalence of HTLV-I/II in Cuba: Antibodies in blood donors and in hematological and nonhematological patients. Vox Sang. 1991, 61, 277–278. [Google Scholar] [CrossRef]
- Rasulee, A.; Le Riverend, E.; Shih, J.; Senjuta, N.; Pavlish, O.; Syrtsev, A.; Klepikov, N.; Lee, H.; Gurtsevitch, V. HTLV-I seroprevalence in blood donors in Cuba. Int. J. Cancer 1993, 54, 885–886. [Google Scholar] [CrossRef]
- Silva Cabrera, E.; Perez Guevara, M.T.; Lubian Caballero, A.L.; de la Fuente Arzola, J.L.; Navea Leyva, L.; Cruz Sui, O. Search for antibodies against human T-cell lymphotropic virus type I (HTLV-I) in blood donors and risk groups. Rev. Cuba. Med. Trop. 1997, 49, 24–27. [Google Scholar]
- Kaplan, J.E.; Yamamura, Y.; Rios-Olivares, E.O.; Cannon, R.O.; Khabbaz, R.F.; Gubler, D.J.; Kaiselburd, E.N.; Hartley, T.M.; Lairmore, M.D. Seroprevalence of human T lymphotropic virus type I in Puerto Rico. Am. J. Trop. Med. Hyg. 1989, 40, 659–662. [Google Scholar] [CrossRef] [PubMed]
- Koenig, R.E.; Tolentino, M.; Taveras, L.; Ferro, F.; Zornoso, C.; Ferreiras, J.; Matos, G.; Oquist, C.; Capellan, M.; Amoros, C.; et al. Prevalence of HTLV infection in the Dominican Republic: Association with neurological disease. AIDS Res. Hum. Retrovir. 1992, 8, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Diaz, H.; Frye-Maldonado, A.C.; Climent-Peris, C.; Velez-Rosario, R. Evaluation of serologic markers for transfusion transmitted infectious diseases for allogeneic blood donors in Puerto Rico. P. R. Health Sci. J. 1997, 16, 255–258. [Google Scholar] [PubMed]
- Diaz Torres, H.M.; Alvarez Vega, N.; Munio Perurena, J.E.; Lubian Caballero, A.L.; Martin Alfonso, D.; Diaz Herrera, D.F.; Blanco de Armas, M. Human T-cell lymphotropic virus type I infection in patients with lymphoproliferative disorders at two sentinel sites in Cuba. Panam. Salud Pública 2010, 27, 17–22. [Google Scholar]
- Estrada, R.A.; Luis, S.; Mustelier, R.; Ruiz, W.; Rodriguez, B.; Miranda, A.; Roman, G.C. Absence of human retroviral antibodies in epidemic neuropathy in Cuba: Report of the first two cases of HTLV-I-associated tropical spastic paraparesis observed in Cuba. J. Neurol. Sci. 1995, 128, 112–113. [Google Scholar] [CrossRef]
- Reyes-Iglesias, Y.; Melendez-Feliciano, R.; Garayalde-Cotroneo, G. Presence of human T lymphotropic virus type I in two patients with progressive myelopathy in Puerto Rico. Neurology 1991, 41, 1515–1516. [Google Scholar] [CrossRef] [PubMed]
- Vilchez, C.; Gonzalez-Reinoso, M.; Cubbison, C.; Perez-Then, E.; Roa, P.; Martinez, A.; Foerster, B.; Oviedo, J.; Stoeter, P. Atrophy, focal spinal cord lesions and alterations of diffusion tensor imaging (DTI) parameters in asymptomatic virus carriers and patients suffering from human T-lymphotrophic virus type 1 (HTLV-1)-associated myelopathy/tropical spastic paraparesis (HAM/TSP). J. Neurovirol. 2014, 20, 583–590. [Google Scholar]
- Rodriguez, E.M.; de Moya, E.A.; Guerrero, E.; Monterroso, E.R.; Quinn, T.C.; Puello, E.; de Quiñones, M.R.; Thorington, B.; Glasner, P.D.; Zacarias, F.; et al. HIV-1 and HTLV-I in sexually transmitted disease clinics in the Dominican Republic. J. Acquir. Immune Defic. Syndr. 1993, 6, 313–318. [Google Scholar]
- Rolo Gomez, F.; De Armas, M.B.; Mato Luis, J.; Lubian Caballero, A.L.; Diaz Torres, H. Confirmation of the presence in Cuba of human T-cell lymphotropic virus type I using the polymerase chain reaction. Rev. Cuba. Med. Trop. 1997, 49, 204–208. [Google Scholar]
- Trejo-Avila, L.M.; Fuentes-Pensamiento, R.; Scorro, M.F.; Diaz-Mendoza, M.L.; Zapata-Benavides, P.; Tamez-Guerra, R.S. Seroprevalence of HTLV-I/II in blood donors in Monterrey, Mexico. Arch. Med. Res. 1996, 27, 97–99. [Google Scholar] [PubMed]
- Kato-Maeda, M.; Ponce-de-León, S.; Sifuentes-Osornio, J.; Rangel-Frausto, M.S.; Calva-Mercado, J.; Infante-Surez, L.; Villareal, F.M.; Ponce-de-León, S. Bloodborne viral infections in patients attending an emergency room in Mexico City: Estimate of seroconversion probability in healthcare workers after an occupational exposure. Infect. Control. Hosp. Epidemiol. 2000, 21, 600–602. [Google Scholar] [CrossRef] [PubMed]
- Gongora-Biachi, R.A.; Gonzalez-Martinez, P.; Castro-Sansores, C.; Bastarrachea-Ortiz, J. Infection with HTLV virus type I-II in patients with cervico-uterine cancer in the Yucatan peninsula, Mexico. Ginecol. Obstet. Mex. 1997, 65, 141–144. [Google Scholar] [PubMed]
- Reeves, W.C.; Saxinger, C.; Brenes, M.M.; Quiroz, E.; Clark, J.W.; Hoh, M.W.; Blattner, W.A. Human T-cell lymphotropic virus type I (HTLV-I) seroepidemiology and risk factors in metropolitan Panama. Am. J. Epidemiol. 1988, 127, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Leon, A.; Dias, R.; Gracia, F. T-cell lymphoma/leukemia secondary to HTLV-1 in adults. Report of a case. Rev. Med. Panama 1998, 23, 41–46. [Google Scholar]
- Levine, P.H.; Reeves, W.C.; Cuevas, M.; Arosemena, J.R.; Jaffe, E.S.; Saxinger, W.C.; Altafulla, M.; De Bernal, J.; Espino, H.; Rios, B.; et al. Human T-cell leukemia virus-I and hematologic malignancies in Panama. Cancer 1989, 63, 2186–2191. [Google Scholar] [CrossRef]
- De Rivera, I.L.; Amador, L.; Mourra, S.; Li, Z.; Rasheed, S. Geographical clustering of human T-cell lymphotropic virus type 1 infection in Honduras. J. Clin. Microbiol. 1995, 33, 2999–3003. [Google Scholar] [CrossRef] [Green Version]
- Segurado, A.; Granade, T.; Parekh, B.; Nunez, C.A.; Meza, R.; Amador, L.; Terrell, S.; George, J.R.; Lal, R.B. Presence of HTLV-I and HTLV-II infection in Honduras. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1997, 16, 308. [Google Scholar] [CrossRef]
- Temple, J.J.; Brammer, M.G.; Andes, W.A.; Covington, S.; Rangan, S. Adult T-cell leukemia-lymphoma. Unusual features of two patients from a low-incidence area. Cancer 1986, 58, 694–698. [Google Scholar] [CrossRef]
- Qiu, X.; Hodges, S.; Lukaszewska, T.; Hino, S.; Arai, H.; Yamaguchi, J.; Swanson, P.; Schochetman, G.; Devare, S.G. Evaluation of a new, fully automated immunoassay for detection of HTLV-I and HTLV-II antibodies. J. Med. Virol. 2008, 80, 484–493. [Google Scholar] [CrossRef]
- Leon, G.; Quiros, A.M.; Lopez, J.L.; Hung, M.; Diaz, A.M.; Goncalves, J.; Da Costa, O.; Hernandez, T.; Chirinos, M.; Gomez, R. Seropositivity for human T-lymphotropic virus types I and II among donors at the Municipal Blood Bank of Caracas and associated risk factors. Panam. Salud Pública 2003, 13, 117–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merino, F.; Robert-Guroff, M.; Clark, J.; Biondo-Bracho, M.; Blattner, W.A.; Gallo, R.C. Natural antibodies to human T-cell leukemia/lymphoma virus in healthy Venezuelan populations. Int. J. Cancer 1984, 34, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Márquez, Y.; Pimentel, Z.; Castillo, S.; SANTIAGO, M.; URDANETA, J.; MARTÍNEZ, A.; ESCALONA, P. Frecuencia del virus linfotropico de las células t humanas tipo i/ii en pacientes que asisten a la unidad programática regional de inmunología clínica del estado Aragua, Venezuela, 2012. SABER. Rev. Multidiscip. Cons. Investig. Univ. Oriente 2016, 28, 83–89. [Google Scholar]
- Bermudez-Forero, M.I.; Berrio-Perez, M.; Herrera-Hernandez, A.M.; Rodriguez-Rodriguez, M.J.; Garcia-Blanco, S.; Orjuela-Falla, G.; Beltran, M. Prevalence of human T-cell lymphotropic virus I and II in Colombian blood donors, 2001–2014: Implications for transfusion safety. Biomedica 2016, 36, 194–200. [Google Scholar] [PubMed] [Green Version]
- Macía, C.; Vargas, S.; Mora, A.M.; Sarmiento, A.M.; Pacheco, R.; Rosso, F. Seroprevalence of human T-lymphotropic virus in blood bank donors at Fundación Valle del Lili, Cali, Colombia, 2008–2014. Biomedica 2016, 36, 108–115. [Google Scholar] [CrossRef] [Green Version]
- Trujillo, J.M.; Concha, M.; Munoz, A.; Bergonzoli, G.; Mora, C.; Borrero, I.; Gibbs, C.J., Jr.; Arango, C. Seroprevalence and cofactors of HTLV-I infection in Tumaco, Colombia. AIDS Res. Hum. Retrovir. 1992, 8, 651–657. [Google Scholar] [CrossRef]
- Martínez-Nieto, O.; Isaza-Ruget, M.; Rangel-Espinosa, N.; Morales-Reyes, O.L. Human T-lymphotropic virus (HTLV I/II) seroprevalence amongst blood-donors in a hospital Bogotá, Colombia, between 1999 and 2004. Rev. Salud Pública 2007, 9, 253–261. [Google Scholar] [CrossRef] [Green Version]
- Cardona-Arias, J.A.; Velez-Quintero, C.; Calle-Gonzalez, O.V.; Florez-Duque, J.; Zapata, J.C. Seroprevalence of human T-lymphotropic virus HTLV and its associated factors in donors of a blood bank of Medellin-Colombia, 2014–2018. PLoS ONE 2019, 14, e0221060. [Google Scholar] [CrossRef] [Green Version]
- Munoz, M.; Carvalho, S.; Donado, J.H.; Barco, G.E.; Jaramillo, S. SHTLV-I/II seroprevalence in blood donors of Hospital Pablo Tobon Uribe Blood Bank during the period 2014–2015. Biomedica 2018, 38, 37–41. [Google Scholar] [CrossRef] [Green Version]
- Maloney, E.M.; Ramirez, H.; Levin, A.; Blattner, W.A. A survey of the human T-cell lymphotropic virus type I (HTLV-I) in south-western Colombia. Int. J. Cancer 1989, 44, 419–423. [Google Scholar] [CrossRef]
- Valencia, M.; Moreno, L. Comorbidity between HTLV-1-associated adult T-cell lymphoma/leukemia and verrucous carcinoma: A case report. Colomb. Med. 2017, 48, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Blank, A.; Yamaguchi, K.; Blank, M.; Zaninovic, V.; Sonoda, S.; Takatsuki, K. Six Colombian patients with adult T-cell leukemia/lymphoma. Leuk. Lymphoma 1993, 9, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Medina, E.A.; Orduz, R.; Morales, O.L.; Martinez, O.; Baldion, M.; Isaza, M.A. Adult T-cell leukemia/lymphoma in HTLV-1 infected patients: Report of two cases in Colombia. Biomedica 2013, 33, 519–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dominguez, M.C.; Torres, M.; Tamayo, O.; Criollo, W.; Quintana, M.; Sanchez, A.; Garcia, F. Autoimmune syndrome in the tropical spastic paraparesis/myelopathy associated with human T-lymphotropic virus infections. Biomedica 2008, 28, 510–522. [Google Scholar] [PubMed]
- Mosquera-Herrera, C.E.; Aspiazu-Miranda, E.P.; de Waard, J.H.; Garcia-Bereguiain, M.A. A high prevalence of human T-lymphotropic virus (HTLV 1/2) infection among Afro-descendants, Esmeraldas province, Ecuador—Need for the implementation of surveys and control programs. Infect. Drug Resist. 2019, 12, 1969–1974. [Google Scholar] [CrossRef] [Green Version]
- Guderian, R.; Guevara, A.; Cooper, P.; Rugeles, M.T.; Arango, C. HTLV-1 infection and tropical spastic paraparesis in Esmeraldas Province of Ecuador. Trans. R. Soc. Trop. Med. Hyg. 1994, 88, 399–400. [Google Scholar] [CrossRef]
- Cevallos, R.; Barberis, L.; Evans, L.; Barriga, J.; Verdier, M.; Bonis, J.; Leonard, G.; Denis, F. HIV-1, HIV-2 and HTLV-I seroprevalence surveys in continental Ecuador and Galapagos. Aids 1990, 4, 1300–1301. [Google Scholar] [CrossRef]
- Ramirez-Soto, M.C.; Huichi-Atamari, M. Prevalence of hepatitis B and human T-lymphotropic virus infection among blood donors at a hospital in the south-central highlands of Peru. Transfus. Med. 2018, 28, 263–265. [Google Scholar] [CrossRef]
- Quispe, N.C.; Feria, E.B.; Santos-Fortuna Ede, L.; Caterino-de-Araujo, A. Confirming the presence of HTLV-1 infection and the absence of HTLV-2 in blood donors from Arequipa, Peru. Rev. Inst. Med. Trop. São Paulo 2009, 51, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Cárcamo, C.P.; Campos, P.E.; García, P.J.; Hughes, J.P.; Garnett, G.P.; Holmes, K.K. Prevalences of sexually transmitted infections in young adults and female sex workers in Peru: A national population-based survey. Lancet Infect. Dis. 2012, 12, 765–773. [Google Scholar] [CrossRef] [Green Version]
- Alarcon, J.O.; Friedman, H.B.; Montano, S.M.; Zunt, J.R.; Holmes, K.K.; Quinnan, G.V., Jr. High endemicity of human T-cell lymphotropic virus type 1 among pregnant women in peru. J. Acquir. Immune Defic. Syndr. 2006, 42, 604–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guevara Miranda, J.; Guzman Rojas, P.; Mejia Cordero, F.A. Acute liver failure as presentation of adult T-cell leukemia in an HTLV-1 patient. Rev. Gastroenterol. Peru 2018, 38, 85–88. [Google Scholar] [PubMed]
- Guevara Miranda, J.; Guzman Rojas, P.; Espinoza-Rios, J.; Mejia Cordero, F. Duodenal Linphoma asociated to Strongyloides stercoralis infection. Two types of HTLV-1 infection. Rev. Gastroenterol. Peru 2017, 37, 169–172. [Google Scholar] [PubMed]
- Rodriguez-Zuniga, M.J.; Cortez-Franco, F.; Qujiano-Gomero, E. Adult T-cell leukemia/lymphoma in a Peruvian hospital in human T-lymphotropic virus type 1 (HTLV-1) positive patients. Int. J. Dermatol. 2017, 56, 503–509. [Google Scholar] [CrossRef]
- Beltran, B.E.; Quinones, P.; Morales, D.; Revilla, J.C.; Alva, J.C.; Castillo, J.J. Diffuse large B-cell lymphoma in human T-lymphotropic virus type 1 carriers. Leuk. Res. Treat. 2012, 2012, 4. [Google Scholar] [CrossRef]
- Barros, N.; Woll, F.; Watanabe, L.; Montes, M. Are increased Foxp3+ regulatory T cells responsible for immunosuppression during HTLV-1 infection? Case reports and review of the literature. BMJ Case Rep. 2012, 2012, e006574. [Google Scholar] [CrossRef] [Green Version]
- Beltran, B.; Palomino, E.; Quinones, P.; Morales, D.; Cotrina, E. Gastric adult T cell leukemia/lymphoma: Report of four cases and review of literature. Rev. Gastroenterol. Peru 2010, 30, 153–157. [Google Scholar]
- Delgado, S.; Gotuzzo, E. Adult T cell lymphoblastic leukemia/lymphoma by HTLV-1 in a young woman. Rev. Chilena Infectol. 2019, 36, 234–237. [Google Scholar] [CrossRef]
- San Martin, H.; Balanda, M.; Vergara, N.; Valenzuela, M.A.; Cartier, L.; Ayala, S.; Ramirez, E. Human T-Lymphotropic Virus Type 1 and 2 Seroprevalence among first-time blood donors in Chile, 2011–2013. J. Med. Virol. 2016, 88, 1067–1075. [Google Scholar] [CrossRef]
- Chandia, L.; Sotomayor, C.; Ordenes, S.; Salas, P.; Navarrete, M.; Lopez, M.; Otth, C. Seroprevalence of human T-cell lymphotropic virus type 1 and 2 in blood donors from the regional hospital of Valdivia, Chile. Med. Microbiol. Immunol. 2010, 199, 341–344. [Google Scholar] [CrossRef]
- Cabrera, M.; Labra, S.; Meneses, P.; Matutes, E.; Cartier, L.; Ford, A.; Greaves, M. Adult T cell leukemia lymphoma in Chile. A clinical pathologic and molecular study of 26 patients. Rev. Med. Chile 1999, 127, 935–944. [Google Scholar] [PubMed]
- Cabrera, M.E.; Labra, S.; Ford, A.; Matutes, E. HTLV-I induced intestinal lymphoma. Leuk. Lymphoma 1999, 35, 637–640. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, M.E.; Labra, S.; Catovsky, D.; Ford, A.M.; Colman, S.M.; Greaves, M.F.; Matutes, E. HTLV-I positive adult T-cell leukaemia/lymphoma (ATLL) in Chile. Leukemia 1994, 8, 1763–1767. [Google Scholar] [PubMed]
- Casanova, E.R.; Llancapi, P.; Bravo, A.; Fuentes, B.; Contreras, G. Adult T-cell lymphoma and Reed-Sternberg cells. A clinical case. Rev. Med. Chile 1994, 122, 1184–1188. [Google Scholar]
- Cartier, L.; Castillo, J.L.; Cabrera, M.E.; Araya, F.; Matutes, E.; Ford, A.M.; Greaves, M.F. HTLV-I positive progressive spastic paraparesis (TSP) associated with a lymphoid disorder in three Chilean patients. Leuk. Lymphoma 1995, 17, 459–464. [Google Scholar] [CrossRef]
- Cabrera, M.E.; Gray, A.M.; Cartier, L.; Araya, F.; Hirsh, T.; Ford, A.M.; Greaves, M.F. Simultaneous adult T-cell leukemia/lymphoma and sub-acute polyneuropathy in a patient from Chile. Leukemia 1991, 5, 350–353. [Google Scholar]
- Montserrat, E.; Lozano, M.; Urbano-Ispizua, A.; Matutes, E.; Feliu, E.; Ercilla, G.; Vives-Corrons, J.L.; Rozman, C. Adult T-cell Leukemia in a Chilean Resident in Spain: Long-Lasting Remission after 2-Deoxycoformycin Treatment. Leuk. Lymphoma 1989, 1, 47–49. [Google Scholar] [CrossRef]
- Barrientos, A.; Lopez, M.; Sotomayor, C.; Pilleux, L.; Calderon, S.; Navarrete, M.; Otth, C. Prevalence of human T-cell lymphotropic virus type 1 and 2 among patients with malignant hematological diseases in south Chile. J. Med. Virol. 2011, 83, 745–748. [Google Scholar] [CrossRef]
- Cabrera, M.E.; Marinov, N.; Guerra, C.; Morilla, R.; Matutes, E. Chronic lymphoproliferative syndromes in Chile. A prospective study in 132 patients. Rev. Med. Chile 2003, 131, 291–298. [Google Scholar]
- Martinez, V.; Franco, C.; Sazunic, I.; Puga, M.; Bronfman, L.; Rodriguez, C. Acquired immunodeficiency syndrome associated with infection by HTLV-1 virus: A clinical case. Rev. Med. Chile 1990, 118, 671–674. [Google Scholar]
- Zoulek, G.; Schatzl, H.; Kawabata, M.; de Cabral, M.B.; Cabello, A.; Freutsmiedl, K.; Villagra, E.; von der Helm, K. A seroepidemiological survey of antibodies to HTLV-I/HTLV-II in selected population groups in Paraguay. Scand. J. Infect. Dis. 1992, 24, 397–398. [Google Scholar] [CrossRef] [PubMed]
- Balduin, B.; Priore, C.; Acosta, C.; Salazar, E.; Rodríguez, F.; Bianchi, S.; Pritsch, O. Infección por virus linfotrópico de células T humanas (HTLV) en Uruguay: Identificación de problemas. An. Fac. Med. Univ. Repúb. Urug. 2017, 4, 41–51. [Google Scholar]
- Muchinik, G.; Bouzas, M.B.; Zapiola, I.; Decaro, J.; García, L.; Gallo, D.; Hanson, C.V. HTLV-I and HTLV-II infection in Uruguay. J. Acquir. Immune Defic. Syndr. 1992, 5, 743–744. [Google Scholar] [PubMed]
- Boada, M.; Grille, S.; Brugnini, A.; Trias, N.; Canesa, C.; Diaz, L.; Lens, D. Adult T-cell leukemia/lymphoma. Report of a case in Uruguay. Medicina 2017, 77, 235–238. [Google Scholar]
- Biglione, M.; Pizarro, M.; Crespo, O.; Severich, I.; Martínez Peralta, L.; Libonatti, O.; Mercedes Avila, M.; Astarloa, L. High prevalence of HTLV-I infection in Argentinian blood donors: A new HTLV-I-endemic area? J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1999, 20, 101–102. [Google Scholar] [CrossRef]
- Del Pino, N.; Martínez Peralta, L.; Pampuro, S.; Pimentel, E.; Libonatti, O. HTLV-I/II seroprevalence and coinfection with other pathogens in blood donors in Buenos Aires. J. Acquir. Immune Defic. Syndr. 1994, 7, 206–207. [Google Scholar]
- Borda, M.A.; Svibel, G.R.; Biglione, M.M.; Berini, C.A. Detection of Human T lymphotropic virus 1 (HTLV-1) Cosmopolitan subtype Transcontinental subgroup (Aa) and HTLV-2 subtype b in blood donors of Corrientes. Rev. Argent. Microbiol. 2019, 51, 307–315. [Google Scholar]
- Moreno, C.; Balangero, M.; Barbás, M.G.; Cudolá, A.; Gallego, S. Serological diagnosis of HTLV-1/2: Combination of screening assays to define the serological status in blood donors. Rev. Argent. Microbiol. 2013, 45, 165–168. [Google Scholar]
- Biglione, M.M.; Astarloa, L.; Salomon, H.E. High prevalence of HTLV-I and HTLV-II among blood donors in Argentina: A South American health concern. AIDS Res. Hum. Retrovir. 2005, 21, 1–4. [Google Scholar] [CrossRef]
- Bouzas, M.B.; Muchinik, G.R.; Zapiola, I.; De Rosa, M.F.; Perez Bianco, R.; Pimentel, E.; Dengra, C.; Del Pino, N.; Gallo, D.; Hanson, C.V. Prevalence of HTLV-I/II among blood bank donors in Argentina. J. Acquir. Immune Defic. Syndr. 1992, 5, 1275–1276. [Google Scholar] [CrossRef]
- Gutfraind, Z.; Blejer, J.L.; Saguier, M.C.; Gomez Carretero, M.L.; Pirola, D.A.; Carreras Vescio, L.A. Seroprevalence of HTLV-I/HTLV-II in blood donors in Buenos Aires (Argentina). Vox Sang. 1994, 67, 408–409. [Google Scholar] [CrossRef] [PubMed]
- Gutfraind, Z.; Blejer, J.L.; Saguier, M.C.; Gomez Carretero, M.L.; Pirola, D.A.; Carreras Vescio, L.A. Evaluation of HTLV-I/II infection in blood donors in Buenos Aires. Medicina 1995, 55, 295–299. [Google Scholar] [PubMed]
- Blejer, J.L.; Saguier, M.C.; Salamone, H.J.; Carreras, L.A. Determination of anti-HTLV-I/II antibodies: Experience in 28,897 blood donations in Buenos Aires. Sangre 1995, 40, 447–451. [Google Scholar] [PubMed]
- Gallego, S.; Maturano, E.; Recalde, A.; Gastaldello, R.; Sileoni, S.; Bepre, H.; Medeot, S. HTLV-I/II seroprevalence and risk factors associated with infection in a blood donor population in Cordoba, Argentina. Rev. Argent. Microbiol. 2001, 33, 182–186. [Google Scholar]
- Gastaldello, R.; Fazzola, P.; Caeiro, L.; Maturano, E.; Perez De Rosas, A.; Fernandez, I.; Racca, R.; Rodriguez, M.B.; Molina, M.; Alonso, S.; et al. Absence of HTLV-I/II virus circulation in blood donors from the provinces of Santa Fe and Santiago del Estero. Rev. Argent. Microbiol. 2002, 34, 107–109. [Google Scholar]
- Remesar, M.; Mangano, A.; Sen, L.; del Pozo, A. Profile of human T-cell lymphocytotrophic virus-I/II infections in an Argentinean blood bank population. Vox Sang. 2002, 83, 364–365. [Google Scholar] [CrossRef]
- Gastaldello, R.; Hall, W.W.; Gallego, S. Seroepidemiology of HTLV-I/II in Argentina: An overview. J. Acquir. Immune Defic. Syndr. 2004, 35, 301–308. [Google Scholar] [CrossRef]
- Mangano, A.M.; Remesar, M.; del Pozo, A.; Sen, L. Human T lymphotropic virus types I and II proviral sequences in Argentinian blood donors with indeterminate Western blot patterns. J. Med. Virol. 2004, 74, 323–327. [Google Scholar] [CrossRef]
- Brun, R.O.; Astarloa, L.; Salomon, H.E.; Biglione, M.M. Prevalence of HTLV-I/II infection among blood donors in Santa Fe Province, Argentina. Medicina 2004, 64, 125–128. [Google Scholar]
- Malan, R.; Berini, C.A.; Eirin, M.E.; Delfino, C.M.; Pedrozo, W.; Krupp, R.; Garcia Plichta, A.; Biglione, M.M. Seroprevalence of HTLV-1/2 in blood donors from Misiones Province. Medicina 2010, 70, 71–74. [Google Scholar]
- Berini, C.A.; Gendler, S.A.; Pascuccio, S.; Eirin, M.E.; McFarland, W.; Page, K.; Carnevali, L.; Murphy, E.; Biglione, M.M. Decreasing trends in HTLV-1/2 but stable HIV-1 infection among replacement donors in Argentina. J. Med. Virol. 2010, 82, 873–877. [Google Scholar] [CrossRef] [PubMed]
- Trenchi, A.; Gastaldello, R.; Balangero, M.; Irizar, M.; Cudolá, A.; Gallego, S. Retrospective study of the prevalence of human T-cell lymphotropic virus-type 1/2, HIV, and HBV in pregnant women in Argentina. J. Med. Virol. 2007, 79, 1974–1978. [Google Scholar] [CrossRef] [PubMed]
- Marin, O.; Hasui, K.; Remondegui, C.; Sato, E.; Aye, M.M.; Takenouchi, N.; Izumo, S.; Tajima, K. Adult T-cell leukemia/lymphoma in Jujuy, north-west Argentina. Pathol. Int. 2002, 52, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Fourcade, C.; Jarry, L.; Mechler, C.; Lionnet, F.; Dardel, P. Association of B-cell lymphoma and T-cell lymphoma in HTLV1 infection. Ann. Biol. Clin. 1997, 55, 491–493. [Google Scholar]
- Gioseffi, O.N.; Nucifora, E.; Fantl, D.; Dufour, C.; Milone, J.; Di Paolo, H. Adult HTLV-I positive leukemia-lymphoma in Argentina. Sangre 1995, 40, 421–424. [Google Scholar]
- Prates, V.; Cobos, M.; Bouzas, B.; Napal, J.; Bordone, J.; Milone, J. The first report of familial adult T-cell leukemia/lymphoma in Argentina. Leuk. Lymphoma 2000, 37, 225–227. [Google Scholar] [CrossRef]
- Pinto, M.T.; Rodrigues, E.S.; Malta, T.M.; Azevedo, R.; Takayanagui, O.M.; Valente, V.B.; Ubiali, E.M.; Covas, D.T.; Kashima, S. HTLV-1/2 seroprevalence and coinfection rate in Brazilian first-time blood donors: An 11-year follow-up. Rev. Inst. Med. Trop. São Paulo 2012, 54, 123–129. [Google Scholar] [CrossRef]
- Catalan-Soares, B.; Carneiro-Proietti, A.B.; Proietti, F.A. Heterogeneous geographic distribution of human T-cell lymphotropic viruses I and II (HTLV-I/II): Serological screening prevalence rates in blood donors from large urban areas in Brazil. Cad. Saúde Pública 2005, 21, 926–931. [Google Scholar] [CrossRef] [Green Version]
- Dourado, I.; Alcantara, L.C.; Barreto, M.L.; da Gloria Teixeira, M.; Galvao-Castro, B. HTLV-I in the general population of Salvador, Brazil: A city with African ethnic and sociodemographic characteristics. J. Acquir. Immune Defic. Syndr. 2003, 34, 527–531. [Google Scholar] [CrossRef]
- Carneiro-Proietti, A.B.; Sabino, E.C.; Leao, S.; Salles, N.A.; Loureiro, P.; Sarr, M.; Wright, D.; Busch, M.; Proietti, F.A.; Murphy, E.L. Human T-lymphotropic virus type 1 and type 2 seroprevalence, incidence, and residual transfusion risk among blood donors in Brazil during 2007–2009. AIDS Res. Hum. Retrovir. 2012, 28, 1265–1272. [Google Scholar] [CrossRef] [Green Version]
- Reboucas, K.; Narici, F.M.; Santos Junior, M.N.; Neres, N.S.M.; Oliveira, M.V.; Souza, C.L. Seroprevalence of transfusion-transmissible infectious diseases at a hemotherapy service located in southwest Bahia, Brazil. Hematol. Transfus. Cell Ther. 2019, 41, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Pessoni, L.L.; Aquino, E.C.; Alcantara, K.C. Prevalence and trends in transfusion-transmissible infections among blood donors in Brazil from 2010 to 2016. Hematol. Transfus. Cell. Ther. 2019, 41, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Pereira, F.M.; de Almeida, M.; Santos, F.L.N.; Carreiro, R.P.; Regis-Silva, C.G.; Galvao-Castro, B.; Grassi, M.F.R. Evidence of New Endemic Clusters of Human T-Cell Leukemia Virus (HTLV) Infection in Bahia, Brazil. Front. Microbiol. 2019, 10, 1002. [Google Scholar] [CrossRef] [PubMed]
- Silva, I.C.; Pinheiro, B.T.; Nobre, A.F.S.; Coelho, J.L.; Pereira, C.C.C.; Ferreira, L.S.C.; Almeida, C.P.S.; Viana, M.; Almeida, D.S.; Falcao, J.R.; et al. Moderate endemicity of the human T-lymphotropic virus infection in the metropolitan region of Belem, Para, Brazil. Rev. Bras. Epidemiol. 2018, 21, e180018. [Google Scholar]
- Ribeiro, I.P.; Kozlowski, A.G.; Dias de Matos, M.A.; da Costa E Silva, Á.M.; dos Santos Carneiro, M.A.; Vicente, A.C.P.; Martins, R.M.B. HTLV-1 and-2 in a first-time blood donor population in Northeastern Brazil: Prevalence, molecular characterization, and evidence of intrafamilial transmission. J. Med. Virol. 2018, 90, 1651–1657. [Google Scholar] [CrossRef]
- Morais, M.P.E.; Gato, C.M.; Maciel, L.A.; Lalwani, P.; Costa, C.A.; Lalwani, J.D.B. Prevalence of Human T-lymphotropic virus type 1 and 2 among blood donors in Manaus, Amazonas State, Brazil. Rev. Inst. Med. Trop. São Paulo 2017, 59, 7. [Google Scholar] [CrossRef] [Green Version]
- De Aguiar, S.A.; de Souza França, S.A.; Santana, B.B.; Santos, M.B.; Freitas, F.B.; Ferreira, G.; Cayres-Vallinoto, I.; Ishak, M.O.G.; Ishak, R.; Vallinoto, A.C.R. Human T-lymphotropic virus 1aA circulation and risk factors for sexually transmitted infections in an Amazon geographic area with lowest human development index (Marajo Island, Northern Brazil). BMC Infect. Dis. 2017, 17, 758. [Google Scholar] [CrossRef] [Green Version]
- Nunes, D.; Boa-Sorte, N.; Grassi, M.F.; Taylor, G.P.; Teixeira, M.G.; Barreto, M.L.; Dourado, I.; Galvão-Castro, B. HTLV-1 is predominantly sexually transmitted in Salvador, the city with the highest HTLV-1 prevalence in Brazil. PLoS ONE 2017, 12, e0171303. [Google Scholar] [CrossRef]
- Gomes, F.V.; Eleutério Junior, J. HTLV-II in blood donors at the Blood Center Net of Ceara—HEMOCE. Rev. Assoc. Méd. Bras. (1992) 2011, 57, 309–312. [Google Scholar] [CrossRef]
- Dias-Bastos, M.R.; Oliveira, C.D.L.; Carneiro-Proietti, A.B.D.F. Decline in prevalence and asymmetric distribution of human T cell lymphotropic virus 1 and 2 in blood donors, State of Minas Gerais, Brazil, 1993 to 2007. Rev. Soc. Bras. Med. Trop. 2010, 43, 615–619. [Google Scholar] [CrossRef] [Green Version]
- Lima, G.M.; Eustaquio, J.M.; Martins, R.A.; Josahkian, J.A.; Pereira Gde, A.; Moraes-Souza, H.; Martins, P.R. Decline in the prevalence of HTLV-1/2 among blood donors at the Regional Blood Center of the City of Uberaba, State of Minas Gerais, from 1995 to 2008. Rev. Soc. Bras. Med. Trop. 2010, 43, 421–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namen-Lopes, M.S.; Martins, M.L.; Drummond, P.C.; Lobato, R.R.; Carneiro-Proietti, A.B. Lookback study of HTLV-1 and 2 seropositive donors and their recipients in Belo Horizonte, Brazil. Transfus. Med. 2009, 19, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Pinto, M.T.; Slavov, S.N.; Valente, V.B.; Ubiali, E.M.; Covas, D.T.; Kashima, S. Evaluation of human T-lymphotropic virus prevalence/co-infection rates for a four-year period in a non-metropolitan blood center in Southeast Brazil. Rev. Soc. Bras. Med. Trop. 2016, 49, 232–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viana, G.M.; Nascimento Mdo, D.; de Oliveira, R.A.; Dos Santos, A.C.; Galvao Cde, S.; da Silva, M.A. Seroprevalence of HTLV-1/2 among blood donors in the state of Maranhao, Brazil. Revi. Bras. Hematol. Hemoter. 2014, 36, 50–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colin, D.D.; Alcantara Junior, L.C.; Santos, F.L.; Uchoa, R.; Tavares-Neto, J. Seroprevalence of human T cell lymphotropic virus infection and associated factors of risk in blood donors of Rio Branco city, AC, Brazil (1998–2001). Rev. Soc. Bras. Med. Trop. 2003, 36, 677–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segurado, A.A.; Malaque, C.M.; Sumita, L.M.; Pannuti, C.S.; Lal, R.B. Laboratory characterization of human T cell lymphotropic virus types 1 (HTLV-1) and 2 (HTLV-2) infections in blood donors from Sao Paulo, Brazil. Am. J. Trop. Med. Hyg. 1997, 57, 142–148. [Google Scholar] [CrossRef]
- Ferreira Junior, O.C.; Vaz, R.S.; Carvalho, M.B.; Guerra, C.; Fabron, A.L.; Rosemblit, J.; Hamerschlak, N. Human T-lymphotropic virus type I and type II infections and correlation with risk factors in blood donors from Sao Paulo, Brazil. Transfusion 1995, 35, 258–263. [Google Scholar] [CrossRef]
- Oliveira, P.D.; Gomes, I.; Souza, V.H.; Pires, E.C.; Arruda, G.B.; Bittencourt, A. Adult T-cell leukemia/lymphoma treatment in Bahia, Brazil. Revi. Bras. Hematol. Hemoter. 2017, 39, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Bittencourt, A.L.; Barbosa, H.S.; Vieira, M.D.; Farre, L. Adult T-cell leukemia/lymphoma (ATL) presenting in the skin: Clinical, histological and immunohistochemical features of 52 cases. Acta Oncol. 2009, 48, 598–604. [Google Scholar] [CrossRef]
- Farre, L.; de Oliveira Mde, F.; Primo, J.; Vandamme, A.M.; Van Weyenbergh, J.; Bittencourt, A.L. Early sequential development of infective dermatitis, human T cell lymphotropic virus type 1-associated myelopathy, and adult T cell leukemia/lymphoma. Clin. Infect. Dis. 2008, 46, 440–442. [Google Scholar] [CrossRef]
- Bittencourt, A.L.; da Gracas Vieira, M.; Brites, C.R.; Farre, L.; Barbosa, H.S. Adult T-cell leukemia/lymphoma in Bahia, Brazil: Analysis of prognostic factors in a group of 70 patients. Am. J. Clin. Pathol. 2007, 128, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, F.H.; Colleoni, G.W.; Teixeira, S.P.; Yamamoto, M.; Michalany, N.S.; Almeida, F.A.; Chiba, A.K.; Petri, V.; Fernandes, M.A.; Pombo-de-Oliveira, M.S. Cutaneous T-cell lymphoma with HTLV-I infection: Clinical overlap with adult T-cell leukemia/lymphoma. Int. J. Dermatol. 2006, 45, 447–449. [Google Scholar] [CrossRef] [PubMed]
- Pombo-de-Oliveira, M.S.; Dobbin, J.A.; Loureiro, P.; Borducchi, D.; Maia, R.C.; Fernandes, M.A.; Cavalcanti, G.B., Jr.; Takemoto, S.; Franchini, G. Genetic mutation and early onset of T-cell leukemia in pediatric patients infected at birth with HTLV-I. Leuk. Res. 2002, 26, 155–161. [Google Scholar] [CrossRef]
- Pombo de Oliveira, M.S.; Matutes, E.; Schulz, T.; Carvalho, S.M.; Noronha, H.; Reaves, J.D.; Loureiro, P.; Machado, C.; Catovsky, D. T-cell malignancies in Brazil. Clinico-pathological and molecular studies of HTLV-I-positive and -negative cases. Int. J. Cancer 1995, 60, 823–827. [Google Scholar] [CrossRef]
- De Oliveira, M.S.; Matutes, E.; Famadas, L.C.; Schulz, T.F.; Calabro, M.L.; Nucci, M.; Andrada-Serpa, M.J.; Tedder, R.S.; Weiss, R.A.; Catovsky, D. Adult T-cell leukaemia/lymphoma in Brazil and its relation to HTLV-I. Lancet 1990, 336, 987–990. [Google Scholar] [CrossRef]
- Bittencourt, A.L.; Andrade, A.C.; Requião, C.; Arruda, M.D.; Araújo, I. Prolonged lymphocytosis as the first manifestation of Hodgkin-like adult T-cell leukemia/lymphoma. Braz. J. Infect. Dis. 2017, 21, 119–122. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos, V.M.; Ribeiro, E.F.; de Faria, P.S.; Barros, I.A.; Oliveira, M.M. A 61-year-old woman with adult T-cell leukemia/lymphoma. Rom. J. Morphol. Embryol. 2016, 57, 563–566. [Google Scholar]
- Oliveira, P.D.; Salvino, M.A.; Santos, H.H.; Bittencourt, A.L. An Unusual Association of Adult T-Cell Leukemia/Lymphoma With Hyalohyphomycosis. Am. J. Dermatopathol. 2016, 38, 370–373. [Google Scholar] [CrossRef]
- Viana, G.M.; da Silva, M.A.; Souza, V.L.; Lopes, N.B.; Nascimento Mdo, D. Endemic transmission of HTLV-2 in blood donors from São Luís do Maranhão, northeastern Brazil: Report of two asymptomatic individuals. Revi. Bras. Hematol. Hemoter. 2015, 37, 130–131. [Google Scholar] [CrossRef] [Green Version]
- Salles, F.; Bacellar, A.; Amorim, M.; Orge, G.; Sundberg, M.; Lima, M.; Santos, S.; Porto, A.; Carvalho, E. Treatment of strongyloidiasis in HTLV-1 and Strongyloides stercoralis coinfected patients is associated with increased TNFalpha and decreased soluble IL2 receptor levels. Trans. R. Soc. Trop. Med. Hyg. 2013, 107, 526–529. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, P.D.; Magalhaes, M.; Argolo, J.M.; Bittencourt, A.L.; Farre, L. Double integration band of HTLV-1 in a young patient with infective dermatitis who developed an acute form of adult T-cell leukemia/lymphoma. J. Clin. Virol. 2013, 56, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Lyra-da-Silva, J.O.; de Mello Gonzaga, Y.B.; de Melo Espíndola, O.; de Andrada-Serpa, M.J.; Dib, C.; Jeunon, T. Adult T-cell leukemia/lymphoma: A case report of primary cutaneous tumoral type. Dermatol. Pract. Concept. 2012, 2, 0202a03. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olivo, R.A.; Martins, F.F.M.; Soares, S.; Moraes-Souza, H. Adult T-cell leukemia/lymphoma: Report of two cases. Rev. Soc. Bras. Med. Trop. 2008, 41, 288–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albuquerque, M.A.; Migliari, D.A.; Sugaya, N.N.; Kuroishi, M.; Capuano, A.C.; Sousa, S.O.; Cavalcanti, M.G. Adult T-cell leukemia/lymphoma with predominant bone involvement, initially diagnosed by its oral manifestation: A case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Pombo De Oliveira, M.S.; Loureiro, P.; Bittencourt, A.; Chiattone, C.; Borducchi, D.; De Carvalho, S.M.; Barbosa, H.S.; Rios, M.; Sill, A.; Cleghorn, F.; et al. Geographic diversity of adult t-cell leukemia/lymphoma in Brazil. The Brazilian ATLL Study Group. Int. J. Cancer 1999, 83, 291–298. [Google Scholar] [CrossRef]
- Barbosa, H.S.; Bittencourt, A.L.; Barreto de Araújo, I.; Pereira Filho, C.S.; Furlan, R.; Pedrosa, C.; Lessa, G.; Harrington, W., Jr.; Galvão Castro, B. Adult T-cell leukemia/lymphoma in northeastern Brazil: A clinical, histopathologic, and molecular study. J. Acquir. Immune Defic. Syndr. 1999, 21, 65–71. [Google Scholar] [CrossRef]
- Gongora-Biachi, R.A.; Gonzalez-Martinez, P.; Castro-Sansores, C.; Vivas-Rosel, M.L.; Gasque-Lopez, F.; Garrido-Hadad, E. Lymphotropic viruses type I and II in pregnant women in Yucatan. Rev. Investig. Clin. 1996, 48, 383–384. [Google Scholar]
- Gongora-Biachi, R.A.; Gonzalez-Martinez, P.; Puerto, F.I.; Sosa-Munoz, J.; Duarte-Zapata, L.; Bastarrachea-Ortiz, J.; Yamaguchi, K.; Nishimura, Y.; Takatsuki, K. A low prevalence of HTLV-I/-II infection among eight population groups from Merida Yucatan, Mexico. J. Acquir. Immune Defic. Syndr. 1992, 5, 104–106. [Google Scholar]
- Castro-Sansores, C.J.; Santos-Rivero, A.; Gonzalez-Martinez, P.; Lara-Perera, D.M.; Alonso-Salomon, G.; Gongora-Biachi, R.A. Co-infection by the human T-cell lymphotropic virus type II in patients infected by the human immunodeficiency virus in Yucatan, Mexico. Arch. Med. Res. 2006, 37, 365–369. [Google Scholar] [CrossRef]
- Gongora-Biachi, R.A.; Lal, D.L.; Rudolph, R.B.; Castro-Sansores, C.; Gonzalez-Martinez, P.; Pavia-Ruz, N. Low prevalence of HTLV-II in Mayan Indians in the Yucatan Peninsula, Mexico. Arch. Med. Res. 1997, 28, 555–558. [Google Scholar]
- Guerena-Burgueno, F.; Benenson, A.S.; Sepulveda-Amor, J.; Ascher, M.S.; Vugia, D.J.; Gallo, D. Prevalence of human T cell lymphotropic virus types 1 and 2 (HTLV-1/2) in selected Tijuana subpopulations. Am. J. Trop. Med. Hyg. 1992, 47, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Zapata-Benavides, P.; Lara-Rodriguez, M.A.; Alcocer-Gonzalez, J.M.; Rodriguez-Padilla, C.; Tamez-Guerra, R.; Trejo-Avila, L.M. Seroprevalence of HTLV-I/II in different groups at risk in northeast Mexico. Vox Sang. 1996, 70, 181–182. [Google Scholar] [CrossRef] [PubMed]
- Khabbaz, R.F.; Hartley, T.M.; Oberle, M.W.; Rosero-Bixby, L. Seroprevalence of human T-lymphotropic virus type I (HTLV-I) in Costa Rica. AIDS Res. Hum. Retrovir. 1990, 6, 959–960. [Google Scholar] [CrossRef] [PubMed]
- Vallejo, A.; Dubon, J.M.; Garcia-Saiz, A. Presence of human T-cell lymphotropic virus types I and II infections in Honduras. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1996, 12, 529–530. [Google Scholar] [CrossRef] [PubMed]
- Castillo, L.C.; Gracia, F.; Roman, G.C.; Levine, P.; Reeves, W.C.; Kaplan, J. Spinocerebellar syndrome in patients infected with human T-lymphotropic virus types I and II (HTLV-I/HTLV-II): Report of 3 cases from Panama. Acta Neurol. Scand. 2000, 101, 405–412. [Google Scholar] [CrossRef]
- Gracia, F.; Castillo, L.; de Lao, S.L.; Archibold, C.A.; Larreategui, M.; Reeves, W.C.; Levine, P. Neurologic diseases associated with the HTLV-1 virus in Panama. Rev. Med. Panama 1990, 15, 197–203. [Google Scholar]
- Gracia, F.; Castillo, L.C.; Larreategui, M.; Roberts, B.; Cedeno, V.; Heneine, W.; Blattner, W.; Kaplan, J.E.; Levine, P.H. Relation between human T-lymphotropic virus type I and neurologic diseases in Panama: 1985–1990. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1995, 10, 192–197. [Google Scholar] [CrossRef]
- Gracia, F.; Reeves, W.C.; Levine, P.H.; Cuevas, M.; Castillo, L.; Chavarria, R.; Grimaldo, V.; Triana, E.; Arosemena, J.R.; Blattner, W.A. Human T-cell lymphotropic virus type I and neurologic disease in Panama, 1985 and 1986. Arch. Neurol. 1990, 47, 634–639. [Google Scholar] [CrossRef]
- Ohtsu, T.; Tsugane, S.; Tobinai, K.; Shimoyama, M.; Nanri, S.; Watanabe, S. Prevalence of antibodies to human T-cell leukemia/lymphoma virus type I and human immunodeficiency virus in Japanese immigrant colonies in Bolivia and Bolivian natives. Jpn. J. Cancer Res. 1987, 78, 1347–1353. [Google Scholar]
- Ferrer, J.F.; Esteban, E.; Murua, A.; Gutierrez, S.; Dube, S.; Poiesz, B.; Feldman, L.; Basombrio, M.A.; Galligan, D. Association and epidemiologic features of Trypanosoma cruzi and human T cell lymphotropic a virus type II in inhabitants of the Paraguayan Gran Chaco. Am. J. Trop. Med. Hyg. 2003, 68, 235–241. [Google Scholar] [CrossRef]
- Brites, C.; Harrington, W., Jr.; Pedroso, C.; Martins Netto, E.; Badaro, R. Epidemiological Characteristics of HTLV-I and II Co-Infection in Brazilian Subjects Infected by HIV-1. Braz. J. Infect. Dis. 1997, 1, 42–47. [Google Scholar] [PubMed]
- Britto, A.P.; Galvao-Castro, B.; Straatmann, A.; Santos-Torres, S.; Tavares-Neto, J. HTLV-I/II infection in the state of Bahia. Rev. Soc. Bras. Med. Trop. 1998, 31, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dal Fabbro, M.M.; Cunha, R.V.; Boia, M.N.; Portela, P.; Botelho, C.A.; Freitas, G.M.; Soares, J.; Ferri, J.; Lupion, J. HTLV 1/2 infection: Prenatal performance as a disease control strategy in State of Mato Grosso do Sul. Rev. Soc. Bras. Med. Trop. 2008, 41, 148–151. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, E.H.; Oliveira-Filho, A.B.; Souza, L.A.; da Silva, L.V.; Ishak, M.O.; Ishak, R.; Vallinoto, A.C. Human T-cell lymphotropic virus in patients infected with HIV-1: Molecular epidemiology and risk factors for transmission in Piaui, Northeastern Brazil. Curr. HIV Res. 2012, 10, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Guimaraes de Souza, V.; Lobato Martins, M.; Carneiro-Proietti, A.B.; Januario, J.N.; Ladeira, R.V.; Silva, C.M.; Pires, C.; Gomes, S.C.; Martins Cde, S.; Mochel, E.G. High prevalence of HTLV-1 and 2 viruses in pregnant women in Sao Luis, state of Maranhao, Brazil. Rev. Soc. Bras. Med. Trop. 2012, 45, 159–162. [Google Scholar] [CrossRef] [Green Version]
- Linhares, M.I.; Eizuru, Y.; de Andrade, G.P.; Fonseca, I.B.; Carvalho Junior, L.B.; Moreira, I.T.; Minamishima, Y. Human T cell leukemia virus type 1 (HTLV-1) antibodies in healthy populations and renal transplanted patients in the north-east of Brazil. Microbiol. Immunol. 1994, 38, 475–478. [Google Scholar] [CrossRef] [Green Version]
- Moreira, E.D.; Ribeiro, T.T., Jr.; Swanson, P.; Sampaio Filho, C.; Melo, A.; Brites, C.; Badaro, R.; Toedter, G.; Lee, H.; Harrington, W., Jr. Seroepidemiology of human T-cell lymphotropic virus type I/II in northeastern Brazil. J. Acquir. Immune Defic. Syndr. 1993, 6, 959–963. [Google Scholar]
- Rego, F.F.; Alcantara, L.C.; Moura Neto, J.P.; Miranda, A.C.; Pereira Ode, S.; Goncalves Mde, S.; Galvao-Castro, B. HTLV type 1 molecular study in Brazilian villages with African characteristics giving support to the post-Columbian introduction hypothesis. AIDS Res. Hum. Retrovir. 2008, 24, 673–677. [Google Scholar] [CrossRef]
- Sequeira, C.G.; Tamegao-Lopes, B.P.; Santos, E.J.; Ventura, A.M.; Moraes-Pinto, M.I.; Succi, R.C. Descriptive study of HTLV infection in a population of pregnant women from the state of Para, Northern Brazil. Rev. Soc. Bras. Med. Trop. 2012, 45, 453–456. [Google Scholar] [CrossRef] [Green Version]
- Vallinoto, A.C.; Azevedo, V.N.; Santos, D.E.; Caniceiro, S.; Mesquita, F.C.; Hall, W.W.; Ishak, M.O.; Ishak, R. Serological evidence of HTLV-I and HTLV-II coinfections in HIV-1 positive patients in Belem, state of Para, Brazil. Mem. Inst. Oswaldo Cruz 1998, 93, 407–409. [Google Scholar] [CrossRef] [Green Version]
- Vallinoto, A.C.; Pontes, G.S.; Muto, N.A.; Lopes, I.G.; Machado, L.F.; Azevedo, V.N.; Carvalhaes, F.A.; Santos, S.E.; Guerreiro, J.F.; Ishak, M.O.; et al. Identification of human T-cell lymphotropic virus infection in a semi-isolated Afro-Brazilian quilombo located in the Marajo Island (Para, Brazil). Mem. Inst. Oswaldo Cruz 2006, 101, 103–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caterino-de-Araujo, A.; Sacchi, C.T.; Goncalves, M.G.; Campos, K.R.; Magri, M.C.; Alencar, W.K. Short Communication: Current Prevalence and Risk Factors Associated with Human T Lymphotropic Virus Type 1 and Human T Lymphotropic Virus Type 2 Infections Among HIV/AIDS Patients in Sao Paulo, Brazil. AIDS Res. Hum. Retrovir. 2015, 31, 543–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farias de Carvalho, S.M.; Pombo de Oliveira, M.S.; Thuler, L.C.; Rios, M.; Coelho, R.C.; Rubim, L.C.; Silva, E.M.; Reis, A.M.; Catovsky, D. HTLV-I and HTLV-II infections in hematologic disorder patients, cancer patients, and healthy individuals from Rio de Janeiro, Brazil. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1997, 15, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, D.L.; Taquette, S.R.; Sodre Barmpas, D.B.; Rodrigues, N.C.; Teixeira, S.A.; Villela, L.H.; Boia, M.N.; Trajano, A.J. Prevalence of HTLV-1/2 in pregnant women living in the metropolitan area of Rio de Janeiro. PLoS Negl. Trop. Dis. 2014, 8, e3146. [Google Scholar] [CrossRef] [PubMed]
- Soares, C.C.; Georg, I.; Lampe, E.; Lewis, L.; Morgado, M.G.; Nicol, A.F.; Pinho, A.A.; Salles, R.C.; Teixeira, S.L.; Vicente, A.C.; et al. HIV-1, HBV, HCV, HTLV, HPV-16/18, and Treponema pallidum infections in a sample of Brazilian men who have sex with men. PLoS ONE 2014, 9, e102676. [Google Scholar] [CrossRef]
- Castro, L.S.; Rezende, G.R.; Fernandes, F.R.P.; Bandeira, L.M.; Puga, M.A.M.; Tanaka, T.S.O.; Weis-Torres, S.; Vicente, A.C.P.; Otsuki, K.; Motta-Castro, A.R.C. Human T cell lymphotropic virus type 1 infection among men who have sex with men in Central Brazil. Braz. J. Infect. Dis. 2018, 22, 472–476. [Google Scholar] [CrossRef]
- Catalan-Soares, B.C.; Almeida, R.T.; Carneiro-Proietti, A.B. Prevalence of HIV-1/2, HTLV-I/II, hepatitis B virus (HBV), hepatitis C virus (HCV), Treponema pallidum and Trypanosoma cruzi among prison inmates at Manhuacu, Minas Gerais State, Brazil. Rev. Soc. Bras. Med. Trop. 2000, 33, 27–30. [Google Scholar] [CrossRef] [Green Version]
- Kozlowski, A.G.; Matos, M.A.; Carneiro, M.A.; Lopes, C.L.; Teles, S.A.; Vicente, C.P.; Martins, R.M. Seroprevalence of Htlv in a Population of Hiv1-Infected Patients in Midwestern Brazil. Rev. Inst. Med. Trop. São Paulo 2016, 58, 80. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, M.A.; Proietti, F.A.; Martins, M.L.; Januario, J.N.; Ladeira, R.V.; Oliveira Mde, F.; Carneiro-Proietti, A.B. Geographic distribution of human T-lymphotropic virus types 1 and 2 among mothers of newborns tested during neonatal screening, Minas Gerais, Brazil. Panam. Salud Pública 2010, 27, 330–337. [Google Scholar] [CrossRef]
- Barros Kanzaki, L.I.; Casseb, J. Unusual finding of HTLV-I infection among Amazonian Amerindians. Arch. Med. Res. 2007, 38, 897–900. [Google Scholar] [CrossRef]
- Gabbai, A.A.; Bordin, J.O.; Vieira-Filho, J.P.; Kuroda, A.; Oliveira, A.S.; Cruz, M.V.; Ribeiro, A.A.; Delaney, S.R.; Henrard, D.R.; Rosario, J.; et al. Selectivity of human T lymphotropic virus type-1 (HTLV-1) and HTLV-2 infection among different populations in Brazil. Am. J. Trop. Med. Hyg. 1993, 49, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Laurentino, R.V.; Lopes, I.G.; Azevedo, V.N.; Machado, L.F.; Moreira, M.R.; Lobato, L.; Ishak, M.O.; Ishak, R.; Vallinoto, A.C. Molecular characterization of human T-cell lymphotropic virus coinfecting human immunodeficiency virus 1 infected patients in the Amazon region of Brazil. Mem. Inst. Oswaldo Cruz 2005, 100, 371–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mota-Miranda, A.C.; Araujo, S.P.; Dias, J.P.; Colin, D.D.; Kashima, S.; Covas, D.T.; Tavares-Neto, J.; Galvao-Castro, B.; Alcantara, L.C. HTLV-1 infection in blood donors from the Western Brazilian Amazon region: Seroprevalence and molecular study of viral isolates. J. Med. Virol. 2008, 80, 1966–1971. [Google Scholar] [CrossRef] [PubMed]
- Braco, I.L.J.; de Sa, K.S.G.; Waqasi, M.; Queiroz, M.A.F.; da Silva, A.N.R.; Cayres-Vallinoto, I.M.V.; Lima, S.S.; de Oliveira Guimaraes Ishak, M.; Ishak, R.; Guerreiro, J.F.; et al. High prevalence of human T-lymphotropic virus 2 (HTLV-2) infection in villages of the Xikrin tribe (Kayapo), Brazilian Amazon region. BMC Infect. Dis. 2019, 19, 459. [Google Scholar] [CrossRef] [Green Version]
- Ishak, R.; Harrington, W.J., Jr.; Azevedo, V.N.; Eiraku, N.; Ishak, M.O.; Guerreiro, J.F.; Santos, S.B.; Kubo, T.; Monken, C.; Alexander, S.; et al. Identification of human T cell lymphotropic virus type IIa infection in the Kayapo, an indigenous population of Brazil. AIDS Res. Hum. Retrovir. 1995, 11, 813–821. [Google Scholar] [CrossRef]
- Ishak, R.; Vallinoto, A.C.; Azevedo, V.N.; Lewis, M.; Hall, W.W.; Guimaraes Ishak, M.O. Molecular evidence of mother-to-child transmission of HTLV-IIc in the Kararao Village (Kayapo) in the Amazon region of Brazil. Rev. Soc. Bras. Med. Trop. 2001, 34, 519–525. [Google Scholar] [CrossRef]
- Nakauchi, C.M.; Linhares, A.C.; Maruyama, K.; Kanzaki, L.I.; Macedo, J.E.; Azevedo, V.N.; Casseb, J.S. Prevalence of human T cell leukemia virus-I (HTLV-I) antibody among populations living in the Amazon region of Brazil (preliminary report). Mem. Inst. Oswaldo Cruz 1990, 85, 29–33. [Google Scholar] [CrossRef] [Green Version]
- Nakauchi, C.M.; Maruyama, K.; Kanzaki, L.I.; Linhares, A.C.; Azevedo, V.N.; Fukushima, T.; Miyauchi, M.; Koshikawa, N.; Tamayama, C.; Mochizuki, S.; et al. Prevalence of HTLV-I antibody among two distinct ethnic groups inhabiting the Amazon region of Brazil. Rev. Inst. Med. Trop. São Paulo 1992, 34, 323–328. [Google Scholar] [CrossRef]
- Bouzas, M.B.; Muchinik, G.; Zapiola, I.; De Rosa, M.F.; Perez Bianco, R.; Cahn, P.; Gallo, D.; Hanson, C. Human T cell lymphotropic virus type II infection in Argentina. J. Infect. Dis. 1991, 164, 1026–1027. [Google Scholar] [CrossRef]
- Berini, C.A.; Delfino, C.; Torres, O.; Garcia, G.; Espejo, R.; Pianciola, L.; Juarez, M.; Arribere, G.; Nadal, M.; Eirin, M.E.; et al. HTLV-1 cosmopolitan and HTLV-2 subtype b among pregnant women of non-endemic areas of Argentina. Sex. Transm. Infect. 2013, 89, 333–335. [Google Scholar] [CrossRef]
- Dipierri, J.E.; Tajima, K.; Cartier Robirosa, L.; Sonoda, S. A seroepidemiological survey of HTLV-I/II carriers in the Puna Jujeña. Medicina 1999, 59, 717–720. [Google Scholar] [PubMed]
- Frutos, M.C.; Gastaldello, R.; Balangero, M.; Remondegui, C.; Blanco, S.; Otsuki, K.; Paulo Vicente, A.C.; Elias, D.; Mangeaud, A.; Nates, S.; et al. Silent dissemination of HTLV-1 in an endemic area of Argentina. Epidemiological and molecular evidence of intrafamilial transmission. PLoS ONE 2017, 12, e0174920. [Google Scholar] [CrossRef] [PubMed]
- Tsugane, S.; Watanabe, S.; Sugimura, H.; Otsu, T.; Tobinai, K.; Shimoyama, M.; Nanri, S.; Ishii, H. Infectious states of human T lymphotropic virus type I and hepatitis B virus among Japanese immigrants in the Republic of Bolivia. Am. J. Epidemiol. 1988, 128, 1153–1161. [Google Scholar] [CrossRef] [PubMed]
- Bandeira, L.M.; Uehara, S.N.; Asato, M.A.; Aguena, G.S.; Maedo, C.M.; Benites, N.H.; Puga, M.A.; Rezende, G.R.; Finotti, C.M.; Cesar, G.A.; et al. High prevalence of HTLV-1 infection among Japanese immigrants in non-endemic area of Brazil. PLoS Negl. Trop. Dis. 2015, 9, e0003691. [Google Scholar] [CrossRef]
- Vallinoto, A.C.; Muto, N.A.; Pontes, G.S.; Machado, L.F.; Azevedo, V.N.; dos Santos, S.E.; Ribeiro-dos-Santos, A.K.; Ishak, M.O.; Ishak, R. Serological and molecular evidence of HTLV-I infection among Japanese immigrants living in the Amazon region of Brazil. Jpn. J. Infect. Dis. 2004, 57, 156–159. [Google Scholar]
- Bandeira, L.M.; Uehara, S.N.O.; Puga, M.A.M.; Rezende, G.R.; Vicente, A.C.P.; Domingos, J.A.; do Lago, B.V.; Niel, C.; Motta-Castro, A.R.C. HTLV-1 intrafamilial transmission among Japanese immigrants in Brazil. J. Med. Virol. 2018, 90, 351–357. [Google Scholar] [CrossRef]
- Barcellos, N.T.; Fuchs, S.C.; Mondini, L.G.; Murphy, E.L. Human T lymphotropic virus type I/II infection: Prevalence and risk factors in individuals testing for HIV in counseling centers from Southern Brazil. Sex. Transm. Dis. 2006, 33, 302–306. [Google Scholar] [CrossRef]
- Bellei, N.C.; Granato, C.F.; Tomyiama, H.; Castelo, A.; Ferreira, O. HTLV infection in a group of prostitutes and their male sexual clients in Brazil: Seroprevalence and risk factors. Trans. R. Soc. Trop. Med. Hyg. 1996, 90, 122–125. [Google Scholar] [CrossRef]
- Borducchi, D.M.; Oliveira, J.S.; Bordin, J.O.; Kerbauy, J. HTLV-I infection among relatives of patients with adult T-cell leukemia/lymphoma in Brazil: Analysis of infection transmission. Leuk. Lymphoma 1998, 31, 411–416. [Google Scholar] [CrossRef]
- Broutet, N.; de Queiroz Sousa, A.; Basilio, F.P.; Sá, H.L.; Simon, F.; Dabis, F. Prevalence of HIV-1, HIV-2 and HTLV antibody, in Fortaleza, Ceara, Brazil, 1993–1994. Int. J. STD AIDS 1996, 7, 365–369. [Google Scholar] [CrossRef]
- Cortes, E.; Detels, R.; Aboulafia, D.; Li, X.L.; Moudgil, T.; Alam, M.; Bonecker, C.; Gonzaga, A.; Oyafuso, L.; Tondo, M. HIV-1, HIV-2, and HTLV-I infection in high-risk groups in Brazil. N. Engl. J. Med. 1989, 320, 953–958. [Google Scholar] [CrossRef] [PubMed]
- De Almeida Rego, F.F.; Mota-Miranda, A.; de Souza Santos, E.; Galvão-Castro, B.; Alcantara, L.C. Seroprevalence and molecular epidemiology of HTLV-1 isolates from HIV-1 co-infected women in Feira de Santana, Bahia, Brazil. AIDS Res. Hum. Retrovir. 2010, 26, 1333–1339. [Google Scholar] [CrossRef] [PubMed]
- De Araujo, A.C.; Casseb, J.S.; Neitzert, E.; de Souza, M.L.; Mammano, F.; Del Mistro, A.; De Rossi, A.; Chieco-Bianchi, L. HTLV-I and HTLV-II infections among HIV-1 seropositive patients in Sao Paulo, Brazil. Eur. J. Epidemiol. 1994, 10, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Dourado, I.; Andrade, T.; Carpenter, C.L.; Galvão-Castro, B. Risk factors for human T cell lymphotropic virus type I among injecting drug users in northeast Brazil: Possibly greater efficiency of male to female transmission. Mem. Inst. Oswaldo Cruz 1999, 94, 13–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etzel, A.; Shibata, G.Y.; Rozman, M.; Jorge, M.L.; Damas, C.D.; Segurado, A.A. HTLV-1 and HTLV-2 infections in HIV-infected individuals from Santos, Brazil: Seroprevalence and risk factors. J. Acquir. Immune Defic. Syndr. 2001, 26, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Galetto, L.R.; Lunge, V.R.; Béria, J.U.; Tietzmann, D.C.; Stein, A.T.; Simon, D. Short communication: Prevalence and risk factors for human T cell lymphotropic virus infection in Southern Brazilian HIV-positive patients. AIDS Res. Hum. Retrovir. 2014, 30, 907–911. [Google Scholar] [CrossRef]
- Guimarães, M.L.; Bastos, F.I.; Telles, P.R.; Galvão-Castro, B.; Diaz, R.S.; Bongertz, V.; Morgado, M.G. Retrovirus infections in a sample of injecting drug users in Rio de Janeiro City, Brazil: Prevalence of HIV-1 subtypes, and co-infection with HTLV-I/II. J. Clin. Virol. 2001, 21, 143–151. [Google Scholar] [CrossRef]
- Kleine Neto, W.; Sanabani, S.S.; Jamal, L.F.; Sabino, E.C. Prevalence, risk factors and genetic characterization of human T-cell lymphotropic virus types 1 and 2 in patients infected with human immunodeficiency virus type 1 in the cities of Ribeirão Preto and São Paulo. Rev. Soc. Bras. Med. Trop. 2009, 42, 264–270. [Google Scholar] [CrossRef] [Green Version]
- Marcon, C.E.M.; Campos, K.R.; Silva, G.B.D.; Schuelter-Trevisol, F.; Schlindwein, A.D.; Trevisol, D.J.; Caterino-de-Araujo, A. The first survey of human T-cell lymphotropic viruses (HTLV) in HIV/AIDS patients in Santa Catarina State, Brazil. Rev. Inst. Med. Trop. São Paulo 2019, 61. [Google Scholar] [CrossRef]
- Morimoto, H.K.; Caterino-De-Araujo, A.; Morimoto, A.A.; Reiche, E.M.; Ueda, L.T.; Matsuo, T.; Stegmann, J.W.; Reiche, F.V. Seroprevalence and risk factors for human T cell lymphotropic virus type 1 and 2 infection in human immunodeficiency virus-infected patients attending AIDS referral center health units in Londrina and other communities in Paraná, Brazil. AIDS Res. Hum. Retrovir. 2005, 21, 256–262. [Google Scholar] [CrossRef]
- Pombo-de-Oliveira, M.S.; Carvalho, S.M.; Borducchi, D.; Dobbin, J.; Salvador, J.; Correa, R.B.; Moellman, A.; Loureiro, P.; Chiattone, C.; Rios, M. Adult T-cell leukemia/lymphoma and cluster of HTLV-I associated diseases in Brazilian settings. Leuk. Lymphoma 2001, 42, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Reiche, E.M.; Bonametti, A.M.; Morimoto, H.K.; Morimoto, A.A.; Wiechemann, S.L.; Matsuo, T.; Vissoci Reiche, F.; Vogler, I.H. Epidemiological, immunological and virological characteristics, and disease progression of HIV-1/HCV-co-infected patients from a southern Brazilian population. Int. J. Mol. Med. 2008, 21, 387–395. [Google Scholar] [PubMed]
- Ribeiro, M.L.; Gonçales, J.P.; Morais, V.M.S.; Moura, L.; Coêlho, M. HTLV 1/2 Prevalence and risk factors in individuals with HIV/AIDS in Pernambuco, Brazil. Rev. Soc. Bras. Med. Trop. 2019, 52, e20180244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bautista, C.T.; Pando, M.A.; Reynaga, E.; Marone, R.; Sateren, W.B.; Montano, S.M.; Sanchez, J.L.; Avila, M.M. Sexual practices, drug use behaviors, and prevalence of HIV, syphilis, hepatitis B and C, and HTLV-1/2 in immigrant and non-immigrant female sex workers in Argentina. J. Immigr. Minor. Health 2009, 11, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Berini, C.A.; Pando, M.A.; Bautista, C.T.; Eirin, M.E.; Martinez-Peralta, L.; Weissenbacher, M.; Avila, M.M.; Biglione, M.M. HTLV-1/2 among high-risk groups in Argentina: Molecular diagnosis and prevalence of different sexual transmitted infections. J. Med. Virol. 2007, 79, 1914–1920. [Google Scholar] [CrossRef]
- Biglione, M.; Avila, M.M.; Biglione, J.; Weisburd, G.; Libonatti, O.; Gessain, A. Molecular characterization of HTLV-II from an intravenous drug addict with AIDS in Argentina. Rev. Argent. Microbiol. 1996, 28, 139–142. [Google Scholar]
- Biglione, M.; Gessain, A.; Quiruelas, S.; Fay, O.; Taborda, M.; Fernandez, E.; Lupo, S.; Panzita, A. Endemic HTLV-II infection among Tobas and Matacos Amerindians from north Argentina. J. Acquir. Immune Defic. Syndr. 1993, 6, 631–633. [Google Scholar]
- De los Angeles Pando, M.; Biglione, M.M.; Toscano, M.F.; Rey, J.A.; Russell, K.L.; Negrete, M.; Gianni, S.; Martinez-Peralta, L.; Salomon, H.; Sosa-Estani, S.; et al. Human immunodeficiency virus type 1 and other viral co-infections among young heterosexual men and women in Argentina. Am. J. Trop. Med. Hyg. 2004, 71, 153–159. [Google Scholar] [CrossRef] [Green Version]
- Lombardi, V.; Carrillo, M.G.; Alimandi, M.; Boxaca, M.; Rossi, P.; Libonatti, O. Overt and latent HIV 1 and HTLV-I infection in cohorts of at high risk individuals in Argentina. Mol. Cell. Probes 1991, 5, 409–417. [Google Scholar] [CrossRef]
- Medeot, S.; Nates, S.; Gallego, S.; Sileoni, S.; Maturano, E.; Recalde, Y.; Giordano, M.; Alvarez, R.B. HTLV-I/II seropositivity in populations at high risk for HIV-1 infection in Cordoba City, Argentina. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1998, 18, 187–188. [Google Scholar] [CrossRef]
- Pampuro, S.E.; Rabinovich, R.D.; Martinez Peralta, L.; Gallo, D.; Hanson, C.; Libonatti, O. Presence of human T-cell lymphotropic virus types I and II and coinfection with human immunodeficiency virus in different groups at risk in Argentina. J. Acquir. Immune Defic. Syndr. 1993, 6, 851–852. [Google Scholar] [PubMed]
- Pando, M.A.; Bautista, C.T.; Maulen, S.; Duranti, R.; Marone, R.; Rey, J.; Vignoles, M.; Eirin, M.E.; Biglione, M.M.; Griemberg, G.; et al. Epidemiology of human immunodeficiency virus, viral hepatitis (B and C), treponema pallidum, and human T-cell lymphotropic I/II virus among men who have sex with men in Buenos Aires, Argentina. Sex. Transm Dis. 2006, 33, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Scapellato, P.G.; Bottaro, E.G.; Seoane, M.B.; Rodriguez Brieschke, M.T.; Scapellato, J.L.; Dato, A.; Vidal, G.I. Clinical, epidemiological and immunological study of patients coinfected with HIV and HTLV-1. Medicina 2004, 64, 413–418. [Google Scholar] [PubMed]
- Flores-Castañeda, M.S.; Salinas-Carmona, M.C.; Leal-González, C.; Yáñez-Rodríguez, A.; Trejo-Avila, L.M. Antibodies against human T-cell lymphotropic viruses in subjects at high risk for HIV in Monterrey. Rev. Investig. Clin. 1992, 44, 37–41. [Google Scholar]
- Gongora-Biachi, R.A.; Gonzalez-Martinez, P.; Castros-Sansores, C.; Pavia-Ruz, N.; Rudolph, D.L.; Lal, R.B. Human T lymphotropic virus type II (HTLV-II) infection among female prostitutes in Yucatan, Mexico. Am. J. Med. Sci. 1993, 306, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Martinez, P.; Castro-Sansores, C.; Vivas-Rosel, M.L.; Gongora-Biachi, R.A. Infection by human T-cell lymphotropic virus type I/II in polytransfused patients in the state of Yucatan, Mexico. Sangre 1994, 39, 45–48. [Google Scholar] [PubMed]
- Vazquez-Valls, E.; Campos-Lopez, P.I.; Torres-Mendoza, B.M.; Alvarez-Maya, I.; Gonzalez-Mendoza, A. Prevalence of anti-HTLV-I antibodies in HIV-seropositive individuals in Guadalajara, Mexico. J. Acquir. Immune Defic. Syndr. 1993, 6, 965–966. [Google Scholar]
- Palenzuela, D.; Rivero, J.; Nazabal, M. Failure to detect serological evidence of HTLV-I/II infection among HIV patients in Cuba. Vox Sang. 1994, 67, 78. [Google Scholar] [CrossRef]
- De Batänjer, E.C.; de Pérez, G.E. HTLV-I/II seroprevalence in Gay men and female sex workers on Margarita Island, Venezuela. Rev. Soc. Bras. Med. Trop. 1998, 31, 391–393. [Google Scholar] [CrossRef]
- Stewart, J.; Heitzinger, K.; Pollett, S.; Calderón, M.; Alarcón, J.; Ton, T.G.; Zunt, J.R. The Changing Epidemiology of Human T-Cell Lymphotropic Virus Type 1 Infection in Peruvian Female Sex Workers, 1993–2010. Am. J. Trop. Med. Hyg. 2017, 96, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Arango, C.; Maloney, E.; Rugeles, M.T.; Bernal, E.; Bernal, C.; Borrero, I.; Herrera, S.; Restrepo, M.; Espinal, A.; Blattner, W.A. HTLV-I and HTLV-II coexist among the Embera and Inga Amerindians of Colombia. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1999, 20, 102–103. [Google Scholar] [CrossRef] [PubMed]
- Duenas-Barajas, E.; Bernal, J.E.; Vaught, D.R.; Nerurkar, V.R.; Sarmiento, P.; Yanagihara, R.; Gajdusek, D.C. Human retroviruses in Amerindians of Colombia: High prevalence of human T cell lymphotropic virus type II infection among the Tunebo Indians. Am. J. Trop. Med. Hyg. 1993, 49, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Fujiyama, C.; Fujiyoshi, T.; Miura, T.; Yashiki, S.; Matsumoto, D.; Zaninovic, V.; Blanco, O.; Harrington, W., Jr.; Byrnes, J.J.; Hayami, M.; et al. A new endemic focus of human T lymphotropic virus type II carriers among Orinoco natives in Colombia. J. Infect. Dis. 1993, 168, 1075–1077. [Google Scholar] [CrossRef] [PubMed]
- Zaninovic, V.; Sanzon, F.; Lopez, F.; Velandia, G.; Blank, A.; Blank, M.; Fujiyama, C.; Yashiki, S.; Matsumoto, D.; Katahira, Y.; et al. Geographic independence of HTLV-I and HTLV-II foci in the Andes highland, the Atlantic coast, and the Orinoco of Colombia. AIDS Res. Hum. Retrovir. 1994, 10, 97–101. [Google Scholar] [CrossRef]
- Ita, F.; Mayer, E.F.; Verdonck, K.; Gonzalez, E.; Clark, D.; Gotuzzo, E. Human T-lymphotropic virus type 1 infection is frequent in rural communities of the southern Andes of Peru. Int. J. Infect. Dis. 2014, 19, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Zurita, S.; Costa, C.; Watts, D.; Indacochea, S.; Campos, P.; Sanchez, J.; Gotuzzo, E. Prevalence of human retroviral infection in Quillabamba and Cuzco, Peru: A new endemic area for human T cell lymphotropic virus type 1. Am. J. Trop. Med. Hyg. 1997, 56, 561–565. [Google Scholar] [CrossRef]
- Alva, I.E.; Orellana, E.R.; Blas, M.M.; Bernabe-Ortiz, A.; Cotrina, A.; Chiappe, M.; Kochel, T.J.; Carcamo, C.P.; Garcia, P.J.; Zunt, J.R.; et al. HTLV-1 and -2 infections among 10 indigenous groups in the Peruvian Amazon. Am. J. Trop. Med. Hyg. 2012, 87, 954–956. [Google Scholar] [CrossRef] [Green Version]
- Blas, M.M.; Alva, I.E.; Garcia, P.J.; Carcamo, C.; Montano, S.M.; Mori, N.; Munante, R.; Zunt, J.R. High prevalence of human T-lymphotropic virus infection in indigenous women from the peruvian Amazon. PLoS ONE 2013, 8, e73978. [Google Scholar] [CrossRef]
- Cartier, L.; Araya, F.; Castillo, J.L.; Zaninovic, V.; Hayami, M.; Miura, T.; Imai, J.; Sonoda, S.; Shiraki, H.; Miyamoto, K.; et al. Southernmost carriers of HTLV-I/II in the world. Jpn. J. Cancer Res. 1993, 84, 1–3. [Google Scholar] [CrossRef]
- Cartier, L.; Tajima, K.; Araya, F.; Castillo, J.L.; Zaninovic, V.; Hayami, M.; Imai, J.; Born, P.; Cardenas, M.; Moreno, J.; et al. Preliminary study of HTLV-I seroprevalence in Chilean Indian populations. Rev. Med. Chile 1993, 121, 241–246. [Google Scholar]
- Inostroza, J.; Diaz, P.; Saunier, C. Prevalence of antibodies to HTLV-1 in South American Indians (Mapuches) from Chile. Scand. J. Infect. Dis. 1991, 23, 507–508. [Google Scholar] [CrossRef] [PubMed]
- Fujiyoshi, T.; Li, H.C.; Lou, H.; Yashiki, S.; Karino, S.; Zaninovic, V.; Oneegllo, S.G.; Camacho, M.; Andrade, R.; Hurtado, L.V.; et al. Characteristic distribution of HTLV type I and HTLV type II carriers among native ethnic groups in South America. AIDS Res. Hum. Retrovir. 1999, 15, 1235–1239. [Google Scholar] [CrossRef] [PubMed]
- Maloney, E.M.; Biggar, R.J.; Neel, J.V.; Taylor, M.E.; Hahn, B.H.; Shaw, G.M.; Blattner, W.A. Endemic human T cell lymphotropic virus type II infection among isolated Brazilian Amerindians. J. Infect. Dis. 1992, 166, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Menna-Barreto, M.; Bender, A.L.; Bonatto, S.L.; Freitas, L.B.; Salzano, F.M.; Tsuneto, L.T.; Petzl-Erler, M.L. Human T-cell lymphotropic virus type II in Guarani Indians, Southern Brazil. Cad. Saúde Pública 2005, 21, 1947–1951. [Google Scholar] [CrossRef] [Green Version]
- Biglione, M.; Vidan, O.; Mahieux, R.; de Colombo, M.; de los Angeles de Basualdo, M.; Bonnet, M.; Pankow, G.; De Efron, M.A.; Zorrilla, A.; Tekaia, F.; et al. Seroepidemiological and molecular studies of human T cell lymphotropic virus type II, subtype b, in isolated groups of Mataco and Toba Indians of northern Argentina. AIDS Res. Hum. Retrovir. 1999, 15, 407–417. [Google Scholar] [CrossRef]
- Bouzas, M.B.; Zapiola, I.; Quiruelas, S.; Gorvein, D.; Panzita, A.; Rey, J.; Carnese, F.P.; Corral, R.; Perez, C.; Zala, C.; et al. HTLV type I and HTLV type II infection among Indians and natives from Argentina. AIDS Res. Hum. Retrovir. 1994, 10, 1567–1571. [Google Scholar] [CrossRef]
- Ferrer, J.F.; Esteban, E.; Dube, S.; Basombrio, M.A.; Segovia, A.; Peralta-Ramos, M.; Dube, D.K.; Sayre, K.; Aguayo, N.; Hengst, J.; et al. Endemic infection with human T cell leukemia/lymphoma virus type IIB in Argentinean and Paraguayan Indians: Epidemiology and molecular characterization. J. Infect. Dis. 1996, 174, 944–953. [Google Scholar] [CrossRef] [Green Version]
- Medeot, S.; Nates, S.; Recalde, A.; Gallego, S.; Maturano, E.; Giordano, M.; Serra, H.; Reategui, J.; Cabezas, C. Prevalence of antibody to human T cell lymphotropic virus types 1/2 among aboriginal groups inhabiting northern Argentina and the Amazon region of Peru. Am. J. Trop. Med. Hyg. 1999, 60, 623–629. [Google Scholar] [CrossRef] [Green Version]
- Echeverria de Perez, G.; Leon-Ponte, M.; Noya, O.; Botto, C.; Gallo, D.; Bianco, N. First description of endemic HTLV-II infection among Venezuelan Amerindians. J. Acquir. Immune Defic. Syndr. 1993, 6, 1368–1372. [Google Scholar]
- Leon-Ponte, M.; Echeverria de Perez, G.; Bianco, N.; Hengst, J.; Dube, S.; Love, J.; Poiesz, B.J. Endemic infection with HTLV-IIB in Venezuelan Indians: Molecular characterization. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1998, 17, 458–464. [Google Scholar] [CrossRef]
- Leon-Ponte, M.; Noya, O.; Bianco, N.; Echeverria de Perez, G. Highly endemic human T-lymphotropic virus type II (HTLV-II) infection in a Venezuelan Guahibo Amerindian group. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1996, 13, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Dangond, F.; Daza, J.S.; Rosania, A.; Quin, M.J.; Zaninovic, V.; Chaplin, B.; Marlink, R.; Hafler, D.A. Tropical spastic paraparesis on the Caribbean coast of Colombia. Am. J. Trop. Med. Hyg. 1995, 52, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Rodgers-Johnson, P.; Gajdusek, D.C.; Morgan, O.S.; Zaninovic, V.; Sarin, P.S.; Graham, D.S. HTLV-I and HTLV-III antibodies and tropical spastic paraparesis. Lancet 1985, 2, 1247–1248. [Google Scholar] [CrossRef]
- Roman, G.C.; Roman, L.N. Tropical spastic paraparesis. A clinical study of 50 patients from Tumaco (Colombia) and review of the worldwide features of the syndrome. J. Neurol. Sci. 1988, 87, 121–138. [Google Scholar] [PubMed]
- Vernant, J.C.; Maurs, L.; Gessain, A.; Barin, F.; Gout, O.; Delaporte, J.M.; Sanhadji, K.; Buisson, G.; de-The, G. Endemic tropical spastic paraparesis associated with human T-lymphotropic virus type I: A clinical and seroepidemiological study of 25 cases. Ann. Neurol. 1987, 21, 123–130. [Google Scholar] [CrossRef]
- Zaninovic, V.; Leon, S.F. Fifteen years of follow-up on HTLV-I positive and HTLV-I negative spastic paraparesis patients in southwestern Colombia, South America. J. Neurovirol. 1996, 2, 357–360. [Google Scholar] [CrossRef]
- Gotuzzo, E.; Cabrera, J.; Deza, L.; Verdonck, K.; Vandamme, A.M.; Cairampoma, R.; Vizcarra, D.; Cabada, M.; Narvarte, G.; De las Casas, C. Clinical characteristics of patients in Peru with human T cell lymphotropic virus type 1-associated tropical spastic paraparesis. Clin. Infect. Dis. 2004, 39, 939–944. [Google Scholar] [CrossRef] [Green Version]
- Gotuzzo, E.; De Las Casas, C.; Deza, L.; Cabrera, J.; Castaneda, C.; Watts, D. Tropical spastic paraparesis and HTLV-I infection: Clinical and epidemiological study in Lima, Peru. J. Neurol. Sci. 1996, 143, 114–117. [Google Scholar] [CrossRef]
- Gotuzzo, E.; Moody, J.; Verdonck, K.; Cabada, M.M.; Gonzalez, E.; Van Dooren, S.; Vandamme, A.M.; Terashima, A.; Vermund, S.H. Frequent HTLV-1 infection in the offspring of Peruvian women with HTLV-1-associated myelopathy/tropical spastic paraparesis or strongyloidiasis. Panam. Salud Pública 2007, 22, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Talledo, M.; Lopez, G.; Huyghe, J.R.; Verdonck, K.; Adaui, V.; Gonzalez, E.; Best, I.; Clark, D.; Vanham, G.; Gotuzzo, E.; et al. Evaluation of host genetic and viral factors as surrogate markers for HTLV-1-associated myelopathy/tropical spastic paraparesis in Peruvian HTLV-1-infected patients. J. Med. Virol. 2010, 82, 460–466. [Google Scholar] [CrossRef]
- Torres-Cabala, C.A.; Curry, J.L.; Li Ning Tapia, E.M.; Ramos, C.; Tetzlaff, M.T.; Prieto, V.G.; Miranda, R.N.; Bravo, F. HTLV-1-associated infective dermatitis demonstrates low frequency of FOXP3-positive T-regulatory lymphocytes. J. Dermatol. Sci. 2015, 77, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Kendall, E.A.; Gonzalez, E.; Espinoza, I.; Tipismana, M.; Verdonck, K.; Clark, D.; Vermund, S.H.; Gotuzzo, E. Early neurologic abnormalities associated with human T-cell lymphotropic virus type 1 infection in a cohort of Peruvian children. J. Pediatr. 2009, 155, 700–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barros, N.; Risco, J.; Rodriguez, C.; Sanchez, C.; Gonzalez, E.; Tanaka, Y.; Gotuzzo, E.; White, A.C.; Montes, M. CD4+ T cell subsets and Tax expression in HTLV-1 associated diseases. Pathog. Glob. Health 2013, 107, 202–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malpica, L.; White, A.C., Jr.; Leguia, C.; Freundt, N.; Barros, N.; Chian, C.; Antunez, E.A.; Montes, M. Regulatory T cells and IgE expression in duodenal mucosa of Strongyloides stercoralis and human T lymphotropic virus type 1 co-infected patients. PLoS Negl. Trop. Dis. 2019, 13, e0007415. [Google Scholar] [CrossRef]
- Cartier, L.; Ramirez, E. Presence of HTLV-I Tax protein in cerebrospinal fluid from HAM/TSP patients. Arch. Virol. 2005, 150, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Cartier-Rovirosa, L.; Mora, C.; Araya, F.; Castillo, J.; Verdugo, R.; Miller, M.A.; Gajdusek, D.C.; Gibbs, C.J., Jr. HTLV-I positive spastic paraparesis in a temperate zone. Lancet 1989, 1, 556–557. [Google Scholar] [CrossRef]
- Ramirez, E.; Cartier, L.; Rodriguez, L.; Alberti, C.; Valenzuela, M.A. In vivo fluctuation of Tax, Foxp3, CTLA-4, and GITR mRNA expression in CD4(+)CD25(+) T cells of patients with human T-lymphotropic virus type 1-associated myelopathy. Braz. J. Med. Biol. Res. 2010, 43, 1109–1115. [Google Scholar] [CrossRef] [Green Version]
- Ramirez, E.; Fernandez, J.; Cartier, L.; Villota, C.; Rios, M. Defective human T-cell lymphotropic virus type I (HTLV-I) provirus in seronegative tropical spastic paraparesis/HTLV-I-associated myelopathy (TSP/HAM) patients. Virus Res. 2003, 91, 231–239. [Google Scholar] [CrossRef]
- Biglione, M.M.; Pizarro, M.; Puca, A.; Salomon, H.E.; Berria, M.I. A cluster of human T-cell lymphotropic virus type I-associated myelopathy/tropical spastic paraparesis in Jujuy, Argentina. J. Acquir. Immune Defic. Syndr. 2003, 32, 441–445. [Google Scholar] [CrossRef]
- Biglione, M.M.; Pizarro, M.; Salomon, H.E.; Berria, M.I. A possible case of myelopathy/tropical spastic paraparesis in an Argentinian woman with human T lymphocyte virus type II. Clin. Infect. Dis. 2003, 37, 456–458. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, L.A.; Villa, A.M.; Kohler, G.; Garcea, O.; Kremenchutzky, M.; Caceres, F.; Sanz, O.P.; Sica, R.E. Further studies on HTLV-I associated myelopathy in Argentina. Medicina 1998, 58, 411–414. [Google Scholar] [PubMed]
- Lupo, S.; Berini, C.; Canepa, C.; Santini Araujo, E.; Biglione, M. Undifferentiated Pleomorphic Sarcoma and the Importance of Considering the Oncogenic and Immune-Suppressant Role of the Human T-Cell Lymphotropic Virus Type 1: A Case Report. Front. Oncol. 2017, 7, e00091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zala, C.; Zapiola, I.; Bouzas, M.B.; Benetucci, J.; Lopez, L.; Gallo, D.; Hanson, C.; Muchinik, G.R. Human T-cell lymphotropic virus type I disease in Argentine intravenous drug users with human immunodeficiency virus type 1 infection. J. Acquir. Immune Defic. Syndr. 1994, 7, 870–871. [Google Scholar]
- Fukutani, E.R.; Ramos, P.I.P.; Kasprzykowski, J.I.; Azevedo, L.G.; Rodrigues, M.M.S.; Lima, J.; de Araujo Junior, H.F.S.; Fukutani, K.F.; de Queiroz, A.T.L. Meta-Analysis of HTLV-1-Infected Patients Identifies CD40LG and GBP2 as Markers of ATLL and HAM/TSP Clinical Status: Two Genes Beat as One. Front. Genet. 2019, 10, 1056. [Google Scholar] [CrossRef] [PubMed]
- Gomes, I.; Melo, A.; Proietti, F.A.; Moreno-Carvalho, O.; Loures, L.A.; Dazza, M.C.; Said, G.; Larouze, B.; Galvao-Castro, B. Human T lymphotropic virus type I (HTLV-I) infection in neurological patients in Salvador, Bahia, Brazil. J. Neurol. Sci. 1999, 165, 84–89. [Google Scholar] [CrossRef]
- Oliveira, P.D.; de Carvalho, R.F.; Bittencourt, A.L. Adult T-cell leukemia/lymphoma in South and Central America and the Caribbean: Systematic search and review. Int. J. STD AIDS 2017, 28, 217–228. [Google Scholar] [CrossRef]
- Oliveira, P.D.; Kachimarek, A.C.; Bittencourt, A.L. Early Onset of HTLV-1 Associated Myelopathy/Tropical Spastic Paraparesis (HAM/TSP) and Adult T-cell Leukemia/Lymphoma (ATL): Systematic Search and Review. J. Trop. Pediatr. 2018, 64, 151–161. [Google Scholar] [CrossRef] [Green Version]
- Casseb, J.; de Oliveira, A.C.; Vergara, M.P.; Montanheiro, P.; Bonasser, F.; Meilman Ferreira, C.; Smid, J.; Duarte, A.J. Presence of tropical spastic paraparesis/human T-cell lymphotropic virus type 1-associated myelopathy (TSP/HAM)-like among HIV-1-infected patients. J. Med. Virol. 2008, 80, 392–398. [Google Scholar] [CrossRef]
- Harrison, L.H.; Vaz, B.; Taveira, D.M.; Quinn, T.C.; Gibbs, C.J.; de Souza, S.H.; McArthur, J.C.; Schechter, M. Myelopathy among Brazilians coinfected with human T-cell lymphotropic virus type I and HIV. Neurology 1997, 48, 13–18. [Google Scholar] [CrossRef]
- De Oliveira Mde, F.; Fatal, P.L.; Primo, J.R.; da Silva, J.L.; Batista Eda, S.; Farré, L.; Bittencourt, A.L. Infective dermatitis associated with human T-cell lymphotropic virus type 1: Evaluation of 42 cases observed in Bahia, Brazil. Clin. Infect. Dis. 2012, 54, 1714–1719. [Google Scholar] [CrossRef] [Green Version]
- Bonamigo, R.R.; Borges, K.; Rietjens, J.; Arenzon, S.; Blanco, L.F.; Loureiro, R. Human T lymphotropic virus 1 and hepatitis C virus as risk factors for inflammatory dermatoses in HIV-positive patients. Int. J. Dermatol. 2004, 43, 568–570. [Google Scholar] [CrossRef] [PubMed]
- Dantas, L.; Netto, E.; Glesby, M.J.; Carvalho, E.M.; Machado, P. Dermatological manifestations of individuals infected with human T cell lymphotropic virus type I (HTLV-I). Int. J. Dermatol. 2014, 53, 1098–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nobre, V.; Guedes, A.C.; Proietti, F.A.; Martins, M.L.; Nassif, G.; Serufo, J.C.; Lambertucci, J.R. Increased prevalence of human T cell lymphotropic virus type 1 in patients attending a Brazilian dermatology clinic. Intervirology 2007, 50, 316–318. [Google Scholar] [CrossRef] [PubMed]
- Okajima, R.; Casseb, J.; Sanches, J.A. Co-presentation of human T-cell lymphotropic virus type 1 (HTLV-1)-associated myelopathy/tropical spastic paraparesis and adult-onset infective dermatitis associated with HTLV-1 infection. Int. J. Dermatol. 2013, 52, 63–68. [Google Scholar] [CrossRef]
- Okajima, R.; Oliveira, A.C.; Smid, J.; Casseb, J.; Sanches, J.A., Jr. High prevalence of skin disorders among HTLV-1 infected individuals independent of clinical status. PLoS Negl. Trop. Dis. 2013, 7, e2546. [Google Scholar] [CrossRef] [Green Version]
- Martins, F.M.; Casseb, J.; Penalva-de-Oliveira, A.C.; de Paiva, M.F.; Watanuki, F.; Ortega, K.L. Oral manifestations of human T-cell lymphotropic virus infection in adult patients from Brazil. Oral Dis. 2010, 16, 167–171. [Google Scholar] [CrossRef]
- Rathsam-Pinheiro, R.H.; Boa-Sorte, N.; Castro-Lima-Vargens, C.; Pinheiro, C.A.; Castro-Lima, H.; Galvao-Castro, B. Ocular lesions in HTLV-1 infected patients from Salvador, State of Bahia: The city with the highest prevalence of this infection in Brazil. Rev. Soc. Bras. Med. Trop. 2009, 42, 633–637. [Google Scholar] [CrossRef] [Green Version]
- Leite, A.C.; Silva, M.T.; Alamy, A.H.; Afonso, C.R.; Lima, M.A.; Andrada-Serpa, M.J.; Nascimento, O.J.; Araujo, A.Q. Peripheral neuropathy in HTLV-I infected individuals without tropical spastic paraparesis/HTLV-I-associated myelopathy. J. Neurol. 2004, 251, 877–881. [Google Scholar] [CrossRef]
- Chavez, M.; Domiguez, M.C.; Blank, A.; Quintana, M.; Eizuru, Y.; Garcia, F. Molecular evolution and geographic origins of type 1 human lymphotrophic virus in Colombia detected by RFLP polymorphism. Biomedica 2004, 24, 20–32. [Google Scholar]
- Magri, M.C.; Brigido, L.F.; Rodrigues, R.; Morimoto, H.K.; Ferreira, J.L.; Caterino-de-Araujo, A. Phylogenetic and similarity analysis of HTLV-1 isolates from HIV-coinfected patients from the south and southeast regions of Brazil. AIDS Res. Hum. Retrovir. 2012, 28, 110–114. [Google Scholar] [CrossRef]
- Miura, T.; Yamashita, M.; Zaninovic, V.; Cartier, L.; Takehisa, J.; Igarashi, T.; Ido, E.; Fujiyoshi, T.; Sonoda, S.; Tajima, K.; et al. Molecular phylogeny of human T-cell leukemia virus type I and II of Amerindians in Colombia and Chile. J. Mol. Evol. 1997, 44, S76–S82. [Google Scholar] [CrossRef] [PubMed]
- Nobre, A.F.S.; Almeida, D.S.; Ferreira, L.C.; Ferreira, D.L.; Junior, E.C.S.; Viana, M.; Silva, I.C.; Pinheiro, B.T.; Ferrari, S.F.; Linhares, A.D.C.; et al. Low genetic diversity of the Human T-cell Lymphotropic Virus (HTLV-1) in an endemic area of the Brazilian Amazon basin. PLoS ONE 2018, 13, e0194184. [Google Scholar] [CrossRef] [Green Version]
- Love, J.L.; Marchioli, C.C.; Dube, S.; Bryz-Gornia, V.; Loughran, T.P., Jr.; Glaser, J.B.; Esteban, E.; Feldman, L.; Ferrer, J.F.; Poiesz, B.J. Expansion of clonotypic T-cell populations in the peripheral blood of asymptomatic Gran Chaco Amerindians infected with HTLV-IIB. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 1998, 18, 178–185. [Google Scholar] [CrossRef]
- Santos, E.L.; Tamegao-Lopes, B.; Machado, L.F.; Ishak Mde, O.; Ishak, R.; Lemos, J.A.; Vallinoto, A.C. Molecular characterization of HTLV-1/2 among blood donors in Belem, State of Para: First description of HTLV-2b subtype in the Amazon region. Rev. Soc. Bras. Med. Trop. 2009, 42, 271–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pardi, D.; Switzer, W.M.; Hadlock, K.G.; Kaplan, J.E.; Lal, R.B.; Folks, T.M. Complete nucleotide sequence of an Amerindian human T-cell lymphotropic virus type II (HTLV-II) isolate: Identification of a variant HTLV-II subtype b from a Guaymi Indian. J. Virol. 1993, 67, 4659–4664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magri, M.C.; Brigido, L.F.; Morimoto, H.K.; Caterino-de-Araujo, A. Human T cell lymphotropic virus type 2a strains among HIV type 1-coinfected patients from Brazil have originated mostly from Brazilian Amerindians. AIDS Res. Hum. Retrovir. 2013, 29, 1010–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallinoto, A.C.; Ishak, M.O.; Azevedo, V.N.; Vicente, A.C.; Otsuki, K.; Hall, W.W.; Ishak, R. Molecular epidemiology of human T-lymphotropic virus type II infection in Amerindian and urban populations of the Amazon region of Brazil. Hum. Biol. 2002, 74, 633–644. [Google Scholar] [CrossRef]
- Switzer, W.M.; Black, F.L.; Pieniazek, D.; Biggar, R.J.; Lal, R.B.; Heneine, W. Endemicity and phylogeny of the human T cell lymphotropic virus type II subtype A from the Kayapo Indians of Brazil: Evidence for limited regional dissemination. AIDS Res. Hum. Retrovir. 1996, 12, 635–640. [Google Scholar] [CrossRef]
- Grande, B.M.; Gerhard, D.S.; Jiang, A.; Griner, N.B.; Abramson, J.S.; Alexander, T.B.; Allen, H.; Ayers, L.W.; Bethony, J.M.; Bhatia, K.; et al. Genome-wide discovery of somatic coding and noncoding mutations in pediatric endemic and sporadic Burkitt lymphoma. Blood 2019, 133, 1313–1324. [Google Scholar] [CrossRef]
- Montes-Mojarro, I.A.; Kim, W.Y.; Fend, F.; Quintanilla-Martinez, L. Epstein—Barr virus positive T and NK-cell lymphoproliferations: Morphological features and differential diagnosis. Semin. Diagn. Pathol. 2020, 37, 32–46. [Google Scholar] [CrossRef]
- Ok, C.Y.; Li, L.; Xu-Monette, Z.Y.; Visco, C.; Tzankov, A.; Manyam, G.C.; Montes-Moreno, S.; Dybkaer, K.; Chiu, A.; Orazi, A.; et al. Prevalence and clinical implications of epstein-barr virus infection in de novo diffuse large B-cell lymphoma in Western countries. Clin. Cancer Res. 2014, 20, 2338–2349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J.I.; Iwatsuki, K.; Ko, Y.H.; Kimura, H.; Manoli, I.; Ohshima, K.; Pittaluga, S.; Quintanilla-Martinez, L.; Jaffe, E.S. Epstein-Barr virus NK and T cell lymphoproliferative disease: Report of a 2018 international meeting. Leuk. Lymphoma 2020, 61, 808–819. [Google Scholar] [CrossRef] [PubMed]
- Koo, G.C.; Tan, S.Y.; Tang, T.; Poon, S.L.; Allen, G.E.; Tan, L.; Chong, S.C.; Ong, W.S.; Tay, K.; Tao, M.; et al. Janus kinase 3-activating mutations identified in natural killer/T-cell lymphoma. Cancer Discov. 2012, 2, 591–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Küçük, C.; Jiang, B.; Hu, X.; Zhang, W.; Chan, J.K.; Xiao, W.; Lack, N.; Alkan, C.; Williams, J.C.; Avery, K.N.; et al. Activating mutations of STAT5B and STAT3 in lymphomas derived from γδ-T or NK cells. Nat. Commun. 2015, 6, 6025. [Google Scholar] [CrossRef] [Green Version]
- Montes-Mojarro, I.A.; Chen, B.J.; Ramirez-Ibarguen, A.F.; Quezada-Fiallos, C.M.; Perez-Baez, W.B.; Duenas, D.; Casavilca-Zambrano, S.; Ortiz-Mayor, M.; Rojas-Bilbao, E.; Garcia-Rivello, H.; et al. Mutational profile and EBV strains of extranodal NK/T-cell lymphoma, nasal type in Latin America. Mod. Pathol. 2020, 33, 781–791. [Google Scholar] [CrossRef]
- Garcia, A.; Olivella, F.; Valderrama, S.; Rodriguez, G. Kaposi’s sarcoma in Colombia. Cancer 1989, 64, 2393–2398. [Google Scholar] [CrossRef]
- Kourí, V.; Martínez, P.A.; Blanco, O.; Capó, V.; Rodríguez, M.E.; Dovigny, M.D.C.; Cardellá, L.; Gala, A.; Jiménez, N.A.; Correa, C.; et al. Simultaneous quantification of human herpesvirus 8 DNA by real time PCR in different tissues of HIV infected cuban patients with Kaposi’s sarcoma. Herpesviridae 2010, 1, 3. [Google Scholar] [CrossRef] [Green Version]
- Maita Zegarra, R.B.; Meléndez Guevara, R.A.; Seminario de Rivera, V. Factor VIII en sarcoma de Kaposi y verruga peruana. Galeno 1985, 15, 14–17. [Google Scholar]
- CA, C. Tumores Cutáneos en el Hospital Cayetano Heredia Entre Los Años. Tesis para Optar el Título de Médico Cirujano 1992–1995. Ph.D. Thesis, Universidad Peruana Cayetano, San Martin, Peru.
- Borges, J.D.; Souza, V.A.; Giambartolomei, C.; Dudbridge, F.; Freire, W.S.; Gregorio, S.A.; Torrez, P.P.; Quiroga, M.; Mayaud, P.; Pannuti, C.S.; et al. Transmission of human herpesvirus type 8 infection within families in american indigenous populations from the Brazilian Amazon. J. Infect. Dis. 2012, 205, 1869–1876. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control. Human T-lymphotropic virus type II among Guaymi Indians-Panama. MMWR. Morb. Mortal. Wkly. Rep. 1992, 41, 209–211. [Google Scholar]
- Gonzalez-Perez, M.P.; Munoz-Juarez, L.; Cardenas, F.C.; Zarranz Imirizaldu, J.J.; Carranceja, J.C.; Garcia-Saiz, A. Human T-cell leukemia virus type I infection in various recipients of transplants from the same donor. Transplantation 2003, 75, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Zaninovic, V.; Biojó, R.; Barreto, P. Paraparesia espástica del Pacífico. Colombia Med. 1981, 12, 111–117. [Google Scholar]
- Zabaleta, M.; Peralta, J.; Birges, J.; Bianco, N.; Echeverria de Perez, G. HTLV-I-associated myelopathy in Venezuela. J. Acquir. Immune Defic. Syndr. 1994, 7, 1289–1290. [Google Scholar] [CrossRef] [PubMed]
- Iwanaga, M.; Watanabe, T.; Yamaguchi, K. Adult T-cell leukemia: A review of epidemiological evidence. Front. Microbiol. 2012, 3, e00322. [Google Scholar] [CrossRef] [Green Version]








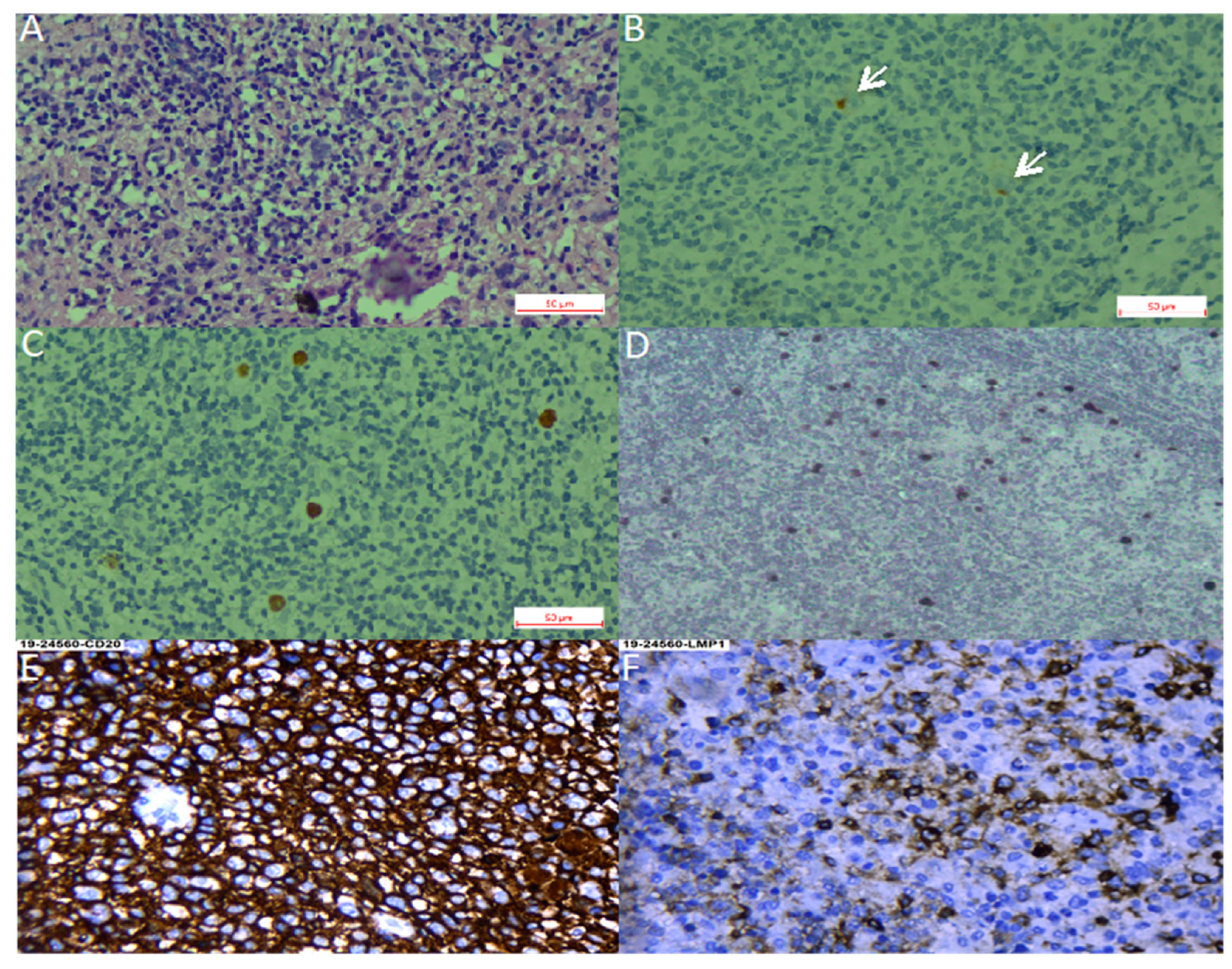{kind=link}
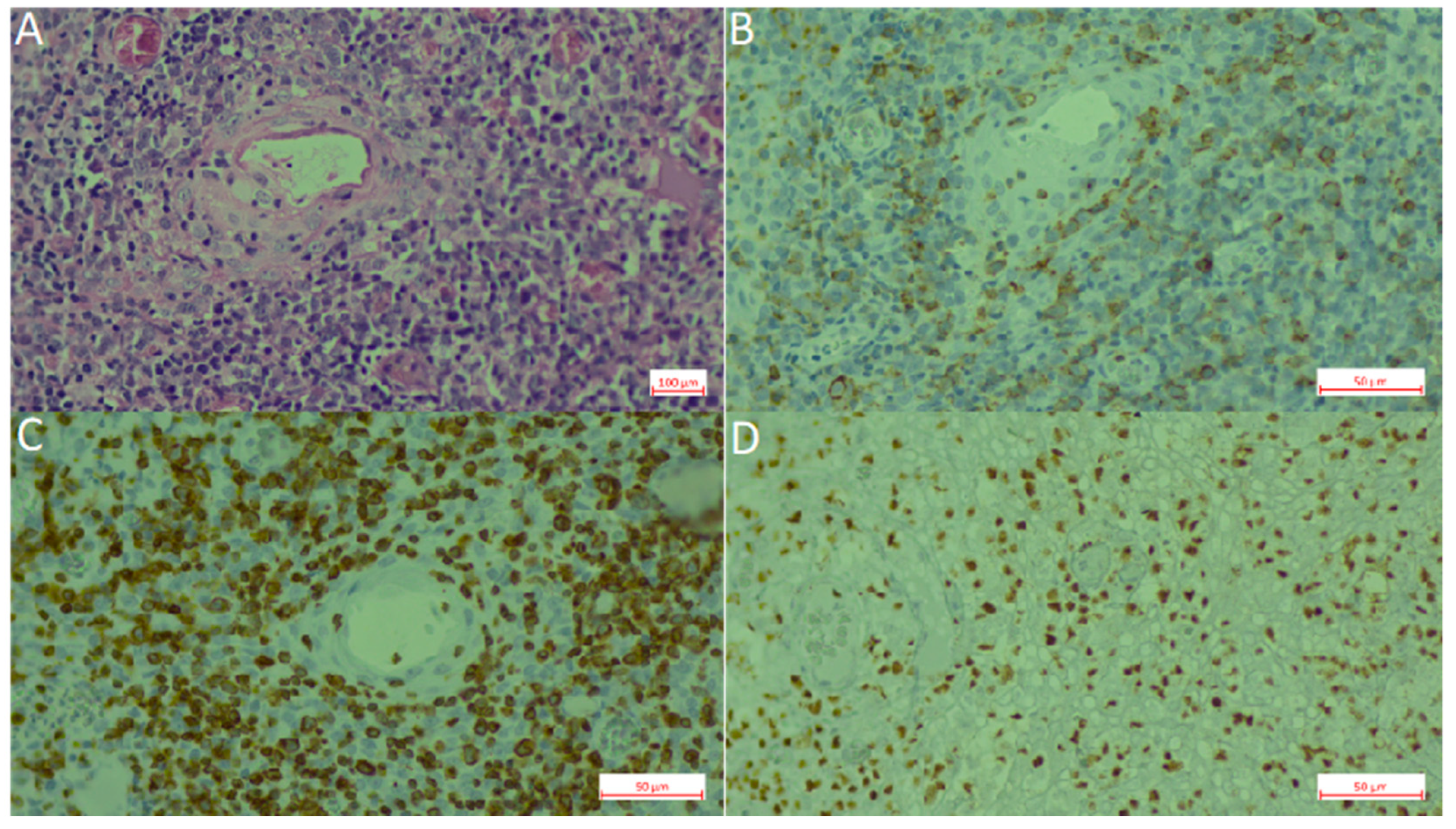{kind=link}
{kind=link}
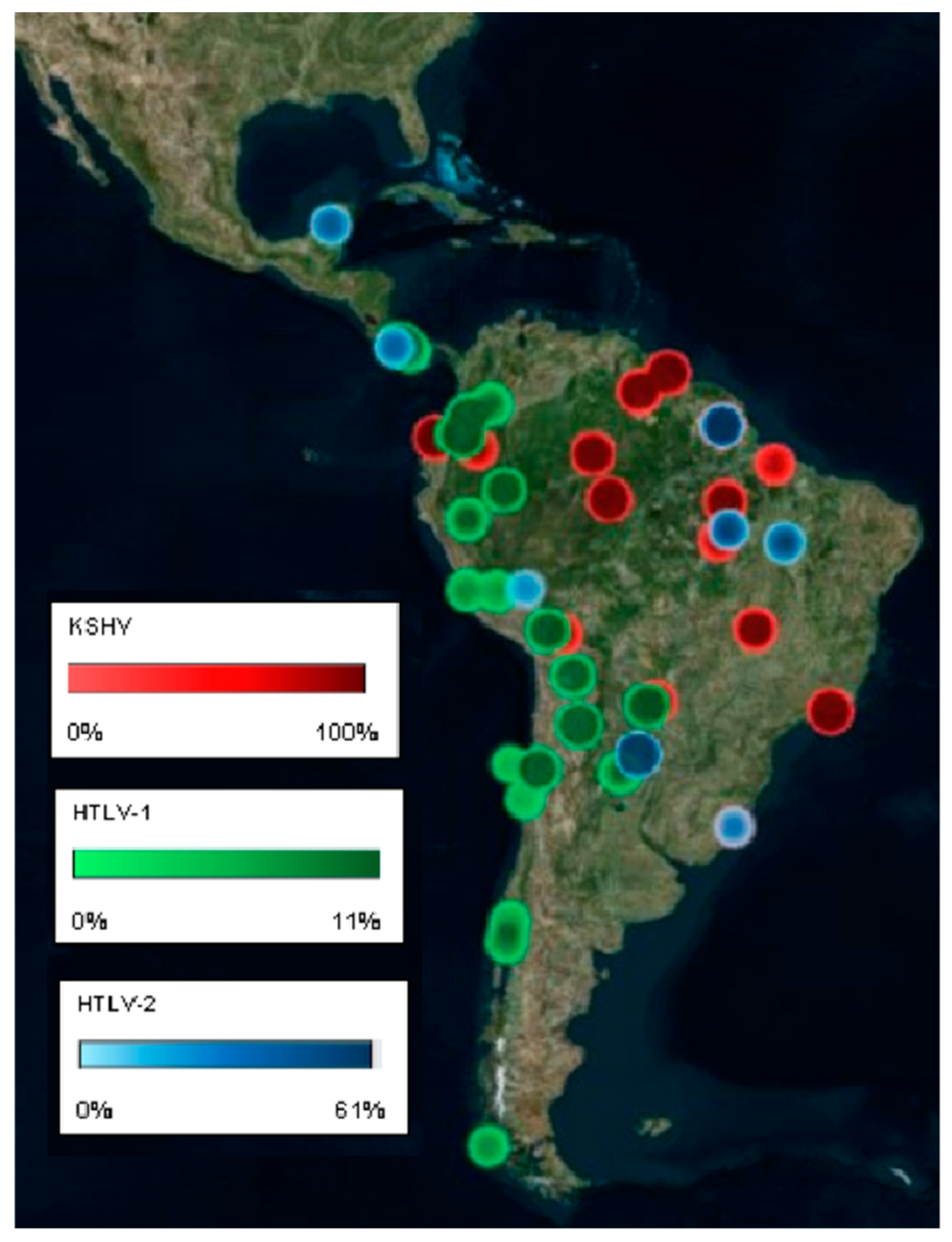{kind=link}
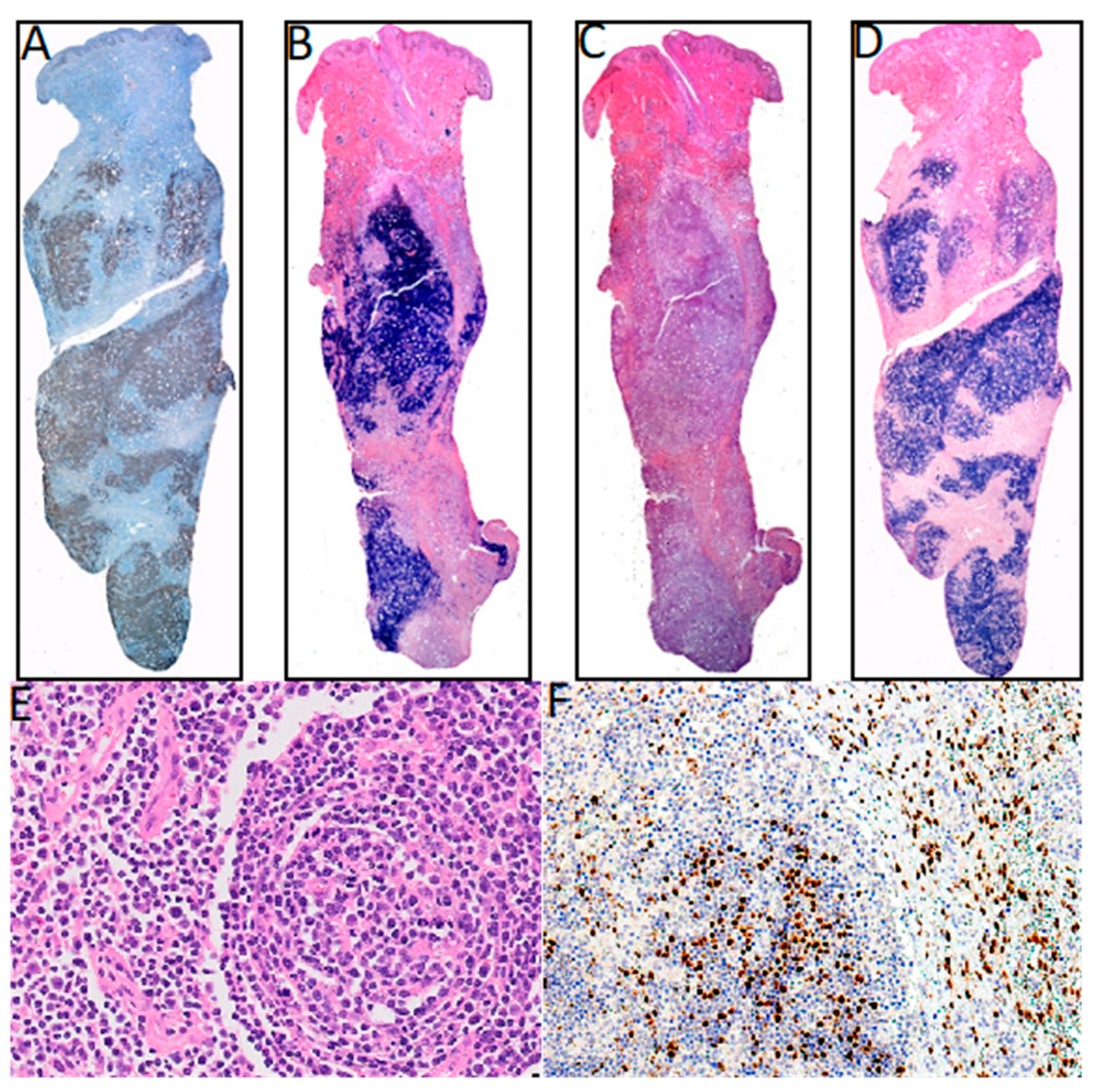{kind=link}
{kind=link}
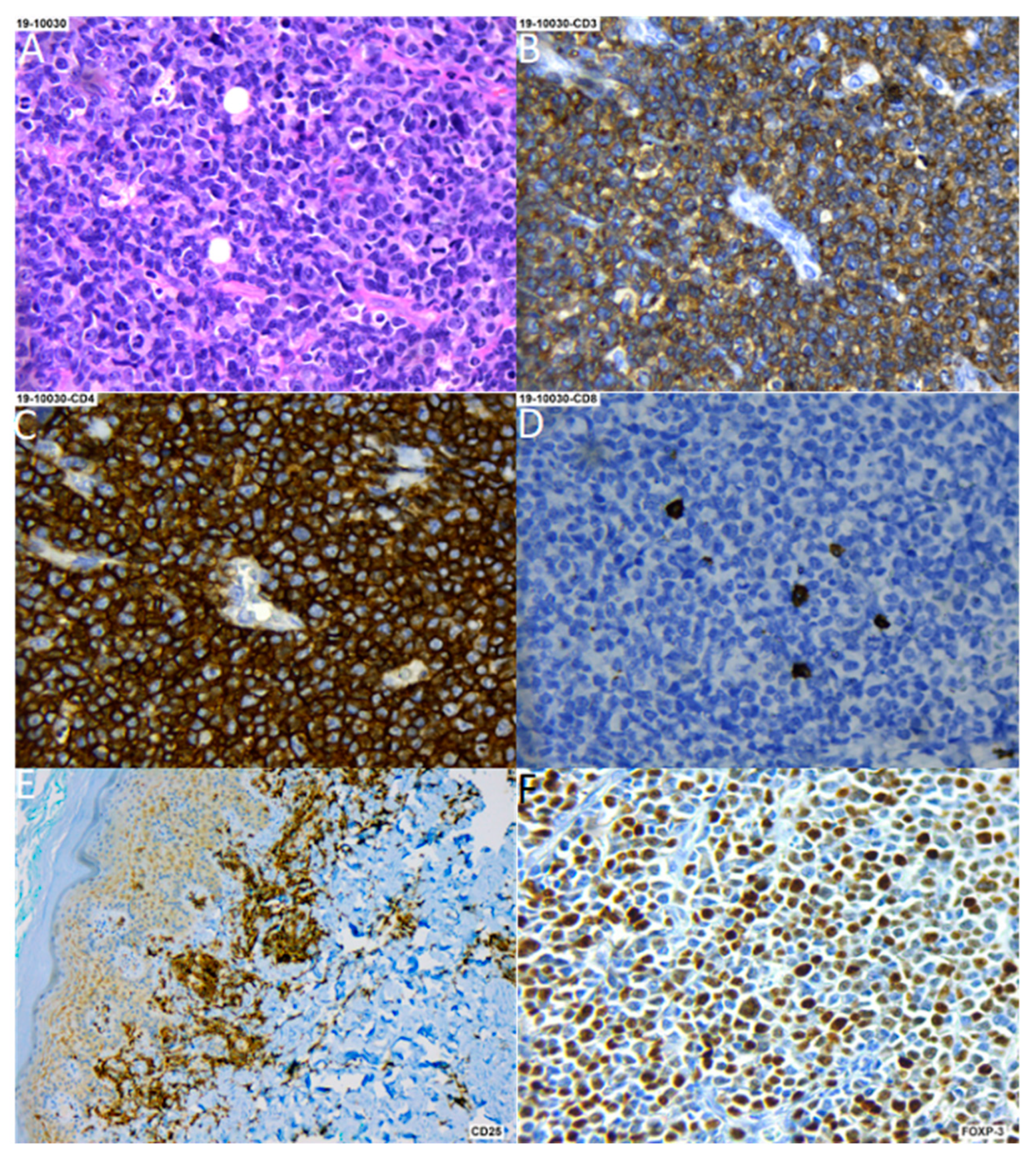{kind=link}
| Country (Ref) | Lymphoma Type | Type of Study | Methods | EBV Association | Description of the Study |
|---|---|---|---|---|---|
| Argentina [10,11,12] | DLBCL (ad/ped) | Cohort | ISH, IHC | 12.6% (12/95) | 26 DLBCL ped; 69 DLBCL ad from Buenos Aires, Argentina. EBV prevalence 72% ped. |
| Argentina [13] | PBL | Case report | ISH | 100% | 1 PBL in HIV+ patient from Buenos Aires, Argentina. |
| Argentina [14] | BL (ped) | Cohort | ISH, IHC | 29% IHC (7/24); 100% ISH (3/3) | 27 pediatric BL, 3 HIV+ from Buenos Aires, Argentina. |
| Argentina [15] | PBL | 4 cases | ISH, IHC | 100% (4/4) | 4 PBL in HIV+ patients from Buenos Aires, Argentina. |
| Argentina [16] | B-NHL (ped) | Cohort | ISH | 40% (16/40) (35% BL; 47% DLBCL) | 23 BL ped, 17 DLBCL ped from Buenos Aires, Argentina. |
| Argentina [17] | PBL | Case report | ISH | 100% | 1 PBL in HIV+ from Buenos Aires, Argentina. |
| Argentina [18] | PBL | Case report | ISH | 100% | 1 PBL in HIV+ from Buenos Aires, Argentina. |
| Argentina [19] | T-NHL (ped) | Cohort | ISH, IHC | 8% (2/25) | 16 lymphoblastic, 8 anaplastic, 1 hepatoesplenic T-cell lymphoma ped from Buenos Aires, Argentina. |
| Argentina/Brazil [20] | HL (ped) | Cohort | ISH, IHC | 54% (Arg; 60/111); 48% (Bra; 31/65) | 111 HL ped from Buenos Aires, Argentina. 65 HL ped from Rio de Janeiro, Brazil. |
| Argentina [21] | PCNSL | 7 cases | ISH, PCR | 100% (6/6) | 7 PCNSL cases HIV+ from Buenos Aires, Argentina. |
| Argentina [22] | HL (ad, ped) | Cohort | ISH | 55% ped (51/92); 31% ad (25/81) | 92 HL ped, 81 HL ad from Buenos Aires, Argentina. |
| Argentina [23] | HIV+ HL, BL, DLBCL | 4 cases | ISH, IHC | 100% (4/4) | 1 HL, 2 BL, 1 DLBCL ped HIV+ from Buenos Aires, Argentina. |
| Argentina [24] | BL (ped) | Cohort | ISH, PCR | 47% (8/17) | 17 BL ped from Buenos Aires, Argentina. |
| Argentina [25,26,27] | HL (ped) | Cohort | ISH | 51% (22/41) | 41 HL ped from Buenos Aires, Argentina. |
| Argentina [28] | BL (ped) | Cohort | ISH | 25% (4/16) | 16 BL ped from La Plata, Argentina. |
| Brazil [29] | DLBCL | Cohort | ISH | 30% (28/93) | 93 DLBCL ad from Sao Paulo, Brazil. |
| Brazil [30] | NT/NKL | Case report | IHC | 100% | 1 NK/NKL from Rio Janeiro, Brazil. |
| Brazil [31] | HVL-LD | Case report | ISH | 100% | 1 HVL- LD from Dom Eliseu City, Pará, Brazil. |
| Brazil [32] | HL (ad/ped, temporal series) | Cohort | ISH | 87–46% (817) | 155 HL ped, 662 HL ad from Sao Paulo, Brazil. |
| Brazil [33] | Intermediate BL with DLBCL | Case report | ISH | 100% | 1 int BL DLBCL from Recife, Brazil. |
| Brazil [34] | DLBCL (>50 yo) | Cohort | ISH | 8.45% (6/71) | 71 DLBCL ad from Sao Paulo, Brazil. |
| Brazil [35] | T/NKL | Case report | ISH | 100% | T/NKL HIV+ from Sao Paulo, Brazil. |
| Brazil [36] | BL (ped) | Cohort | ISH | 100% (7/7) | 4 BL ped, 3 BL ad from Amazonas, Brazil. |
| Brazil [37] | BL (ped) | Cohort | ISH | 54.1% (33/61) | 61 BL ped from Rio de Janeiro, Brazil. |
| Brazil [38] | HL (ad, ped) | Cohort | ISH | 43% (56/130) | 130 HL from Sao Paulo, Brazil. |
| Brazil [39] | HVL-LD | Case report | ISH | 100% | 1 HVL-LD from Manaus Amazonas, Brazil. |
| Brazil [40] | DLBCL, Palatine tonsil | Cohort | ISH | 0% (0/26) | 26 DLBCL from Bahia, Brazil. |
| Brazil [41,42,43] | HL (ped) | Cohort | ISH | 44.8% (43/96) | 96 HL ped from Rio de Janeiro, Brazil. |
| Brazil [44,45] | HL (ad) | Cohort | ISH | 52.6% (51/97) | 97 HL ad from Sao Paulo, Brazil. |
| Brazil [46] | ENKTCL (ad, ped) | Cohort | ISH, PCR | 100% (74/74) | 74 ENKTCL from Sao Paulo, Brazil. |
| Brazil [47] | HL (ad) | Cohort | ISH | 22% (5/23) | 23 HL ad from Sao Paulo, Brazil. |
| Brazil [48] | CNS DLBCL (ad) | Cohort | ISH | 5.5% total (2/36) (40% IS) | 36 CNS DLBCL from Sao Paulo, Brazil. |
| Brazil [49] | HL (stomach) | 5 cases | ISH | 80% (4/5) | 5 HL from Sao Paulo, Brazil. |
| Brazil [50] | B-NHL (ped) | Cohort | ISH, qPCR | 23% (7/30) | 30 NHL ped from Rio de Janeiro and Sao Paulo, Brazil. |
| Brazil [51] | HL + PTL | Case report | ISH | 100% | HL PTL from Sao Paulo, Brazil. |
| Brazil [52] | HL (ad, ped) | Cohort | ISH, IHC | 50.3% (85/169) | 169 HL from Sao Paulo, Brazil. |
| Brazil [53,54] | BL (ad, ped) | Cohort | ISH | 52.6 % (123/234) | North Region(n = 17 cases), Central West Region(n = 17 cases), Northeast Region(n = 86 cases), Southeast Region(n = 72 cases), South Region(n = 42 cases) |
| Brazil [55] | BL (ped) | Cohort | ISH | 66% (33/50) | 143 pediatricos y 88 adultos, 3 sin edad). |
| Brazil [56] | BL (ped) | Cohort | ISH | 61% (33/54) | San pablo |
| Brazil [57] | PBL | 11 cases | ISH, PCR | 100% (11/11) | Rio de janeiro |
| Brazil [58] | HL (ad, ped) | Cohort | ISH, IHC | 48% (22/46) | San pablo |
| Brazil [59] | PCNSL | 10 cases | IHC | 10% (1/10) | Florianopolis, South of Brazil |
| Brazil [60] | HL (ad) | Cohort | IHC, PCR | 37% (11/30); 43% Circulating EBV | 14 patients <15 years y 32 >15 years |
| Brazil [61] | HL (ped) | Cohort | ISH | 86.7% (78/90) | Niterói RJ |
| Brazil [62,63,64] | B-NHL (ped) | Cohort | ISH, PCR | 72% (21/29) | 29 NHL from Rio de Janeiro, Brazil. |
| Brazil [65] | HL (ad) | Cohort | ISH, IHC | 75.6% (28/37) | 37 HL ad from Ceara, Brazil. |
| Brazil [66] | HL (ad) | Cohort | IHC | 45.8% (38/83) | 83 HL ad from Rio de Janeiro, Brazil. |
| Brazil [67] | HL (ad, ped) | Cohort | IHC | 55% (35/64) | 64 HL ad from Rio de Janeiro, Brazil. |
| Brazil [68,69] | HL (ad) | Cohort | ISH, IHC | 64.1% (50/78) | 78 HL ad from Rio de Janeiro, Brazil. |
| Brazil [70] | HL (ad, ped) | Cohort | ISH | 63.5% (61/96) | 96 HL from Sao Paulo and Ceara, Brazil. |
| Brazil [71] | ENKTCL | Cohort | ISH | 100% (16/16) | 16 ENKTCL from Sao Paulo, Brazil. |
| Brazil [72] | BL (ped) | Cohort | ISH | 73% (8/11) | 11 BL ped from Recife, Brazil. |
| Brazil [73] | HL (ped) | Cohort | ISH | 57.7% (15/26) | 26 HL ped from Curitiba, Brazil. |
| Brazil [74] | BL (ped) | Cohort | ISH | 87% (47/54) | 54 BL ped from Bahia, Brazil. |
| Brazil [75] | BL | Cohort | ISH | 71% (17/24) | 24 BL from Sao Paulo, Brazil. |
| Brazil [76] | HL (ped) | Cohort | ISH | 72% (18/25) | 25 HL ped from Sao Paulo, Brazil. |
| Mexico [77] | HVL-LD | Cohort | ISH | 100% (20/20) | 20 HVL-LD ped from Mexico City, Mexico. |
| Mexico [78] | HL (ad, ped) | Cohort | ISH | 76.1% ped (22/42); 66.6% ad (16/24) | 42 HL ped, 24 HL ad from Mexico City, Mexico. |
| Mexico [79] | PCL | Case report | ISH | 100% | 1 PCL from Mexico City, Mexico. |
| Mexico [80] | PBL | 5 cases | PCR | 80% (4/5) | 5 PBL ad HIV+ from Mexico City, Mexico. |
| Mexico [81] | DLBCL (>50 yrs) | Cohort | ISH | 7% (9/136) | 136 DLBCL ad from Mexico City, Mexico. |
| Mexico [82] | HL (mostly ad) | Cohort | ISH, IHC | 61.4% (35/57) | 54 HL ad, 3 HL ped from Mexico City, Mexico. |
| Mexico [83] | ENKTCL | Cohort | ISH | 96% (22/23) | 23 ENKTCL from Mexico City, Mexico. |
| Mexico/Bolivia [84] | HVL-LD /ACTCLC | 4 cases | ISH | 75% (3/4) | 4 ACTCLC ped from Mexico City and La Paz |
| Mexico [85] | PTLD | 8 cases | ISH | 100% (8/8) | 8 PTLD ad from Mexico City, Mexico. |
| Mexico [86] | NHL, Intestinal | Cohort | ISH | 63% (12/19) | 7 T, 6 high grade B, 6 low grade B-NHLs from Mexico City, Mexico. |
| Mexico [87,88] | HL (ad) | Cohort | IHC | 70% (35/50) | 50 HL ad from Mexico City, Mexico. |
| Mexico [89] | HL (ad, ped) | Cohort | ISH, IHC | 67% (18/27) | 3 HL ped, 24 HL ad from Mexico City, Mexico. |
| PR [90] | HL & NHL (ad, ped) | Cohort | IHC | 50% HL (11/22); 35% NHL (22/63) | 22 HL, 63 NHL from San Juan de Puerto Rico, Puerto Rico. |
| DR [91] | HL (ped) | Cohort | IHC | 64.3% (18/28) | 28 HL ped from Santiago, Dominican Republic |
| Cuba [92] | BL (ped) | 7 cases | EBV Serology | 85.7% (6/7) | EBV prevalence in 7 BL ped from La Habana, Cuba. |
| Colombia [93,94] | HL (ad, ped) | Cohort | ISH, IHC | 67% (45/67) 60.4% ad; 84.2% ped | 48 HL ad, 19 HL ped from Bogotá, Colombia |
| Peru [95] | DLBCL (ad) | Cohort | ISH | 28% (33/117) | 117 DLBCL ad from Lima and Arequipa, Peru. |
| Peru [96] | LBCL in cardiac myxoma (ad) | Case report | ISH | 100% | LBCL ad from Lima, Peru. |
| Peru [97] | HVL-LD | 4 cases | ISH | 100% (3/3) | 4 HVL-LD ped from Lima, Peru. |
| Peru [98] | EBV+ DLBCL GI (ad) | 5 cases | ISH | 100% (5/5) | 5 DLBCL GI ad from Lima, Peru. |
| Peru [99] | Systemic T/NKL | 6 cases | ISH, IHC | 100% (6/6) | 6 T/NKL ped from Lima, Peru. |
| Peru [100,101] | EBV+ DLBCL (>50 yo) | Cohort | ISH | 14% (28/199) | 199 DLBCL ad from Lima, Peru. |
| Peru [102] | DLCBL in a HTLV-1+ | Case report | ISH | 100% | DLBCL ad from Lima, Peru. |
| Peru [103] | Cutaneous T/NKL (11/15 HVL-LD) | Cohort | ISH | 100% (15/15) | 12 T/NKL ped, 2 T/NKL ad from Lima, Peru. |
| Peru [104] | ENKTCL | Cohort | PCR | 99% (76/77) | 77 ENKTCL from Lima, Peru. |
| Peru [105] | HVL-LD | 6 cases | ISH | 100% (6/6) | 6 HVL-LD ped from Lima, Peru. |
| Peru [106] | ENKTCL | Cohort | ISH, IHC | 96% (27/28) | 28 ENKTCL ad from Lima, Peru. |
| Peru [107] | Nasal lymphoma | Cohort | ISH | 93% (14/13; 11/11 T-cell) | 13 Nasal lymphoma from Lima, Peru. |
| Peru [108] | HL (mostly ped) | Cohort | ISH, IHC | 94% (30/32) | 32 HL from Lima, Peru. |
| Ecuador [109] | HVL-LD | 2 cases | ISH | 100% | 1 HVL-LD ped, 1 HVL-LD ad from Quito, Ecuador. |
| Ecuador [110] | HL and NHL (ad) | Cohort | ISH, qPCR | 55.5% HL (5/9); 59.5% NHL (25/42) | 9 HL ad, 42 NHL ad from Guayaquil, Ecuador. |
| Chile [111] | EBV+ DLBCL | Case report | ISH | 100% (Leukocytoclastic vasculitis) | DLBCL from Santiago, Chile. |
| Chile [112] | Nasal lymphoma | Cohort | ISH | DLCBL 0% (0/3); T-cell 0% (0/1); NKT 100% (6/6) | 3 DLBCL, 1 T-cell lymphoma, 6 NKT from Valdivia, Chile. |
| Chile [113] | ENKTCL | Cohort | ISH | 78% (7/9) | 9 ENKTCL ad from Santiago, Chile. |
| Chile /Argentina /Brazil [114] | BL (mostly ped) | Cohort | ISH | 41% (7/17 Arg); 50% (5/10 Chile); 58% (7/12 Br) | 37 BL ped, 2 BL ad from Buenos Aires, Argentina; Santiago, Chile; Campinas, Brazil. |
| Honduras [115] | HL (ped) | Cohort | ISH | 100% (11/11) | 11 HL ped from Tegucigalpa, Honduras. |
| CR [116] | HL (ad, ped) | Cohort | IHC | 40% (16/40) | 6 HL ped, 34 HL ad from San Jose, Costa Rica. |
| CR [117] | HL (ped) | Cohort | ISH, IHC | 81% (34/42) | 42 HL from San José, Costa Rica. |
| CR/Mexico [118] | HL (ad, >15 yo) | Cohort | ISH, SB | 36% (5/14) CR; 77% (24/31) Mexico | 45 HL ad from Mexico City, Mexico; San Jose, Costa Rica. |
| Bolivia [119] | NHL | 8 cases | ISH | 75% (6/8) | 8 NHL from Santa Cruz, Bolivia. |
| Guatemala [120] | ENKTCL | Cohort | ISH | 87% (73/84) | 59 ENKTCL from Guatemala City, Guatemala. |
| Country (Ref) | Type of Study | Methods | Results | Description of the Study |
|---|---|---|---|---|
| Brazil [148] | Prevalence | EIA, IFA | 25.1% KSHV+ | Screening of blood donors from Sao Paolo, Salvador and Manaos (February–December 2003). n = 3493 |
| Brazil [150] | Prevalence | EIA, IFA | 31.3% KSHV+ | Screening of non-Amerindians blood donors from Mapuera and Manaos (Amazon). n = 1120 |
| Brazil [149] | Prevalence | IFA | 1.1% KSHV+ health care workers | Screening of health care workers (n = 757) and HIV/AIDS patients in Sao Paolo (1999–2008). |
| Brazil [147] | Prevalence | EIA, IFA | 4.6% KSHV+ | Screening of blood donors from Vitoria and Sao Paolo (January 1998–April 1999). n = 747 |
| Brazil [153] | Prevalence | EIA | 16.3% KSHV+ | Screening of 81 low-income families from Belem Para, derived from a previous rotavirus study. n = 467 |
| Brazil [145] | Prevalence | IFA | 4% KSHV+ | Screening of blood donors from Sao Paolo. n = 400 |
| Brazil [146] | Prevalence | IFA | 3.8% KSHV+ | Screening of blood donors from Sao Paolo (2000–2002). n = 319 |
| Brazil [152] | Prevalence | ISH | 6.83% KSHV+ | Screening of children (0–20 yo) from Campinas after removal of either/both tonsil or adenoids. n = 293 |
| Brazil [151] | Prevalence | IFA, WB | 9.35% KSHV+ | Screening of children (0–12 yo) from Rio de Janeiro. n = 171 |
| Brazil [154] | Case report | IFA | 40 yo female with UCD hyaline variety; 62 yo with MCD mixed hyaline and plasma cell. Patients died, because of progression to NHL | Description of 3 patients with CD of which two were KSHV+ |
| Brazil [155] | Case report | IHC, Histology | 41 yo male with KSHV+ MCD co-presented with KS. 35 yo male had no KSHV test | Description of two HIV/AIDS patients with MCD plasma cell variant |
| Brazil [156] | Case report | IHC | 32 yo male with MCD plasmablastic variant | Description of an HIV/AIDS patient with a history of KS in spite of controlled HIV load |
| Brazil [157] | Case report | IHC | 40 yo male with MCD plasmablastic variant | Description of an HIV/AIDS patient with MCD co-existing with KS |
| Brazil [158] | Case report | Histology | 37 yo male with MCD. No KSHV or HIV test | Description of a patient with MCD plasma cell variant |
| Brazil [159] | Case report | PCR | 44 yo male with PEL | Description of an HIV/AIDS patient |
| Brazil [160] | CSS | PCR | One (2%) bone marrow sample was KSHV+ | Screening of patients with multiple myeloma. n = 48 |
| Arg [146] | Prevalence | IFA | 3.6% KSHV+ | Screening of blood donors from Buenos Aires, Bahia Blanca and Cordoba (January 2000–December 2002). n = 1859 |
| Arg [161] | Prevalence | PCR | 6.6% KSHV+ | Screening of blood donors from Buenos Aires and San Salvador de Jujuy. n = 772 |
| Arg [162] | Prevalence | EIA | 7.8% KSHV+ | Screening of blood donors from Buenos Aires. n = 577 |
| Arg [163] | Prevalence | EIA | 6.4% KSHV+ | Screening of repository samples from a previous cervical cancer study from 9 countries. Concordia Argentina. n = 968 |
| Arg [164] | CSS | PCR | One KSHV+ | Description of DLBCLs in HIV+ patients. n = 11 |
| Arg [165] | Case report | IFA, PCR | 36 yo male with MCD hyaline vascular. 49 yo male MCD plasmablastic co-presenting with KS. | Report of two cases of KSHV+ MCD in HIV+ patients |
| Arg [13] | Case report | PCR | 34 yo male with DLBCL EBV+ and KSHV+ | Description of a DLBCL in an HIV/AIDS patient |
| Arg [166] | Case report | PCR | 72 yo male HIV- with KSHV+ PEL | Description of a PEL |
| Arg [167] | Research study | IFA, PCR, Seq | I MCD and 1 PEL are described | KSHV genotyping |
| Col [163] | Prevalence | EIA | 13.32% KSHV+ | Screening of repository samples from a previous cervical cancer study from 9 countries. n= 1883 from Colombia (Bogota City) |
| Chile [146] | Prevalence | IFA | 2.6% KSHV+ | Screening of blood donors from Santiago (2000–2002). n = 300 |
| Peru [168] | Prevalence | IFA | 56.2% KSHV+ | Screening of blood donors from one Hospital in Lima. n = 128 |
| Peru [169] | CSS | IHC | Two UCD hyaline variety are reported as KSHV+. One MCD plasma cell was KSHV negative. | Description of CD patients from two hospitals in Lima. n = 10 |
| Mex [170] | CSS | IHC | Only one neoplasm was a KSHV+ MCD | Description of CD patients from a Mexico City hospital (2000–2015). n = 39 |
| Mex [171] | CSS | Histology | 5 MCDs are found but no test for KSHV infection | Description of CD patients from a Mexico City hospital between 1996–2003. n = 11. |
| Mex [172] | CSS | Histology | 1 (4.8%) PEL | Analysis of malignant neoplasms in HIV+ patients from a Mexico City hospital (January 2005–July 2008). n = 21 |
| Mex [173] | Case report | IHC | 73 yo HIV- female. EBV- lymphoma | Description of CD coexisting with a DLBCL. |
| Mex [174] | Case report | IHC | 36 yo HIV+ male | Description of a KS coexisting with a plasmablastic lymphoma and previous history of CD. |
| PR [175] | CSS | Histology | 4.8% developed neoplasia, Lymphomas are reported but are not classified further | HIV+ patients from a Bayamon Institute. n = 3576 |
| Cuba [176] | Prevalence | IF, WB | 1.2% KSHV+ blood donors | Screening of blood donors (n = 171) and risk populations. |
| Cuba [177] | Research Study | PCR, Seq | 2 PEL patients are included. No association is found between specific KSHV strains and any disease. | Molecular classification of KSHV strains isolated from KS patients, lymph node lesions and contacts of KS patients. n = 90 |
| Cuba [178] | Prevalence | IF | 16.9% KSHV+ | Screening of archival samples from a previous oral cancer study. n = 379 |
| Cuba [179] | Case report | Histology | 4 cases hyaline-vascular histological variety and 1 case to plasmacellular variety. | Description of five cases of CD |
| CR [163] | Prevalence | EIA | 9.81% KSHV+ | Screening of repository samples from a previous cervical cancer study from 9 countries. n= 1008 from Costa Rica (Guanacaste province) |
| Country (Ref) | KSHV Prevalence Risk Groups | ||||
|---|---|---|---|---|---|
| HIV+ | FSW | Oral Cancer Patients | Close Contacts | MSM | |
| Cuba [176,187] | 20.8% n = 154 | 33.5% n = 191 | 46.1–72.7% X = 62.9% n = 35 | ||
| Brazil [149,150,188,189,190,191,192] | 13.9–52.6% X = 21.8% n = 2358 | 6.7% n = 90 | |||
| Honduras [193] | 31.8% n = 22 | 9.4% n = 96 | |||
| Colombia [180] | 8% n = 25 | ||||
| Peru [181] | 66.5% n = 197 | 26.7% n = 300 | |||
| Argentina [194] | 17.4% n = 144 | ||||
| Country | Type of Study | Methods | HTLV Association | Description of Study |
|---|---|---|---|---|
| (Ref) | (Main Finding) | |||
| Mexico [226] | Prevalence | PA, WB | 0.39% HTLV-1/2+ | Screening of blood donors from Monterrey. n = 1017 |
| Mexico [227] | Prevalence | EIA | 2.8% HTLV+ | Screening of emergency room patients from Mexico City. n = 909 |
| Mexico [228] | Prevalence | EIA, PA, WB | 0.3% HTLV+ healthy women | Screening of healthy women (n = 662) & cervical cancer patients from Yucatan. |
| Panama [229] | Prevalence | EIA | 5% HTLV+ | Screening sera from previous studies (meningitis and enterovirus). n = 754 |
| Panama [230] | Case report | EIA, WB | HTLV-1+ | Description of ATLL patient |
| Panama [231] | CSS | EIA, IFA, WB, RIPA | 7 cases HTLV+ | Analysis of hematologic malignancies. n = 136 |
| 3 cases confirmed ATLL | ||||
| Hond [232] | Prevalence | EIA, WB, PCR | 8.1% HTLV-1+ of non- mestizos | Screening of blood donors from 15 cities of the Atlantic coast (n = 2651) |
| 0.5% HTLV-1+ of mestizos | ||||
| Hond [233] | Prevalence | EIA, WB | 0.3% HTLV-1+ | Screening of healthy individuals from Tegucigalpa and San Pedro Sula. n = 899 |
| 1.1% HTLV-2+ | ||||
| Hond [234] | Case report | EIA | HTLV+ | Description of ATLL patient |
| Nicar [235] | Technical paper | EIA, WB, PCR | 0.24% HTLV-1+ | Test of a new assay in blood donors. n = 410 |
| Cuba [215] | Prevalence | EIA, WB, RIPA | 0.27% HTLV+ | Screening of blood donors. n = 2579 |
| Cuba [216] | Prevalence | EIA, WB | 0.99% HTLV-1+ blood donors | Screening of blood donors (n = 1409) & risk groups. |
| Cuba [214] | Prevalence | PA, EIA, IF, WB | 0.25% HTLV+ in blood donors | Screening of blood donors (n = 2429) & patients with hematological and non-hematological disorders from 13 provinces. |
| 0.72% in patients | ||||
| Cuba [178] | Prevalence | EIA | 4.2% HTLV-1+ | Screening of archival samples from a previous oral cancer study. n = 379 |
| Cuba [220] | CSS | EIA, WB, PCR | 5 ATLL reported | Hematological neoplasms in 2 sentinel centers from Havana & Matanzas, (1997–2006). n = 1281 |
| DR [218] | Prevalence | EIA, WB, RIPA, IFA | 2.5% HTLV+ low risk group 0% Children | Screening of low (n = 2552) and high risk populations. |
| PR [219] | Prevalence | Undisclosed | 0.25% HTLV+ | Database search of transfusion transmitted pathogens in blood donors. n = 400 |
| PR [217] | Prevalence | EIA, WB, RIPA | O.2% HTLV-1+ | Archival samples from a Dengue surveillance study & blood donors from Ponce. n = 1881 |
| 1% IVDU | ||||
| Venez [236] | Prevalence | EIA, WB, PCR | 0.2% HTLV+ | Screening of blood donors from Caracas. n = 23,413 |
| Venez [237] | Prevalence | EIA | 1% HTLV+ Caracas | Screening of healthy individuals. n = 769 |
| 13.7% in the Amazonas | ||||
| Venez [238] | Prevalence | EIA, WB | 0.58% HTLV+ | Screening of healthy individuals from an immunology clinic in Maracay City. n = 514 |
| Colom [239] | Prevalence | Undisclosed | 0.3 % HTLV+ | Databases search of Colombian blood banks (2001–2014). n = 5,105,159 |
| Colom [240] | Prevalence | EIA | 0.24% HTLV+ | Databases search of Cali blood banks (2008–2014). n = 77,117 |
| Colom [241] | Prevalence | PA, WB | 0.7% HTLV-1+ children | Screening of random subjects from Tumaco. n = 1077 |
| 5.3% 20 y & older | ||||
| 7.8% IVDU | ||||
| Colom [242] | Prevalence | EIA | 0.3% HTLV+ | Screening of blood donors from Bogota (1999–2004). n = 8913 |
| Colom [243] | Prevalence | EIA, WB | 0.176% HTLV+ | Databases search of Medellin blood banks (2014–2018). n = 52,159 |
| HTLV-1:HTLV-2 (3:1) | ||||
| Colom [244] | Prevalence | EIA, WB | 0.06% HTLV+ | Database search of one Medellin blood bank (2014–2015). n = 14,423 |
| HTLV-1:HTLV-2 (8:1) | ||||
| Colom [245] | CSS | EIA, RIA, WB | 4.3% HTLV+ lowland | Comparison between Coastal and high-altitude towns. n = 670 |
| 0.9% upland regions | ||||
| Colomb [246] | Case report | EIA | HTLV+ ATLL | HTLV+ ATLL co-presenting with a verrucous carcinoma |
| Colom [247] | Case Report | EIA, WB, PCR | Clinical presentation similar to ATLL from Japan | Description of six ATLL patients from Cali. |
| Colom [248] | Case Report | EIA, WB | HTLV-1+ ATLL | Description of two ATLL patients |
| Colom [249] | Case control | EIA, WB | 100% of TSP/HAM & ATLL cases were HTLV-1+ | Screening for auto-antibodies in TSP/HAM (n = 37) and ATLL (n = 10) patients. |
| Ecuador [250] | Prevalence | EIA, IF, WB | 3.5% HTLV+ | Screening of random subjects from the Esmeralda Province. n = 227 |
| Ecuador [251] | Prevalence | EIA, WB | 2.4% HTLV+ in Afro descendant, 0% in the Chachis | Screening of random subjects from the Esmeralda Province. n = 142 |
| Ecuador [252] | Prevalence | EIA, RIPA, WB | 0.42% HTLV-1+ in continental regions | Screening of healthy individuals (n = 744) and risk groups throughout Ecuador. |
| 1.57% in Galapagos Island | ||||
| Peru [253] | Prevalence | EIA, WB | 3.4% HTLV+ | Databases search of blood banks from Abancay (2010–2015). n = 2895 |
| Peru [254] | Prevalence | EIA, WB | 0.9% HTLV-1+ | Databases search of blood banks from Arequipa in 2005. n = 2732 |
| Peru [255] | Prevalence | EIA, WB | 0.3% HTLV-1+ | Screening of random subjects from 24 cities. n = 1535 |
| 0% HTLV-2 | ||||
| Peru [256] | Prevalence | EIA | 1.7% HTLV-1+ | Screening of pregnant women from Lima. n = 2492 |
| Peru [257] | Case report | Undisclosed | HTLV-1+ | Acute liver failure as presentation of ATLL. |
| Peru [258] | Case report | Undisclosed | HTLV-1+ | Co-presentation of ATLL and strongyloidiasis. |
| Peru [259] | Case report | WB | HTLV+ | Description of three ATLL patients. |
| Peru [260] | Case report | EIA, WB | 3/7 tumors EBV+ | Description of seven patients with DLBCL in HTLV-1 carriers. |
| HTLV provirus in tumor was not assessed | ||||
| Peru [261] | Case report | EIA HTLV-1 | HTLV-1+ | Description of two cases of ATLL and concomitant S. stercoralis. |
| Peru [262] | Case report | EIA, WB, IH | HTLV-1+ | Description of four patients with gastric ATLL |
| Peru [263] | Case Report | EIA, PCR | HTLV-1+ | Description of one ATLL patient |
| Chile [264] | Prevalence | EIA, IF, PCR | 0.12% HTLV+ | Databases search of blood banks from 12 Chilean regions (2011–2013). n = 694,016 |
| HTLV-1: HTLV-2 (7.3:1) | ||||
| Chile [265] | Prevalence | EIA, IF, PCR | 0.24% HTLV-1+ | Databases search of blood banks from Valdivia (May 2009–May 2010). n = 6237 |
| Female:Male (3:1) | ||||
| Chile [266] | CSS | EIA, SB, PCR | Clinical and laboratory features of HTLV-I+ ATLL | Description of ATLL patients from the Santiago area (1989–1998). n = 26 |
| Chile [267] | Case report | EIA, PA, PCR | Intestinal involvement and progression into a leukemic phase | Description of one ATLL patient |
| Chile [268] | Case report | EIA, SB, PCR | Clinical and laboratory features of HTLV-I+ ATLL | Description of nine ATLL patients |
| Chile [269] | Case report | EIA, WB | Provirus was not assessed | Description of an ATLL with Reed-Sternberg cells |
| Chile [270] | Case report | EIA, WB, SB | HTLV-1+ ATLL | Description of three ATLL patients co-presenting with TSP/HAM |
| Chile [271] | Case report | EIA, CSF, SB | HTLV-1+ ATLL | ATLL case preceded by TSP/HAM |
| Chile [272] | Case report | EIA, SB | HTLV-1+ ATLL | Chilean immigrant in Spain with ATLL |
| Chile [273] | CSS | PCR, RFLP | 18.2% HTLV+ (15 HTLV-1 & 1 HTLV-2) | Analysis of hematological malignancies from Valdivia. n = 88 |
| Chile [274] | CSS | Undisclosed | 23 neoplasia of T cells | Analysis of chronic LPD from one hospital in Santiago (1999–2001). n = 132 |
| 11 HTLV-1+ ATLL | ||||
| Chile [275] | Case report | WB | HTLV+ ATLL | ATLL case in an HIV+ patient |
| Parag [276] | Prevalence | PA, EIA, WB, RIPA | 0% HTLV+ healthy | Screening of healthy volunteers (n = 338) and risk groups. |
| Urug [277] | Prevalence | EIA | 0.13% HTLV+ | Data from the National Registry Report of blood banks, 2012–2014. n = 297,371 |
| Urug [278] | Prevalence | PA, IFA, WB, RIPA | 0.75% HTLV-1+ | Screening of blood donors (n = 266) and risk groups. |
| Urug [279] | Case report | Undisclosed | HTLV-1+ | ATLL of a Peruvian immigrant co-presenting with multiple parasitosis. |
| Arg [280] | Prevalence | PA, EIA, WB | 0.9% HTLV-1+ | Databases search of blood banks from Jujuy city. n = 14,228 |
| 0.04% HTLV-2+ | ||||
| Arg [281] | Prevalence | EIA, PA, IFA, WB | 0.05% HTLV-1+ | Databases search of blood banks from Buenos Aires. n = 12,891 |
| 0.03% HTLV-2+ | ||||
| Arg [282] | Prevalence | EIA, PA, WB, Phylogenetic study | 0.011% HTLV-1+ | Databases search of blood banks from Corrientes. n = 9422 |
| 0.021% HTLV-2+ 1 | ||||
| HTLV-1 Subtype A | ||||
| HTLV-2 Subtype B | ||||
| Arg [283] | Prevalence | EIA, PA | 0.11% HTLV+ | Database search of a blood bank from Cordoba. n = 20,210 |
| Arg [284] | CSS | EIA, PA, WB | 0.028% HTLV-1+ | Databases search of blood banks from 9 different provinces. n = 123,233 |
| 0,025% HTLV-2+ | ||||
| Arg [285] | Prevalence | PA, IF, WB, PCR | 0.19% HTLV-1/2+ | Databases search of blood banks from Buenos Aires. n = 2050 |
| Arg [286] | Prevalence | PA, WB | 0.06% HTLV-1+ | Databases search of blood banks from Buenos Aires. n = 12,846 |
| Arg [287] | Prevalence | PA, WB | 0.036% HTLV-1+ | Databases search of blood banks from Buenos Aires. n = 19,426 |
| 0.01% HTLV-2+ | ||||
| Arg [288] | Prevalence | PA, WB | 0.035% HTLV-1 | Databases search of blood banks from Buenos Aires. n = 28,897 |
| 0.007% HTLV-2 | ||||
| Arg [289] | Prevalence | PA, IF | 0.26% HTLV-1 | Databases search of blood banks from Cordoba. n = 5476 |
| Arg [290] | Prevalence | PA, IF, WB | 0% HTLV-1 | Databases search of blood banks from Santa Fe and Santiago del Estero. n = 1327 |
| Arg [291] | Prevalence | PA, EIA, WB, PCR | 0.033% HTLV-1+ | Databases search of blood banks from Buenos Aires. n = 76,246 |
| 0.013% HTLV-2+ | ||||
| Arg [292] | Prevalence | Undisclosed | 1.0% HTLV+ Jujuy | Databases search of blood banks from Northern and Center regions. n = 130,599 |
| 0.7% HTLV+ Salta | ||||
| 0.6% HTLV+ Formosa | ||||
| Arg [293] | Prevalence | PA, WB, PCR | 0.034% HTLV-1+ | Databases search of blood banks from Buenos Aires. n = 86,238 |
| 0.014% HTLV-2+ | ||||
| Arg [294] | Prevalence | PA, WB | 0.03% HTLV-1+ | Databases search of blood banks from Santa Fe. n = 9425 |
| 0.05% HTLV-2+ | ||||
| Arg [295] | Prevalence | EIA, PA, WB | 0.00072% HTLV+ | Databases search of blood banks from Misiones. n = 6912 |
| Arg [296] | Prevalence | EIA | 0.07% HTLV-1+ | Databases search of blood banks from Buenos Aires. n = 28,483 |
| 0.03% HTLV-2+ | ||||
| Arg [297] | Prevalence | EIA | 0.191% HTLV+ | Screening of pregnant women from Córdoba. n = 3143 |
| Arg [298] | Prevalence | PVT, IH, Proviral DNA integration | 5 cases HTLV-1+ from native American: ATLL | 34 cases of lymphoma resembling ATLL |
| Arg [299] | Case Report | Undisclosed | HTLV-1+ of Guinean origin | Association of B-cell lymphoma and T-cell lymphoma in HTLV-1 infection. |
| NHL B and one T without phenotype of ATLL | ||||
| Arg [300] | Case report | Undisclosed | HTLV-1+ | ATLL cases |
| 5 cases | ||||
| Arg [301] | 2 cases report | Undisclosed | HTLV-1+ | ATLL from 2 asymptomatic brothers |
| Brazil [302] | Prevalence | EIA, PCR | 0.1% HTLV+ | Databases search of blood banks from Riberao Preto, Sao Paulo. n = 301,400 |
| HTLV-1:2 (2:1) | ||||
| Brazil [303] | Prevalence | EIA, WB | 0.04% HTLV+ in South | Databases search of blood banks from 27 urban cities. n = 6,218,619 |
| 1% in Northeast | ||||
| Brazil [304] | Prevalence | EIA, WB, PCR | 1.76% HTLV-1+ Subtype A | Databases search of blood banks from Salvador. n = 1385 |
| Brazil [305] | Prevalence | EIA, WB | 0.08%-0.2% HTLV+ | Databases search of blood banks from Sao Paulo, Minas Gerais & Pernambuco. n = 281,760 |
| Brazil [306] | Prevalence | EIA | 0.63% HTLV+ | Databases search of blood banks from Southwest Bahia. n = 34,400 |
| Brazil [307] | Prevalence | EIA | 0.09% HTLV+ | Databases search of blood banks from Goiás. n = 137,209 |
| Brazil [308] | Prevalence | EIA | 0.77% HTLV-1+ | Databases search of blood banks from Salvador Bahia. n = 233,876 |
| 0.025% HTLV-2+ | ||||
| Brazil [309] | Prevalence | PCR | 1.4% HTLV-1 | Databases search of blood banks from Belém, Pará. n = 1059 |
| 0.5% HTLV-2 | ||||
| Brazil [310] | Prevalence | EIA, PCR | 0.059% HTLV-1+ | Databases search of blood banks from Piauí. n = 37,306 |
| 0.037% HTLV-2+ | ||||
| HTLV-1 subgroup A | ||||
| Brazil [311] | Prevalence | EIA, WB | 0.13% HTLV+ | Databases search of blood banks from Manaus. n = 87,402 |
| Brazil [312] | Prevalence | EIA | 0.58% HTLV+ | Databases search of blood banks from Marajó Island. n = 1899 |
| Brazil [313] | Prevalence | EIA | 1.48% HTLV-1+ | Databases search of blood banks from Salvador Bahía. n = 3451 |
| Brazil [314] | Prevalence | EIA | 0.019% HTLV-1+ | Databases search of blood banks from Fortaleza. n = 679,610 |
| 0.005% HTLV-2+ | ||||
| Brazil [315] | Prevalence | EIA | 0.1% HTLV+ | Databases search of blood banks from Minas Gerais. n = 3,249,944 |
| Brazil [316] | Prevalence | EIA | 0.02% HTLV+ | Databases search of blood banks from Uberata. n = 147,489 |
| Brazil [317] | Prevalence | EIA | 0.1% HTLV-1 | Databases search of blood banks from Belo Horizonte. n = 422,600 |
| 0.002% HTLV-2 | ||||
| Brazil [318] | CSS | EIA | 0.02% HTLV+ | Databases search of blood banks from Riberao Preto. n = 377,243 |
| Brazil [319] | Prevalence | EIA, WB | 0.15% HTLV+ | Databases search of blood banks from Maranhao. n = 365,564 |
| Brazil [320] | Prevalence | EIA, WB | 0.66% HTLV+ | Databases search of blood banks from Rio Branco. n = 11121 |
| Brazil [321] | Prevalence | EIA | 0.3% HTLV+ | Databases search of blood banks from Sao Paulo. n = 351,639 |
| Brazil [322] | Prevalence | EIA, WB | 0.17% HTLV+ | Databases search of blood banks from Sao Paulo. n = 17063 |
| Brazil [323] | CSS | Undisclosed | 83 ATLL (26 smoldering, 23 chronic, 16 acute, 13 lymphoma and five primary cutaneous) | ATLL treatment and response in Salvador, Bahia |
| Brazil [324] | CSS | EIA, WB, PCR, IH | HTLV-1+ | 52 cases ATLL from Salvador, Bahía. |
| Brazil [325] | Case report | EIA, WB, IH | HTLV-1 in CSF + ATLL | Simultaneous development of ATLL and HAM/TSP in a pediatric patient with IDH. |
| Brazil [326] | CSS | EIA, WB | HTLV+ ATLL | Prognostic Factors of 72 ATLL. |
| Brazil [327] | Case report | EIA, WB, Nested PCR | HTLV-1+ ATLL with monoclonal integration. | ATLL case |
| Brazil [328] | Case report | EIA, WB, PCR | HTLV-1+, four with p16 deletion, one with p53 mutation | 8 cases of pediatric ATLL patients |
| FC, Cytogenetic | ||||
| Brazil [329] | CSS | EIA WB, Nested PCR | HTLV-1+ found in 48 ATLL. | 188 patients with a T-cell disorder. 53 ATLL. Rio de Janeiro, Brazil |
| Brazil [330] | Cohort | EIA, PA, WB, Sequencing | HTLV-1+ found in 11 cases. | 14 cases of ATLL, Rio de Janeiro. |
| Brazil [331] | Case report | EIA | HTLV-1+ | Hodgkin-like ATLL from Salvador, Bahía. |
| Brazil [332] | Case report | EIA | HTLV-1+ | ATLL from Brasilia. |
| Brazil [333] | Case report | EIA | HTLV-1+ | ATLL with Hyalohyphomycosis |
| Brazil [334] | Case report | EIA | HTLV-2+ | Two HTLV-2+ ATLL cases in Maranhao, Northeast Brazil. |
| Brazil [335] | Case report | EIA | HTLV-1+ | ATLL in a patient with Strongyloides stercoralis. |
| Brazil [336] | Case report | EIA | HTLV-1+ | IDH progressing to ATL. |
| Brazil [337] | Case report | EIA | HTLV-1+ | Primary cutaneous type of ATLL. |
| Brazil [338] | Case report | EIA | HTLV-1+ | 2 ATLL cases from Minas Gerais. |
| Brazil [339] | Case report | EIA | HTLV-1+ | ATLL case. |
| Brazil [340] | CSS | EIA, WB, PCR | HTLV-1+ | 195 ATLL cases from Rio de Janeiro. |
| 9% also with HAM/TSP | ||||
| Brazil [341] | CSS | EIA, PCR | HTLV-1+ | 28 ATLL from Bahía. |
| Country (Ref) | HTLV Prevalence Risk Groups | |||||||
|---|---|---|---|---|---|---|---|---|
| HIV+ | STD | FSW | MSM | Cervical Cancer | IVDU | Blood Transfusion | Close Contacts | |
| Brazil [356,365,367,368,370,371,373,376,391,392,393,394,395,396,397,398,399,400,401,402,403,404,405,406,407,408] | 1.1–16.3% NT = 531/8154 (6.5%) n = 96 (H-1) n = 69 (H-2) | 0.5% NT = 2/395 n = 2 (H-1) | 1.4–3.2% NT = 31/1336 (2.3%) n = 30 (H-1) n = 1 (H-2) | 0.7–4.7% NT = 38/1871 (2%) n = 9 (H-1) | 11.7–35.2% NT = 165/854 (19.3%) n = 78 (H-1) n = 28 (H-2) | 7–10.2% NT = 41/422 (9.7%) n = 41 (H-1) | 21.2–35.1% NT = 159/517 (30.7%) n = 159 (H-1) | |
| Argentina [387,409,410,411,412,413,414,415,416,417,418] | 1.6–27.7% NT = 114/1158 (9.8%) n = 59 (H-1) n = 18 (H-2) | 1% NT = 4/400 | 1.5–1.6% NT = 17/1069 (1.6%) n = 6 (H-1) n = 1 (H-2) | 0.5–3% NT = 26/1216 (2.1%) n = 2 (H-1) | 1.5–33.6% NT = 149/1128 (13.2%) n = 69 (H-1) n = 47 (H-2) | 31.5% NT = 29/92 n = 29 (H-1) | ||
| Mexico [228,343,344,346,347,419,420,421,422] | 0–12.5% NT = 31/642 (4.8%) n = 4 (H-1) n = 24 (H-2) | 0–1.8% NT = 7/462 (1.5%) n = 0 (H-1) n = 5 (H-2) | 0–0.9% NT = 1/239 (0.4%) | 1.4–6.5% NT = 9/195 (4.6%) | 20.7% NT = 106 | 0–0.8% NT = 3/834 (0.36%) | ||
| DR [218,224] | 5.5% NT = 6/108 | 2.8% NT = 14/494 | 4.2% NT = 13/308 | 2–14.3% NT = 11/120 (9.2%) | ||||
| Cuba [216,423] | 0% NT = 0/268 | 1.7% NT = 25/1444 n = 25 (H-1) | 10% NT = 29/921 n = 29 (H-1) | |||||
| Venezuela [424] | 0% NT = 0/141 | 1% NT = 1/100 n = 1 (H-1) | ||||||
| Ecuador [252] | 0.6% NT = 1/159 n = 1 (H-1) | 1.4% NT = 2/141 n = 2 (H-1) | ||||||
| CR [348] | 0.7% NT = 3/436 n = 3 (H-1) | |||||||
| Colombia [241] | 7.8% NT = 13/167 n = 13 (H-1) | |||||||
| Peru [425] | 9.5% NT = 184/1938 n = 184 (H-1) | |||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chabay, P.; Lens, D.; Hassan, R.; Rodríguez Pinilla, S.M.; Valvert Gamboa, F.; Rivera, I.; Huamán Garaicoa, F.; Ranuncolo, S.M.; Barrionuevo, C.; Morales Sánchez, A.; et al. Lymphotropic Viruses EBV, KSHV and HTLV in Latin America: Epidemiology and Associated Malignancies. A Literature-Based Study by the RIAL-CYTED. Cancers 2020, 12, 2166. https://doi.org/10.3390/cancers12082166
Chabay P, Lens D, Hassan R, Rodríguez Pinilla SM, Valvert Gamboa F, Rivera I, Huamán Garaicoa F, Ranuncolo SM, Barrionuevo C, Morales Sánchez A, et al. Lymphotropic Viruses EBV, KSHV and HTLV in Latin America: Epidemiology and Associated Malignancies. A Literature-Based Study by the RIAL-CYTED. Cancers. 2020; 12(8):2166. https://doi.org/10.3390/cancers12082166
Chicago/Turabian StyleChabay, Paola, Daniela Lens, Rocio Hassan, Socorro María Rodríguez Pinilla, Fabiola Valvert Gamboa, Iris Rivera, Fuad Huamán Garaicoa, Stella Maris Ranuncolo, Carlos Barrionuevo, Abigail Morales Sánchez, and et al. 2020. "Lymphotropic Viruses EBV, KSHV and HTLV in Latin America: Epidemiology and Associated Malignancies. A Literature-Based Study by the RIAL-CYTED" Cancers 12, no. 8: 2166. https://doi.org/10.3390/cancers12082166