
A Growth Modulation Index-Based GEISTRA Score as a New Prognostic Tool for Trabectedin Efficacy in Patients with Advanced Soft Tissue Sarcomas: A Spanish Group for Sarcoma Research (GEIS) Retrospective Study

 , , , , , , and add
Show full author list
, , , , , , and add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Database and Objectives
2.2. Patients and Treatments
2.3. GEISTRA Score Design
2.4. Statistical Methods
3. Results
3.1. Characteristics of Patients and Treatments
3.2. Response to Treatment and Survival Analysis
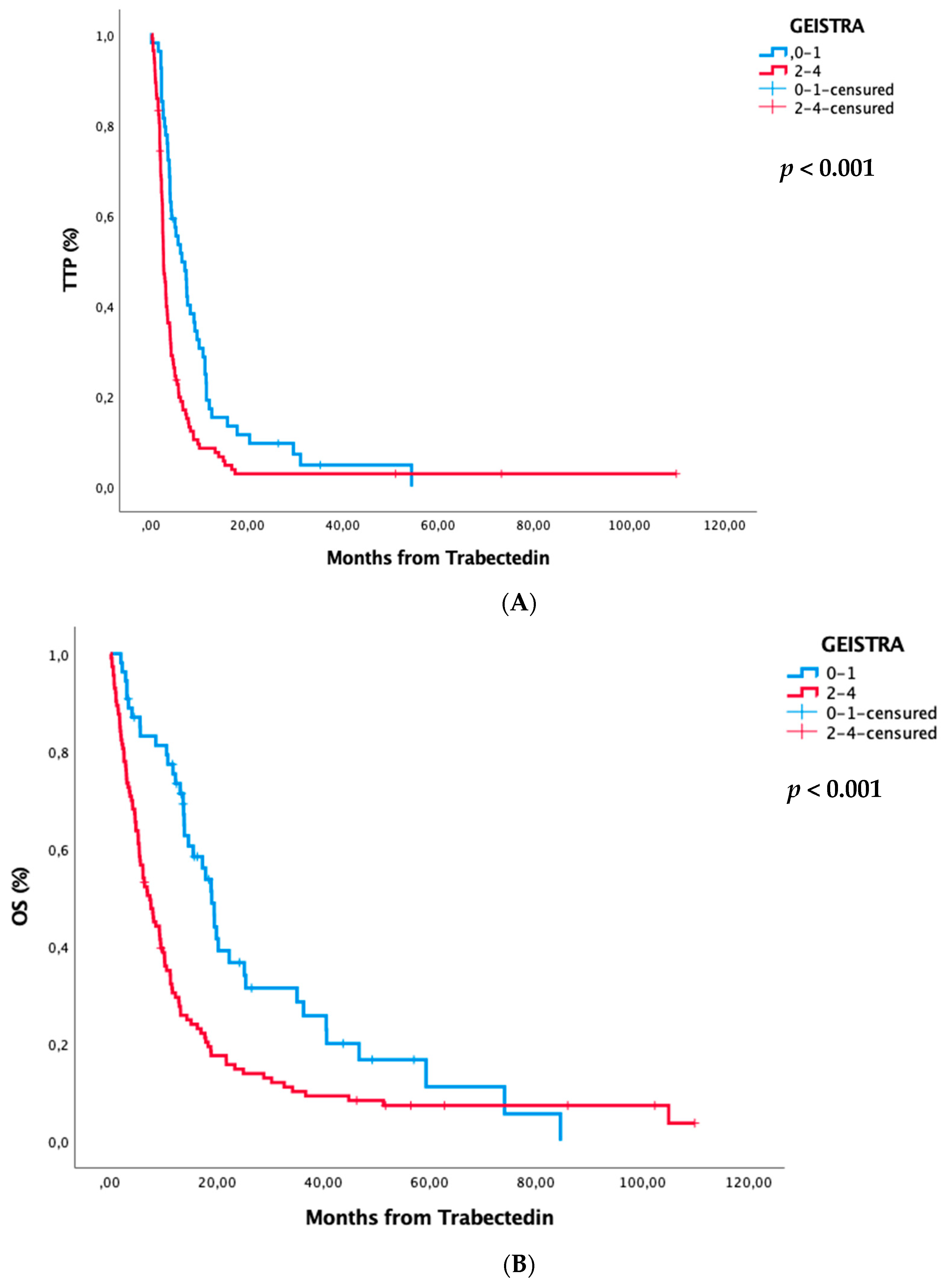
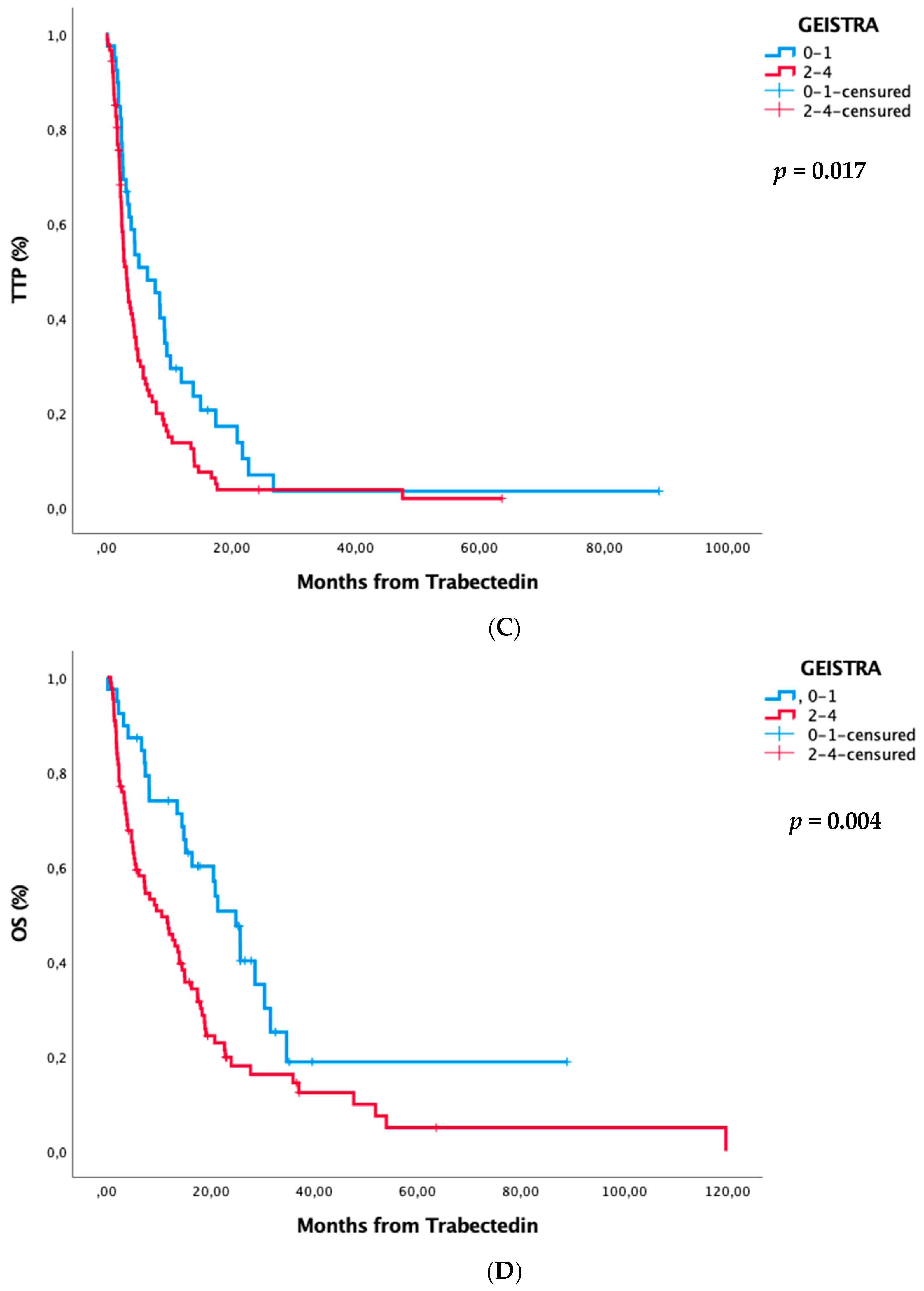
3.3. GEISTRA Score
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fletcher, C.; Bridge, J.; Antonescu, C.; Mertens, F. WHO Classification of Tumours: Soft Tissue and Bone Tumours (WHO Classification of Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2020; Volume 3. [Google Scholar]
- Judson, I.; Verweij, J.; Gelderblom, H.; Hartmann, J.T.; Schöffski, P.; Blay, J.-Y.; Kerst, J.M.; Sufliarsky, J.; Whelan, J.; Hohenberger, P.; et al. Doxorubicin Alone versus Intensified Doxorubicin Plus Ifosfamide for First-Line Treatment of Advanced or Metastatic Soft-Tissue Sarcoma: A Randomised Controlled Phase 3 Trial. Lancet Oncol. 2014, 15, 415–423. [Google Scholar] [CrossRef]
- Ryan, C.W.; Merimsky, O.; Agulnik, M.; Blay, J.-Y.; Schuetze, S.M.; Van Tine, B.A.; Jones, R.L.; Elias, A.D.; Choy, E.; Alcindor, T.; et al. PICASSO III: A Phase III, Placebo-Controlled Study of Doxorubicin with or Without Palifosfamide in Patients With Metastatic Soft Tissue Sarcoma. J. Clin. Oncol. 2016, 34, 3898–3905. [Google Scholar] [CrossRef]
- Casali, P.; Abecassis, N.; Aro, H.; Bauer, S.; Biagini, R.; Bielack, S.; Bonvalot, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brodowicz, T.; et al. Corrections to “Soft Tissue and Visceral Sarcomas: Esmo–Euracan Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up”. Ann. Oncol. 2018, 29, iv268–iv269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dossi, R.; Frapolli, R.; Di Giandomenico, S.; Paracchini, L.; Bozzi, F.; Brich, S.; Castiglioni, V.; Borsotti, P.; Belotti, D.; Uboldi, S.; et al. Antiangiogenic Activity of Trabectedin in Myxoid Liposarcoma: Involvement of Host TIMP-1 and TIMP-2 and Tumor Throm-Bospondin-1. Int. J. Cancer 2014, 136, 721–729. [Google Scholar] [CrossRef] [PubMed]
- Incalci, M.D.; Badri, N.; Galmarini, C.M.; Allavena, P. Trabectedin, a Drug Acting on Both Cancer Cells and the Tumour Microenvironment. Br. J. Cancer 2014, 111, 646–650. [Google Scholar] [CrossRef] [Green Version]
- D’Incalci, M.; Erba, E.; Damia, G.; Galliera, E.; Carrassa, L.; Marchini, S.; Mantovani, R.; Tognon, G.; Fruscio, R.; Jimeno, J.; et al. Unique Features of the Mode of Action of ET-743. Oncology 2002, 7, 210–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, A.K.; Galmarini, C.M.; D’Incalci, M. Unique Features of Trabectedin Mechanism of Action. Cancer Chemother. Pharmacol. 2016, 77, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Demetri, G.D.; Chawla, S.; Von Mehren, M.; Ritch, P.; Baker, L.H.; Blay, J.Y.; Hande, K.R.; Keohan, M.L.; Samuels, B.L.; Schuetze, S.; et al. Efficacy and Safety of Trabectedin in Patients with Advanced or Metastatic Liposarcoma or Leiomyosarcoma After Failure of Prior Anthracyclines and Ifosfamide: Results of a Randomized Phase II Study of Two Different Schedules. J. Clin. Oncol. 2009, 27, 4188–4196. [Google Scholar] [CrossRef] [PubMed]
- Demetri, G.D.; Von Mehren, M.; Jones, R.L.; Hensley, M.L.; Schuetze, S.M.; Staddon, A.P.; Milhem, M.; Elias, A.; Ganjoo, K.N.; Tawbi, H.; et al. Efficacy and Safety of Trabectedin or Dacarbazine for Metastatic Liposarcoma or Leiomyosarcoma After Failure of Conventional Chemotherapy: Results of a Phase III Randomized Multicenter Clinical Trial. J. Clin. Oncol. 2016, 34, 786–793. [Google Scholar] [CrossRef]
- Cousin, S.; Taieb, S.; Penel, N. A Paradigm Shift in Tumour Response Evaluation of Targeted Therapy. Curr. Opin. Oncol. 2012, 24, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Von Hoff, D.D. There Are No Bad Anticancer Agents, Only Bad Clinical Trial De-signs--Twenty-First Richard and Hinda Rosenthal Foundation Award Lecture. Clinical Cancer Research. Off. J. Am. Assoc. Cancer Res. 1998, 4, 1079–1086. [Google Scholar]
- Cousin, S.; Blay, J.Y.; Bertucci, F.; Isambert, N.; Italiano, A.; Bompas, E.; Ray-Coquard, I.; Perrot, D.; Chaix, M.; Bui-Nguyen, B.; et al. Correlation between Overall Survival and Growth Modulation Index in Pre-treated Sarcoma Patients: A Study from the French Sarcoma Group. Ann. Oncol. 2013, 24, 2681–2685. [Google Scholar] [CrossRef]
- Penel, N.; Demetri, G.D.; Blay, J.Y.; Cousin, S.; Maki, R.G.; Chawla, S.P.; Judson, I.; Von Mehren, M.; Schöffski, P.; Verweij, J.; et al. Growth Modulation Index as Metric of Clinical Benefit Assessment among Advanced Soft Tissue Sarcoma Patients Receiving Tra-Bectedin as a Salvage Therapy. Ann. Oncol. 2012, 24, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Buonadonna, A.; Benson, C.; Casanova, J.; Kasper, B.; Pousa, A.L.; Mazzeo, F.; Brodowicz, T.; Penel, N. A Noninterventional, Multicenter, Prospective Phase IV Study of Trabectedin in Patients with Advanced Soft Tissue Sarcoma. Anti-Cancer Drugs 2017, 28, 1157–1165. [Google Scholar] [CrossRef]
- Martinez-Trufero, J.; Hindi, N.; Cruz, J.; Alvarez Alvarez, R.M.; Diaz Beveridge, R.P.; Valverde Morales, C.M.; Gutierrez, A.; Pajares Bernad, I.; Lopez-Pousa, A.; Vaz Salgado, M.A.; et al. Correlation between a New Growth Modulation Index (GMI)-Based Geistra Score and Efficacy Outcomes in Patients (PTS) with Advanced Soft Tissue Sar-Comas (ASTS) Treated with Trabectedin (T): A Spanish Group for Research on Sarcomas (GEIS-38 Study). J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 11070. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Verschoor, A.J.; Litière, S.; Marréaud, S.; Judson, I.; Toulmonde, M.; Wardelmann, E.; Van Der Graaf, W.; Le Cesne, A.; Gronchi, A.; Gelderblom, H. Prognostic Relevance of Distant Metastases versus Locally Advanced Disease in Soft Tissue Sarcomas: An EORTC-STBSG Database Study. Eur. J. Cancer 2018, 94, 187–198. [Google Scholar] [CrossRef] [Green Version]
- Van Glabbeke, M.; Verweij, J.; Judson, I.; Nielsen, O. Progression-Free Rate as the Principal End-Point for Phase II Trials in Soft-Tissue Sarcomas. Eur. J. Cancer 2002, 38, 543–549. [Google Scholar] [CrossRef]
- Endo, M.; Takahashi, S.; Araki, N.; Sugiura, H.; Ueda, T.; Yonemoto, T.; Takahashi, M.; Morioka, H.; Hiraga, H.; Hiruma, T.; et al. Time Lapse Analysis of Tumor Response in Patients with Soft Tissue Sarcoma Treated with Trabectedin: A Pooled Analysis of Two Phase II Clinical Trials. Cancer Med. 2020, 9, 3656–3667. [Google Scholar] [CrossRef] [Green Version]
- Le Cesne, A.; Blay, J.Y.; Judson, I.; Van Oosterom, A.; Verweij, J.; Radford, J.; Lorigan, P.; Rodenhuis, S.; Ray-Coquard, I.; Bonvalot, S.; et al. Phase II Study of ET-743 in Advanced Soft Tissue Sarcomas: A European Organisation for the Research and Treatment of Cancer (EORTC) Soft Tissue and Bone Sarcoma Group Trial. J. Clin. Oncol. 2005, 23, 576–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Sanctis, R.; Marrari, A.; Marchetti, S.; Mussi, C.; Balzarini, L.; Lutman, F.R.; Daolio, P.; Bastoni, S.; Bertuzzi, A.F.; Quagliuolo, V.; et al. Efficacy of Trabectedin in Advanced Soft Tissue Sarcoma: Beyond Lipo-and Leiomyosarcoma. Drug Des. Dev. Ther. 2015, 9, 5785–5791. [Google Scholar] [CrossRef] [Green Version]
- Kawai, A.; Araki, N.; Sugiura, H.; Ueda, T.; Yonemoto, T.; Takahashi, M.; Morioka, H.; Hiraga, H.; Hiruma, T.; Kunisada, T.; et al. Trabectedin Monotherapy after Standard Chemotherapy versus Best Supportive Care in Patients with Advanced, Transloca-Tion-Related Sarcoma: A Randomised, Open-Label, Phase 2 Study. Lancet Oncol. 2015, 16, 406–416. [Google Scholar] [CrossRef]
- Grosso, F.; Jones, R.L.; Demetri, G.D.; Judson, I.; Blay, J.-Y.; Le Cesne, A.; Sanfilippo, R.; Casieri, P.; Collini, P.; Dileo, P.; et al. Efficacy of Trabectedin (Ecteinascidin-743) in Advanced Pretreated Myxoid Liposarcomas: A Retrospective Study. Lancet Oncol. 2007, 8, 595–602. [Google Scholar] [CrossRef]
- Penel, N.; Glabbeke, M.V.; Mathoulin-Pelissier, S.; Judson, I.; Sleijfer, S.; Bui, B.; Schoffski, P.; Ouali, M.; Marreaud, S.; Brouste, V.; et al. Performance Status Is the Most Powerful Risk Factor for Early Death among Patients with Advanced Soft Tissue Sarcoma. Br. J. Cancer 2011, 104, 1544–1550. [Google Scholar] [CrossRef]
- Leahy, M.; Del Muro, X.G.; Reichardt, P.; Judson, I.; Staddon, A.; Verweij, J.; Baffoe-Bonnie, A.; Jönsson, L.; Musayev, A.; Justo, N.; et al. Chemotherapy Treatment Patterns and Clinical Outcomes in Patients with Metastatic Soft Tissue Sarcoma. the Sarcoma Treat-Ment and Burden of Illness in North America and Europe (SABINE) Study. Ann. Oncol. 2012, 23, 2763–2770. [Google Scholar] [CrossRef] [PubMed]
- Samuels, B.L.; Chawla, S.; Patel, S.; Von Mehren, M.; Hamm, J.; Kaiser, P.E.; Schuetze, S.; Li, J.; Aymes, A.; Demetri, G.D. Clinical Outcomes and Safety with Trabectedin Therapy in Patients with Advanced Soft Tissue Sarcomas Following Failure of Prior Chemotherapy: Results of a Worldwide Expanded Access Program Study. Ann. Oncol. 2013, 24, 1703–1709. [Google Scholar] [CrossRef] [PubMed]
- Le Cesne, A.; Ray-Coquard, I.; Duffaud, F.; Chevreau, C.; Penel, N.; Bui-Nguyen, B.; Piperno-Neumann, S.; Delcambre-Lair, C.; Rios, M.; Chaigneau, L.; et al. Trabectedin in Patients with Advanced Soft Tissue Sarcoma: A Retrospective National Analysis of the French Sarcoma Group. Eur. J. Cancer 2015, 51, 742–750. [Google Scholar] [CrossRef] [PubMed]
- De Nonneville, A.; Barbolosi, D.; Andriantsoa, M.; El-Cheikh, R.; Duffaud, F.; Bertucci, F.; Salas, S. Validation of Neutrophil Count as An Algorithm-Based Predictive Factor of Progression-Free Survival in Patients with Metastatic Soft Tissue Sarcomas Treated with Trabectedin. Cancers 2019, 11, 432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, H.; Iwata, S.; Wakamatsu, T.; Hayakawa, K.; Yonemoto, T.; Wasa, J.; Oka, H.; Ueda, T.; Tanaka, S. Efficacy and Safety of Trabectedin for Patients with Unresectable and Relapsed Soft-Tissue Sarcoma in Japan: A Japanese Musculoskeletal Oncology Group Study. Cancer 2020, 126, 1253–1263. [Google Scholar] [CrossRef]
- Maretty-Kongstad, K.; Aggerholm-Pedersen, N.; Keller, J.; Safwat, A. A Validated Prognostic Biomarker Score for Adult Patients with Nonmetastatic Soft Tissue Sarcomas of the Trunk and Extremities. Transl. Oncol. 2017, 10, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Tsuda, Y.; Ogura, K.; Kobayashi, E.; Hiruma, T.; Iwata, S.; Asano, N.; Kawai, A.; Chuman, H.; Ishii, T.; Morioka, H.; et al. Impact of Geriatric Factors on Surgical and Prognostic Outcomes in Elderly Patients with Soft-Tissue Sarcoma. Jpn. J. Clin. Oncol. 2017, 47, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Blay, J.-Y.; Casali, P.G.; Nieto, A.; Tanović, A.; Le Cesne, A. Efficacy and Safety of Trabectedin as an Early Treatment for Advanced or Metastatic Liposarcoma and Leiomyosarcoma. Futur. Oncol. 2014, 10, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Martin-Broto, J.; Pousa, A.L.; Peñas, R.D.L.; Del Muro, X.G.; Gutierrez, A.; Martinez-Trufero, J.; Cruz, J.; Alvarez, R.; Cubedo, R.; Redondo, A.; et al. Randomized Phase II Study of Trabectedin and Doxorubicin Compared with Doxorubicin Alone as First-Line Treatment in Patients With Advanced Soft Tissue Sarcomas: A Spanish Group for Research on Sarcoma Study. J. Clin. Oncol. 2016, 34, 2294–2302. [Google Scholar] [CrossRef] [PubMed]
- Italiano, A.; Laurand, A.; Laroche, A.; Casali, P.; Sanfilippo, R.; Le Cesne, A.; Judson, I.; Blay, J.-Y.; Ray-Coquard, I.; Bui, B.; et al. ERCC5/XPG, ERCC1, and BRCA1 Gene Status and Clinical Benefit of Trabectedin in Patients with Soft Tissue Sarcoma. Cancer 2011, 117, 3445–3456. [Google Scholar] [CrossRef]
- Schöffski, P.; Taron, M.; Jimeno, J.; Grosso, F.; Sanfilipio, R.; Casali, P.; Le Cesne, A.; Jones, R.; Blay, J.-Y.; Poveda, A.; et al. Predictive Impact of DNA Repair Functionality on Clinical Outcome of Advanced Sarcoma Patients Treated with Trabectedin: A Retrospective Multicentric Study. Eur. J. Cancer 2011, 47, 1006–1012. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients Characteristics | Whole Series (n = 357) n (%) | Training Cohort n = 191 | Validation Cohort n = 166 | p | |
|---|---|---|---|---|---|
| Age (Years) | Median (range): 50 (14–79) | 50 (14–78) | 51 (14–79) | 0.094 | |
| Sex | Men | 169 (47.3) | 98 (51.3) | 70 (42.2) | 0.11 |
| Women | 188 (52.7) | 93 (48.7) | 95 (57.6) | ||
| Histology | L-sarcoma | 193 (54.1) | 96 (50.3) | 97 (58.4) | 0.14 |
| Leiomyosarcoma | 113 (31.7)) | 57 (29.8) | 56 (33.7) | 0.49 | |
| Liposarcoma | 80 (22.4) | 39 (20.4) | 41 (24.7) | 0.37 | |
| Non-L-sarcoma | 164 (45.9) | 95 (49.7) | 69 (41.6) | 0.14 | |
| UPS | 37 (10.4) | 27 (14.1) | 10 (6) | 0.014 | |
| Other | 127 (35.6) | 68 (35.6) | 59 (35.5) | 1 | |
| TR-sarcoma | 92 (25.7) | 50 (26.2) | 42 (25.3) | 0.904 | |
| Non-TR-sarcoma | 265 (74.2) | 141 (73.8) | 124 (74.7) | ||
| FNCLCC tumor grade a | 1 | 44 (12.3) | 23 (12) | 21 (12.7) | 0.47 |
| 2 | 89 (24.9) | 43 (22.5) | 46 (27.7) | ||
| 3 | 187 (52.4) | 105 (55) | 82 (49.4) | ||
| Missing | 37 (10.4) | 20 (10.5) | 17 (10.2) | ||
| Prior chemotherapy lines for advanced disease | 0–1 | 154 (43.1) | 75 (39.3) | 79 (47.6) | 0.24 |
| 2 | 135 (37.8) | 79 (41.3) | 56 (33.7) | ||
| ≥3 | 68 (19.0) | 37 (19.4) | 31 (18.7) | ||
| Prior anthracycline administration setting | Adjuvant treatment | 133 (37.3) | 60 (31.4) | 73 (44) | 0.016 |
| First-line for advanced disease | 224 (62.7) | 131 (68.6) | 93 (56) | ||
| Stage at initial diagnosis | Nonmetastatic | 276 (77.3) | 146 (76.4) | 130 (78.3) | 0.52 |
| Metastatic disease | 78 (21.8) | 45 (23.6) | 33 (19.9) | ||
| Missing | 3 (0.8) | 0 (0) | 3 (1.8) | ||
| Metastasis-free interval (months) | Median (range) | 10.4 (0–177.2) | 10.1 (0–174.5) | 10.4 (0–177.2) | 0.32 |
| Karnofsky performance status | 0–80 | 199 (55.7) | 142 (55.3) | 57 (58.8) | 0.39 |
| >80 | 153 (42.8) | 115 (44.7) | 38 (39.2) | ||
| Missing | 5 (1.4) | 3 (1.2) | 2 (2.1) | ||
| Univariate Analysis HR (95% CI) | Multivariate Analysis HR (95% CI) | |||||||
|---|---|---|---|---|---|---|---|---|
| Prognostic Factor | Median TTP | p-Value | Median OS | p-Value | TTP | p-Value | OS | p-Value |
Metastasis-free interval (months)
| 0.001 | 0.002 | <0.001 | 0.01 | ||||
| 2.8 (2.3–3.2) | 8 (5.7–10.2) | 1.6 (1.2–2.0) | 1.4 (1.1–1.9) | |||||
| 4.1 (2.8–5.4) | 14.7 (12–17.3) | |||||||
Metastatic at diagnosis
| 0.047 | 0.022 | 0.67 | 0.51 | ||||
| 3.5 (2.9–4) | 11.7 (9.2–14.1) | 0.9 (0.6–1.3) | 1.1 (0.8–1.7) | |||||
| 4.4 (1.9–6.9) | 18 (9–27) | |||||||
Age (years)
| 0.16 | 0.081 | ||||||
| 3.7 (2.7–4.6) | 13.5 (10.1–16.9) | |||||||
| 3.5 (2.8–4.1) | 11.3 (8.5–14.1) | |||||||
Sex
| 0.5 | 0.098 | ||||||
| 3.7 (3.1–4.4) | 10.2 (7.7–12.7) | |||||||
| 3.5 (2.6–4.5) | 13.9 (11.3–16.4) | |||||||
Karnofsky PS
| <0.001 | <0.001 | <0.001 | <0.001 | ||||
| 5.9 (4–7.7) | 19.5 (16.8–22.2) | |||||||
| 2.7 (2.3–3) | 7.4 (5.4–9.4) | 1.6 (1.2–2.1) | 1.9 (1.5–2.5) | |||||
FNCLCC tumor grade a
| <0.001 | <0.001 | 0.015 | 0.027 | ||||
| 7.6 (5.4–9.8) | 25.7 (13.8–37.6) | |||||||
| 3.7 (2.2–5.2) | 15.2 (10.9–19.4) | |||||||
| 3 (2.5–3.5) | 8.9 (6.1–11.6) | 1.4 (1.1–1.8) | 1.4 (1.0–1.8) | |||||
Histology
| <0.001 | <0.001 | <0.001 | <0.001 | ||||
| 5.1 (3.8–6.4) | 17.9 (14.3–21.5) | |||||||
| 2.8 (2.3–3.3) | 7.3 (5.6–9) | 1.9 (1.5–2.4) | 1.8 (1.4–2.3) | |||||
| 5.1 (3.8–6.4) | <0.001 | 17.9 (14.3–21.5) | <0.001 | ||||
| 2.2 (1.6–3) | 3.7 (2.5–4.9) | |||||||
| 3.1 (2.6–3.6) | 8 (6.2–9.8) | |||||||
| 4.0 (3.0–3.9) | 0.1 | 13.9 (8.4–19.3) | 0.293 | ||||
| 3.3 (2.7–3.8) | 11.6 (9.3–13.8) | |||||||
Previous response
| 0.33 | 0.087 | ||||||
| 3 (2.4–3.5) | 10.6 (8–13.2) | |||||||
| 4.6 (3–6.1) | 17 (12–22) | |||||||
| 3.4 (3–4) | 9.9 (5.9–13.8) | |||||||
Previous anthracycline b
| 0.15 | 1 | ||||||
| 3.8 (2.7–4.8) | 13.1 (8.9–17.3) | |||||||
| 3.4 (2.8–3.9) | 11.8 (9.3–14.2) | |||||||
Previous gemcitabine b
| 0.091 | 0.83 | ||||||
| 3.4 (2.9–3.9) | 12.2 (9.3–15.2) | |||||||
| 3.8 (2.9–4.7) | 12 (9.4–14.6) | |||||||
Previous chemotherapy line for advanced disease
| 0.12 | 0.48 | ||||||
| 3.8 (2.8–4.8) | 12.2 (8.8–15.7) | |||||||
| 3.8 (3.1–4.5) | 13.1 (10.8–15.5) | |||||||
| 3.3 (2.5–4) | 9.2 (5.4–13.1) | |||||||
| Outcome Endpoints | GMI 0–1.33 | GMI > 1.33 | p-Value |
|---|---|---|---|
Response to trabectedin
| <0.001 | ||
| 7 (6.4%) | 14 (20.5%) | ||
| 21 (19.1%) | 39 (57.4%) | ||
| 82 (74.5%) | 15 (22.1%) | ||
| Median OS from trabectedin (95% CI) | 6.4 (4–8.9) | 25.2 (14–36.4) | <0.001 |
| Median OS from initial diagnosis (95% CI) | 34.8 (30.2–39.4) | 64.6 (51.1–78.1) | <0.001 |
| Median OS from metastatic disease (95% CI) | 23 (17.3–28.6) | 32.7 (27.8–37.7) | <0.001 |
| Median TTP trabectedin (95% CI) | 2.3 (2–2.6) | 8.2 (6.2–10.1) | <0.001 |
| Prognostic Factors | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| GMI 0–1.33 | GMI > 1.33 | p-Value | Odds Ratio (95% CI) | p-Value | |
Metastasis-free interval (months)
| 0.003 | 0.01 | |||
| 52 (46%) | 13 (22%) | ||||
| 62 (54%) | 46 (78%) | 2.81 (1.29–6.16) | |||
Metastatic at diagnosis
| 0.013 | ||||
| 36 (29%) | 9 (13%) | ||||
| 87 (71%) | 59 (87%) | ||||
Age (years)
| 1 | ||||
| 64 (52%) | 35 (51%) | ||||
| 59 (48%) | 33 (48%) | ||||
Sex
| 0.37 | ||||
| 60 (49%) | 38 (56%) | ||||
| 63 (51%) | 30 (44%) | ||||
Karnofsky PS
| 0.039 | 0.044 | |||
| 73 (61%) | 29 (43%) | ||||
| 47 (39%) | 39 (57%) | 2.14 (1.02–4.5) | |||
FNCLCC tumor grade a
| 0.55 | ||||
| 13 (12%) | 10 (16%) | ||||
| 30 (27%) | 13 (21%) | ||||
| 67 (61%) | 38 (62%) | ||||
Histology
| 0.023 | 0.031 | |||
| 54 (44%) | 42 (62%) | 2.26 (1.08–4.74) | |||
| 69 (56%) | 26 (38%) | ||||
Histology
| 0.032 | ||||
| 54 (44%) | 42 (62%) | ||||
| 22 (18%) | 5 (7%) | ||||
| 47 (38%) | 21 (31%) | ||||
Histology
| 0.458 | ||||
| 61(25%) | 31(26.3%) | ||||
| 178(75%) | 87(73.7%) | ||||
Previous best response
| <0.001 | ||||
| 32 (26%) | 5 (8%) | ||||
| 34 (28%) | 11 (17%) | ||||
| 55 (45%) | 49 (75%) | ||||
Previous best response
| <0.001 | <0.001 | |||
| 66 (54%) | 16 (25%) | ||||
| 55 (45%) | 49 (75%) | 4.96 (2.24–10.97) | |||
Previous anthracycline
| 0.26 | ||||
| 35 (28%) | 25 (37%) | ||||
| 88 (71%) | 43 (63%) | ||||
Gemcitabine
| 0.54 | ||||
| 54 (44%) | 26 (38%) | ||||
| 69 (56%) | 42 (62%) | ||||
Number of prior lines for advanced disease
| 0.022 | ||||
| 41 (33%) | 34 (50%) | ||||
| 52 (42%) | 27 (40%) | ||||
| 30 (24%) | 7 (10%) | ||||
| Training Cohort | Validation Cohort | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| TTP | OS | TTP | OS | ||||||
| GEISTRA Staging Group | GEISTRA Score | mTTP (95% CI) | p-Value | mOS (95% CI) | p-Value | mTTP (95% CI) | p-Value | mOS (95% CI) | p-Value |
| 0 | 0–1 | 6.4 (3.8–8.9) | <0.001 | 19 (16.4–21.7) | <0.001 | 6.5 (1.7–11.3) | 0.017 | 24.9 (18.4–31.3) | 0.004 |
| 1 | 2–4 | 2.5 (2–3) | 7.4 (5.7–9.2) | 3.1 (2.3–3.9) | 10.5 (5.3–15.7) | ||||
| Whole series | 3.4 (2.8–4) | 11.2 (8.9–13.5) | 3.4 (2.8–4) | 11.2 (8.9–13.5) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Trufero, J.; De Sande-González, L.M.; Luna, P.; Martin-Broto, J.; Álvarez, R.; Marquina, G.; Diaz-Beveridge, R.; Poveda, A.; Cano, J.M.; Cruz-Jurado, J.; et al. A Growth Modulation Index-Based GEISTRA Score as a New Prognostic Tool for Trabectedin Efficacy in Patients with Advanced Soft Tissue Sarcomas: A Spanish Group for Sarcoma Research (GEIS) Retrospective Study. Cancers 2021, 13, 792. https://doi.org/10.3390/cancers13040792
Martínez-Trufero J, De Sande-González LM, Luna P, Martin-Broto J, Álvarez R, Marquina G, Diaz-Beveridge R, Poveda A, Cano JM, Cruz-Jurado J, et al. A Growth Modulation Index-Based GEISTRA Score as a New Prognostic Tool for Trabectedin Efficacy in Patients with Advanced Soft Tissue Sarcomas: A Spanish Group for Sarcoma Research (GEIS) Retrospective Study. Cancers. 2021; 13(4):792. https://doi.org/10.3390/cancers13040792
Chicago/Turabian StyleMartínez-Trufero, Javier, Luis Miguel De Sande-González, Pablo Luna, Javier Martin-Broto, Rosa Álvarez, Gloria Marquina, Roberto Diaz-Beveridge, Andrés Poveda, Juana María Cano, Josefina Cruz-Jurado, and et al. 2021. "A Growth Modulation Index-Based GEISTRA Score as a New Prognostic Tool for Trabectedin Efficacy in Patients with Advanced Soft Tissue Sarcomas: A Spanish Group for Sarcoma Research (GEIS) Retrospective Study" Cancers 13, no. 4: 792. https://doi.org/10.3390/cancers13040792