Value of Serum NEUROG1 Methylation for the Detection of Advanced Adenomas and Colorectal Cancer

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
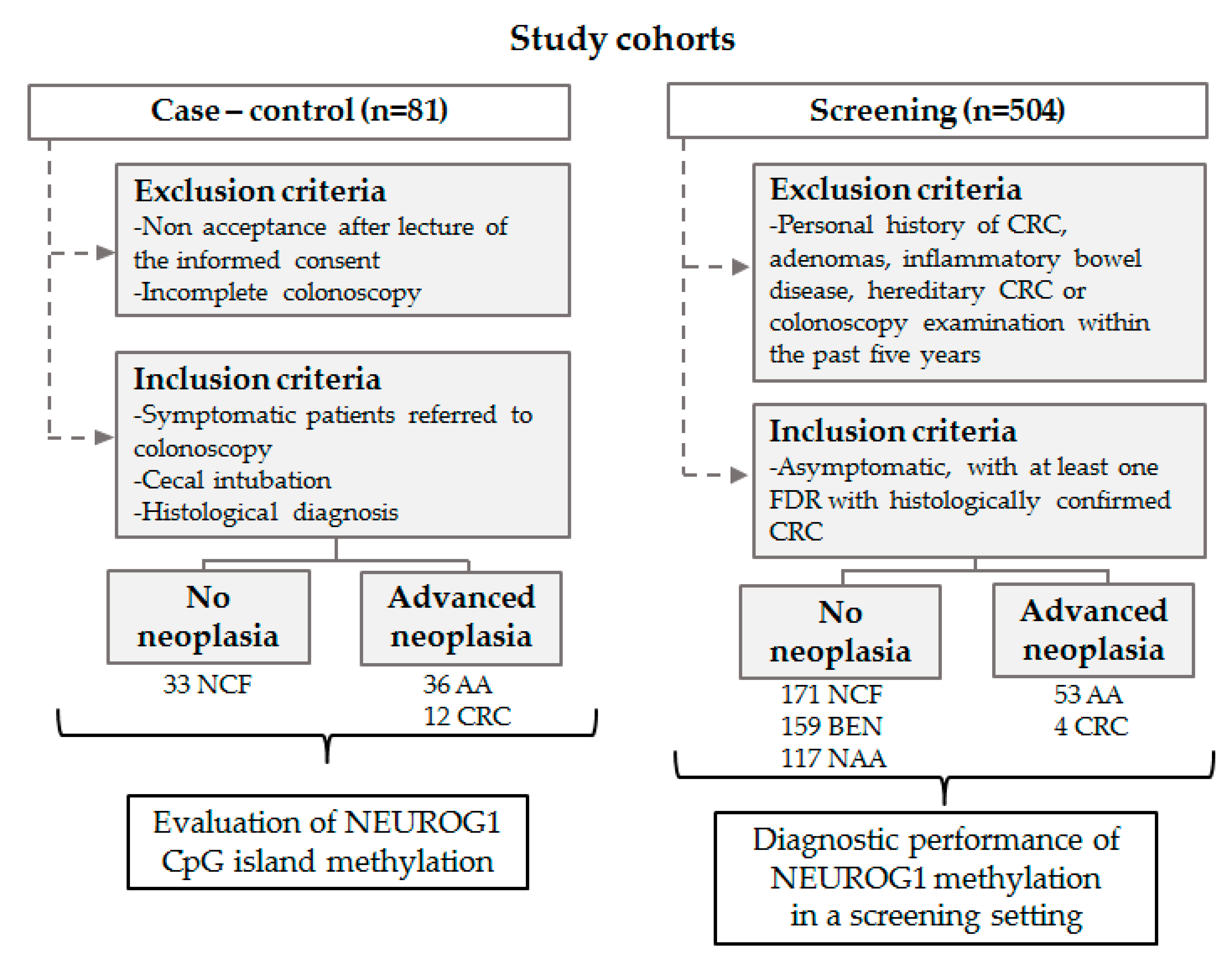
2.1. Study Population and Study Design
2.2. Blood Samples and Stool Samples
2.3. DNA Extraction and Sodium Bisulfite Modification
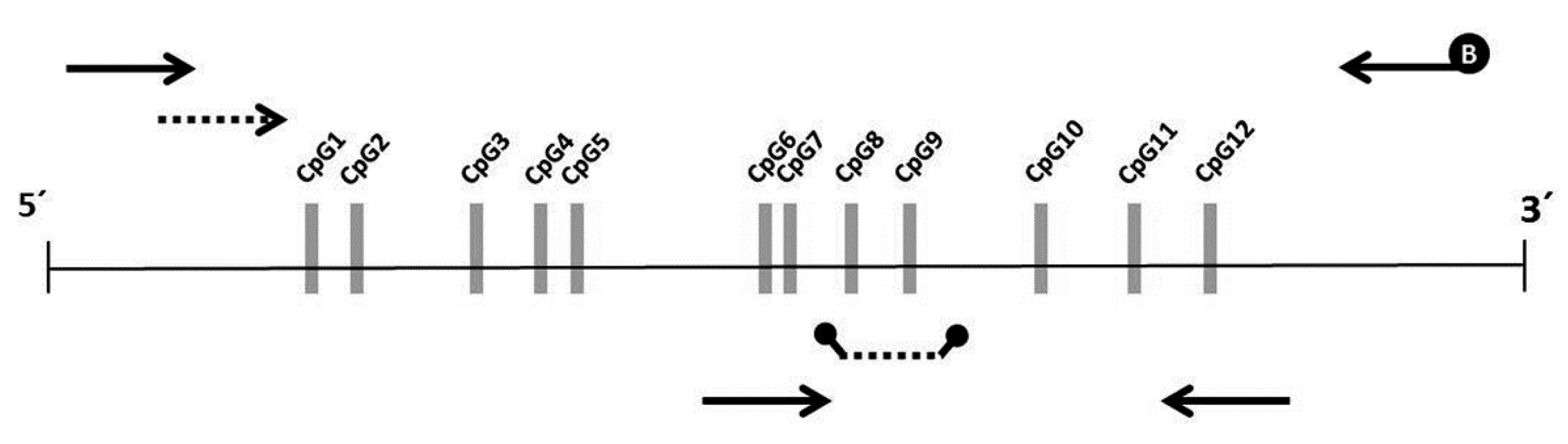
2.4. Bisulfite Pyrosequencing
2.5. Nested Methylation-Specific qPCR
2.6. Statistical Analysis
3. Results
3.1. Selection of CpG Sites in Serum NEUROG1 in the Case-Control Cohort
3.2. Methylation Analysis of Serum NEUROG1 in the Screening Cohort
3.3. Diagnostic Performance of Serum NEUROG1 Methylation for the Detection of Advanced Neoplasia and Advanced Adenomas
3.4. Evaluation of a Diagnostic Model Including Serum NEUROG1 Methylation and FIT
4. Discussion
5. Patents
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AA | Advanced Adenomas |
| AN | Advanced Neoplasia |
| AUC | Area Under the Curve |
| CRC | Colorectal Cancer |
| CIMP | CpG island methylator phenotype |
| Cq | Quantification Cycle |
| FIT | Fecal Immunochemical Test |
| FDR | First-Degree Relative |
| IQR | Interquartile Range |
| MS-qPCR | Methylation-Specific qPCR |
| NMP | Normalized Methylation Percentage |
| ROC | Receiver-Operating Characteristic |
References
- Arnold, M.; Abnet, C.C.; Neale, R.E.; Vignat, J.; Giovannucci, E.L.; McGlynn, K.A.; Bray, F. Global Burden of 5 Major Types Of Gastrointestinal Cancer. Gastroenterology 2020. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Stock, C.; Hoffmeister, M. Colorectal cancer screening: The time to act is now. BMC Med. 2015, 13, 262–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rösch, T.; Altenhofen, L.; Kretschmann, J.; Hagen, B.; Brenner, H.; Pox, C.; Schmiegel, W.; Theilmeier, A.; Aschenbeck, J.; Tannapfel, A.; et al. Risk of Malignancy in Adenomas Detected During Screening Colonoscopy. Clin. Gastroenterol. Hepatol. 2018, 16, 1754–1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samadder, N.J.; Smith, K.R.; Hanson, H.; Pimentel, R.; Wong, J.; Boucher, K.; Ahnen, D.; Singh, H.; Ulrich, C.M.; Burt, R.W.; et al. Increased risk of colorectal cancer among family members of all ages, regardless of age of index case at diagnosis. Clin. Gastroenterol. Hepatol. 2015, 13, 2305–2311. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Kharazmi, E.; Brenner, H.; Xu, X.; Sundquist, K.; Sundquist, J.; Fallah, M. Calculating Starting Age for Screening in Relatives of Patients With Colorectal Cancer Based on Data From Large Nationwide Datasets. Gastroenterology 2020. [Google Scholar] [CrossRef] [PubMed]
- Castro, I.; Cubiella, J.; Rivera, C.; González-Mao, C.; Vega, P.; Soto, S.; Hernandez, V.; Iglesias, F.; Teresa Alves, M.; Bujanda, L.; et al. Fecal immunochemical test accuracy in familial risk colorectal cancer screening. Int. J. Cancer 2014, 134, 367–375. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.S.; Piper, M.A.; Perdue, L.A.; Rutter, C.M.; Webber, E.M.; O’Connor, E.; Smith, N.; Whitlock, E.P. Screening for colorectal cancer: Updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 2016, 315, 2576–2594. [Google Scholar] [CrossRef] [Green Version]
- Imperiale, T.F.; Gruber, R.N.; Stump, T.E.; Emmett, T.W.; Monahan, P.O. Performance Characteristics of Fecal Immunochemical Tests for Colorectal Cancer and Advanced Adenomatous Polyps: A Systematic Review and Meta-analysis. Ann. Intern. Med. 2019, 170, 319–329. [Google Scholar] [CrossRef] [Green Version]
- Barnert, J.; Messmann, H. Diagnosis and management of lower gastrointestinal bleeding. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 637–646. [Google Scholar] [CrossRef]
- Zorzi, M.; Hassan, C.; Capodaglio, G.; Narne, E.; Turrin, A.; Baracco, M.; Dal Cin, A.; Fiore, A.; Martin, G.; Repici, A.; et al. Divergent long-term detection rates of proximal and distal advanced neoplasia in fecal immunochemical test screening programs: A retrospective cohort study. Ann. Intern. Med. 2018, 169, 602–609. [Google Scholar] [CrossRef]
- Curtin, K.; Slattery, M.L.; Samowitz, W.S. CpG island methylation in colorectal cancer: Past, present and future. Pathol. Res. Int. 2011, 2011, 902674. [Google Scholar] [CrossRef] [Green Version]
- Advani, S.M.; Advani, P.; DeSantis, S.M.; Brown, D.; VonVille, H.M.; Lam, M.; Loree, J.M.; Mehrvarz Sarshekeh, A.; Bressler, J.; Lopez, D.S.; et al. Clinical, Pathological, and Molecular Characteristics of CpG Island Methylator Phenotype in Colorectal Cancer: A Systematic Review and Meta-analysis. Transl. Oncol. 2018, 11, 1188–1201. [Google Scholar] [CrossRef] [PubMed]
- Weisenberger, D.J.; Siegmund, K.D.; Campan, M.; Young, J.; Long, T.I.; Faasse, M.A.; Kang, G.H.; Widschwendter, M.; Weener, D.; Buchanan, D.; et al. CpG island methylator phenotype underlies sporadic microsatellite instability and is tightly associated with BRAF mutation in colorectal cancer. Nat. Genet. 2006, 38, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Ogino, S.; Cantor, M.; Kawasaki, T.; Brahmandam, M.; Kirkner, G.J.; Weisenberger, D.J.; Campan, M.; Laird, P.W.; Loda, M.; Fuchs, C.S. CpG island methylator phenotype (CIMP) of colorectal cancer is best characterised by quantitative DNA methylation analysis and prospective cohort studies. Gut 2006, 55, 1000–1006. [Google Scholar] [CrossRef] [PubMed]
- Kaneda, A.; Yagi, K. Two groups of DNA methylation markers to classify colorectal cancer into three epigenotypes. Cancer Sci. 2011, 102, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.E.; Arends, M.J.; Silva, A.L.; Wyllie, A.H.; Greger, L.; Ito, Y.; Vowler, S.L.; Huang, T.H.-M.; Tavaré, S.; Murrell, A.; et al. Sequential DNA methylation changes are associated with DNMT3B overexpression in colorectal neoplastic progression. Gut 2011, 60, 499–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, Y.; Zumwalt, T.J.; Goel, A. DNA methylation patterns as noninvasive biomarkers and targets of epigenetic therapies in colorectal cancer. Epigenomics 2016, 8, 685–703. [Google Scholar] [CrossRef] [Green Version]
- Krishnamurthy, N.; Spencer, E.; Torkamani, A.; Torkamani, A.; Nicholson, L. Liquid biopsies for cancer: Coming to a patient near you. J. Clin. Med. 2017, 6, 3. [Google Scholar] [CrossRef] [Green Version]
- Herbst, A.; Rahmig, K.; Stieber, P.; Philipp, A.; Jung, A.; Ofner, A.; Crispin, A.; Neumann, J.; Lamerz, R.; Kolligs, F.T. Methylation of NEUROG1 in serum is a sensitive marker for the detection of early colorectal cancer. Am. J. Gastroenterol. 2011, 106, 1110–1118. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Worm Ørntoft, M.B. Review of Blood-Based Colorectal Cancer Screening: How Far Are Circulating Cell-Free DNA Methylation Markers From Clinical Implementation? Clin. Colorectal Cancer 2018, 17, e415–e433. [Google Scholar] [CrossRef]
- Jung, G.; Hernández-Illán, E.; Moreira, L.; Balaguer, F.; Goel, A. Epigenetics of colorectal cancer: Biomarker and therapeutic potential. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 111–130. [Google Scholar] [CrossRef] [PubMed]
- Philipp, A.B.; Nagel, D.; Stieber, P.; Lamerz, R.; Thalhammer, I.; Herbst, A.; Kolligs, F.T. Circulating cell-free methylated DNA and lactate dehydrogenase release in colorectal cancer. BMC Cancer 2014, 14, 245. [Google Scholar] [CrossRef] [Green Version]
- Wagner, P.D.; Srivastava, S. New paradigms in translational science research in cancer biomarkers. Transl. Res. 2012, 159, 343–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindholm, C.R.; Anderson, J.C.; Srivastava, A. The dark side of the colon: Current issues surrounding the significance, prevalence, detection, diagnosis and management of serrated polyps. Curr. Opin. Gastroenterol. 2019, 35, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Church, T.R.; Wandell, M.; Lofton-Day, C.; Mongin, S.J.; Burger, M.; Payne, S.R.; Castaños-Vélez, E.; Blumenstein, B.A.; Rösch, T.; Osborn, N.; et al. Prospective evaluation of methylated SEPT9 in plasma for detection of asymptomatic colorectal cancer. Gut 2014, 63, 317–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, J.; Hu, B.; Gui, Y.C.; Tan, Z.B.; Xu, J.W. Diagnostic Value and Clinical Significance of Methylated SEPT9 for Colorectal Cancer: A Meta-Analysis. Med. Sci. Monit. 2019, 25, 5813–5822. [Google Scholar] [CrossRef]
- Hariharan, R.; Jenkins, M. Utility of the methylated SEPT9 test for the early detection of colorectal cancer: A systematic review and meta-analysis of diagnostic test accuracy. BMJ Open Gastroenterol. 2020, 7, e000355. [Google Scholar] [CrossRef]
- Cubiella, J.; Digby, J.; Rodríguez-Alonso, L.; Vega, P.; Salve, M.; Díaz-Ondina, M.; Strachan, J.A.; Mowat, C.; McDonald, P.J.; Carey, F.A.; et al. The fecal hemoglobin concentration, age and sex test score: Development and external validation of a simple prediction tool for colorectal cancer detection in symptomatic patients. Int. J. Cancer 2017, 140, 2201–2211. [Google Scholar] [CrossRef] [Green Version]
- He, X.X.; Yuan, S.Y.; Li, W.B.; Yang, H.; Ji, W.; Wang, Z.Q.; Hao, J.Y.; Chen, C.; Chen, W.Q.; Gao, Y.Z.; et al. Improvement of Asia-Pacific colorectal screening score and evaluation of its use combined with fecal immunochemical test. BMC Gastroenterol. 2019, 19, 226. [Google Scholar] [CrossRef] [Green Version]
- Johnson, D.A.; Barclay, R.L.; Mergener, K.; Weiss, G.; König, T.; Beck, J.; Potter, N.T. Plasma Septin9 versus fecal immunochemical testing for colorectal cancer screening: A prospective multicenter study. PLoS ONE 2014, 9, e98238. [Google Scholar] [CrossRef]
- Jin, P.; Kang, Q.; Wang, X.; Yang, L.; Yu, Y.; Li, N.; He, Y.; Han, X.; Hang, J.; Zhang, J.; et al. Performance of a second-generation methylated SEPT9 test in detecting colorectal neoplasm. J. Gastroenterol. Hepatol. 2015, 30, 830–833. [Google Scholar] [CrossRef] [PubMed]
- Symonds, E.L.; Pedersen, S.K.; Baker, R.T.; Murray, D.H.; Gaur, S.; Cole, S.R.; Gopalsamy, G.; Mangira, D.; LaPointe, L.C.; Graeme, P. A blood test for methylated BCAT1 and IKZF1 vs. a fecal immunochemical test for detection of colorectal neoplasia. Clin. Transl. Gastroenterol. 2016, 7, e137. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.K.; Symonds, E.L.; Baker, R.T.; Murray, D.H.; McEvoy, A.; Van Doorn, S.C.; Mundt, M.W.; Cole, S.R.; Gopalsamy, G.; Mangira, D.; et al. Evaluation of an assay for methylated BCAT1 and IKZF1 in plasma for detection of colorectal neoplasia. BMC Cancer 2015, 15, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Vecchio Blanco, G.; Cretella, M.; Paoluzi, O.A.; Caruso, A.; Mannisi, E.; Servadei, F.; Romeo, S.; Grasso, E.; Sileri, P.; Giannelli, M.; et al. Adenoma, advanced adenoma and colorectal cancer prevalence in asymptomatic 40- to 49-year-old subjects with a first-degree family history of colorectal cancer. Colorectal Dis. 2013, 15, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Ching, J.Y.; Chan, V.; Wong, M.C.; Suen, B.Y.; Hirai, H.W.; Lam, T.Y.; Lau, J.Y.; Ng, S.S.; Wu, J.C.; et al. Diagnostic accuracy of faecal immunochemical test for screening individuals with a family history of colorectal cancer. Aliment. Pharmacol. Ther. 2013, 38, 835–841. [Google Scholar] [CrossRef]
- Quintero, E.; Carrillo, M.; Leoz, M.L.; Cubiella, J.; Gargallo, C.; Lanas, A.; Bujanda, L.; Gimeno-García, A.Z.; Hernández-Guerra, M.; Nicolás-Pérez, D.; et al. Risk of Advanced Neoplasia in First-Degree Relatives with Colorectal Cancer: A large multicenter cross-sectional study. PLoS Med. 2016, 13, e1002008. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Colorectal Findings | n | Mean ± SD | Median (IQR) | p-Value 1 | |
|---|---|---|---|---|---|
| a | b | ||||
| No neoplasia | 330 | 1.96 ± 10.39 | 0.00 (0.00–0.00) | ||
| No colorectal findings | 171 | 2.32 ± 9.53 | 0.00 (0.00–0.00) | ||
| Benign pathologies | 159 | 1.58 ± 11.26 | 0.00 (0.00–0.00) | 0.083 | |
| Inflammatory polyps | 4 | 0.00 | 0.00 | 0.229 | |
| Hyperplastic polyps | 38 | 3.03 ± 16.31 | 0.00 (0.00–0.00) | 0.037 | |
| Hemorrhoids | 65 | 0.45 ± 1.89 | 0.00 (0.00–0.00) | 0.122 | |
| Diverticula | 46 | 2.33 ± 14.73 | 0.00 (0.00–0.00) | 0.526 | |
| Other benign pathologies | 6 | 0.00 | 0.00 | 0.141 | |
| Non-advanced adenomas | 117 | 1.15 ± 9.30 | 0.00 (0.00–0.00) | 0.192 | 0.547 |
| Advanced neoplasia | 57 | 10.92 ± 27.79 | 0.00 (0.00–3.52) | <0.001 | <0.001 |
| Advanced adenomas | 53 | 10.85 ± 28.51 | 0.00 (0.00–2.74) | <0.001 | <0.001 |
| Cancer | 4 | 11.91 ± 17.93 | 4.87 (0.00–30.86) | 0.026 | 0.011 |
| Characteristic | n | Mean ± SD | Median (IQR) | p-Value 1 |
|---|---|---|---|---|
| Number | ||||
| 1–2 | 138 | 3.55 ± 16.40 | 0.00 (0.00–0.00) | 0.429 |
| ≥3 | 32 | 6.84 ± 24.51 | 0.00 (0.00–0.32) | |
| Size | ||||
| <10 mm | 123 | 2.69 ± 14.74 | 0.00 (0.00–0.00) | 0.001 |
| ≥10 mm | 47 | 8.05 ± 24.78 | 0.00 (0.00–2.05 | |
| Histology | ||||
| Tubular | 143 | 2.65 ± 14.60 | 0.00 (0.00–0.00) | <0.001 |
| Villous component | 27 | 12.21 ± 30.00 | 0.46 (0.00–6.50) | |
| Adenomas | ||||
| Non-advanced | 117 | 1.15 ± 9.30 | 0.00 (0.00–0.00) | <0.001 |
| Advanced | 53 | 10.85 ± 28.51 | 0.00 (0.00–2.74) | |
| Location | ||||
| Distal | 129 | 5.32 ± 20.70 | 0.00 (0.00–0.13) | 0.680 |
| Only proximal | 41 | 0.56 ± 2.06 | 0.00 (0.00–0.00) |
| Advanced Neoplasia | Advanced Adenomas | |||||||
|---|---|---|---|---|---|---|---|---|
| NEUROG1 Cut-Off (NMP) | Specificity % (95% CI) | Sensitivity % (95% CI) | NPV % (95% CI) | PPV % (95% CI) | Sensitivity % (95% CI) | NPV % (95% CI) | PPV % (95% CI) | Detection % Distal/Proximal1 |
| >1.3518% | 90.60 (87.5–93.1) | 33.33 (21.4–47.1) | 91.4 (88.4–93.9) | 31.1 (19.9–44.3) | 32.08 (19.9–46.3) | 91.8 (88.9–94.2) | 28.8 (17.8–42.1) | 28.21/42.86 (NS) |
| >7.4194% | 95.30 (92.9–97.1) | 17.54 (8.7–29.9) | 90.1 (87.0–92.6) | 32.3 (16.7–51.4) | 15.09 (6.7–27.6) | 90.4 (87.4–92.9) | 27.6 (12.7–47.2) | 17.95/21.43 (NS) |
| Advanced Neoplasia | Advanced Adenomas | |||||||
|---|---|---|---|---|---|---|---|---|
| Cut-Off | Specificity % (95% CI) | Sensitivity % (95% CI) | NPV % (95% CI) | PPV % (95% CI) | Sensitivity % (95%CI) | NPV % (95% CI) | PPV % (95% CI) | Detection % Distal/Proximal |
| FIT >0.2684 | 95.75 (93.4–97.4) | 45.61 a (32.4–59.3) | 93.2 (90.6–95.4) | 57.8 (42.2–72.3) | 41.51 c (28.1–55.9) | 93.243 (90.6–95.4) | 53.7 (37.4–69.3) | 48.72/21.43 (NS) |
| FIT >0.4190 | 98.21 (96.5–99.2) | 29.82 b (18.4–43.4) | 91.6 (88.8–94.0) | 68.0 (46.5–85.1) | 26.42 d (15.3–40.3) | 91.8 (89.0–94.1) | 63.6 (40.7–82.8) | 35.90/0.00 * |
| NEUROG1 + FIT >0.2899 | 95.75 (93.4–97.4) | 50.88 a (37.3–64.4) | 93.9 (91.2–95.9) | 60.4 (45.3–74.2) | 47.17 c (33.3–61.4) | 93.9 (91.2–95.9) | 56.8 (41.0–71.7) | 53.85/28.57 (NS) |
| NEUROG1 + FIT >0.4598 | 98.21 (96.5–99.2) | 40.35 b (27.6–54.2) | 92.8 (90.1–95.0) | 72.4 (55.4–88.1) | 35.85 d (23.1–50.2) | 92.8 (90.1–95.0) | 70.4 (49.8–86.2) | 43.59/14.29 (NS) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otero-Estévez, O.; Gallardo-Gomez, M.; Páez de la Cadena, M.; Rodríguez-Berrocal, F.J.; Cubiella, J.; Hernandez Ramirez, V.; García-Nimo, L.; De Chiara, L. Value of Serum NEUROG1 Methylation for the Detection of Advanced Adenomas and Colorectal Cancer. Diagnostics 2020, 10, 437. https://doi.org/10.3390/diagnostics10070437
Otero-Estévez O, Gallardo-Gomez M, Páez de la Cadena M, Rodríguez-Berrocal FJ, Cubiella J, Hernandez Ramirez V, García-Nimo L, De Chiara L. Value of Serum NEUROG1 Methylation for the Detection of Advanced Adenomas and Colorectal Cancer. Diagnostics. 2020; 10(7):437. https://doi.org/10.3390/diagnostics10070437
Chicago/Turabian StyleOtero-Estévez, Olalla, María Gallardo-Gomez, María Páez de la Cadena, Francisco Javier Rodríguez-Berrocal, Joaquín Cubiella, Vicent Hernandez Ramirez, Laura García-Nimo, and Loretta De Chiara. 2020. "Value of Serum NEUROG1 Methylation for the Detection of Advanced Adenomas and Colorectal Cancer" Diagnostics 10, no. 7: 437. https://doi.org/10.3390/diagnostics10070437