Design and Development of a Methodology Based on Expert Systems, Applied to the Treatment of Pressure Ulcers

 , , and
, , and
Abstract
:1. Introduction
1.1. Related Concepts
1.1.1. Health Assessment Process for Pressure Ulcers
- Gathering information about the patient and her wound.
- Evaluation of the collected information: patient’s potential risk factors, such as the stage in which the chronic wound is classified, its size, whether it presents exudate or infection, among others [18].
- Development of a treatment plan.
Scales for Risk Assessment of PU
1.1.2. Use of Expert Systems in Decision-Support Tools
1.1.3. Expert Systems in Health Applications
2. Materials and Methods
2.1. Definition of the Methodology
2.1.1. Conceptual Design of the Proposed Methodology
2.1.2. Previous Considerations
- Guideline 1—Design an artifact: the proposed methodology, developed through a software-supported artifact that implements an expert systems, is presented in detail throughout Section 2. Its purpose is to help the healthcare team in the difficult stages of monitoring and assessing the status of PU. To do this, first the artifact supported by specifically developed software performs the calculation of two index values named ‘Technical Risk’ and ‘Expert Risk’. These are obtained as a result of processing the input information by means of two fuzzy inference engines working concurrently. Subsequently, these calculated risk indices are combined in order to produce an overall risk indicator called ‘Global Risk’, which allows to establish the risk level related to the non-improvement of the ulcer status with the current treatment. Finally, different recommendations can be established based on the interpretation of the Global Risk, as a result of which it might be necessary to immediately change the treatment that the patient is currently receiving, and to choose a new one. To facilitate all the necessary calculations, the implementation of the artifact has been carried out in the shape of an application developed using the MATLAB© software. This makes it possible to facilitate and systematize its usage as a way to show its viability.
- Guideline 2—Relevance of the problem: the design and definition of a methodology that allows to keep watch over the PU monitoring and assessment stages is a relevant fact in the healthcare field, not only because of the repercussion associated with the social factors (swiftness of treatment, satisfaction, costs reduction, etc.), but also due to the progress itself in the implementation and use of information technologies in the healthcare industry. On the other hand, in many cases it may happen either that the professional in charge of the treatment is not properly trained in the subject matter, or that it may not be the same person who performs all the treatment sessions, thus making it difficult to monitor and assess it. For all the above-mentioned reasons, the design of a methodology to be applied in the field of chronic wounds is considered sufficiently relevant to justify its development.
- Guideline 3—Design evaluation: Section 3 presents a case study that illustrates with examples how the methodology works. In addition to showing the operation of the software-supported artifact, in Section 4, the usefulness and effectiveness of the methodology for solving the target problem are analyzed.
- Guideline 5—Rigor in the research: the new methodology has been framed within the context of information systems and design science research, through the design of a software-supported device based on expert systems, with all of that being approached in Section 1. Furthermore, their mathematical developments are basically grounded on the concepts of fuzzy inference systems, commonly proven and acknowledged, given their effectiveness and capability of managing the uncertainty level associated with any decision-making process.
- Guideline 6—Design as a search: in Section 1 a description of the context in which the proposed methodology is framed has been carried out.
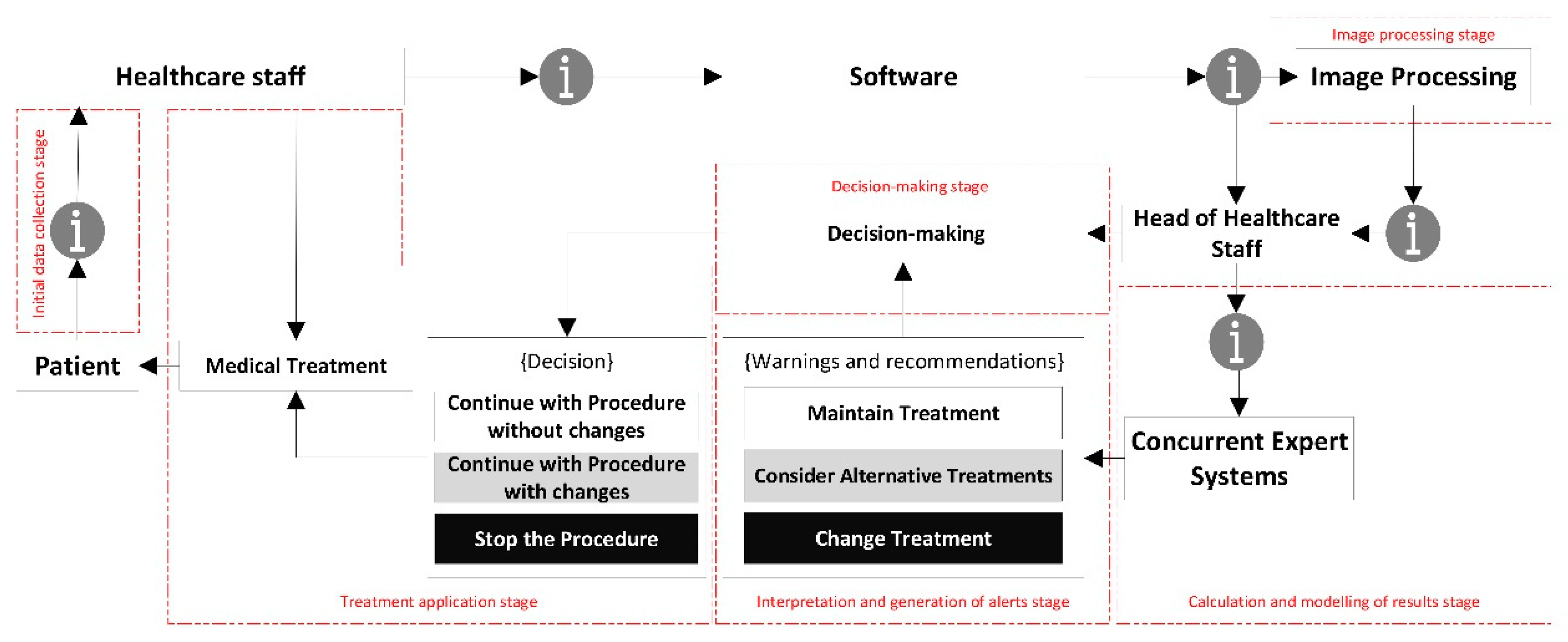
2.1.3. Description of the Methodology
Initial Data Collection Stage
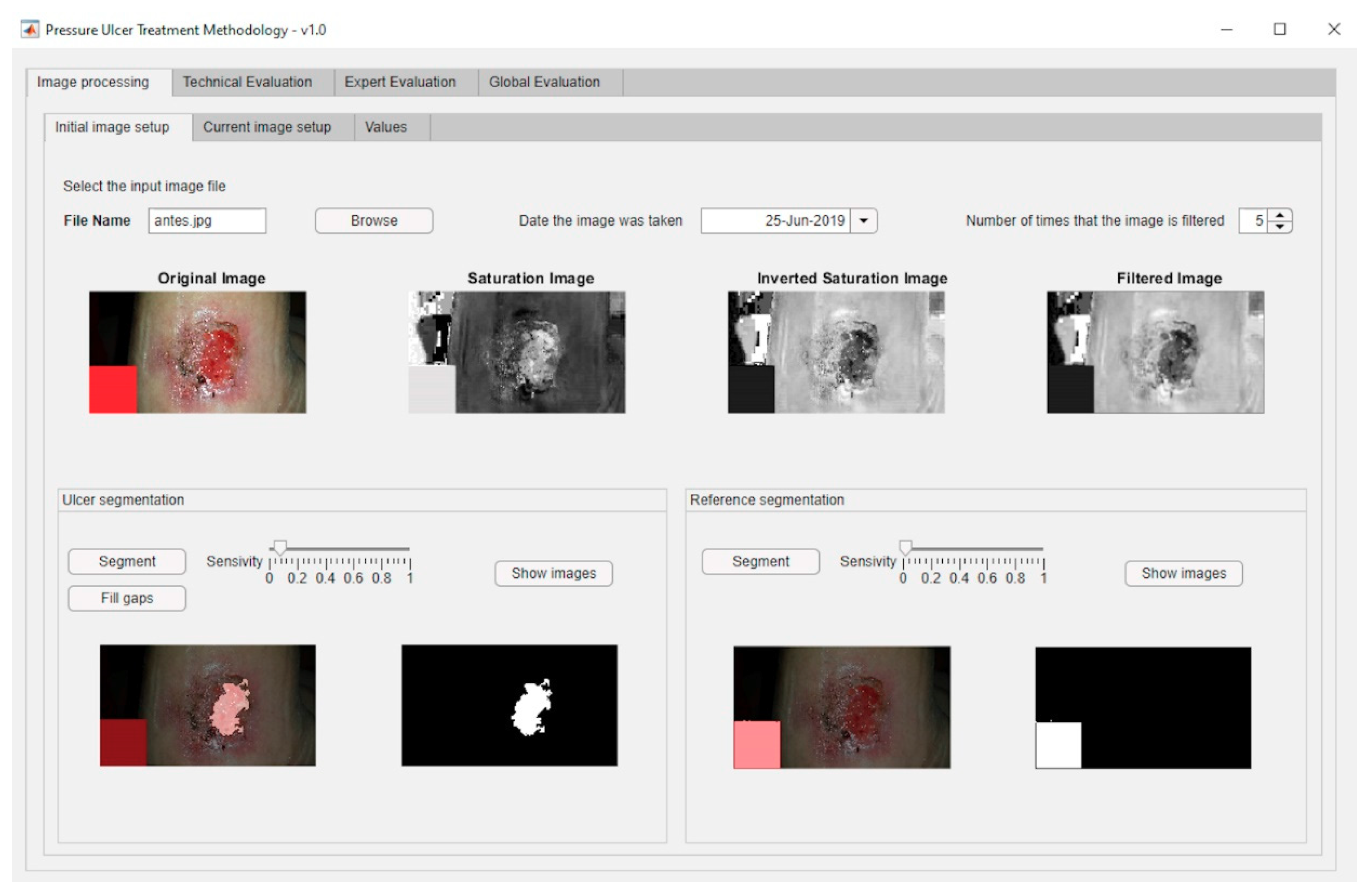
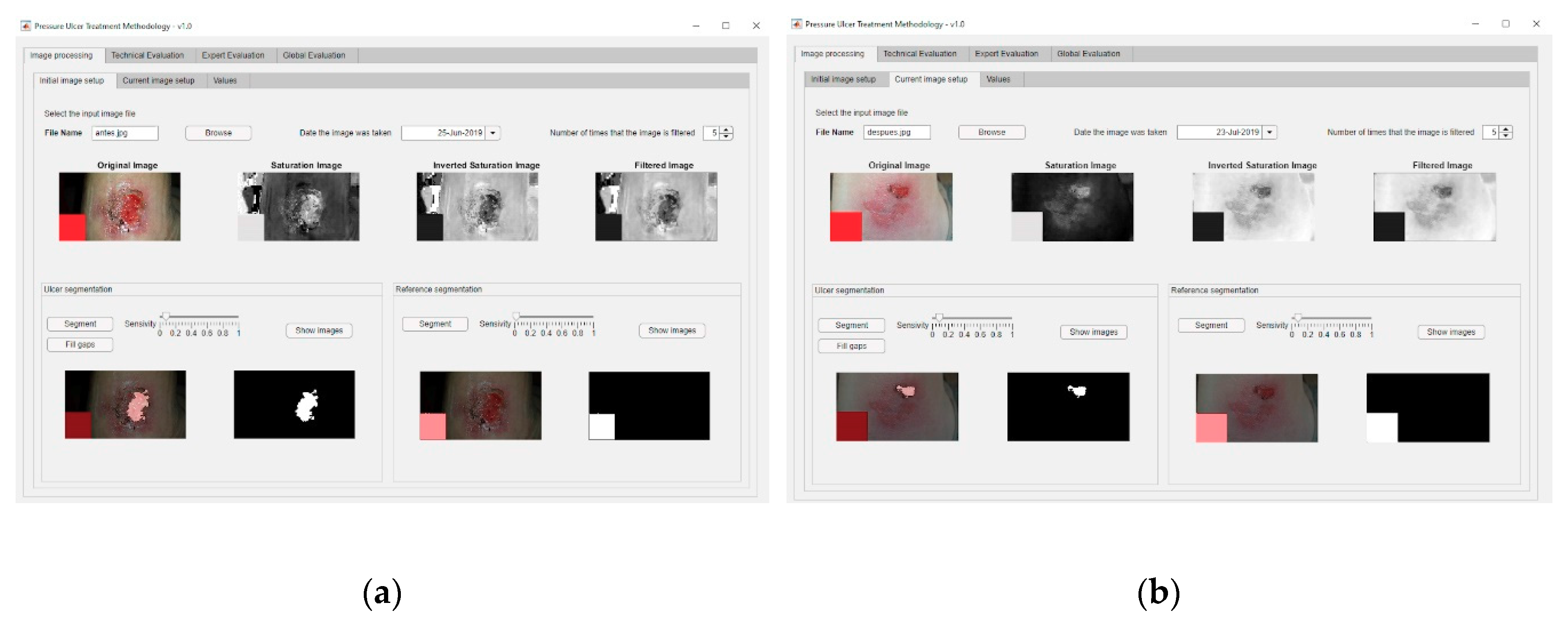
Image Processing Stage
- Pre-processing: the saturation plane of the digital image is selected, inverted, and subsequently filtered as many times as necessary.
- Segmentation: the image is segmented in order to isolate the wound region in order to subsequently calculate its surface area measured in pixels. It is important to say that this segmentation uses a reference pattern that must be pointed at by the user. Additionally, it is possible to establish a sensitivity parameter associated to the segmentation threshold.
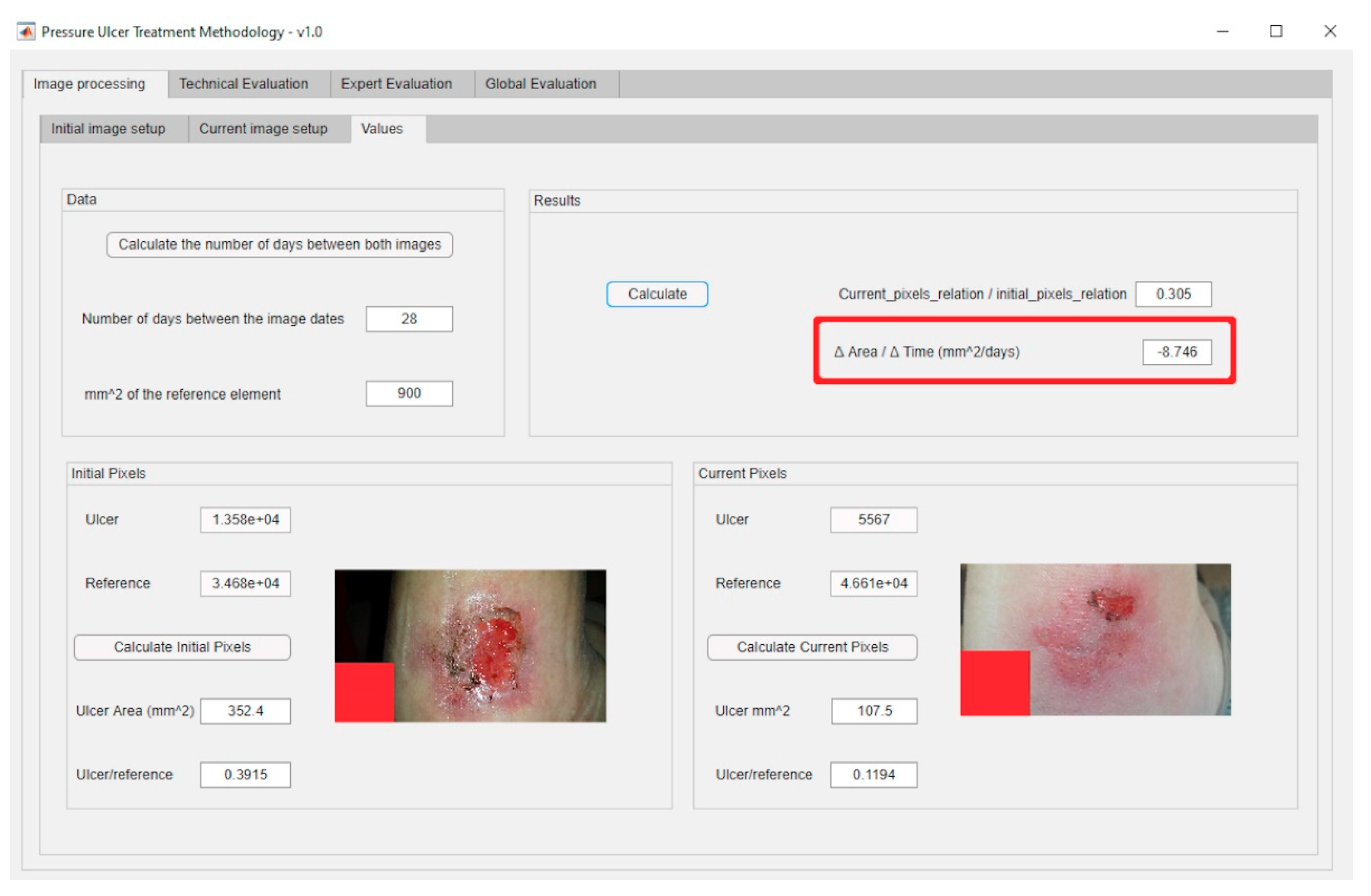
Calculation and Modelling of Results Stage
Interpretation and Generation of Alerts Stage
- Continue with the current treatment: no additional actions are recommended, as the evolution of the PU healing does not require it.
- Consider alternative treatments: it is recommended to consider potential alternative treatments or therapies for the cure of PU to replace the current one.
- Change the treatment immediately: it is recommended to stop right away the treatment that the patient is currently being given for her PU and replace it with a different one.
Decision Stage
Treatment Application Stage
- Continue with the procedure without changes: it is recommended to continue with the current treatment.
- Continue with the current treatment with changes: it is recommended to continue with the current treatment while considering alternative ones.
- Stop the procedure: it is recommended to interrupt the current treatment and start with a new one as recommended by the expert.
2.2. Implementation of the Methodology
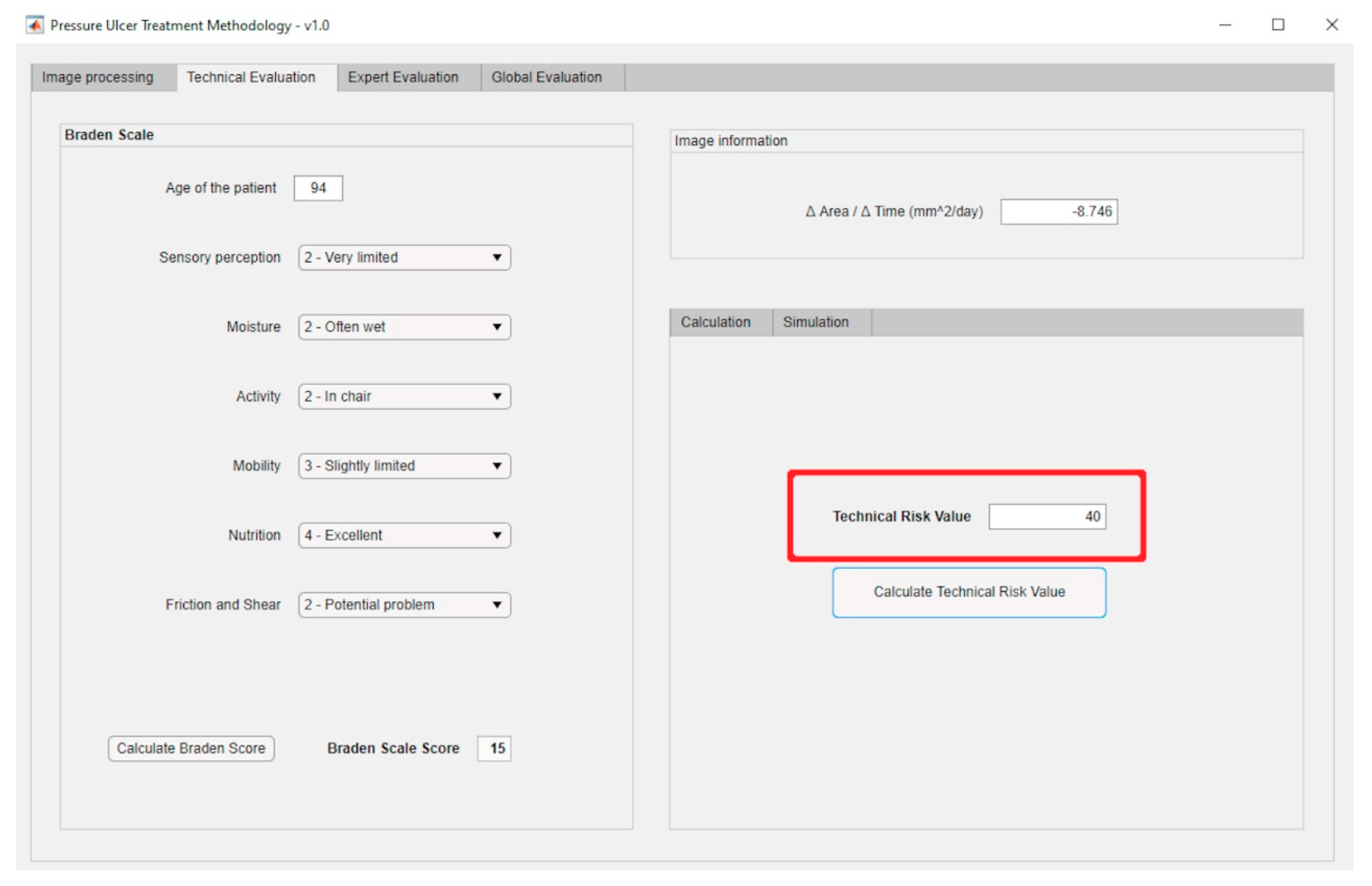
2.2.1. Technical Risk and Expert Risk Concepts
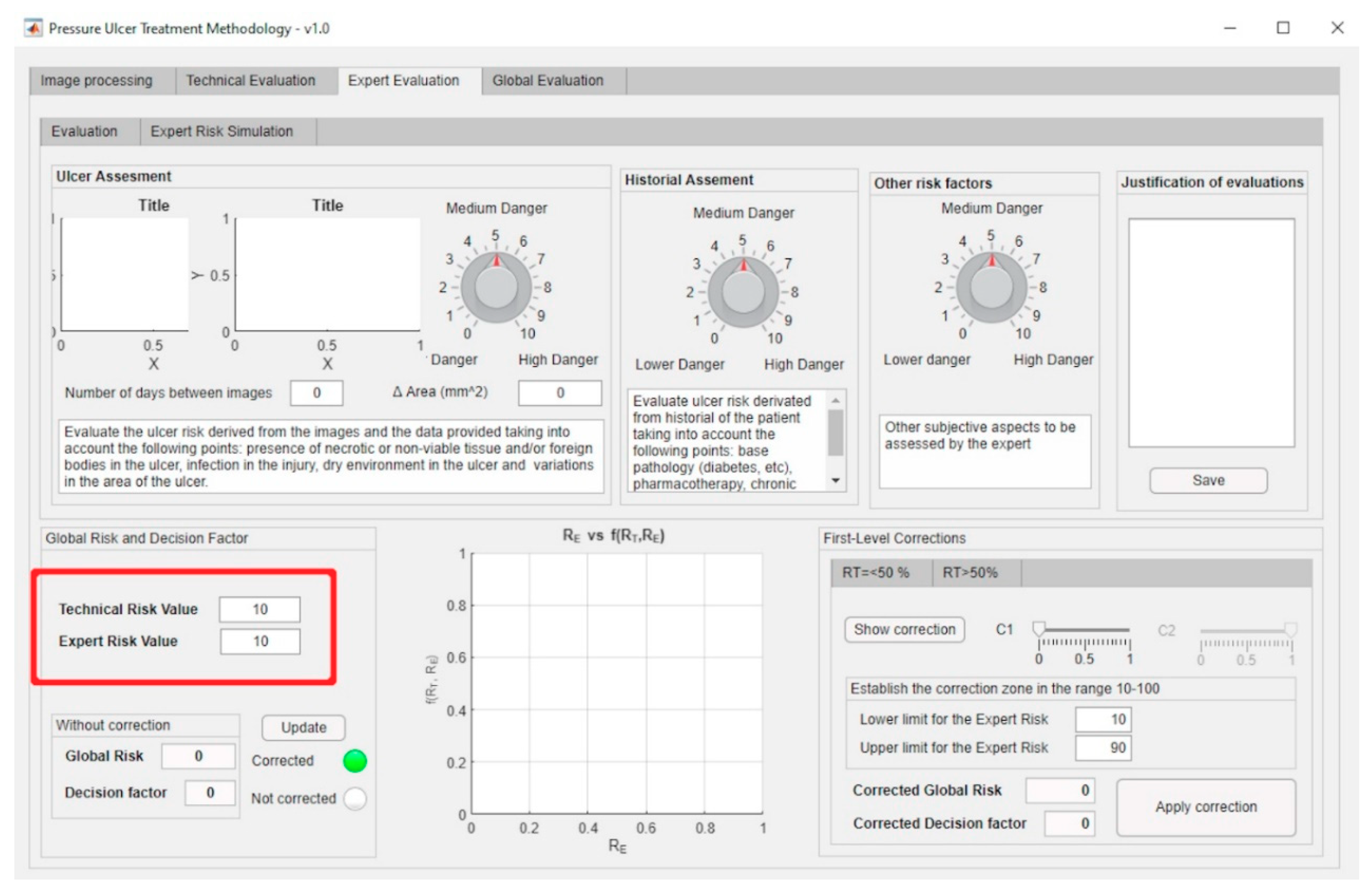
2.2.2. Global Risk and Decision Factor Concepts
Inference Systems: Calculation of Expert and Technical Risk
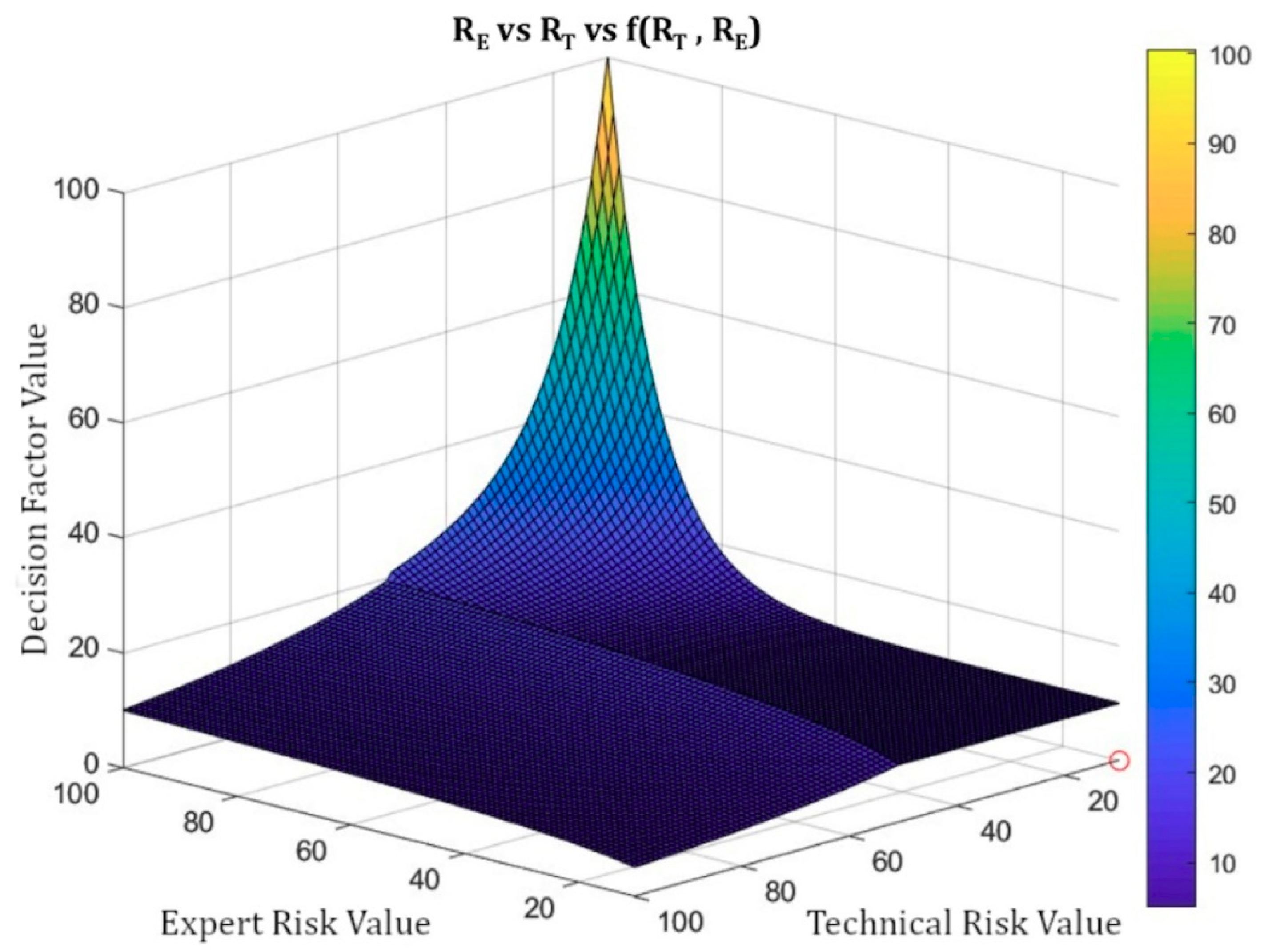
Calculation and Modelling of the Decision Factor
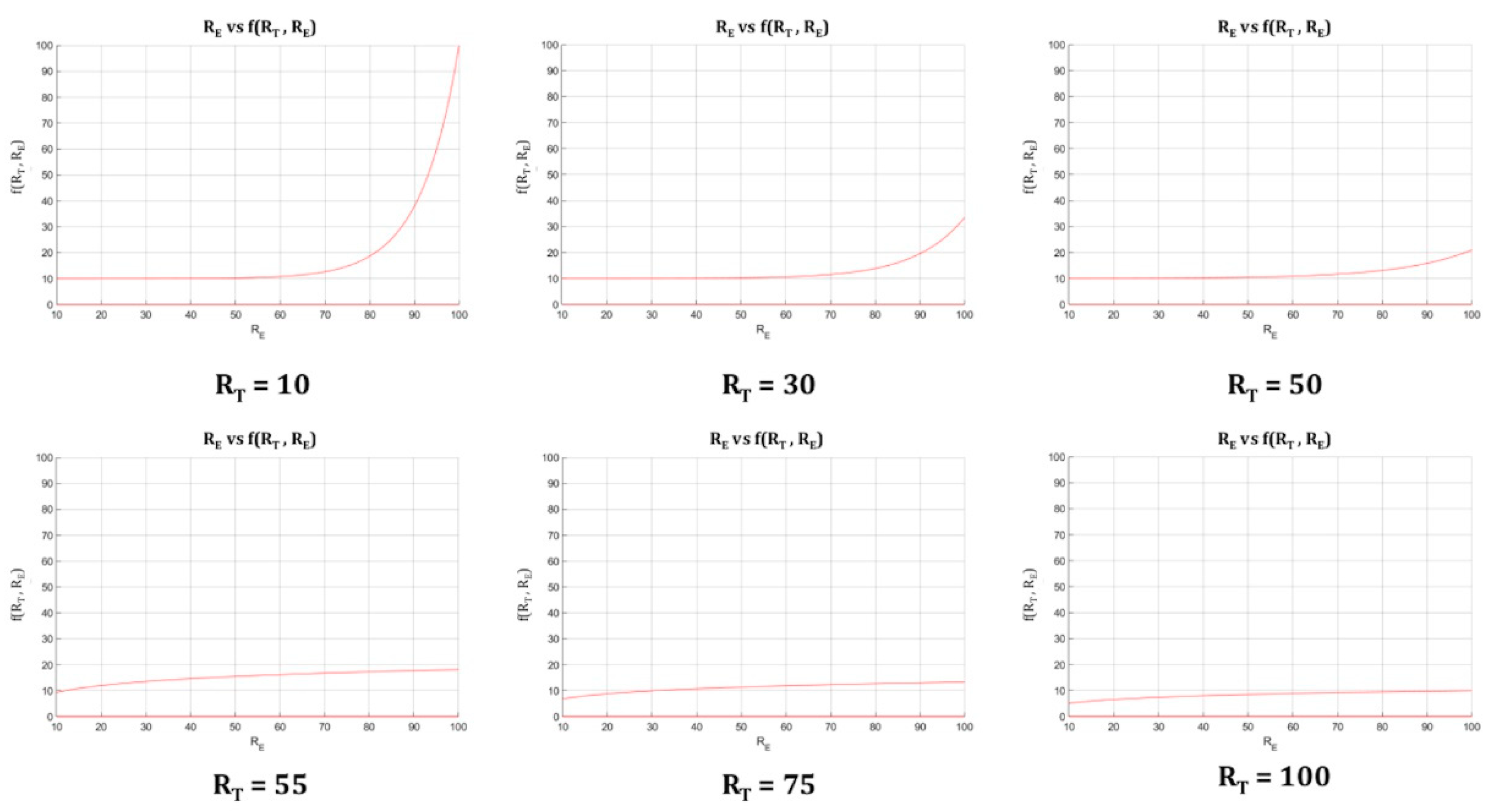
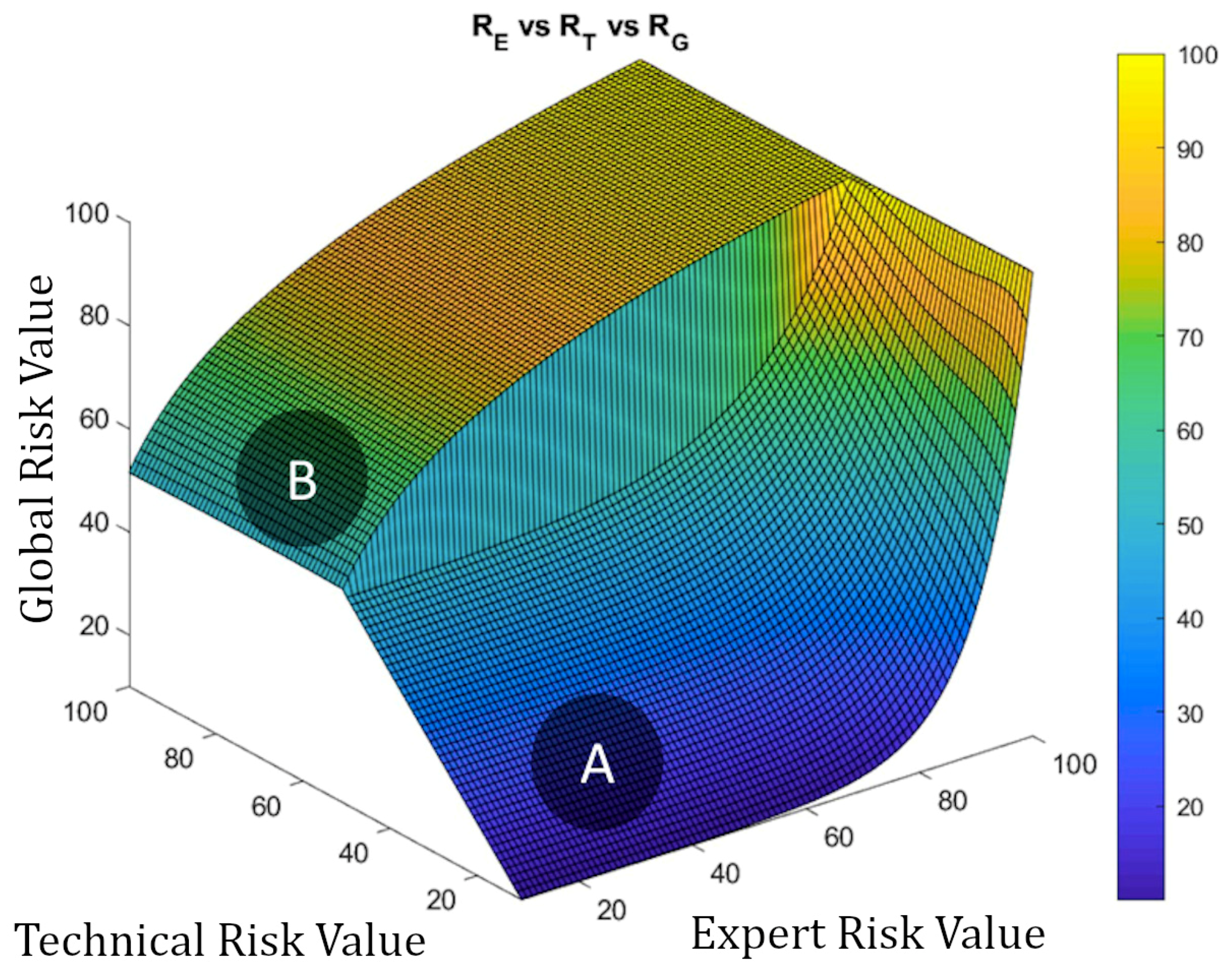
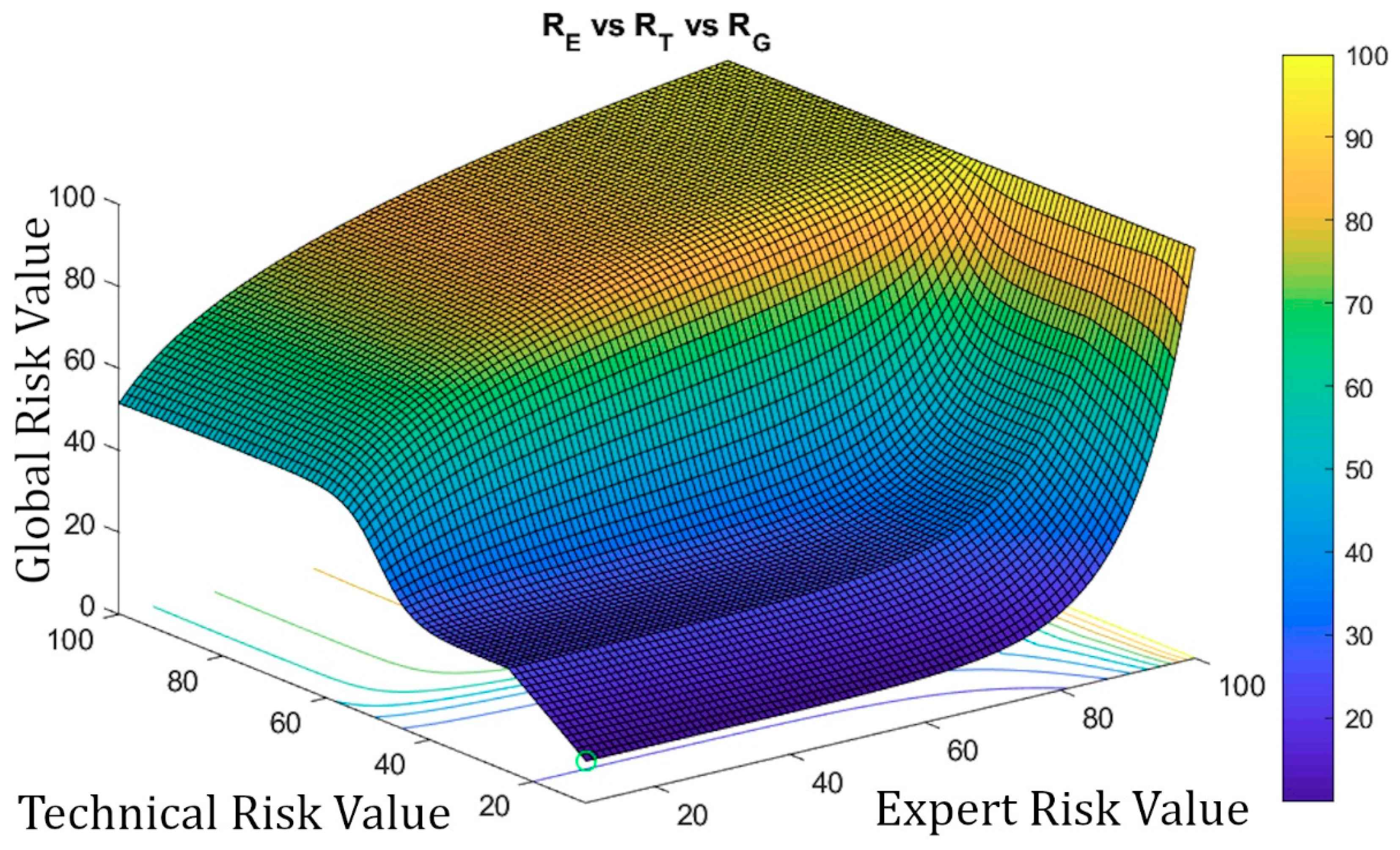
- For Technical Risk values up to 50, the Decision Factor value must be high, in order to obtain a high Global Risk value. It is established that the value of the Decision Factor must grow rapidly as the Expert Risk value increases. This means that, when the Technical Risk values do not indicate a critical state, that is, when they do not support a change in the treatment, then it will be in the hands of the expert to raise the severity level of the ulcer status through her considerations, thus, leading to a high Global Risk value.
- For Technical Risk values above 50, the Decision Factor value is not required to be as high as in the former case in order to produce a high Global Risk value, so it will be possible to obtain high Global Risk figures with low Expert Risk values. That is why, in these kind of cases where the Technical Risk is a dominant factor, the ‘change treatment immediately’ state prevails over the expert’s valuation, and it will be required then that she proves that the ratings reducing the previously established alert level are appropriate.
- Exponential curves: these allow to model the relationship between the Technical Risk, the Expert Risk, and the Decision Factor values for Technical Risk values up to 50, since:
- ◦
- The Decision Factor value is virtually unchanged before the exponential zone is reached.
- ◦
- These curves grow rapidly in the exponential zone.
- ◦
- The Decision Factor will be a function that depends on the Technical Risk functions ( and ), as well as on the Technical Risk and the Expert Risk, values.
- Logarithmic curves: this type of curves allow to model the relationship between the Expert Risk and the Decision Factor values for Technical Risk values above 50, since:
- ◦
- They show a high growth rate in the first section, that is, for Expert Risk values from 20 to 30, after which the growth rate decreases.
- ◦
- The decision factor will be a function that depends on the Technical Risk functions ( and ) as well as on the Technical Risk and the Expert Risk values.
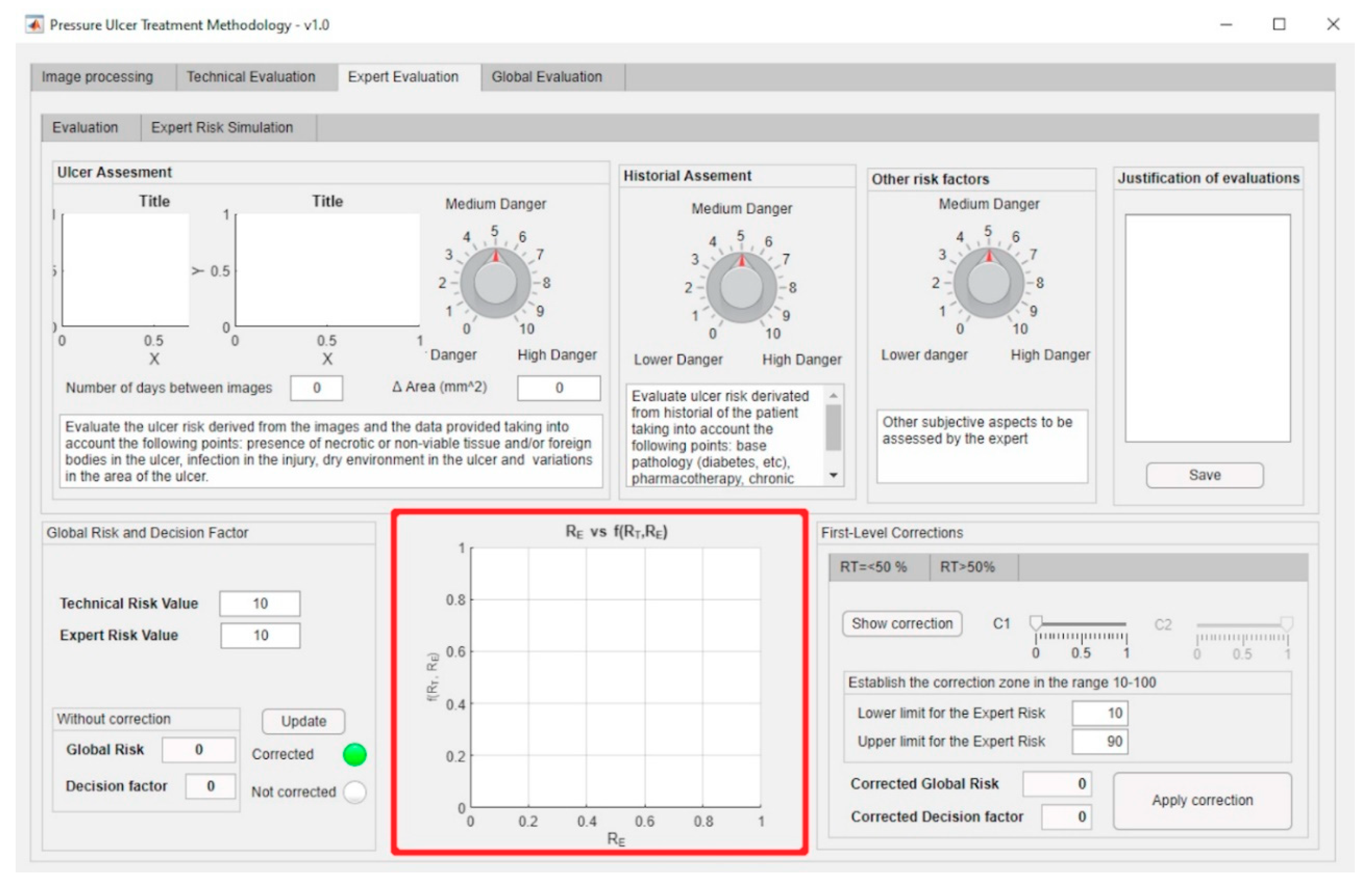
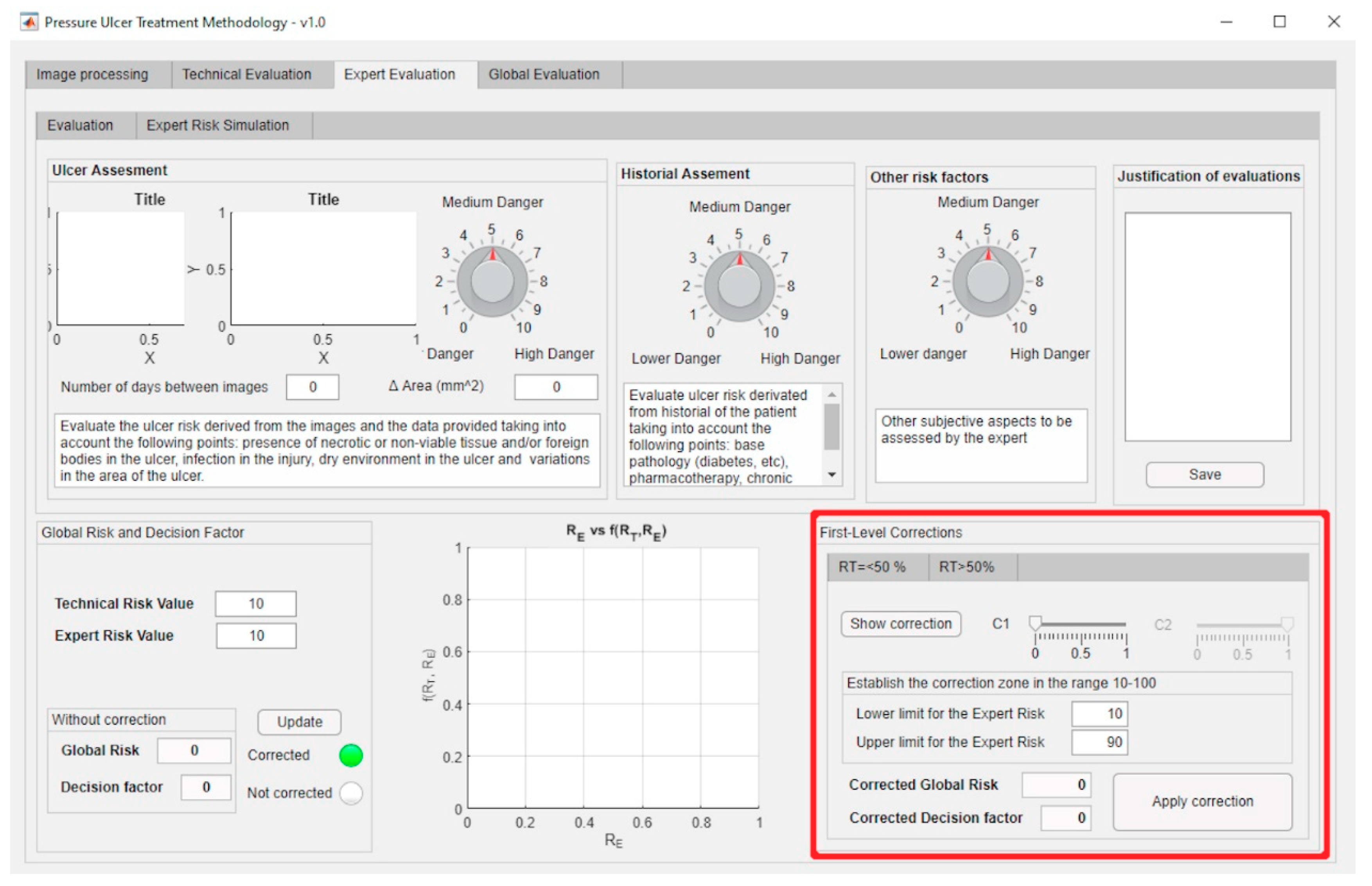
First-Level Corrections
First Level Correction-Exponential Zone
First Level Correction-Logarithmic Zone
2.2.3. Determination of Global Risk and Alert Level
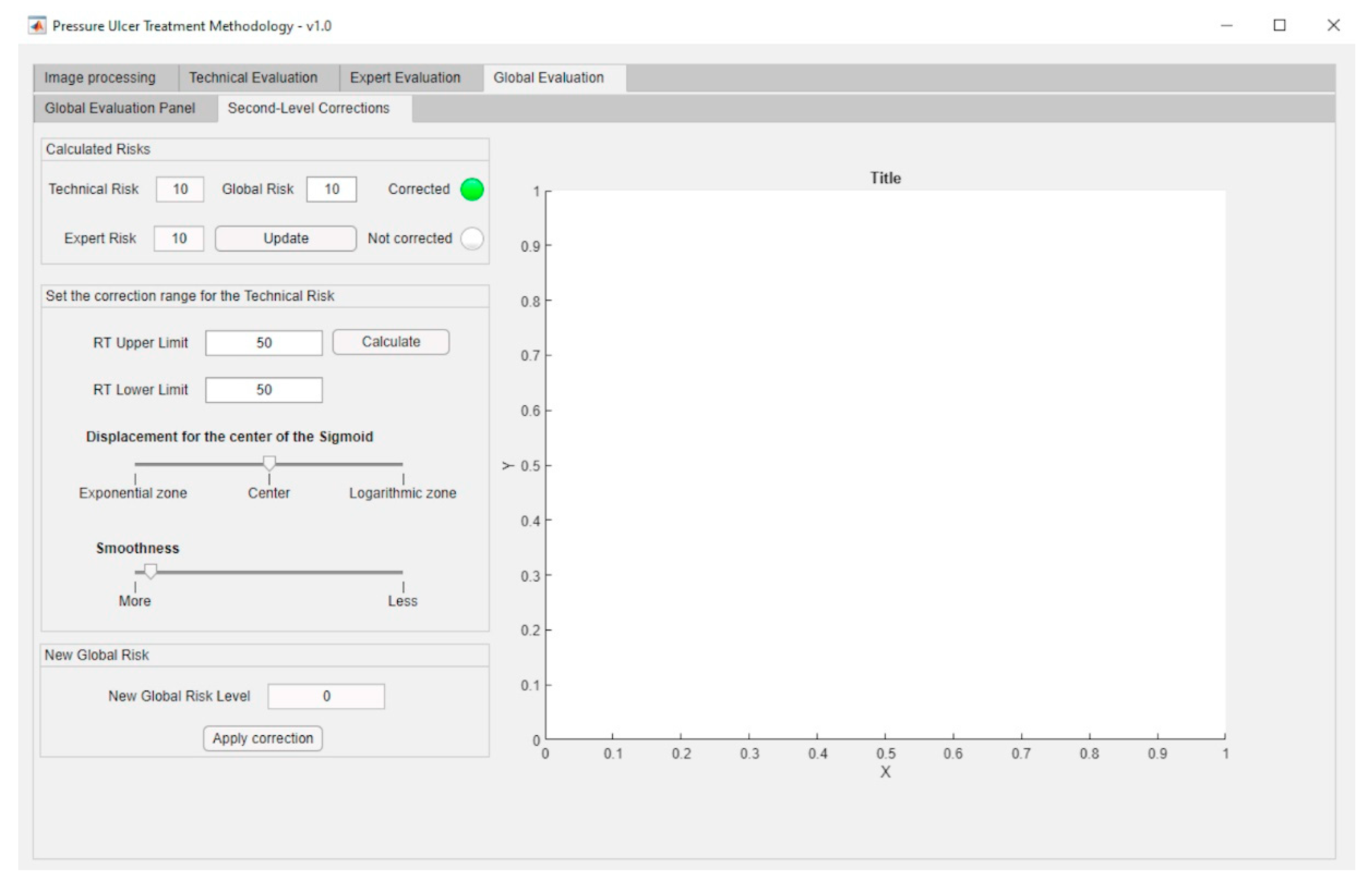
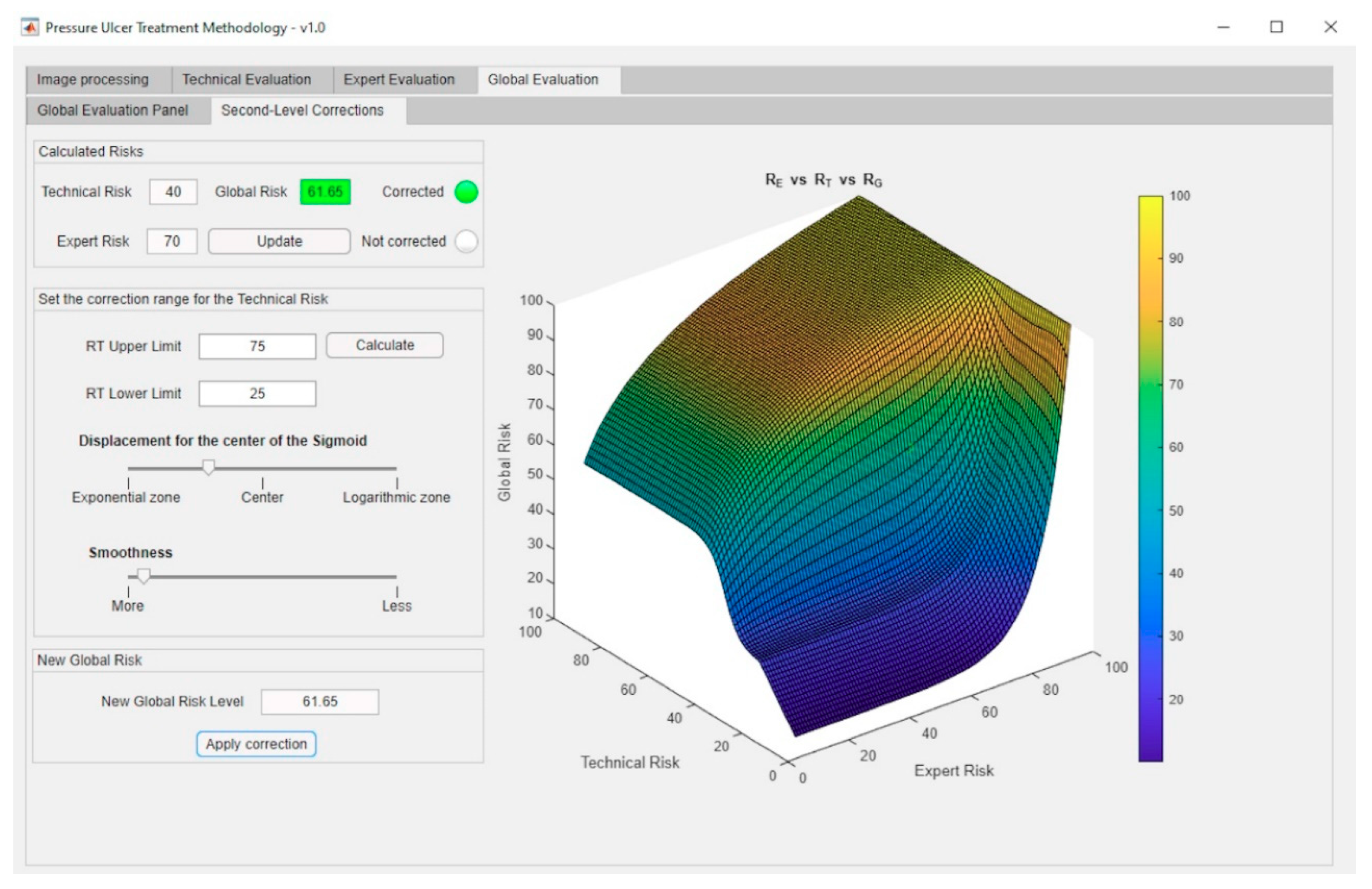
Second-Level Corrections
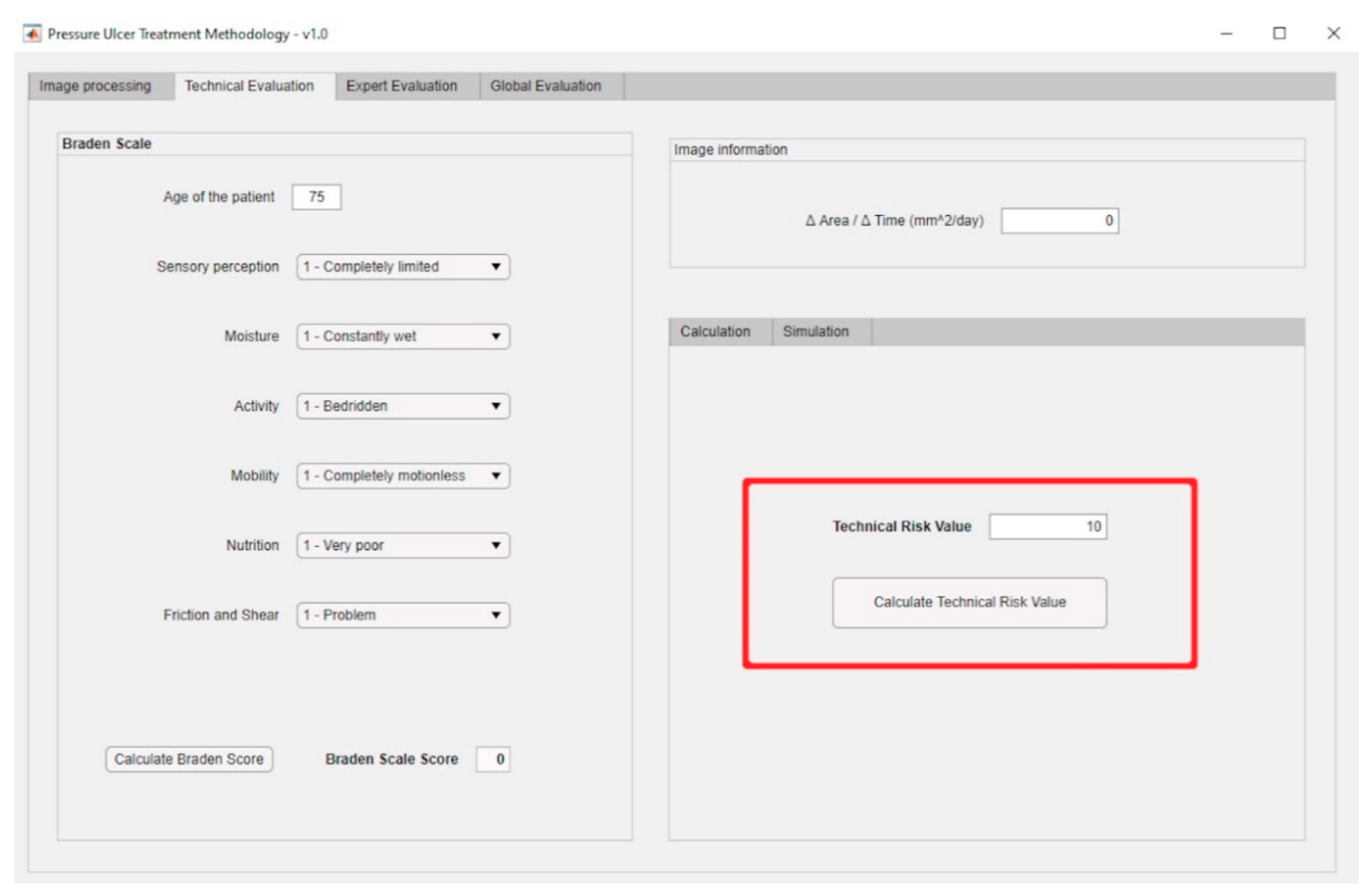
2.2.4. Treatment Evaluation
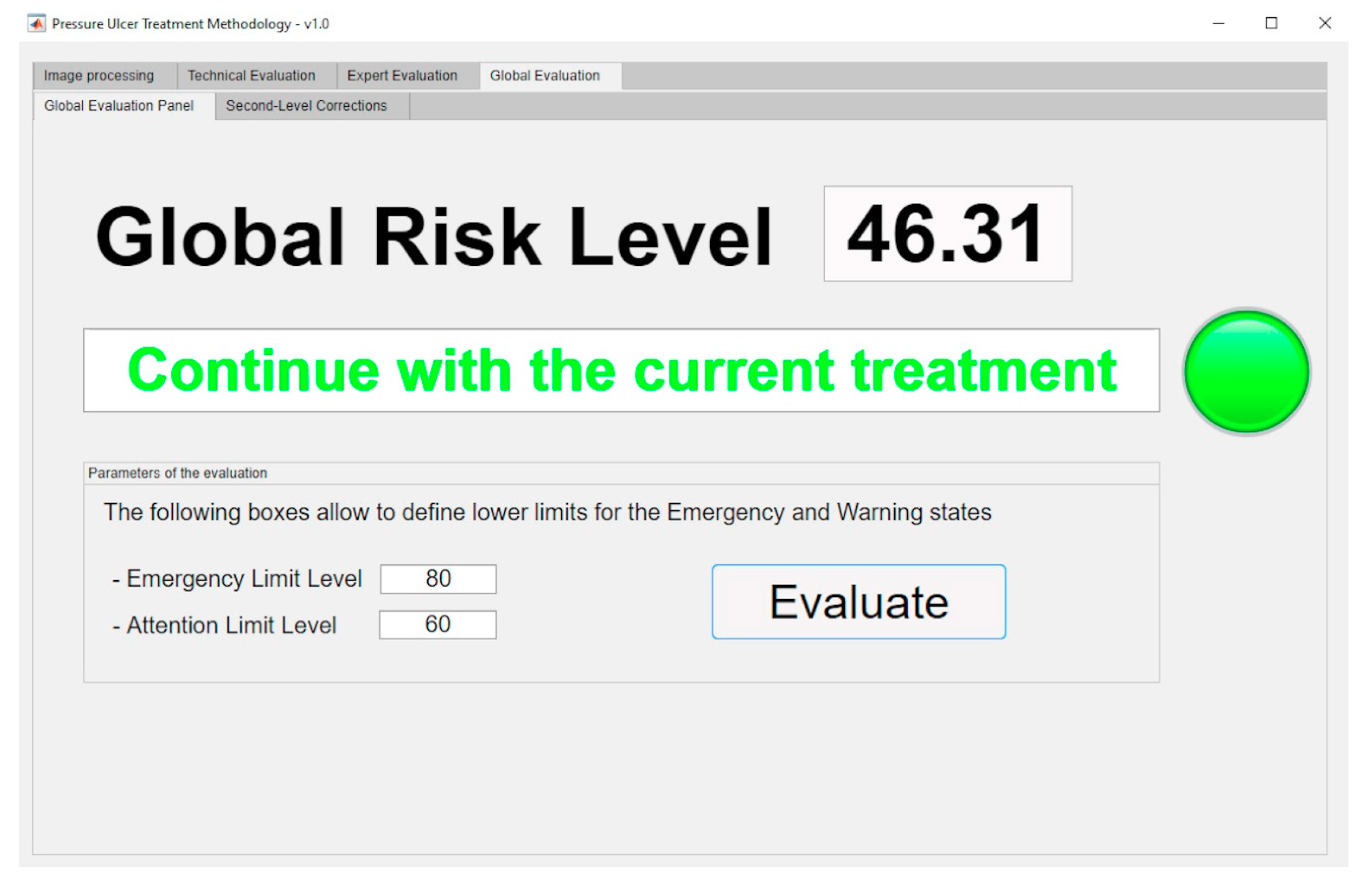
- Continue with the current treatment: the Global Risk value lies within the range [0–60).
- Evaluate alternative treatments: the Global Risk value lies within the range [60–80).
- Change treatment immediately: the Global Risk value lies within the range [80–100]
2.2.5. Implementation of the Artifact at Software Level
3. Practical Example and Results
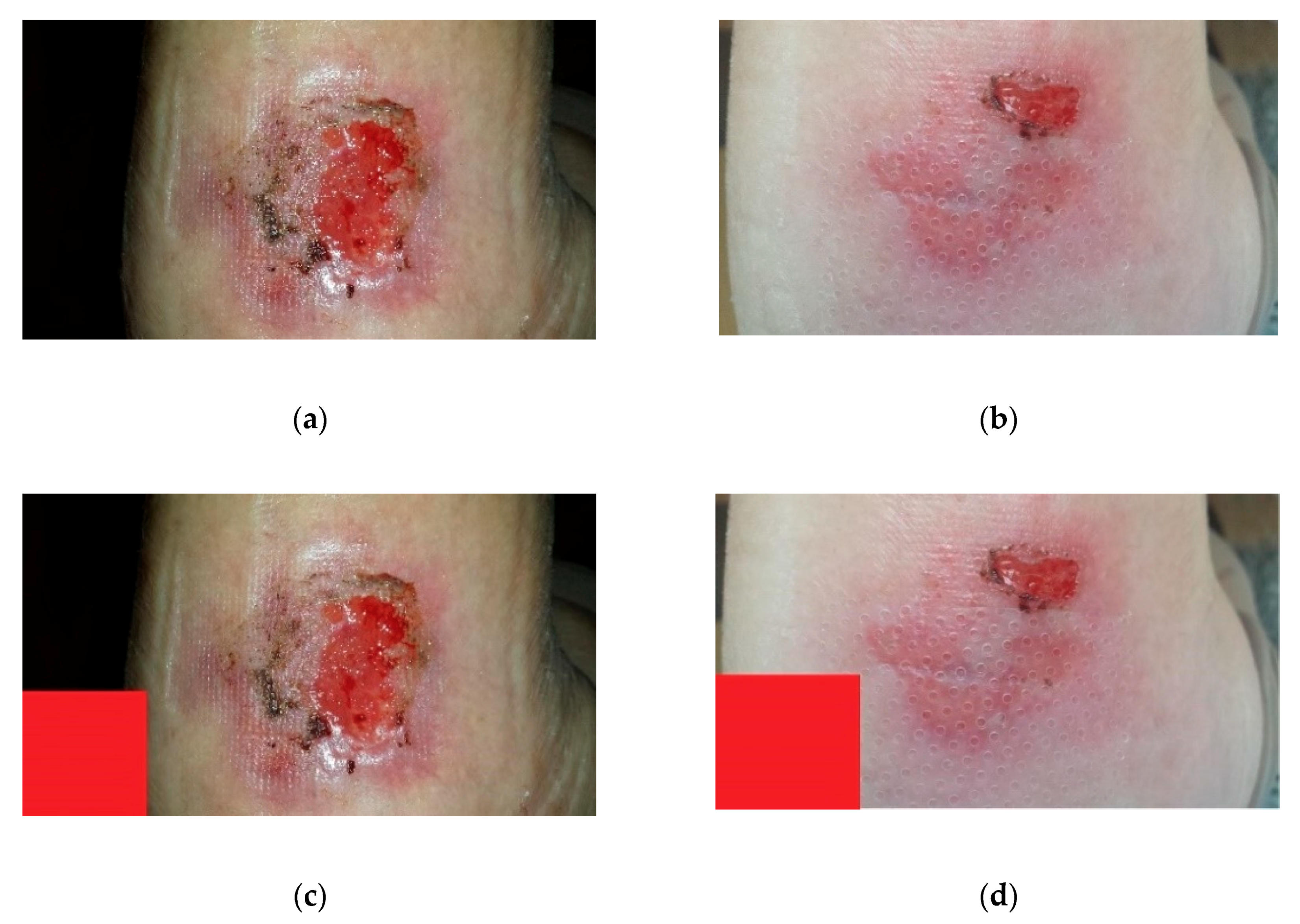
3.1. Stage 1: Data Collection
3.2. Stage 2: Image Processing
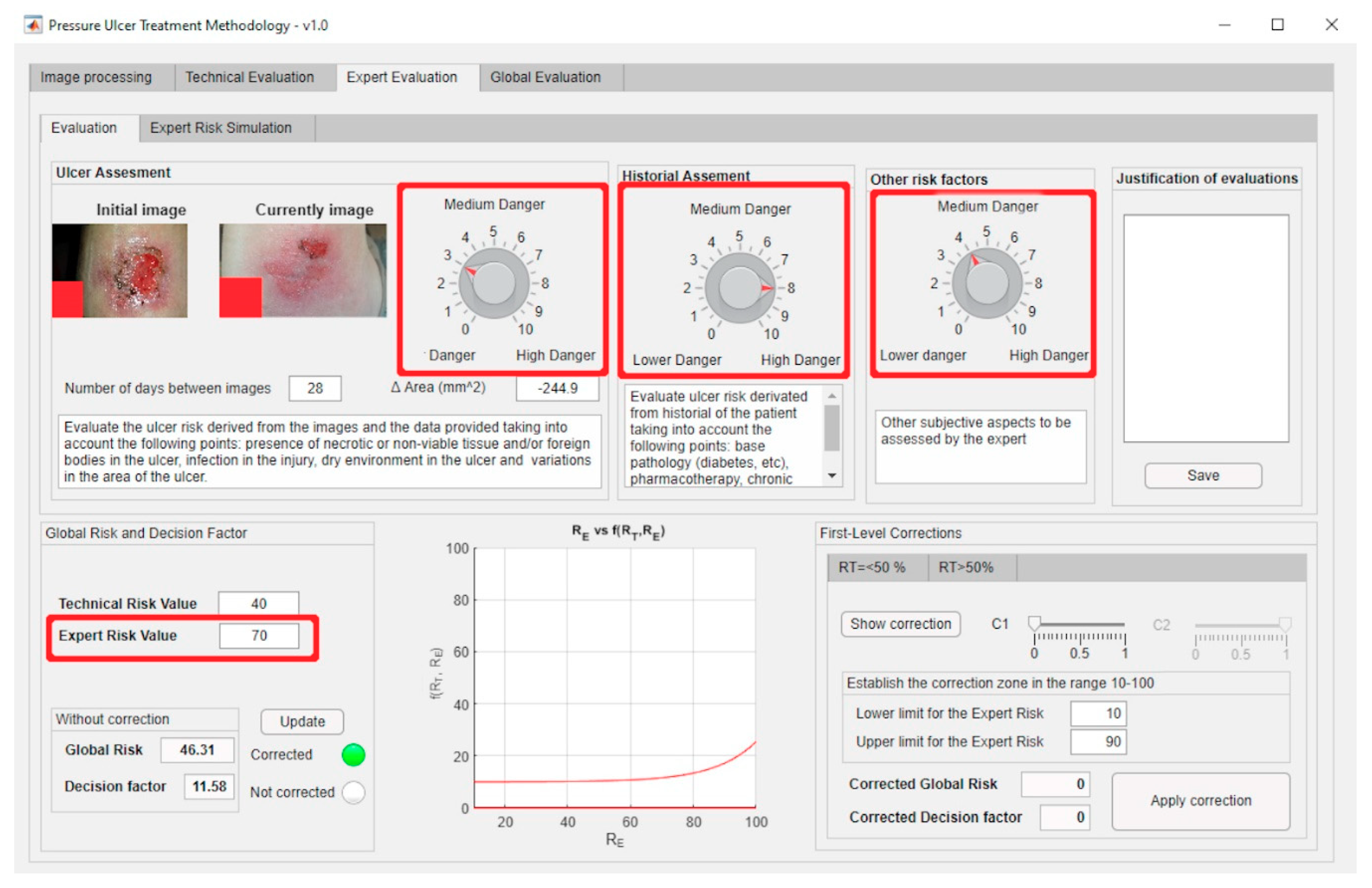
3.3. Stage 3: Calculation and Modelling of Results
- Evaluation of the images: she considered a slightly low risk level, since there is no necrotic tissue, foreign bodies or infection present, the ulcer environment is wet, and the wound surface area has decreased since the last picture (3/10).
- Assessing the patient’s health history: this is an elderly female patient with reduced mobility. She suffers diabetes that is currently undergoing treatment. It is therefore considered a potentially high risk (8/10).
- Other risk factors: a telephone interview with the caregiver finds that the patient has improved in her diet. It was also observed that, because of the wound status improvement, she is not in so much pain anymore and her mobility has improved (4/10).
3.4. Stage 4: Interpretation of Results and Generation of Alerts
3.5. Stage 5: Decision-Making
3.6. Stage 6: Treatment Application
- Although the patient had experienced an improvement, it was observed that the current treatment effects were clearly slowing down, therefore not justifying its cost, and its effectiveness was being jeopardized.
- A decision was made to switch the treatment to another one involving a lower cost but similar healing efficacy.
4. Discussion
- All the stages, from the collection of information to the fuzzification of the input and output variables, can be modified without harming the operation of the inference systems, and, therefore, without affecting the methodology procedures.
- The use of concurrent inference systems allows the expert, who is in charge of managing the second inference system, to assess the accuracy of the measurements that were taken autonomously and loaded into the first system as input variables. The expert can thus detect measurement errors caused by malpractice, manufacturing defects, or the inappropriate usage of the medical instruments involved.
- The second concurrent system, based on the expert’s assessment, is implicitly conditioned by the measurements system. That is, if the expert validates the measurements obtained and categorizes them as reliable, then they will have a greater weight on the final decision associated to the assessment of the treatment, and this will indirectly condition their evaluations by minimizing their errors and subjectivity. Thus, if the system for example detects a combination of technical criteria that advises for a certain change of treatment, it will be the expert who must remarkably change their evaluations to allow the results of the application of the methodology to change substantially. This must be argued and justified by the expert giving appropriate reasons, thus, conditioning her work to be strict and detailed. It would happen similarly in the opposite case, when the Technical Risk values advise to continue with the current treatment, where the expert must correct these indications according to several different options.
- The presented methodology is to be used as an on-the-spot tool, meaning that it works as a decision support tool within the healthcare evaluation process of pressure ulcers. Therefore, it concerns to the health expert to decide whether the behavior of the inference system is appropriate and if it is consistent with the usual distribution of cases. If not, she is granted the choice of either modifying the prior evaluations in the second inference system, or making corrections in the first and second level models. These corrections are in themselves tools to allow for reducing the error in the results by adjusting the calculation models of the decision factor behavior, while at the same time getting those results closer to reality and narrowing down the uncertainty in the models’ definition. Similarly, the second level corrections allow to manage the transition zones between the exponential model, which manages Technical Risk values up to 50, and the logarithmic model, applied when these values are over 50. There is in fact a fictitious alteration in the merging zone of both models, and that is the reason why the expert is offered a tool to modify it, adjusting it to the observed data.
5. Conclusions
- To make a helping system available to healthcare personnel who might not be experts in the treatment and/or healing of chronic wounds, PU in this case.
- To make a system available to enable the monitoring of the healing process of PU, allowing such process to be performed with full knowledge of all its previous details, regardless of who performed the treatment before. This also facilitates comparisons between the PU status at different times.
- The potential application of the monitoring of PU (generally used in patients having a reduced mobility) both to outpatient and hospital care, this one reserved only to bedridden patients.
- To reduce the mistakes in the diagnosis and treatment stages of PU patients by providing the experts with tools allowing to streamline diagnosis work, and also to consolidate and coalesce the information available.
- To lower the length of treatments by reducing the number of evaluation mistakes and supervising the monitoring process, while at the same time cutting down the costs associated with the use of the appropriate healthcare equipment.
- As already mentioned, the methodology is to be used as an on-the-spot tool, meaning that it does not record its decisions beyond a specific application associated to a particular moment in time. With that, the behavior of the inference system is not affected by any corrections other than those allowed during its application, and that limits its usefulness. The incorporation of an associated database and the definition of adaptive algorithms that could modify the behavior of the system between measurements depending on a set of pre-defined rules, would substantially improve the applicability of the methodology.
- The nature itself of the expert systems as autonomous decision-making elements is conditioned by the definition and the influence of the expert throughout the whole process. Although this autonomous behavior might be considered desirable, the specific importance of the environment where it is to be applied compels the participation of an expert in the final decision making. The reliability of an autonomous system in the recommendation of a PU diagnosis and the evaluation of its treatment is unavoidably limited by the potential consequences of a mistake. Even if this situation must still evolve, in this case the use of expert systems, together with the presence of an expert for reviewing and managing them, is considered acceptable.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Soldevilla Agreda, J.J.; Torra i Bou, J.E.; Posnett, J.; Verdú Soriano, J.; San Miguel, L.; Mayan Santos, J.M. Una aproximación al impacto del coste económico del tratamiento de las úlceras por presión en España. Gerokomos 2007, 18, 43–52. [Google Scholar] [CrossRef] [Green Version]
- Terry, M.; Halstead, L.S.; O’Hare, P.; Gaskill, C.; Ho, P.S.; Obecny, J.; James, C.; Lauderdale, M.E. Feasibility study of home care wound management using telemedicine. Adv. Skin Wound Care 2009, 22, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Martínez-Esperanza, E. Evaluación de las guías de práctica clínica españolas sobre úlceras por presión en cuanto a su calidad, grado de evidencia de sus recomendaciones y su aplicación en los medios asistenciales-GNEAUPP. Ph.D. Thesis, Universidad de Alicante, Alicante, Spain, 2012. [Google Scholar]
- Scholz, J.A. What is telemedicine? Ohio Nurses Rev. 1999, 74, 16. [Google Scholar] [PubMed]
- Mars, M. Telemedicine and advances in urban and rural healthcare delivery in Africa. Prog. Cardiovasc. Dis. 2013, 56, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Hjelm, N.M. Benefits and drawbacks of telemedicine. J. Telemed. Telecare 2005, 11, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.; Patterson, V. Introduction to the practice of telemedicine. J. Telemed. Telecare 2005, 11, 3–9. [Google Scholar] [CrossRef]
- Ekeland, A.G.; Bowes, A.; Flottorp, S. Methodologies for assessing telemedicine: A systematic review of reviews. Int. J. Med. Inform. 2012, 81, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Eren, A.; Subasi, A.; Coskun, O. A decision support system for telemedicine through the mobile telecommunications platform. J. Med. Syst. 2008, 32, 31–35. [Google Scholar] [CrossRef]
- Rudi, R.; Celler, B.G. Design and implementation of expert-telemedicine system for diabetes management at home. In Proceedings of the 2006 International Conference on Biomedical and Pharmaceutical Engineering, Singapore, 11–14 December 2006; pp. 595–599. [Google Scholar]
- Norris, A.C. Essentials of Telemedicine and Telecare; John Wiley & Sons, Ltd.: Chichester, UK, 2001. [Google Scholar]
- Darkins, A.W.; Cary, M.A. Telemedicine and telehealth: Principles, policies, performance, and pitfalls; Springer: New York, NY, USA, 2000. [Google Scholar]
- Eren, H.; Webster, J.G. The e-medicine, e-health, m-health, telemedicine, and telehealth handbook; CRC Press: Boca Raton, FL, USA, 2015. [Google Scholar]
- Burg, G. Telemedicine and teledermatology; Karger: Basel, Switzerland, 2003. [Google Scholar]
- Gott, M.; European Foundation for the Improvement of Living and Working. Telematics for Health: The Role of Telehealth and Telemedicine in Home and Communities; CRC Press: Boca Raton, FL, USA, 1995. [Google Scholar]
- Berner, E.S. Clinical decision support systems: Theory and practice; Springer: New York, NY, USA, 2007. [Google Scholar]
- Castillejo, J.A.P. Telemedicina, una herramienta también para el médico de familia. Atención Primaria 2013, 45, 129–132. [Google Scholar] [CrossRef] [Green Version]
- Papadakis, M.A.; Mcphee, S.J. Current Medical Diagnosis & Treatment; McGraw-Hill Education: New York, NY, USA, 2019. [Google Scholar]
- Dziedzic, M.E. Fast Facts about Pressure Ulcer Care for Nurses: How to Prevent, Detect, and Resolve Them in a Nutshell; Springer: New York, NY, USA, 2013. [Google Scholar]
- Maklebust, J. Preventing pressure ulcers in home care patients. Home Healthc. Nurse 1999, 17, 229–237. [Google Scholar] [CrossRef]
- Fernández, F.P.G.; Hidalgo, P.L.P.; Ágreda, J.J.S.; García, C.B. Pressure ulcer risk assessment scales. Gerokomos 2008, 19, 136–144. [Google Scholar]
- Wake, W.T. Pressure Ulcers: What Clinicians Need to Know. Perm. J. 2010, 14, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burstein, F.; Holsapple, C.W. Handbook on Decision Support. Systems 1; Springer: Berlin, Germany, 2008. [Google Scholar]
- Burstein, F.; Holsapple, C.W. Handbook on Decision Support. Systems 2; Springer: Berlin, Germany, 2008. [Google Scholar]
- Bonczek, R.H.; Holsapple, C.W.; Whinston, A.B.; Schmidt, J.W. Foundations of Decision Support. Systems; Academic Press: New York, NY, USA, 1981. [Google Scholar]
- Hevner, A.R.; Chatterjee, S. Design Research in Information Systems: Theory and Practice; Springer: New York, NY, USA, 2010. [Google Scholar]
- Pfeifer, R.; Lüthi, H.J. Decision Support Systems and Expert Systems: A Complementary Relationship? In Expert Systems and Artificial Intelligence in Decision Support Systems; Sol, H.G., Takkenberg, C.A.T., De Vries Robbé, P.F., Eds.; Springer: Dordrecht, The Netherlands, 1987; pp. 41–51. [Google Scholar]
- Lucas, P.; van der Gaag, L. Principles of Expert Systems; Addison-Wesley: Wokingham, UK, 1991. [Google Scholar]
- Krishnamoorthy, C.S.; Rajeev, S. Artificial Intelligence and Expert Systems for Engineers; CRC Press: Boca Raton, FL, USA, 1996. [Google Scholar]
- Liao, S.H. Expert system methodologies and applications-a decade review from 1995 to 2004. Expert Syst. Appl. 2005, 28, 93–103. [Google Scholar] [CrossRef]
- Kumar, Y.; Jain, Y. Research Aspects of Expert System. Int. J. Comput. Bus. Res. 2012, 1, 11. [Google Scholar]
- Merritt, D. Building Expert Systems in Prolog; Springer: New York, NY, USA, 1989. [Google Scholar]
- Marston, M.; Allen, J.; Mistree, F. The decision support problem technique: Integrating descriptive and normative approaches in decision based design. Eng. Valuat. Cost Anal. 2000, 3, 107–129. [Google Scholar]
- Allen, J.K.; Seepersad, C.C.; Choi, H.J.; Panchal, J.H.; McDowell, D.L.; Mistree, F. Decision Making in Engineering Design. In Integrated Design of Multiscale, Multifunctional Materials and Products; Elsevier: Burlington, MA, USA, 2010; pp. 65–86. [Google Scholar]
- Mistree, F.; Smith, W.F.; Bras, B.; Allen, J.K.; Muster, D. Decision-based Design: A Contemporary Paradigm for Ship Design. Trans. Soc. Nav. Archit. Mar. Eng. 1990, 98, 565–597. [Google Scholar]
- Chien, C.F.; Kim, K.H.; Liu, B.; Gen, M. Advanced decision and intelligence technologies for manufacturing and logistics. J. Intell. Manuf. 2012, 23, 2133–2135. [Google Scholar] [CrossRef] [Green Version]
- Hazelrigg, G.A. A Framework for Decision-Based Engineering Design. J. Mech. Des. 1998, 120, 653–658. [Google Scholar] [CrossRef]
- Lewis, K.; Chen, W.; Schmidt, L. Decision Making in Engineering Design; Asme Press: New York, NY, USA, 2006. [Google Scholar]
- Myers, W. Introduction to Expert Systems. IEEE Expert 1986, 1, 100–109. [Google Scholar] [CrossRef]
- Buchanan, B.G. Expert systems: Working systems and the research literature. Expert Syst. 1986, 3, 32–50. [Google Scholar] [CrossRef]
- Todd, B.S. An Introduction to Expert Systems; Oxford University Computing Laboratory: Oxford, UK, 1992. [Google Scholar]
- Grosan, C.; Abraham, A. Rule-Based Expert Systems. In Intelligence System Reference Library; Springer: Berlin, Germany, 2011; pp. 149–185. [Google Scholar]
- Berzal, F. Redes Neuronales & Deep Learning; Independently Published: Granada, Spain, 2018. [Google Scholar]
- Jackson, P. Introduction to Expert Systems; Addison-Wesley Publishing Co., Inc: Wokingham, UK, 1986. [Google Scholar]
- Leondes, C.T. Expert Systems The Technology of Knowledge Management and Decision Making for the 21st Century; Academic Press: San Diego, CA, USA, 2002. [Google Scholar]
- Hevner, A.R.; March, S.T.; Park, J.; Ram, S. Design science in information systems research. MIS Q. Manag. Inf. Syst. 2004, 28, 75–105. [Google Scholar] [CrossRef] [Green Version]
- Rienhoff, O.; Piccolo, U.; Schneider, B. Expert Systems and Decision Support. in Medicine; Lecture Notes in Medical Informatics; Reichertz, P.L., Lindberg, D.A.B., Eds.; Springer: Berlin, Germany, 1988; Volume 36. [Google Scholar]
- Kim, H.M.; Lowery, J.C.; Hamill, J.B.; Wilkins, E.G. Accuracy of a web-based system for monitoring chronic wounds. Telemed. J. e-Health 2003, 9, 129–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosmopoulos, D.I.; Tzevelekou, F.L. Automated pressure ulcer lesion diagnosis for telemedicine systems. IEEE Eng. Med. Biol. Mag. 2007, 26, 18–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowery, J.C.; Hamill, J.B.; Wilkins, E.G.; Clements, E. Technical Overview of a Web-based Telemedicine System for Wound Assessment. Adv. Ski. Wound Care 2002, 15, 165–169. [Google Scholar] [CrossRef]
- Goh, Z.; Goh, L.J.; Zhu, X. Effectiveness of Telemedicine for Distant Wound Care Advice towards Patient Outcomes: Systematic Review and Meta-Analysis. Int. Arch. Nurs. Health Care 2017, 3, 70. [Google Scholar] [CrossRef]
- Halstead, L.S.; Dang, T.; Elrod, M.; Convit, R.J.; Rosen, M.J.; Woods, S. Teleassessment compared with live assessment of pressure ulcers in a wound clinic: A pilot study. Adv. Skin Wound Care 2003, 16, 91–96. [Google Scholar] [CrossRef]
- Binder, B.; Hofmann-Wellenhof, R.; Salmhofer, W.; Okcu, A.; Kerl, H.; Soyer, H.P. Teledermatological monitoring of leg ulcers in cooperation with home care nurses. Arch. Dermatol. 2007, 143, 1511–1514. [Google Scholar] [CrossRef] [Green Version]
- Braun, R.P.; Vecchietti, J.L.; Thomas, L.; Prins, C.; French, L.E.; Gewirtzman, A.J.; Saurat, J.H.; Salomon, D. Telemedical wound care using a new generation of mobile telephones: A feasibility study. Arch. Dermatol. 2005, 141, 254–258. [Google Scholar] [CrossRef] [Green Version]
- Hofmann-Wellenhof, R.; Salmhofer, W.; Binder, B.; Okcu, A.; Kerl, H.; Soyer, H.P. Feasibility and acceptance of telemedicine for wound care in patients with chronic leg ulcers. J. Telemed. Telecare 2006, 12, 15–17. [Google Scholar] [CrossRef]
- Braden, B.J.; Maklebust, J.; Maklebust, J. Preventing pressure ulcers with the Braden scale: An update on this easy-to-use tool that assesses a patient’s risk. Am. J. Nurs. 2005, 105, 70–72. [Google Scholar] [CrossRef]
- Matlab Image Processing Toolbox Documentation. Available online: https://www.mathworks.com/help/images/index.html?s_tid=CRUX_lftnav (accessed on 29 May 2020).
- Kroon, D.J. Region Growing-File Exchange-MATLAB Central. Available online: https://www.mathworks.com/matlabcentral/fileexchange/19084-regiongrowing?focused=5098324&tab=function (accessed on 29 May 2020).
- Mamdani, E.H.; Assilian, S. An experiment in linguistic synthesis with a fuzzy logic controller. Int. J. Man. Mach. Stud. 1975, 7, 1–13. [Google Scholar] [CrossRef]
- Mamdani, E.H. Advances in the linguistic synthesis of fuzzy controllers. Int. J. Man. Mach. Stud. 1976, 8, 669–678. [Google Scholar] [CrossRef]
- Mamdani, E.H. Application of fuzzy logic to approximate reasoning using linguistic synthesis. Comput. IEEE Trans. 1977, 26, 1182–1191. [Google Scholar] [CrossRef]
- Ross, T.J. Fuzzy Logic. with Engineering Applications, 3rd ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2010. [Google Scholar]
- Zadeh, L.A. Fuzzy Set. Inf. Control. 1965, 8, 338–353. [Google Scholar] [CrossRef] [Green Version]
- Zadeh, L.A. The concept of a linguistic variable and its application to approximate reasoning-I. Inf. Sci. 1975, 8, 199–249. [Google Scholar] [CrossRef]
- Sambariya, D.K.; Prasad, R. Selection of Membership Functions Based on Fuzzy Rules to Design an Efficient Power System Stabilizer. Int. J. Fuzzy Syst. 2017, 19, 813–828. [Google Scholar] [CrossRef]
- Starczewski, J.T. Defuzzification of Uncertain Fuzzy Sets. In Advanced Concepts in Fuzzy Logic and Systems with Membership Uncertainty; Springer: Berlin, Germany, 2013; pp. 77–135. [Google Scholar]
- Sugeno, M. An introductory survey of fuzzy control. Inf. Sci. 1985, 36, 59–83. [Google Scholar] [CrossRef]
- Billo, E.J. Excel for Scientists and Engineers: Numerical Methods; Wiley-Interscience: Hoboken, NJ, USA, 2007. [Google Scholar]
- Fuzzy Logic Toolbox-MATLAB. Available online: https://www.mathworks.com/products/fuzzy-logic.html (accessed on 29 May 2020).
- MATLAB-MathWorks-MATLAB & Simulink. Available online: https://www.mathworks.com/products/matlab.html (accessed on 29 May 2020).


























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Follow-up of the Monitoring and Assessment Stages within the Pressure Ulcers (PU) Treatment Process | ||
|---|---|---|
| Design needs for the artifact | Technical requirements | Restrictions associated to the environment |
| It must include a device to register information about the patient’s health status, regardless of her location | Mobile device with wireless data connectivity, screen, camera, keyboard and data templates | Mobile data service available at the patient’s location |
| It must have the ability to capture images of the wounds | ||
| It must have the ability to transmit the information collected, as well as to receive information and upload it to the information system | ||
| It must have the ability to manage the information about all the visits of the healthcare team to the patient, recorded on a historian | Graphical user interface | Visibility and resolution conditions of the graphic elements |
| It must have the ability to detect if the wounds under control increase or decrease its size in the period between visits | Image processing and subsequent calculations derived from said processing | Image control and quality |
| It must provide a metric corresponding to the global patient’s status, associated to the evaluation of the medical treatment | Braden, or similar, scale | Homogeneity in the assessment of the scale score by different healthcare professionals |
| It must make available all the information stored in the system, as well as any other coming from the treatments applied to the patient after the healthcare team | Computer equipment and software application with healthcare templates | IT support |
| It must combine the expert evaluations with the rest of the process information in the system | Expert systems that combine data coming from devices and data from healthcare assessment | |
| It must allow the processing of the information collected by the devices together with the evaluations of the expert establishing, based on them, recommendations regarding the treatment that the patient is currently undergoing | ||
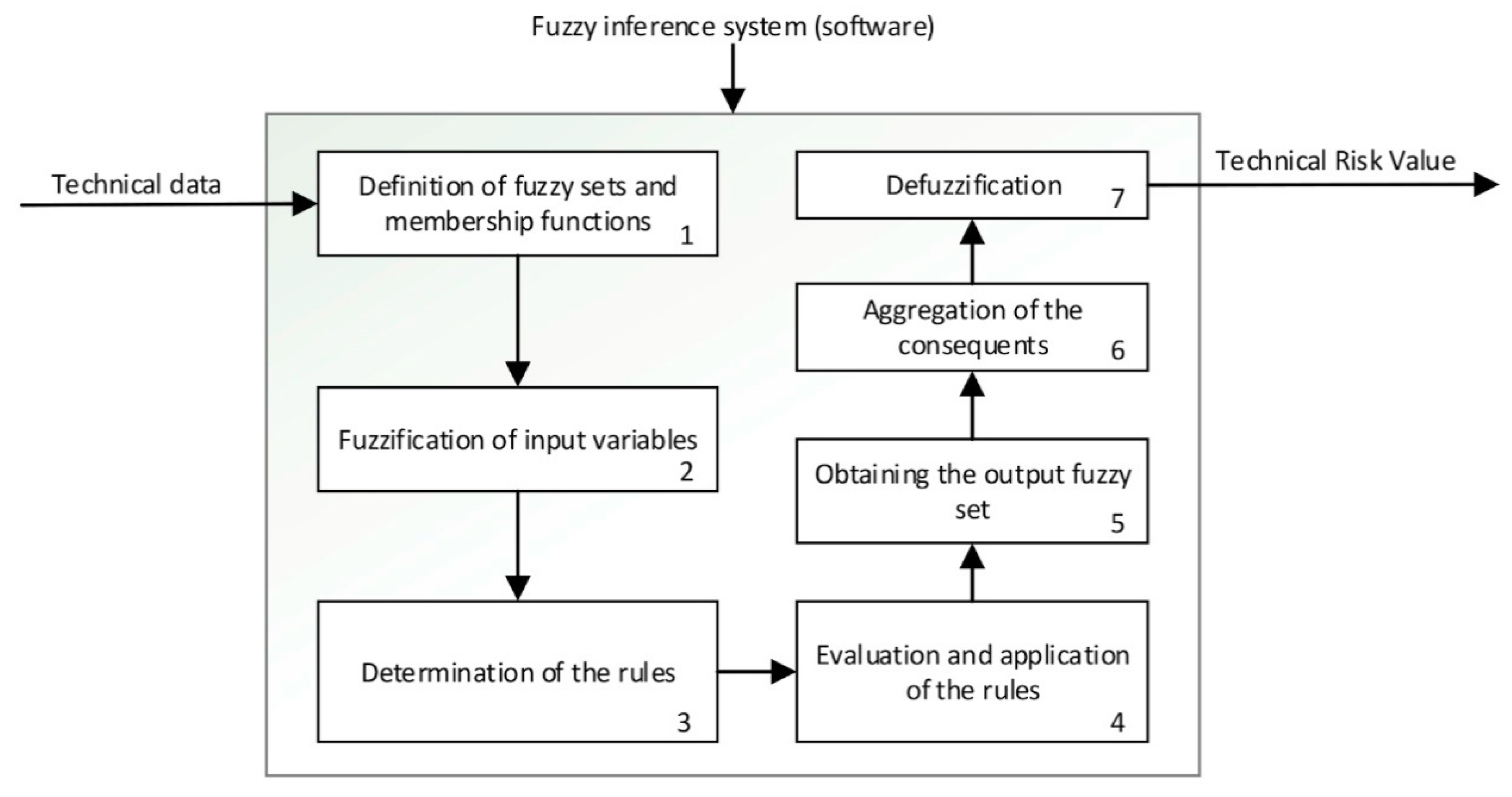
| Point | Step | Description |
|---|---|---|
| 1 | Definition of the fuzzy sets and the membership functions See Figure 6-Step 1 | Firstly, the different fuzzy sets and the respective membership functions for each input variable of the system are established [62,63,64,65]. These functions make it possible to determine the degree of membership of a certain value to a specific set in the range from zero to one. This is equivalent, respectively, to not belonging at all, or fully belonging to, the qualitative trait that represents the section of the membership function. Trapezoidal functions have been chosen for this, since they make it possible to maximize the degree of belonging to a set within a continuous range of values. |
| 2 | Fuzzification of input variables See Figure 6-Step 2 | The fuzzification process of the input variables makes possible to determine the degree of membership (in the range from zero to one) of a specific value, associated with a certain input variable, within a certain fuzzy set. |
| 3 | Determination of the rules See Figure 6-Step 3 | After the fuzzy sets and the membership functions have been determined, and the fuzzification process of the input variables has been carried out, then the rules governing the behavior of the system are established. These rules allow to perform the combination of the antecedents, that is of the input values, by using fuzzy operators of the ‘AND’ and ‘OR’ types. After this, combinations of the ‘IF’… ‘AND’/‘OR’… ‘THEN’ … types are carried out, allowing to connect the input values with the consequents, i.e., the outputs of the system. |
| 4 | Evaluation and application of the rules See Figure 6-Step 4 | After performing the previous steps described in this table, it is possible to apply the fuzzy operators. There are different methods for their application [62]. The ‘AND’ operator will be used with the ‘intersection’ fuzzy operator and the ‘OR’ operator with the ‘union’ one, also equivalent to the ‘minimum’ and ‘maximum’ operators, respectively. When the ‘AND’ connector is used to connect two membership functions, the minimum of their membership degrees is returned, while in the case of the operator ‘OR’ the maximum one is returned. |
| 5 | Obtaining the output fuzzy set See Figure 6-Step 5 | After evaluating and applying the rules, the consequent of these rules is determined by using the implication method [62]. The minimum is chosen in this case, which is translated into a truncation of the consequent’s membership function, that has been previously defined as a fuzzy set based on the value obtained from the fuzzy operation. |
| 6 | Aggregation of consequents See Figure 6-Step 6 | After evaluating all the rules and obtaining their individual consequents, the global consequent (representative of the risk) is determined. |
| 7 | Defuzzification See Figure 6-Step 7 | Finally, a numerical value for the risk level is obtained by applying the centroid method [62,66,67]. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casal-Guisande, M.; Comesaña-Campos, A.; Cerqueiro-Pequeño, J.; Bouza-Rodríguez, J.-B. Design and Development of a Methodology Based on Expert Systems, Applied to the Treatment of Pressure Ulcers. Diagnostics 2020, 10, 614. https://doi.org/10.3390/diagnostics10090614
Casal-Guisande M, Comesaña-Campos A, Cerqueiro-Pequeño J, Bouza-Rodríguez J-B. Design and Development of a Methodology Based on Expert Systems, Applied to the Treatment of Pressure Ulcers. Diagnostics. 2020; 10(9):614. https://doi.org/10.3390/diagnostics10090614
Chicago/Turabian StyleCasal-Guisande, Manuel, Alberto Comesaña-Campos, Jorge Cerqueiro-Pequeño, and José-Benito Bouza-Rodríguez. 2020. "Design and Development of a Methodology Based on Expert Systems, Applied to the Treatment of Pressure Ulcers" Diagnostics 10, no. 9: 614. https://doi.org/10.3390/diagnostics10090614