Nanoparticle-Based Biosensing Assay for Universally Accessible Low-Cost TB Detection with Comparable Sensitivity as Culture

 ,
,
Abstract
:1. Introduction
1.1. Constraints of Current Methods
1.2. Novelty of the Paper
1.3. Novelty of the MACE Technique
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. Instrumentation
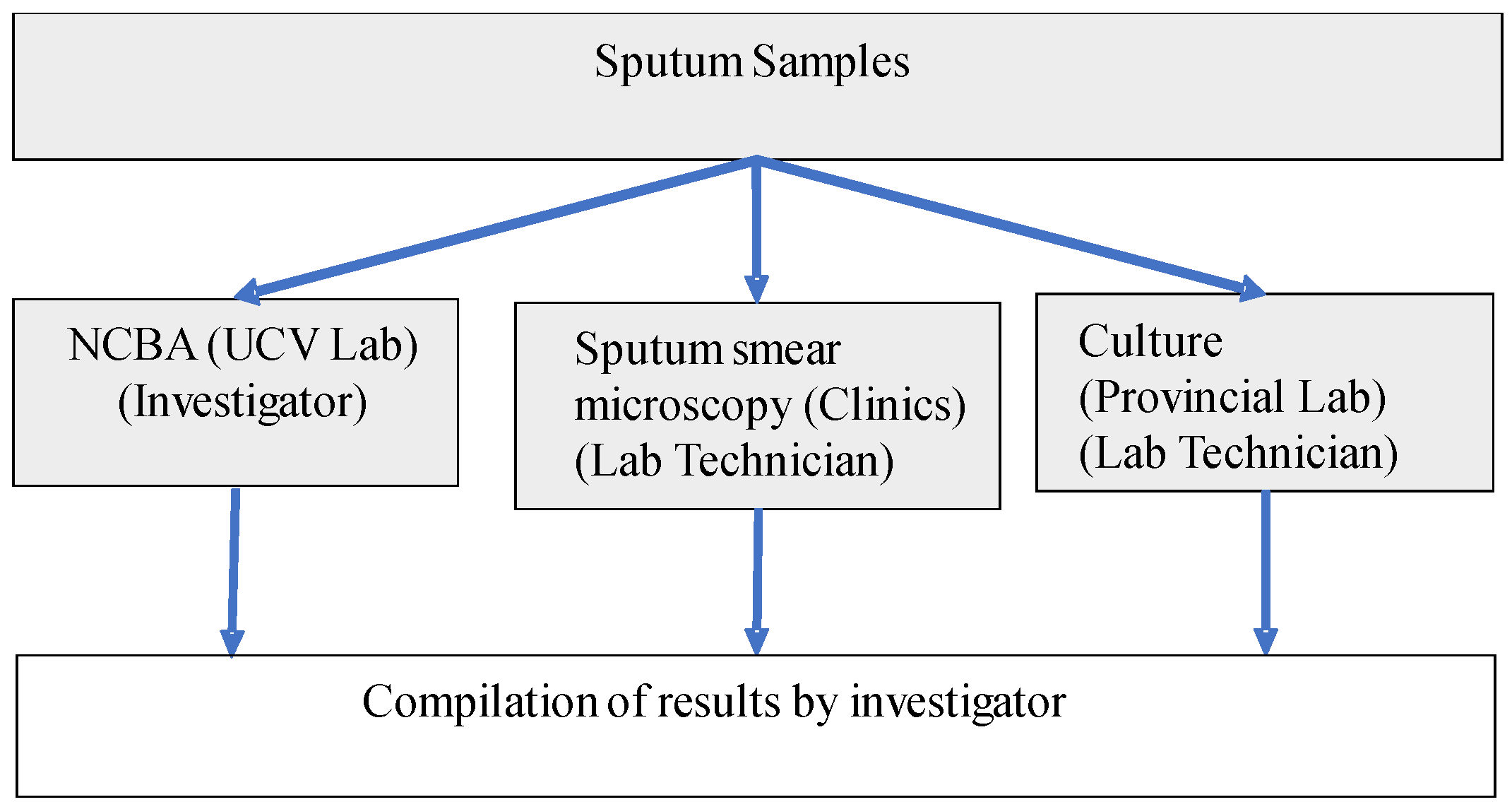
2.3. Clinical Samples
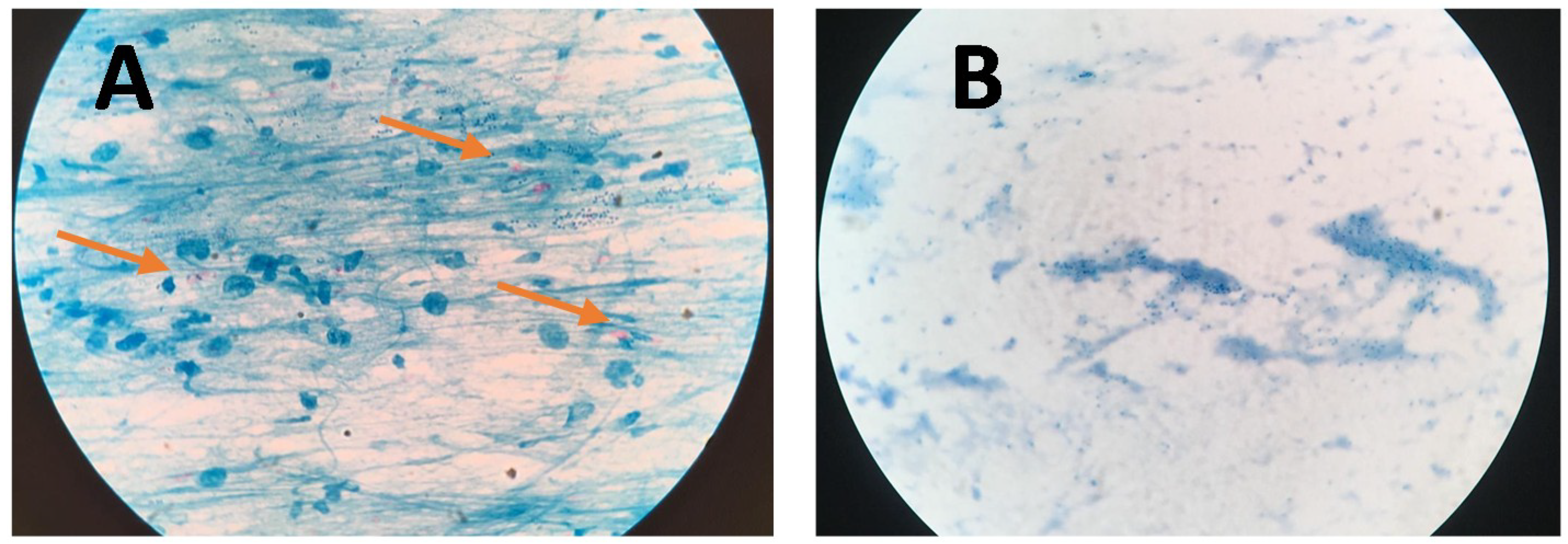
2.4. Sputum Smear Microscopy (SSM) by Ziehl–Neelsen Staining
2.5. Standard Culture by the Lowenstein-Jensen Method
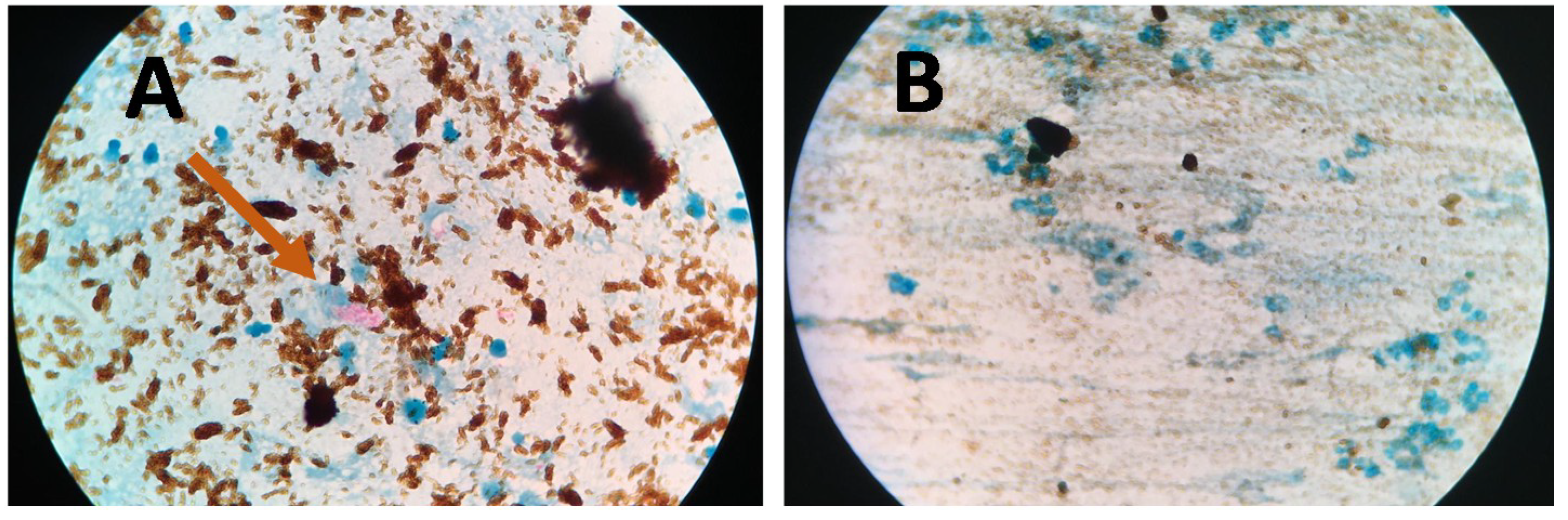
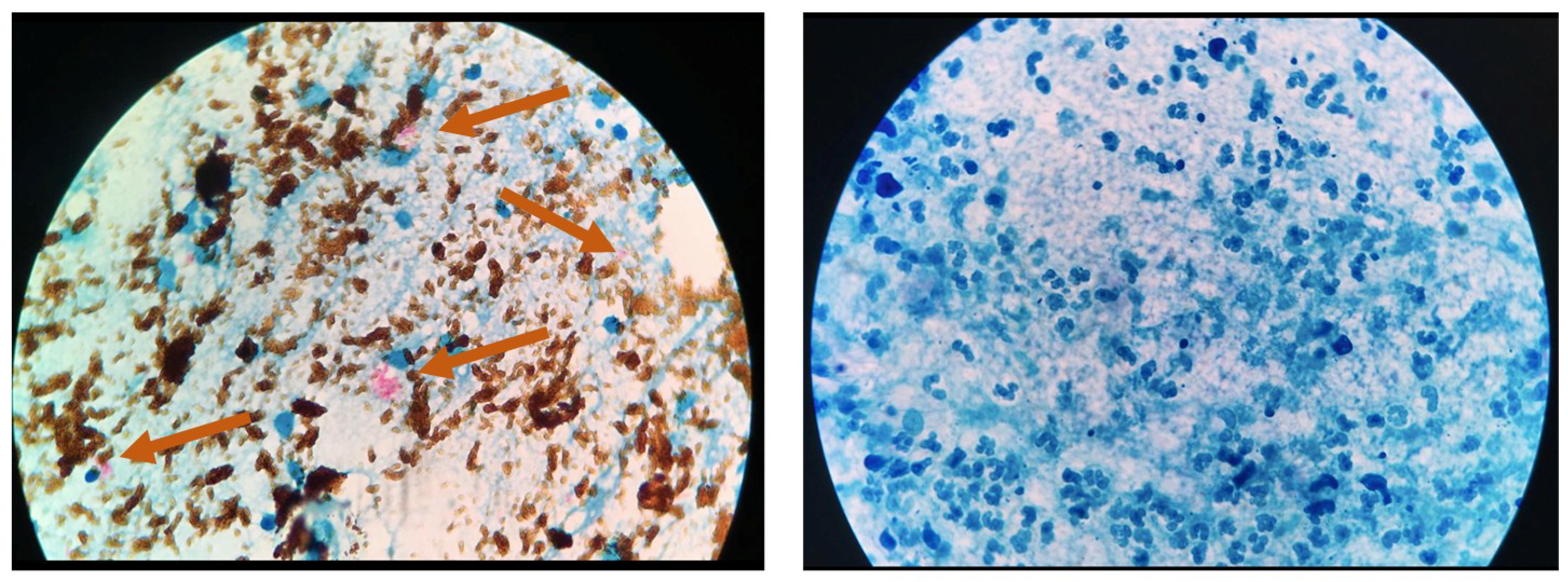
2.6. Nanoparticle-Based Colorimetric Biosensing Assay (NCBA)
2.7. Mathematical Modeling of the Mtb Population
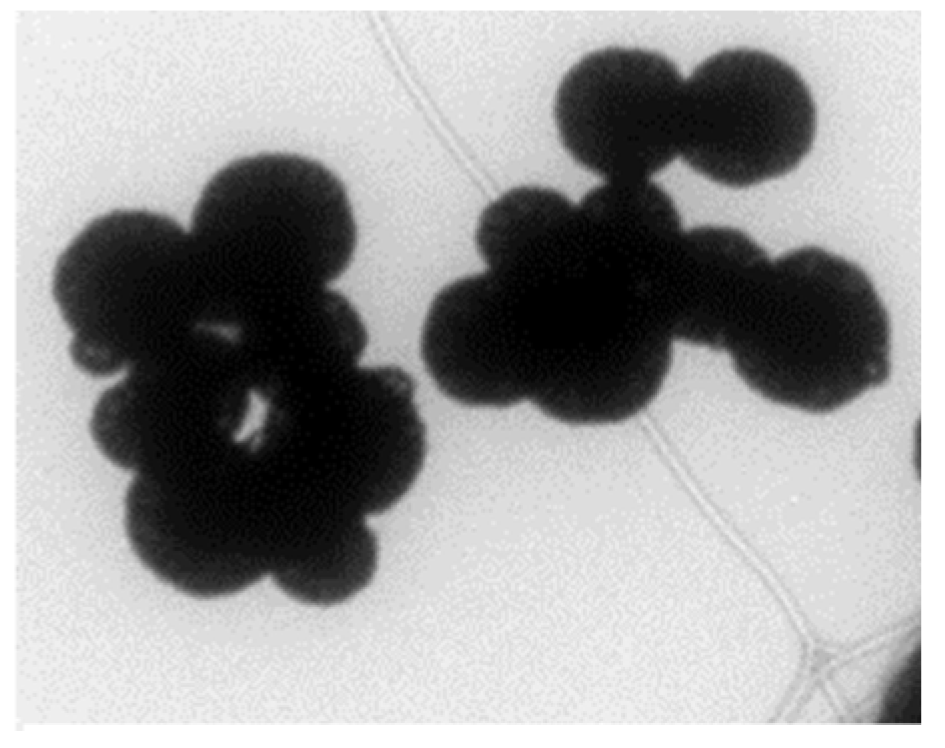
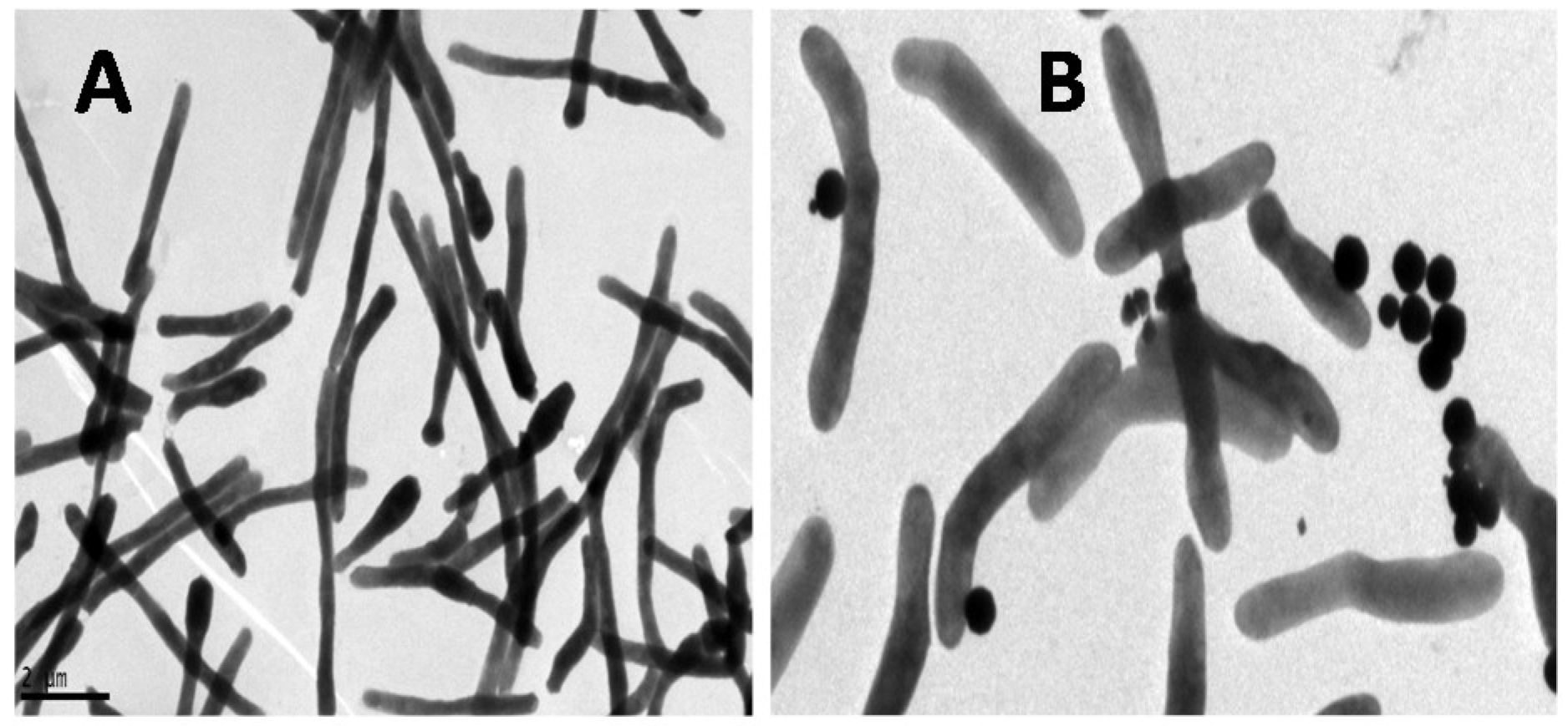
2.8. GMNP-Cell Interaction for Transmission Electron Microscope (TEM) Imaging
2.9. Ethics
3. Results
3.1. GMNP
3.2. GMNP-Cells
3.3. Clinical Samples
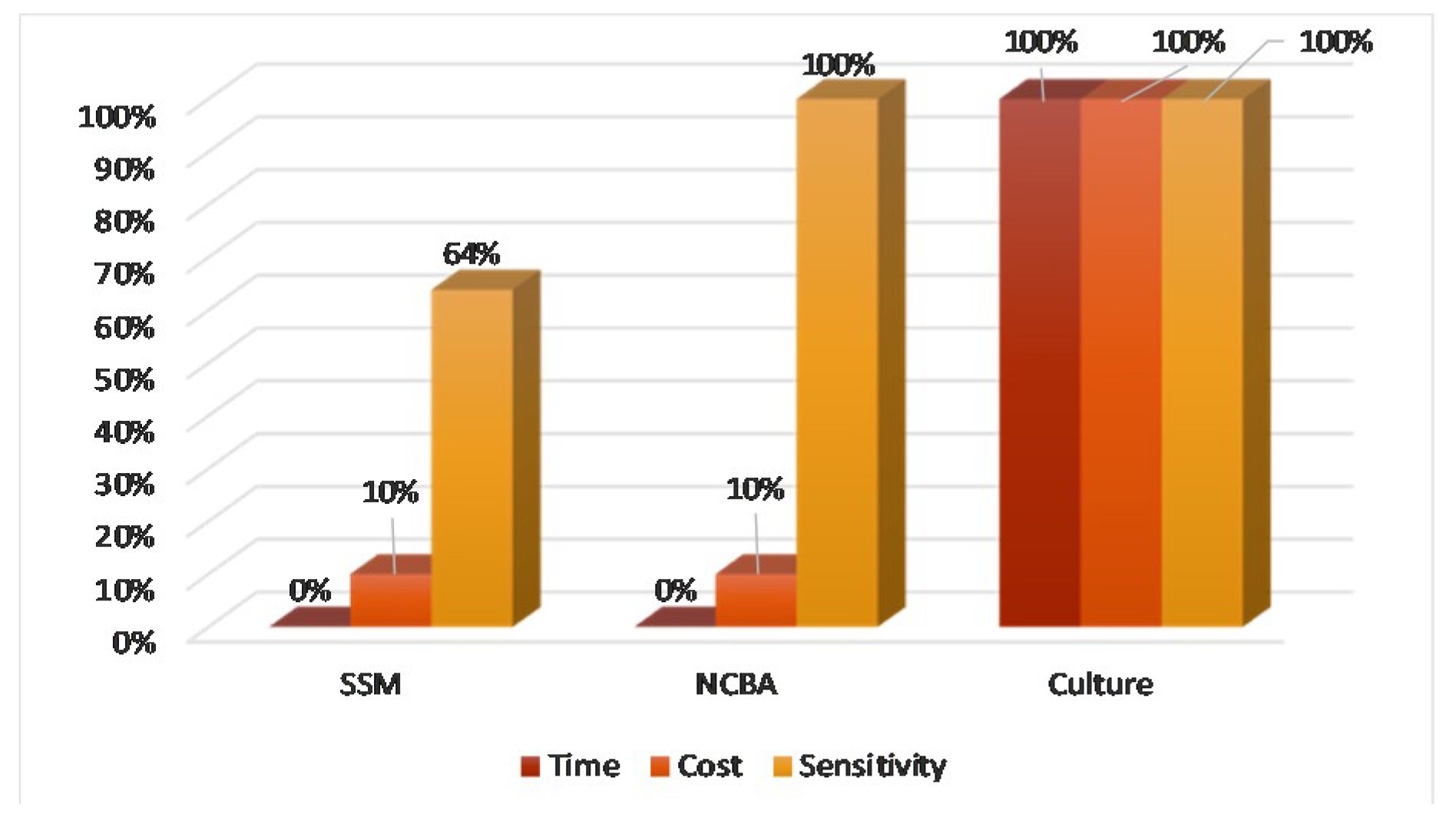
3.4. NCBA vs. SSM vs. Culture
4. Discussion
4.1. Mechanism of GMNP-Cell Interaction
4.2. NCBA v.s SSM vs. Culture
4.3. NCBA for TB Incidence
4.4. NCBA for Detection of Early Onset of Disease
4.5. NCBA to Profile TB Population
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- TB statistics | Incidence, prevalence, high burden. TB Facts |TB Tests Drugs Stat. Available online: https://tbfacts.org/tb-statistics/ (accessed on 11 December 2019).
- Parsons, L.M.; Somoskövi, Á.; Gutierrez, C.; Lee, E.; Paramasivan, C.N.; Abimiku, A.; Spector, S.; Roscigno, G.; Nkengasong, J. Laboratory Diagnosis of Tuberculosis in Resource-Poor Countries: Challenges and Opportunities. Clin. Microbiol. Rev. 2011, 24, 314–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, T.; Zhong, J.; Zhang, J.; Li, C.; Yu, X.; Xiao, J.; Jia, X.; Ding, N.; Ma, G.; Wang, G.; et al. Pan-Genomic Study of Mycobacterium tuberculosis Reflecting the Primary/Secondary Genes, Generality/Individuality, and the Interconversion Through Copy Number Variations. Front. Microbiol. 2018, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakamoto, H.; Lee, S.; Ishizuka, A.; Hinoshita, E.; Hori, H.; Ishibashi, N.; Komada, K.; Norizuki, M.; Katsuma, Y.; Akashi, H.; et al. Challenges and opportunities for eliminating tuberculosis – leveraging political momentum of the UN high-level meeting on tuberculosis. BMC Public Health 2019, 19, 76. [Google Scholar] [CrossRef] [PubMed]
- Tuberculosis in Developing Countries. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/00001729.htm (accessed on 18 September 2019).
- Mehaffy, C.; Belisle, J.T.; Dobos, K.M. Mycobacteria and their sweet proteins: An overview of protein glycosylation and lipoglycosylation in M. tuberculosis. Tuberculosis 2019, 115, 1–13. [Google Scholar] [CrossRef] [PubMed]
- MacNeil, A. Global Epidemiology of Tuberculosis and Progress Toward Achieving Global Targets — 2017. MMWR Morb. Mortal. Wkly. Rep. 2019, 68. [Google Scholar] [CrossRef] [Green Version]
- Issues and threats of Tuberculosis in Nepal | Connecting our members with evidence and expertise. Available online: https://www.ghdonline.org/ic/discussion/issues-and-threats-of-tuberculosis-in-nepal/ (accessed on 1 May 2018).
- Hobby, G.L.; Holman, A.P.; Iseman, M.D.; Jones, J.M. Enumeration of Tubercle Bacilli in Sputum of Patients with Pulmonary Tuberculosis. Antimicrob. Agents Chemother. 1973, 4, 94–104. [Google Scholar] [CrossRef] [Green Version]
- Steingart, K.R.; Ng, V.; Henry, M.; Hopewell, P.C.; Ramsay, A.; Cunningham, J.; Urbanczik, R.; Perkins, M.D.; Aziz, M.A.; Pai, M. Sputum processing methods to improve the sensitivity of smear microscopy for tuberculosis: a systematic review. Lancet Infect. Dis. 2006, 6, 664–674. [Google Scholar] [CrossRef]
- Desikan, P. Sputum smear microscopy in tuberculosis: Is it still relevant? Indian J. Med. Res. 2013, 137, 442–444. [Google Scholar]
- Olaru, I.D.; Heyckendorf, J.; Grossmann, S.; Lange, C. Time to Culture Positivity and Sputum Smear Microscopy during Tuberculosis Therapy. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [Green Version]
- Demers, A.-M.; Verver, S.; Boulle, A.; Warren, R.; van Helden, P.; Behr, M.A.; Coetzee, D. High yield of culture-based diagnosis in a TB-endemic setting. BMC Infect. Dis. 2012, 12, 218. [Google Scholar] [CrossRef] [Green Version]
- Afsar, I.; Gunes, M.; Er, H.; Sener, A.G. Comparison of culture, microscopic smear and molecular methods in diagnosis of tuberculosis. Rev. Esp. Quimioter. 2018, 31, 435–438. [Google Scholar] [PubMed]
- Kik, S.V.; Denkinger, C.M.; Chedore, P.; Pai, M. Replacing smear microscopy for the diagnosis of tuberculosis: what is the market potential? Eur. Respir. J. 2014, 43, 1793–1796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashif Munir, M.; Shabbir, I.; Iqbal, R.; Ullah Khan, S. Comparison of detection of Acid Fast Bacilli in clinical samples by AFB Smear microscopy and Culture in the diagnosis of Tuberculosis in a tertiary care setting. Pak J Che Med 2009, 15, 14–18. [Google Scholar]
- Das, S.; Narang, P.; Nagamiah, S.; Mishra, P.S.; Deotale, V.; Mendiratta, D.K. Evaluation of variants of carbol fuchsin solution to stain acid-fast bacilli in-situ by the pot method. Available online: https://www.ingentaconnect.com/content/iuatld/ijtld/2015/00000019/00000012/art00012%3bjsessionid=cb82amdbsq0bt.x-ic-live-03# (accessed on 30 September 2019).
- Shea, Y.R.; Davis, J.L.; Huang, L.; Kovacs, J.A.; Masur, H.; Mulindwa, F.; Opus, S.; Chow, Y.; Murray, P.R. High Sensitivity and Specificity of Acid-Fast Microscopy for Diagnosis of Pulmonary Tuberculosis in an African Population with a High Prevalence of Human Immunodeficiency Virus. J. Clin. Microbiol. 2009, 47, 1553–1555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, V.; Nicol, M.P.; Tow, L.A. Sputum processing prior to Mycobacterium tuberculosis detection by culture or nucleic acid amplification testing: a narrative review. Res. Rev. J. Microbiol. Biotechnol. 2016, 5, 120–130. [Google Scholar]
- Ho, J.; Marks, G.B.; Fox, G.J. The impact of sputum quality on tuberculosis diagnosis: a systematic review. Int. J. Tuberc. Lung Dis. 2015, 19, 537–544. [Google Scholar] [CrossRef]
- Nathavitharana, R.R.; Cudahy, P.G.T.; Schumacher, S.G.; Steingart, K.R.; Pai, M.; Denkinger, C.M. Accuracy of line probe assays for the diagnosis of pulmonary and multidrug-resistant tuberculosis: a systematic review and meta-analysis. Eur. Respir. J. 2017, 49. [Google Scholar] [CrossRef]
- Rufai, S.B.; Kumar, P.; Singh, A.; Prajapati, S.; Balooni, V.; Singh, S. Comparison of Xpert MTB/RIF with Line Probe Assay for Detection of Rifampin-Monoresistant Mycobacterium tuberculosis. J. Clin. Microbiol. 2014, 52, 1846–1852. [Google Scholar] [CrossRef] [Green Version]
- Desikan, P.; Panwalkar, N.; Mirza, S.B.; Chaturvedi, A.; Ansari, K.; Varathe, R.; Chourey, M.; Kumar, P.; Pandey, M. Line probe assay for detection of Mycobacterium tuberculosis complex: An experience from Central India. Indian J. Med. Res. 2017, 145, 70–73. [Google Scholar] [CrossRef]
- Hillemann, D.; Rüsch-Gerdes, S.; Boehme, C.; Richter, E. Rapid Molecular Detection of Extrapulmonary Tuberculosis by the Automated GeneXpert MTB/RIF System. J. Clin. Microbiol. 2011, 49, 1202–1205. [Google Scholar] [CrossRef] [Green Version]
- WHO | Xpert MTB/RIF - rapid TB test - WHO publishes policy and guidance for implementers. Available online: https://www.who.int/tb/features_archive/xpert_rapid_tb_test/en/ (accessed on 6 December 2019).
- Engel, N.; Wachter, K.; Pai, M.; Gallarda, J.; Boehme, C.; Celentano, I.; Weintraub, R. Addressing the challenges of diagnostics demand and supply: insights from an online global health discussion platform. BMJ Glob. Health 2016, 1, e000132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pantoja, A.; Fitzpatrick, C.; Vassall, A.; Weyer, K.; Floyd, K. Xpert MTB/RIF for diagnosis of tuberculosis and drug-resistant tuberculosis: a cost and affordability analysis. Eur. Respir. J. 2013, 42, 708–720. [Google Scholar] [CrossRef] [PubMed]
- Tanimura, T.; Jaramillo, E.; Weil, D.; Raviglione, M.; Lönnroth, K. Financial burden for tuberculosis patients in low- and middle-income countries: a systematic review. Eur. Respir. J. 2014, 43, 1763–1775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reed, J.L.; Basu, D.; Butzler, M.A.; McFall, S.M. XtracTB Assay, a Mycobacterium tuberculosis molecular screening test with sensitivity approaching culture. Sci. Rep. 2017, 7, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Floyd, K.; Glaziou, P.; Houben, R.M.G.J.; Sumner, T.; White, R.G.; Raviglione, M. Global tuberculosis targets and milestones set for 2016–2035: definition and rationale. Int. J. Tuberc. Lung Dis. 2018, 22, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Publicaciones de Análisis de Situación de Salud. Available online: https://www.dge.gob.pe/portal/index.php?option=com_content&view=article&id=255%20&Itemid=105 (accessed on 23 October 2019).
- WHO | Global tuberculosis report 2019. Available online: http://www.who.int/tb/publications/global_report/en/ (accessed on 23 October 2019).
- Gordillo-Marroquín, C.; Gómez-Velasco, A.; Sánchez-Pérez, H.J.; Pryg, K.; Shinners, J.; Murray, N.; Muñoz-Jiménez, S.G.; Bencomo-Alerm, A.; Gómez-Bustamante, A.; Jonapá-Gómez, L.; et al. Magnetic Nanoparticle-Based Biosensing Assay Quantitatively Enhances Acid-Fast Bacilli Count in Paucibacillary Pulmonary Tuberculosis. Biosensors 2018, 8, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhusal, N.; Shrestha, S.; Pote, N.; Alocilja, E.C. Nanoparticle-Based Biosensing of Tuberculosis, an Affordable and Practical Alternative to Current Methods. Biosensors 2019, 9, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akbarzadeh, A.; Samiei, M.; Davaran, S. Magnetic nanoparticles: preparation, physical properties, and applications in biomedicine. Nanoscale Res. Lett. 2012, 7, 144. [Google Scholar] [CrossRef] [Green Version]
- Tuberculosis (TB). Available online: https://www.who.int/news-room/fact-sheets/detail/tuberculosis (accessed on 14 October 2019).
- gli_mycobacteriology_lab_manual_quadri.indd. 154. Available online: https://www.scribd.com/document/305681530/gli-mycobacteriology-lab-manual-web-pdf (accessed on 12 December 2019).
- Mohan, A.; Padiadpu, J.; Baloni, P.; Chandra, N. Complete Genome Sequences of a Mycobacterium smegmatis Laboratory Strain (MC2 155) and Isoniazid-Resistant (4XR1/R2) Mutant Strains. Genome Announc. 2015, 3. [Google Scholar]
- Tyagi, J.S.; Sharma, D. Mycobacterium smegmatis and tuberculosis. Trends Microbiol. 2002, 10, 68–69. [Google Scholar] [CrossRef]
- Ragas, A.; Roussel, L.; Puzo, G.; Rivière, M. The Mycobacterium tuberculosis Cell-surface Glycoprotein Apa as a Potential Adhesin to Colonize Target Cells via the Innate Immune System Pulmonary C-type Lectin Surfactant Protein A. J. Biol. Chem. 2007, 282, 5133–5142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boradia, V.M.; Malhotra, H.; Thakkar, J.S.; Tillu, V.A.; Vuppala, B.; Patil, P.; Sheokand, N.; Sharma, P.; Chauhan, A.S.; Raje, M.; et al. Mycobacterium tuberculosis acquires iron by cell-surface sequestration and internalization of human holo-transferrin. Nat. Commun. 2014, 5, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Stokes, R.W.; Norris-Jones, R.; Brooks, D.E.; Beveridge, T.J.; Doxsee, D.; Thorson, L.M. The Glycan-Rich Outer Layer of the Cell Wall of Mycobacterium tuberculosis Acts as an Antiphagocytic Capsule Limiting the Association of the Bacterium with Macrophages. Infect. Immun. 2004, 72, 5676–5686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daffé, M.; Draper, P. The Envelope Layers of Mycobacteria with Reference to their Pathogenicity. In Advances in Microbial Physiology; Poole, R.K., Ed.; Academic Press: Cambridge, MA, USA, 1997; Volume 39, pp. 131–203. [Google Scholar]
- Incidence of tuberculosis (per 100,000 people) | Data. Available online: https://data.worldbank.org/indicator/SH.TBS.INCD?name_desc=true (accessed on 25 October 2019).
- Figure 2. The slow road to diagnosis of pulmonary tuberculosis (TB)... Available online: https://www.researchgate.net/figure/The-slow-road-to-diagnosis-of-pulmonary-tuberculosis-TB-when-sputum-smear-microscopy-is_fig7_281642259 (accessed on 15 October 2019).
- James, B.W.; Williams, A.; Marsh, P.D. The physiology and pathogenicity of Mycobacterium tuberculosis grown under controlled conditions in a defined medium. J. Appl. Microbiol. 2000, 88, 669–677. [Google Scholar] [CrossRef] [PubMed]
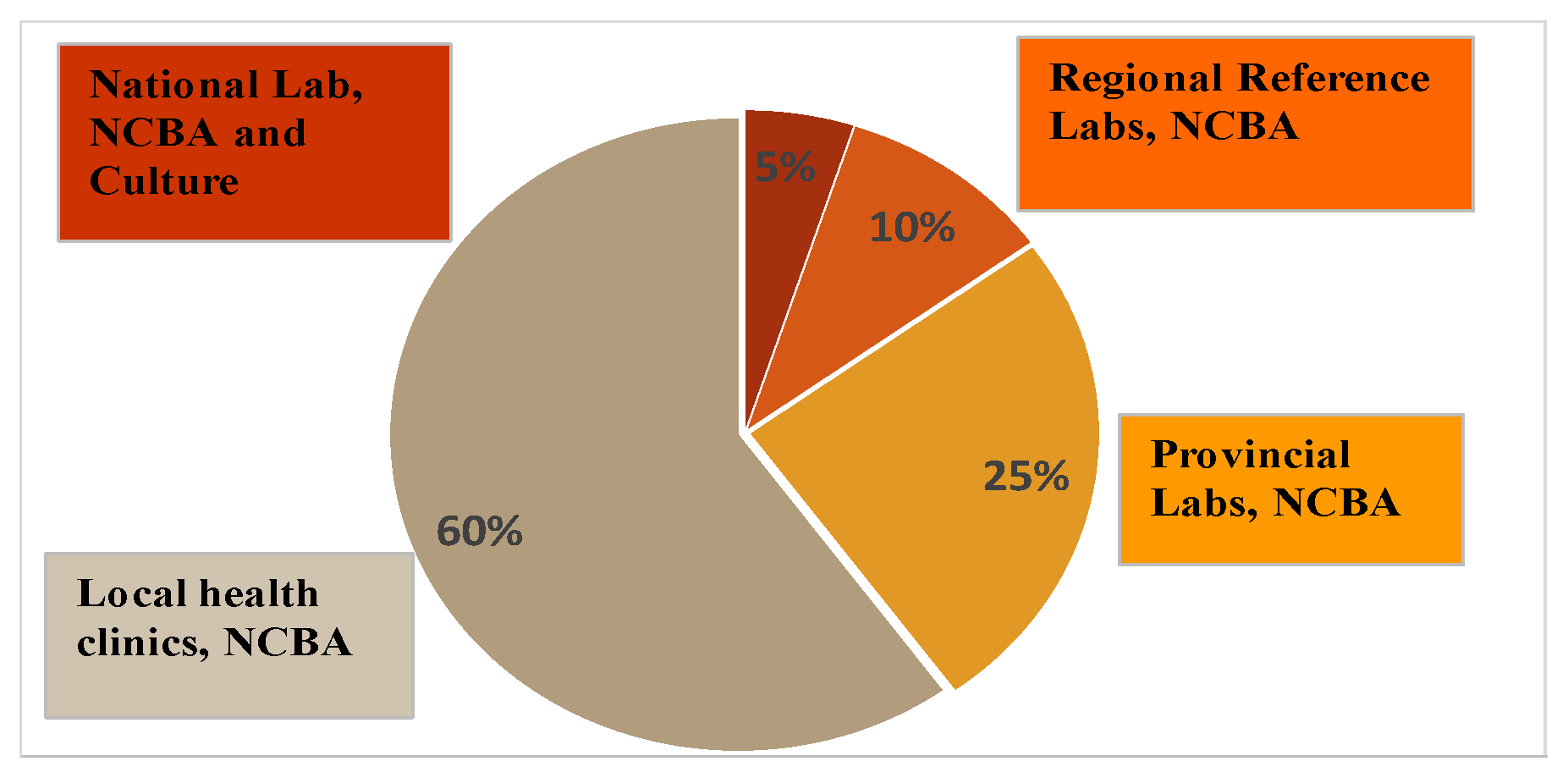
- Figure 4. Diagnostic needs at different health system levels. Available online: https://www.researchgate.net/figure/Diagnostic-needs-at-different-health-system-levels_fig8_281642259 (accessed on 17 October 2019).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| City # | No. Samples | SSM | NCBA | Culture | ||||
|---|---|---|---|---|---|---|---|---|
| No. | Fraction | Positive | Negative | Positive | Negative | Positive | Negative | |
| 1 | 98 | 9% | 15 | 83 | 18 | 80 | 17 | 81 |
| 2 | 119 | 11% | 9 | 110 | 13 | 106 | 13 | 106 |
| 3 | 213 | 19% | 36 | 177 | 50 | 163 | 50 | 163 |
| 4 | 72 | 6% | 6 | 66 | 11 | 61 | 11 | 61 |
| 5 | 58 | 5% | 11 | 47 | 21 | 37 | 21 | 37 |
| 6 | 123 | 11% | 22 | 101 | 36 | 87 | 36 | 87 |
| 7 | 82 | 7% | 5 | 77 | 10 | 72 | 9 | 73 |
| 8 | 153 | 14% | 13 | 140 | 25 | 128 | 25 | 128 |
| 9 | 190 | 17% | 5 | 185 | 10 | 180 | 9 | 181 |
| Total | 1108 | 100% | 122 | 986 | 194 | 914 | 191 | 917 |
| Sensitivity | Specificity | PPV | NPV | Accuracy | |
|---|---|---|---|---|---|
| SSM | 63.9% (56.6–70.7) | 100.0% (99.6–100.0) | 100.0% | 93.0% (91.7–94.1) | 93.8% (92.2–95.1) |
| NCBA | 100.0% (98.1–100.0) | 99.7% (99.1–99.9) | 98.5% (95.4–99.5) | 100.0% | 99.7% (99.2–99.9) |
| End of Month | Symptoms | Est. Mtb Load in Patient, CFU/mL | Detectable by SSM and Est. Grade? | Detectable by NCBA? | Detectable by Culture? |
|---|---|---|---|---|---|
| 1st | Not feeling well | 6.3 x100 | |||
| 2nd | Cough at night | 4.0 × 101 | No | Yes | Yes, result in 4th month |
| 3rd | Intense coughing | 2.5 × 102 | No | Yes | Yes, result in 5th month |
| 4th | Onset of hemoptoic cough or hemoptysis | 1.6 × 103 | No | Yes | Yes, result in 6th month |
| 5th | Onset of dyspnea | 9.1 × 103 | Yes, 1+ and 2+ | Yes | Yes, result in 7th month |
| 6th | Dyspnea | 3.9 × 104 | Yes, 3+ | Yes | Yes, result in 8th month |
| 7th | Dyspnea | 8.0 × 104 | Yes, 4+ | Yes | Yes, result in 9th month |
| City | No. Samples | SSM+ | NCBA+ | Culture+ | ||
|---|---|---|---|---|---|---|
| >104 (High) | 101–103 (Low) | >104 (High) | 101–103 (Low) | >104 (High) | ||
| 1 | 98 | 15% | 3% | 15% | 2% | 15% |
| 2 | 119 | 8% | 3% | 8% | 3% | 8% |
| 3 | 213 | 17% | 7% | 17% | 7% | 17% |
| 4 | 72 | 8% | 7% | 8% | 7% | 8% |
| 5 | 58 | 19% | 17% | 19% | 17% | 19% |
| 6 | 123 | 18% | 11% | 18% | 11% | 18% |
| 7 | 82 | 6% | 6% | 6% | 5% | 6% |
| 8 | 153 | 8% | 8% | 8% | 8% | 8% |
| 9 | 190 | 3% | 3% | 2% | 2% | 3% |
| Total | 1108 | 11% | 6% | 11% | 6% | 11% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Briceno, R.K.; Sergent, S.R.; Benites, S.M.; Alocilja, E.C. Nanoparticle-Based Biosensing Assay for Universally Accessible Low-Cost TB Detection with Comparable Sensitivity as Culture. Diagnostics 2019, 9, 222. https://doi.org/10.3390/diagnostics9040222
Briceno RK, Sergent SR, Benites SM, Alocilja EC. Nanoparticle-Based Biosensing Assay for Universally Accessible Low-Cost TB Detection with Comparable Sensitivity as Culture. Diagnostics. 2019; 9(4):222. https://doi.org/10.3390/diagnostics9040222
Chicago/Turabian StyleBriceno, Ruben Kenny, Shane Ryan Sergent, Santiago Moises Benites, and Evangelyn C. Alocilja. 2019. "Nanoparticle-Based Biosensing Assay for Universally Accessible Low-Cost TB Detection with Comparable Sensitivity as Culture" Diagnostics 9, no. 4: 222. https://doi.org/10.3390/diagnostics9040222