
Design and Definition of a New Decision Support System Aimed to the Hierarchization of Patients Candidate to Be Admitted to Intensive Care Units

 , , and
, , and
Abstract
:1. Introduction
1.1. General Triage Guidelines and Protocols for Sanitary Collapse Situations
1.2. Hierarchization Processes
2. Materials and Methods
2.1. Conceptual Design of the System
2.2. Implementation of the System
2.2.1. Weightings Calculation Blocks
- Experts’ weightings calculation: Taking the values of the Vague Fuzzy Decision Vectors of Experts, first the IFOWG operator [43] is applied to determine the weighting vector of the experts by means of the method based on the normal distribution [44]. As it is not possible to objectively weight the experts’ assessments, the normal distribution is taken as a common representation of natural scoring processes. By means of IFOWG it is possible to aggregate the opinion of the different experts on each one of them. Later, the score [43] associated to each expert is calculated, which will be normalized and weighted in the [0–1] range, so that the sum of all of them is equal to 1.
- Criteria’s weightings calculation: The block associated to the calculation of the criteria weightings is similar to the experts’ one. The only difference lies in the operator being used, in this case the IFHG [43] operator that makes use of the previously calculated vector of the experts’ weightings. The use of this hybrid operator allows for the combination of the effects of the direct weightings, making use of the experts’ weighting vector, and organized by considering a normal distribution associated to the assessment of the criteria by these same experts. Same as in the previous case, the score is later calculated, and after that the normalization and weighting of the different weights obtained is carried out.
2.2.2. Hierarchy Block
3. Simulations and Results
3.1. Preliminary Assessments
3.2. Weightings Calculation Blocks
3.2.1. Determination of the Experts’ Weightings Vector
3.2.2. Determination of the Criteria Weighting Vector
3.3. Patients’ Status Assessment
3.4. Hierarchy Block
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Joebges, S.; Biller-Andorno, N. Ethics Guidelines on COVID-19 Triage-an Emerging International Consensus. Crit. Care 2020, 24, 201. [Google Scholar] [CrossRef] [PubMed]
- Jöbges, S.; Vinay, R.; Luyckx, V.A.; Biller-Andorno, N. Recommendations on COVID-19 Triage: International Comparison and Ethical Analysis. Bioethics 2020, 34, 948–959. [Google Scholar] [CrossRef] [PubMed]
- Rubio, O.; Estella, A.; Cabre, L.; Saralegui-Reta, I.; Martin, M.C.; Zapata, L.; Esquerda, M.; Ferrer, R.; Castellanos, A.; Trenado, J.; et al. Ethical Recommendations for a Difficult Decision-Making in Intensive Care Units Due to the Exceptional Situation of Crisis by the COVID-19 Pandemia: A Rapid Review & Consensus of Experts. Med. Intensiva 2020, 44, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Velavan, T.P.; Meyer, C.G. The COVID-19 Epidemic. Trop. Med. Int. Health 2020, 25, 278–280. [Google Scholar] [CrossRef] [Green Version]
- Casal-Guisande, M.; Cerqueiro-Pequeño, J.; Comesaña-Campos, A.; Bouza-Rodríguez, J.B. Conceptual Proposal of a Hierarchization System for Patients Candidate to Intensive Care Units in Health Catastrophe Situations. In Proceedings of the 8th International Conference on Technological Ecosystems for Enhancing Multiculturality, Salamanca, Spain, 21–23 October 2020; pp. 496–500. [Google Scholar]
- Guidelines—International Society for Priorities in Health. Available online: https://prioritiesinhealth.org/guidelines (accessed on 27 January 2021).
- Herrmann, J.W. Engineering Decision Making and Risk Management; John Wiley & Sons, Inc.: New Jersey, NJ, USA, 2015; ISBN 9781118919330. [Google Scholar]
- Turban, E.; Aronson, J.E.; Liang, T.-P. Decision Support Systems and Intelligent Systems, 7th ed.; Prentice Hall: Hoboken, NJ, USA, 2007; ISBN 9780470755891. [Google Scholar]
- Ching-Lai, H.; Kwangsun, Y. Multiple Attribute Decision Making: Methods and Applications a State-of-the-Art Survey; Springer: Berlin/Heidelberg, Germany, 1981; ISBN 9783642483189. [Google Scholar]
- Adunlin, G.; Diaby, V.; Xiao, H. Application of Multicriteria Decision Analysis in Health Care: A Systematic Review and Bibliometric Analysis. Health Expect. 2015, 18, 1894–1905. [Google Scholar] [CrossRef] [Green Version]
- Diaz-Ledezma, C.; Parvizi, J. Surgical Approaches for Cam Femoroacetabular Impingement: The Use of Multicriteria Decision Analysis Hip. In Proceedings of the Clinical Orthopaedics and Related Research; Springer New York LLC: New York, NY, USA, 2013; Volume 471, pp. 2509–2516. [Google Scholar]
- Maruthur, N.M.; Joy, S.; Dolan, J.; Segal, J.B.; Shihab, H.M.; Singh, S. Systematic Assessment of Benefits and Risks: Study Protocol for a Multi-Criteria Decision Analysis Using the Analytic Hierarchy Process for Comparative Effectiveness Research. F1000Research 2013, 2, 160. [Google Scholar] [CrossRef] [Green Version]
- Pecchia, L.; Martin, J.L.; Ragozzino, A.; Vanzanella, C.; Scognamiglio, A.; Mirarchi, L.; Morgan, S.P. User Needs Elicitation via Analytic Hierarchy Process (AHP). A Case Study on a Computed Tomography (CT) Scanner. BMC Med. Inform. Decis. Mak. 2013, 13, 1–11. [Google Scholar] [CrossRef]
- Hummel, M.J.M.; Volz, F.; Van Manen, J.G.; Danner, M.; Dintsios, C.M.; Ijzerman, M.J.; Gerber, A. Using the Analytic Hierarchy Process to Elicit Patient Preferences: Prioritizing Multiple Outcome Measures of Antidepressant Drug Treatment. Patient 2012, 5, 225–237. [Google Scholar] [CrossRef]
- Kwak, N.K.; McCarthy, K.J.; Parker, G.E. A Human Resource Planning Model for Hospital/Medical Technologists: An Analytic Hierarchy Process Approach. J. Med. Syst. 1997, 21, 173–187. [Google Scholar] [CrossRef]
- Ashour, O.M.; Okudan Kremer, G.E. A Simulation Analysis of the Impact of FAHP-MAUT Triage Algorithm on the Emergency Department Performance Measures. Expert Syst. Appl. 2013, 40, 177–187. [Google Scholar] [CrossRef]
- Abdel-Basset, M.; Manogaran, G.; Gamal, A.; Smarandache, F. A Group Decision Making Framework Based on Neutrosophic TOPSIS Approach for Smart Medical Device Selection. J. Med. Syst. 2019, 43, 38. [Google Scholar] [CrossRef]
- Malekpoor, H.; Mishra, N.; Sumalya, S.; Kumari, S. An Efficient Approach to Radiotherapy Dose Planning Problem: A TOPSIS Case-Based Reasoning Approach. Int. J. Syst. Sci. Oper. Logist. 2017, 4, 4–12. [Google Scholar] [CrossRef]
- Li, D.P.; He, J.Q.; Cheng, P.F.; Wang, J.Q.; Zhang, H.Y. A Novel Selection Model of Surgical Treatments for Early Gastric Cancer Patients Based on Heterogeneous Multicriteria Group Decision-Making. Symmetry 2018, 10, 223. [Google Scholar] [CrossRef] [Green Version]
- Chung, S.; Kim, S.; Kim, J.; Sohn, K. Use of Multiattribute Utility Theory for Formulary Management in a Health System. Am. J. Health Syst. Pharm. 2010, 67, 128–135. [Google Scholar] [CrossRef]
- Abbas, A.; Bilal, K.; Zhang, L.; Khan, S.U. A Cloud Based Health Insurance Plan Recommendation System: A User Centered Approach. Future Gener. Comput. Syst. 2015, 43–44, 99–109. [Google Scholar] [CrossRef]
- Amaral, T.M.; Costa, A.P.C. Improving Decision-Making and Management of Hospital Resources: An Application of the PROMETHEE II Method in an Emergency Department. Oper. Res. Health Care 2014, 3, 1–6. [Google Scholar] [CrossRef]
- Uzun, D.; Uzun, B.; Sani, M.; Helwan, A.; Nwekwo, C.; Veysel, F.; Sentürka, N.; Ozsahin, I. Evaluating Cancer Treatment Alternatives Using Fuzzy PROMETHEE Method. Int. J. Adv. Comput. Sci. Appl. 2017, 8. [Google Scholar] [CrossRef] [Green Version]
- Maisaini, M.; Uzun, B.; Ozsahin, I.; Uzun, D. Evaluating Lung Cancer Treatment Techniques Using Fuzzy Promethee Approach. In Proceedings of the Advances in Intelligent Systems and Computing; Springer: Berlin, Germany, 2019; Volume 896, pp. 209–215. [Google Scholar]
- Sarigül, F.; Hülagü, S.; Uzun Ozsahin, D. Evaluation of Oral Antiviral Treatments for Chronic Hepatitis B Using Fuzzy PROMETHEE. In Applications of Multi-Criteria Decision-Making Theories in Healthcare and Biomedical Engineering; Elsevier: Amsterdam, The Netherlands, 2021; pp. 249–260. [Google Scholar]
- Zeng, Q.L.; Li, D.D.; Yang, Y. Bin VIKOR Method with Enhanced Accuracy for Multiple Criteria Decision Making in Healthcare Management. J. Med. Syst. 2013, 37, 9908. [Google Scholar] [CrossRef]
- Manupati, V.K.; Ramkumar, M.; Baba, V.; Agarwal, A. Selection of the Best Healthcare Waste Disposal Techniques during and Post COVID-19 Pandemic Era. J. Clean. Prod. 2021, 281, 125175. [Google Scholar] [CrossRef]
- Chang, T.H. Fuzzy VIKOR Method: A Case Study of the Hospital Service Evaluation in Taiwan. Inf. Sci. 2014, 271, 196–212. [Google Scholar] [CrossRef]
- Bastani, H.; Bastani, O.; Sinchaisri, W.P. Improving Human Decision-Making with Machine Learning. arXiv 2021, arXiv:2108.08454. [Google Scholar] [CrossRef]
- Hsu, J.-C.; Wu, F.-H.; Lin, H.-H.; Lee, D.-J.; Chen, Y.-F.; Lin, C.-S.; Hsu, J.-C.; Wu, F.-H.; Lin, H.-H.; Lee, D.-J.; et al. AI Models for Predicting Readmission of Pneumonia Patients within 30 Days after Discharge. Electronics 2022, 11, 673. [Google Scholar] [CrossRef]
- Arnaud, E.; Elbattah, M.; Gignon, M.; Dequen, G. Deep Learning to Predict Hospitalization at Triage: Integration of Structured Data and Unstructured Text. In Proceedings of the 2020 IEEE International Conference on Big Data, Atlanta, GA, USA, 10–13 December 2020; pp. 4836–4841. [Google Scholar] [CrossRef]
- Casal-Guisande, M.; Comesaña-Campos, A.; Dutra, I.; Cerqueiro-Pequeño, J.; Bouza-Rodríguez, J.-B. Design and Development of an Intelligent Clinical Decision Support System Applied to the Evaluation of Breast Cancer Risk. J. Pers. Med. 2022, 12, 169. [Google Scholar] [CrossRef]
- Casal-Guisande, M.; Comesaña-Campos, A.; Cerqueiro-Pequeño, J.; Bouza-Rodríguez, J.-B. Design and Development of a Methodology Based on Expert Systems, Applied to the Treatment of Pressure Ulcers. Diagnostics 2020, 10, 614. [Google Scholar] [CrossRef]
- Comesaña-Campos, A.; Casal-Guisande, M.; Cerqueiro-Pequeño, J.; Bouza-Rodríguez, J.B. A Methodology Based on Expert Systems for the Early Detection and Prevention of Hypoxemic Clinical Cases. Int. J. Environ. Res. Public Health 2020, 17, 8644. [Google Scholar] [CrossRef] [PubMed]
- Casal-Guisande, M.; Comesaña-Campos, A.; Pereira, A.; Bouza-Rodríguez, J.-B.; Cerqueiro-Pequeño, J. A Decision-Making Methodology Based on Expert Systems Applied to Machining Tools Condition Monitoring. Mathematics 2022, 10, 520. [Google Scholar] [CrossRef]
- Kochenderfer, M.J. Decision Making Under Uncertainty: Theory and Application; The MIT Press: Cambridge, MA, USA, 2015; ISBN 9780262029254. [Google Scholar]
- Celikyilmaz, A.; Türksen, I.B. Modeling Uncertainty with Fuzzy Logic; Springer: Berlin/Heidelberg, Germany, 2009; Volume 240, ISBN 978-3-540-89923-5. [Google Scholar]
- Zadeh, L.A. Fuzzy Sets. Inf. Control. 1965, 8, 338–353. [Google Scholar] [CrossRef] [Green Version]
- Bellman, R.E.; Zadeh, L.A. Decision-Making in a Fuzzy Environment. Manag. Sci. 1970, 17, B-141. [Google Scholar] [CrossRef]
- Gau, W.L.; Buehrer, D.J. Vague Sets. IEEE Trans. Syst. Man Cybern. 1993, 23, 610–614. [Google Scholar] [CrossRef]
- Atanassov, K.T. Intuitionistic Fuzzy Sets; Physica-Verlag Heidelberg: Heidelberg, Germany, 1999; ISBN 9783790824636. [Google Scholar]
- Bustince, H.; Burillo, P. Vague Sets Are Intuitionistic Fuzzy Sets. Fuzzy Sets Syst. 1996, 79, 403–405. [Google Scholar] [CrossRef]
- Xu, Z.; Yager, R.R. Some Geometric Aggregation Operators Based on Intuitionistic Fuzzy Sets. Int. J. Gen. Syst. 2006, 35, 417–433. [Google Scholar] [CrossRef]
- Xu, Z. An Overview of Methods for Determining OWA Weights. Int. J. Intell. Syst. 2005, 20, 843–865. [Google Scholar] [CrossRef]
- Thunnissen, D.P. Propagating and Mitigating Uncertainty in the Design of Complex Multidisciplinary Systems. Ph.D. Thesis, California Institute of Technology, Pasadena, CA, USA, 2005. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Equity. |
| Maximizing benefit, broadly understood as the maximization of benefit for the largest possible number of patients according to the available resources. |
| Considering the patient’s age and life span. |
| Other additional criteria. |
| Patient’s will. |
| Therapeutic ceiling, understood as the termination of therapy. |
| Additional recommendations: generally advocating for transparent decision-making processes. In the case of the UK, the use of decision support tools is recommended when they are available. |
| Periodical re-evaluation of the patient’s status. |
| Who decides? The recommendation is generally given that decisions be made by expert teams from the health field, with at least two professionals involved in the procedure. |
| 1st Priority Level | 2nd Priority Level | 3rd Priority Level | 4th Priority Level |
|---|---|---|---|
| Applicable to patients who need to be intensively monitored and who must be provided with intensive care services, such as invasive mechanical ventilation or continuous extra-renal depuration, among others. | Applicable to patients who also need to be intensively monitored, and who might demand an immediate intervention. They might require an oxygen-therapy supply, but in a non-invasive way. They might have issues in any other body organ. | Applicable to patients that have a small probability of recovery because of their base diseases. They may still be provided with palliative care. | Applicable to patients for whom ICU admission would not result in a substantial benefit because of their status. |
| Intuitionistic Fuzzy Set | Vague Fuzzy Set |
|---|---|
| Intuitionistic Fuzzy Weighted Geometric (direct weighting of vague values) | |
| Intuitionistic Fuzzy Ordered Weighted Geometric (weighting in an orderly manner of vague values) | |
| Intuitionistic Fuzzy Hybrid Geometric (combination of the two previous approaches) |
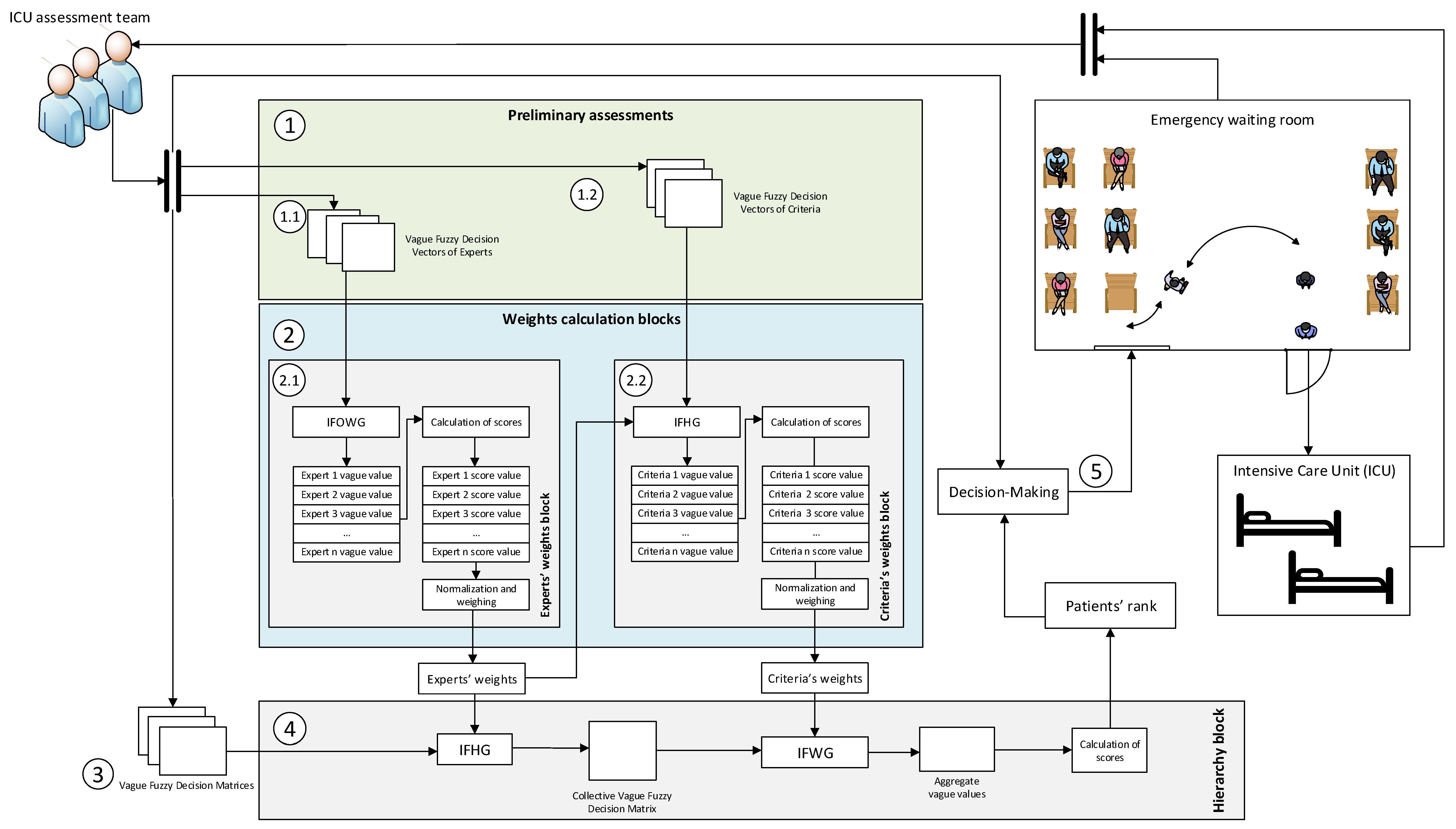
| Stage 1—Preliminary Assessments |
| Each member of the team in charge of determining the admittance to the ICU will assess the experience and importance of each other team member, these expressed by means of vague fuzzy numbers and stored into the Vague Fuzzy Decision Vectors of Experts. Later, the experts will establish the criteria to be used to assess the admittance to the ICU taking into account the applicable protocols and recommendations. After that, each one of the experts will evaluate the importance of the different criteria, which will be also expressed using vague fuzzy numbers and will be stored into the Vague Fuzzy Decision Vectors of Criteria. |
| Stage 2—Weightings Calculation Blocks |
| Starting from the Vague Fuzzy Decision Vectors of Experts and of Criteria, in the 2.1 and 2.2 blocks from Figure 1 the aggregated weighting vectors associated to the experts and to the criteria are calculated by applying a series of operators. The weighting vectors calculated in this stage will be later necessary to allow the aggregation of the patients’ status assessment in Stage 4. |
| Stage 3—Patients’ Status Assessment |
| Each member of the admittance team will assess the status of each patient taking into account the previously determined criteria. The assessment associated to the different patients’ status, produced by each expert, will be stored into a matrix named Vague Fuzzy Decision Matrix, as shown in Figure 1. |
| Stage 4—Hierarchy Block |
| By applying the operators indicated in Stage 2 on the matrices obtained in Stage 3, and taking into account the weighting vectors previously obtained, it is possible to establish a ranking or patients according to the previously established assessments. |
| Stage 5—Decision-Making |
| Starting from the information associated to the ranking obtained as a result of Stage 4, the admittance team will decide which patients will be admitted to the ICU. It is essential to point out that there will be a periodical evaluation of both the evolution and the priority of the patients currently in the ICU. |
| E1 | E2 | E3 | E4 | E5 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| E1 | - | - | 0.7 | 0.8 | 0.5 | 0.8 | 0.9 | 1 | 0.6 | 0.9 |
| E2 | 0.5 | 0.8 | - | - | 0.6 | 0.9 | 0.8 | 1 | 0.8 | 1 |
| E3 | 0.5 | 0.6 | 0.8 | 1 | - | - | 1 | 1 | 0.7 | 0.8 |
| E4 | 0.6 | 0.7 | 0.7 | 0.9 | 0.7 | 1 | - | - | 0.8 | 0.9 |
| E5 | 0.7 | 0.8 | 0.6 | 0.8 | 0.6 | 0.9 | 0.7 | 0.9 | - | - |
| C1 | C2 | C3 | C4 | C5 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| E1 | 0.4 | 0.7 | 0.8 | 1 | 0.2 | 0.5 | 0.5 | 0.9 | 0.7 | 0.9 |
| E2 | 0.6 | 0.8 | 0.6 | 0.9 | 0.4 | 0.7 | 0.6 | 0.8 | 0.5 | 0.8 |
| E3 | 0.5 | 0.8 | 0.8 | 0.9 | 0.5 | 0.8 | 0.3 | 0.5 | 0.6 | 1 |
| E4 | 0.7 | 0.8 | 1 | 1 | 0.5 | 0.7 | 0.6 | 0.7 | 0.5 | 0.7 |
| E5 | 0.6 | 0.8 | 0.6 | 0.9 | 0.6 | 0.8 | 0.7 | 0.8 | 0.4 | 0.6 |
| E1 | E2 | E3 | E4 | E5 | |||||
|---|---|---|---|---|---|---|---|---|---|
| 0.56 | 0.77 | 0.70 | 0.84 | 0.56 | 0.90 | 0.84 | 0.98 | 0.71 | 0.93 |
| E1 | E2 | E3 | E4 | E5 |
|---|---|---|---|---|
| 0.33 | 0.54 | 0.46 | 0.83 | 0.64 |
| E1 | E2 | E3 | E4 | E5 |
|---|---|---|---|---|
| 0.12 | 0.19 | 0.16 | 0.30 | 0.23 |
| C1 | C2 | C3 | C4 | C5 | |||||
|---|---|---|---|---|---|---|---|---|---|
| 0.58 | 0.80 | 0.71 | 0.56 | 0.73 | 0.50 | 0.77 | 0.76 | 0.94 | 0.45 |
| C1 | C2 | C3 | C4 | C5 |
|---|---|---|---|---|
| 0.37 | 0.70 | 0.16 | 0.28 | 0.27 |
| C1 | C2 | C3 | C4 | C5 |
|---|---|---|---|---|
| 0.21 | 0.39 | 0.09 | 0.16 | 0.15 |
| E1 | P1 | P2 | P3 | P4 | P5 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| C1 | 0.3 | 0.6 | 0.6 | 0.9 | 0.7 | 0.7 | 0.3 | 0.6 | 0.8 | 0.9 |
| C2 | 0.4 | 0.9 | 0.7 | 0.7 | 0.8 | 1 | 0.6 | 0.9 | 0.3 | 0.7 |
| C3 | 0.2 | 0.7 | 0.3 | 0.7 | 0.4 | 0.5 | 0.6 | 0.9 | 0.4 | 0.5 |
| C4 | 0.7 | 0.9 | 0.4 | 0.9 | 0.3 | 0.9 | 0.4 | 0.8 | 0.7 | 1 |
| C5 | 0.6 | 0.8 | 0.8 | 0.9 | 0.5 | 0.7 | 0.9 | 1 | 0.5 | 0.8 |
| E2 | P1 | P2 | P3 | P4 | P5 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| C1 | 0.5 | 0.7 | 0.7 | 0.8 | 0.5 | 0.7 | 0.5 | 0.6 | 0.7 | 0.7 |
| C2 | 0.6 | 0.9 | 0.6 | 0.9 | 0.7 | 0.8 | 0.7 | 0.9 | 0.5 | 0.6 |
| C3 | 0.7 | 0.8 | 0.4 | 0.6 | 0.6 | 0.7 | 0.4 | 0.8 | 0.6 | 0.7 |
| C4 | 0.7 | 0.9 | 0.6 | 0.8 | 0.3 | 0.8 | 0.7 | 0.8 | 0.6 | 1 |
| C5 | 0.8 | 0.8 | 0.7 | 0.7 | 0.6 | 0.9 | 0.7 | 0.7 | 0.5 | 0.9 |
| E3 | P1 | P2 | P3 | P4 | P5 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| C1 | 0.6 | 0.7 | 0.8 | 0.8 | 0.6 | 0.9 | 0.6 | 0.6 | 0.8 | 0.9 |
| C2 | 0.5 | 1 | 0.5 | 0.7 | 0.8 | 1 | 0.6 | 0.9 | 0.6 | 0.8 |
| C3 | 0.6 | 0.6 | 0.6 | 0.8 | 0.7 | 0.7 | 0.5 | 0.7 | 0.7 | 0.7 |
| C4 | 0.6 | 0.9 | 0.5 | 1 | 0.4 | 0.9 | 0.9 | 0.9 | 0.5 | 0.8 |
| C5 | 0.7 | 0.7 | 0.6 | 0.7 | 0.8 | 0.9 | 0.5 | 0.8 | 0.7 | 1 |
| E4 | P1 | P2 | P3 | P4 | P5 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| C1 | 0.3 | 0.6 | 0.7 | 0.9 | 0.4 | 0.9 | 0.8 | 0.8 | 0.6 | 0.9 |
| C2 | 0.5 | 0.9 | 0.7 | 0.7 | 0.5 | 0.8 | 0.5 | 0.9 | 0.6 | 0.8 |
| C3 | 0.8 | 0.9 | 0.3 | 0.9 | 0.8 | 0.9 | 0.4 | 1 | 0.7 | 0.8 |
| C4 | 0.3 | 0.5 | 0.8 | 0.8 | 0.6 | 0.8 | 0.7 | 0.8 | 0.6 | 1 |
| C5 | 0.4 | 0.4 | 0.3 | 0.9 | 0.6 | 0.7 | 0.7 | 0.9 | 0.8 | 0.9 |
| E5 | P1 | P2 | P3 | P4 | P5 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| C1 | 0.5 | 0.7 | 0.6 | 0.9 | 0.2 | 1 | 0.7 | 0.9 | 0.9 | 1 |
| C2 | 0.8 | 1 | 0.5 | 0.7 | 0.4 | 0.9 | 0.4 | 1 | 0.7 | 1 |
| C3 | 0.7 | 0.8 | 0.3 | 0.9 | 0.7 | 0.9 | 0.7 | 0.9 | 0.6 | 0.8 |
| C4 | 0.6 | 0.7 | 0.7 | 0.9 | 0.4 | 0.9 | 0.6 | 0.9 | 0.5 | 0.7 |
| C5 | 0.2 | 0.3 | 0.1 | 0.7 | 0.4 | 0.8 | 0.5 | 0.7 | 0.7 | 0.9 |
| P1 | P2 | P3 | P4 | P5 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| C1 | 0.444 | 0.679 | 0.685 | 0.852 | 0.402 | 0.848 | 0.611 | 0.709 | 0.767 | 0.871 |
| C2 | 0.575 | 0.939 | 0.593 | 0.736 | 0.591 | 0.878 | 0.547 | 0.929 | 0.540 | 0.786 |
| C3 | 0.640 | 0.766 | 0.352 | 0.787 | 0.672 | 0.771 | 0.486 | 0.864 | 0.603 | 0.725 |
| C4 | 0.566 | 0.764 | 0.632 | 0.860 | 0.414 | 0.847 | 0.634 | 0.847 | 0.554 | 0.916 |
| C5 | 0.489 | 0.537 | 0.390 | 0.773 | 0.551 | 0.804 | 0.633 | 0.796 | 0.665 | 0.890 |
| P1 | 0.536 | 0.766 |
| P2 | 0.553 | 0.789 |
| P3 | 0.515 | 0.845 |
| P4 | 0.580 | 0.840 |
| P5 | 0.608 | 0.832 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casal-Guisande, M.; Comesaña-Campos, A.; Cerqueiro-Pequeño, J.; Bouza-Rodríguez, J.-B. Design and Definition of a New Decision Support System Aimed to the Hierarchization of Patients Candidate to Be Admitted to Intensive Care Units. Healthcare 2022, 10, 587. https://doi.org/10.3390/healthcare10030587
Casal-Guisande M, Comesaña-Campos A, Cerqueiro-Pequeño J, Bouza-Rodríguez J-B. Design and Definition of a New Decision Support System Aimed to the Hierarchization of Patients Candidate to Be Admitted to Intensive Care Units. Healthcare. 2022; 10(3):587. https://doi.org/10.3390/healthcare10030587
Chicago/Turabian StyleCasal-Guisande, Manuel, Alberto Comesaña-Campos, Jorge Cerqueiro-Pequeño, and José-Benito Bouza-Rodríguez. 2022. "Design and Definition of a New Decision Support System Aimed to the Hierarchization of Patients Candidate to Be Admitted to Intensive Care Units" Healthcare 10, no. 3: 587. https://doi.org/10.3390/healthcare10030587