Long-Term Influence of the Practice of Physical Activity on the Self-Perceived Quality of Life of Women with Breast Cancer: A Randomized Controlled Trial

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
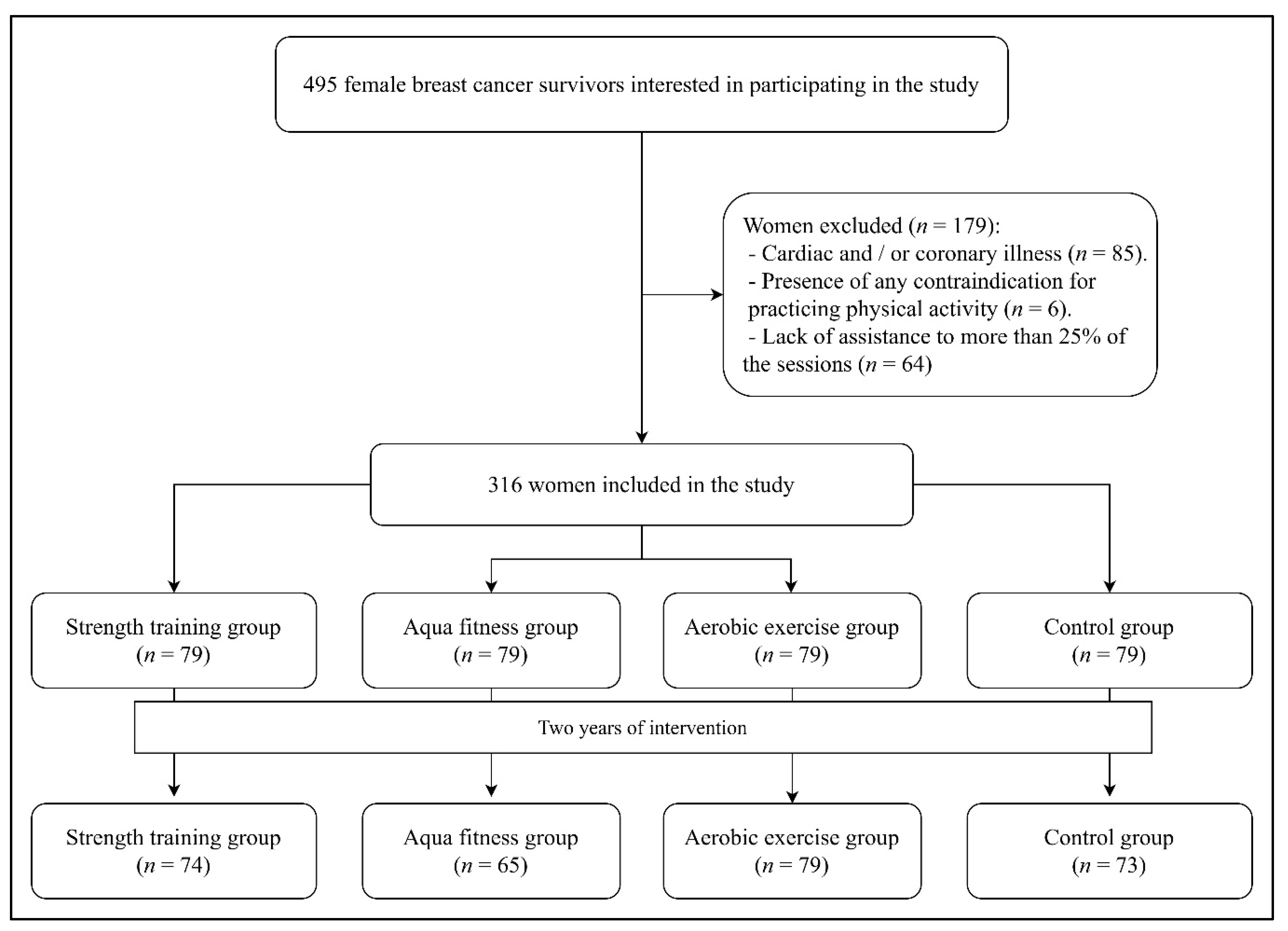
2.1. Experimental Design and Sample
2.2. Procedure
2.3. Programs of PA
2.4. Data Analysis
3. Results
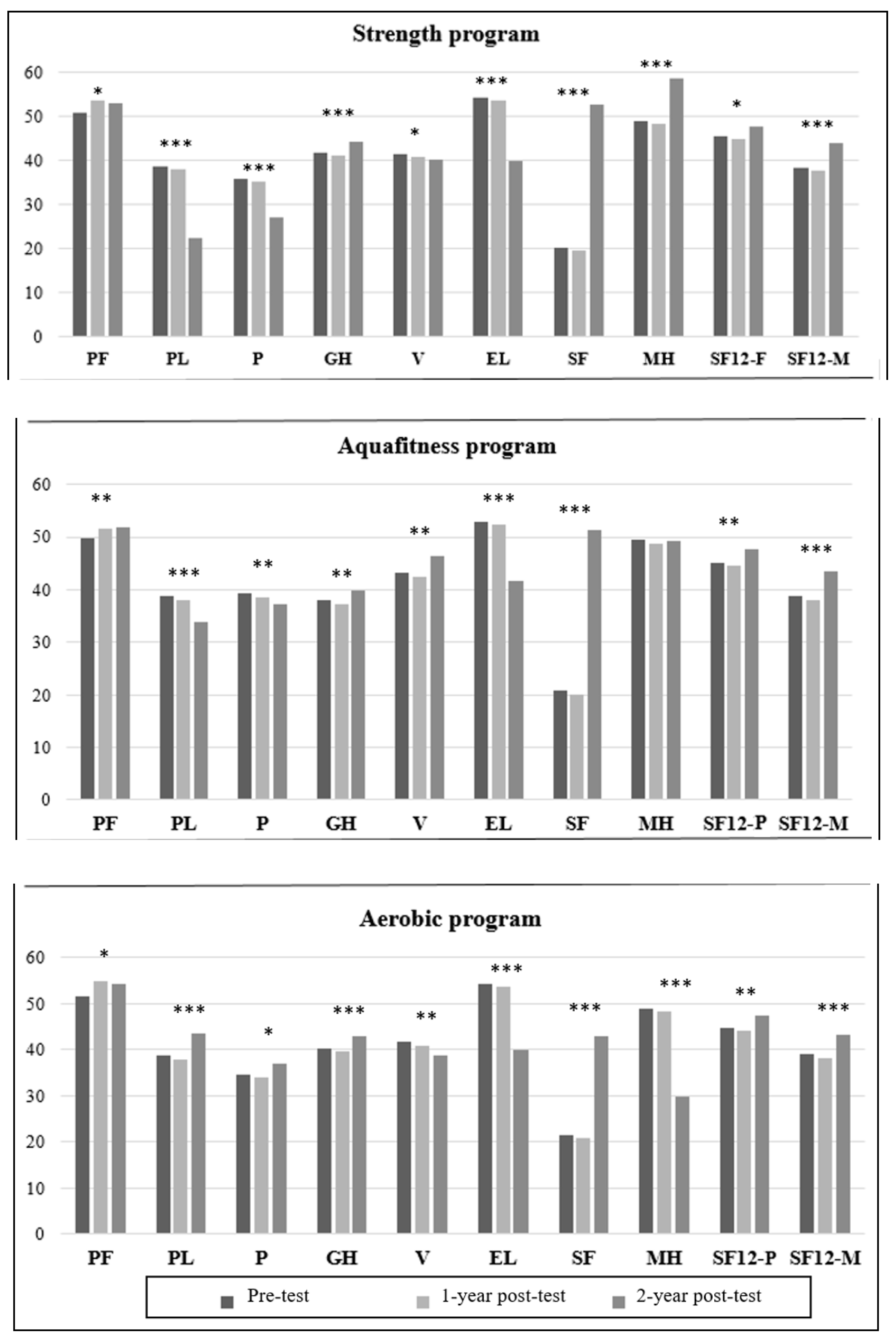
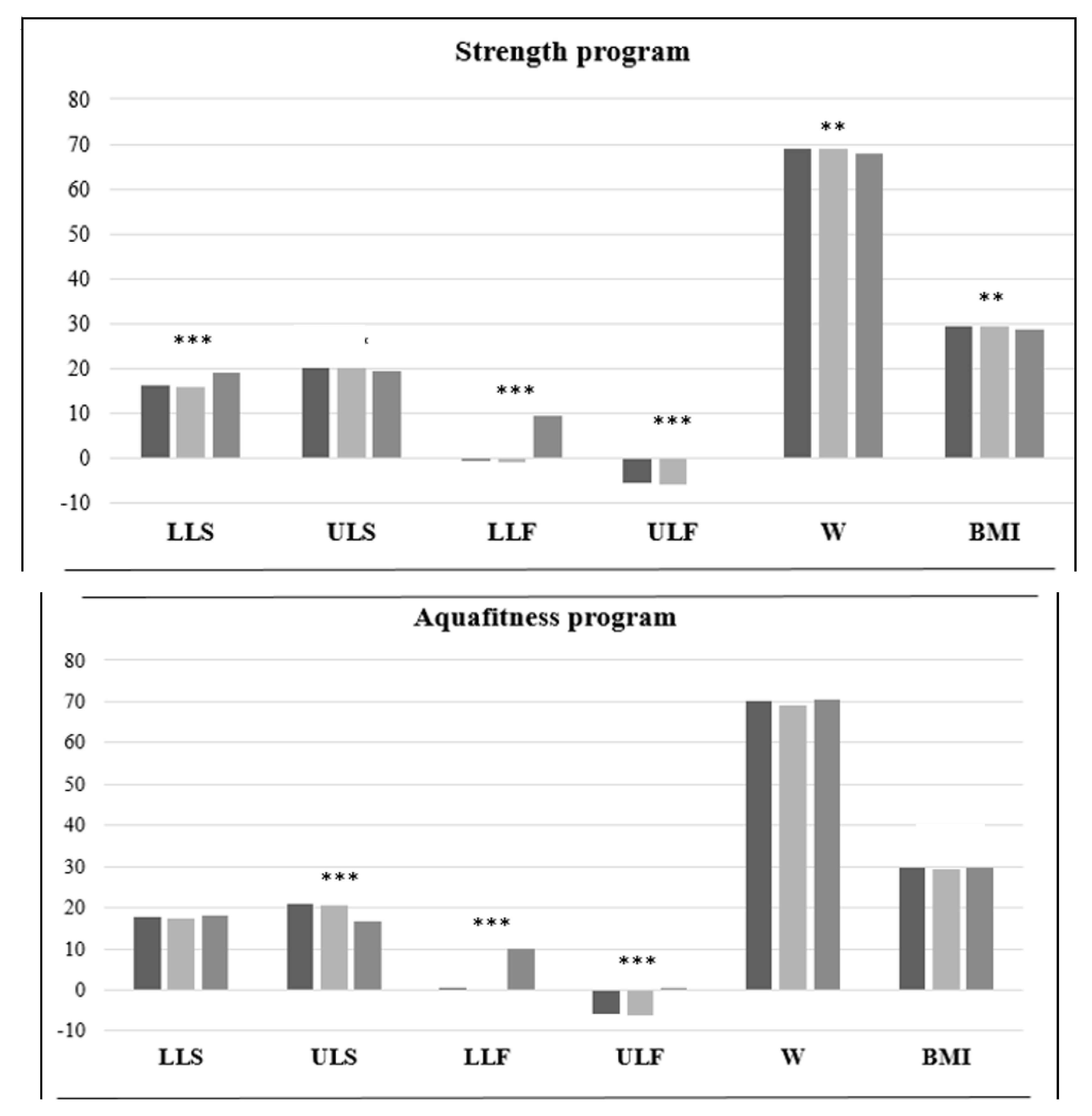
3.1. Strength Program
3.2. Aqua Fitness Program
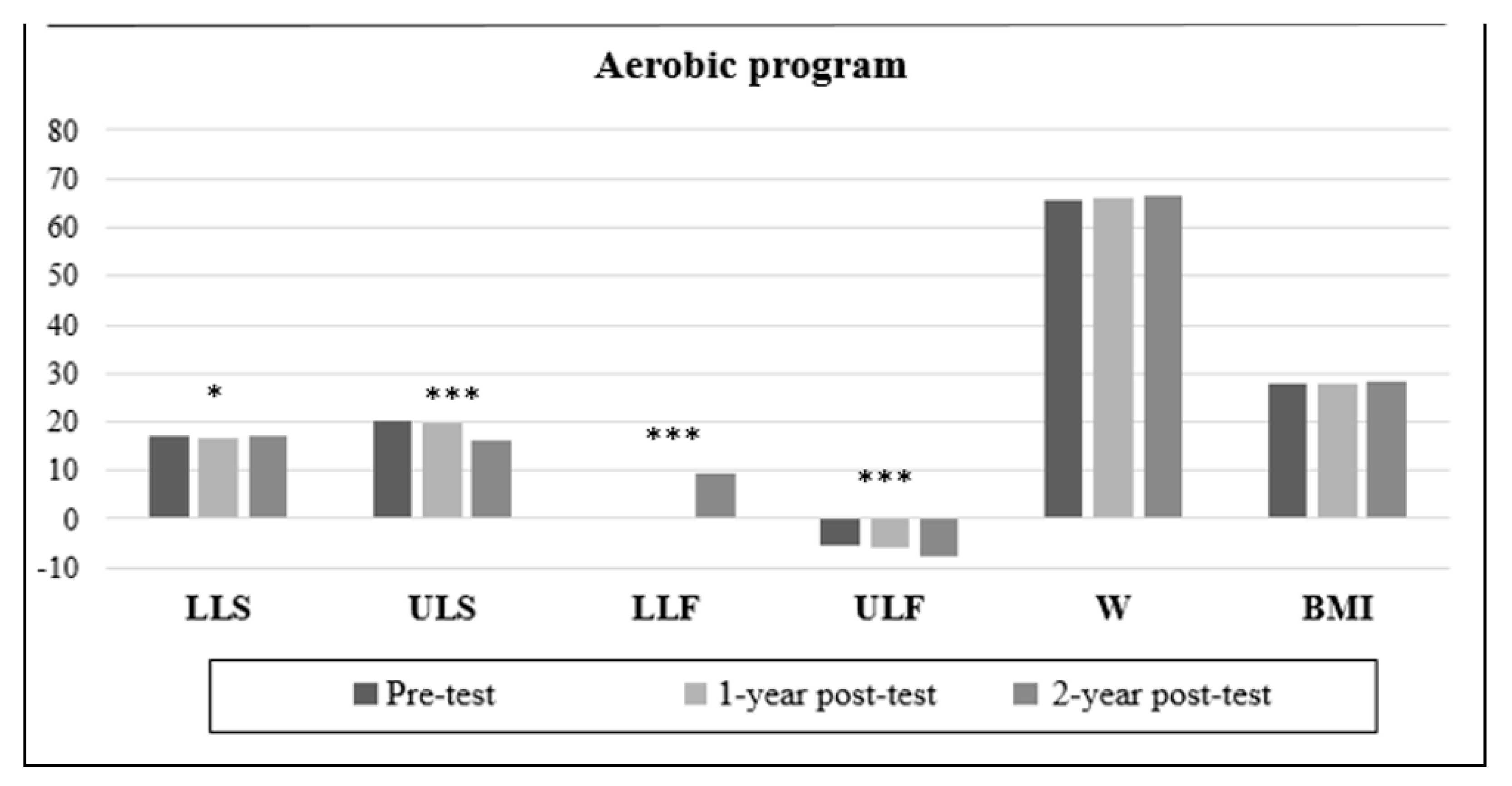
3.3. Aerobic Exercise Program
3.4. Comparative Results between Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- McGuire, S. World Cancer Report 2014; World Health Organization, International Agency for Research on Cancer; WHO Press: Geneva, Switzerland, 2015. [Google Scholar]
- Carlson, C.L. Effectiveness of the World Health Organization cancer pain relief guidelines: An integrative review. J. Pain Res. 2016, 9, 515–534. [Google Scholar] [CrossRef] [Green Version]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.; Estève, J.; et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): Analysis of individual records for 37,513,025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- Rugo, H.S.; Finn, R.S.; Gelmon, K.; Joy, A.A.; Harbeck, N.; Castrellon, A.; Mukai, H.; Walshe, J.M.; Mori, A.; Gauthier, E.; et al. Progression-free survival outcome is independent of objective response in patients with estrogen receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer treated with palbociclib plus letrozole compared with letrozole: Analysis from PALOMA-2. Clin. Breast Cancer 2019, 20, e173–e180. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.M.L.; American College of Sports Medicine. ACSM’s Guide to Exercise and Cancer Survivorship; Human Kinetics: Champaing, IL, USA, 2012. [Google Scholar]
- Wattanapisit, A. Physical activity for adult cancer survivors: A literature review. Walailak J. Sci. Technol. 2017, 14, 1–10. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Betof, A.S.; Dewhirst, M.W.; Jones, L.W. Effects and potential mechanisms of exercise training on cancer progression: A translational perspective. Brain Behav. Immun. 2013, 30, S75–S87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cave, J.; Paschalis, A.; Huang, C.; West, M.; Copson, E.; Jack, S.; Grocott, M.P.W. A systematic review of the safety and efficacy of aerobic exercise during cytotoxic chemotherapy treatment. Support. Care Cancer 2018, 26, 3337–3351. [Google Scholar] [CrossRef]
- Schmitz, K.H. Incorporating strength training into cancer care: Translating PAL into the strength after Breast Cancer Program. Obesity 2017, 25, S32–S33. [Google Scholar] [CrossRef] [Green Version]
- De Luca, V.; Minganti, C.; Borrione, P.; Grazioli, E.; Cerulli, C.; Guerra, E.; Bonifacino, A.; Parisi, A. Effects of concurrent aerobic and strength training on breast cancer survivors: A pilot study. Public Health 2016, 136, 126–132. [Google Scholar] [CrossRef]
- Dolan, L.B.; Campbell, K.; Gelmon, K.; Neil-Sztramko, S.; Holmes, D.; McKenzie, D.C. Interval versus continuous aerobic exercise training in breast cancer survivors: A pilot RCT. Support. Care Cancer 2016, 24, 119–127. [Google Scholar] [CrossRef]
- Ax, A.; Johansson, B.; Carlsson, M.; Nordin, K.; Börjeson, S. Exercise: A positive feature on functioning in daily life during cancer treatment–Experiences from the Phys-Can Study. Eur. J. Oncol. Nurs. 2020, 44, 101713. [Google Scholar] [CrossRef] [Green Version]
- Mustian, K.; Alfano, C.; Heckle, C.; Kleckner, A.S.; Kleckner, I.R.; Leach, C.R.; Mohr, D.; Palesh, O.G.; Peppone, L.J.; Piper, B.F.; et al. Clinical benefits of exercise and psychological interventions in patients with cancer-related fatigue. JAMA Oncol. 2017, 3, 961–968. [Google Scholar] [CrossRef] [PubMed]
- Rikli, R.E.; Jones, C.J. Development and validation of a functional fitness test for community-residing older adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Senior Fitness Test Manual; Human Kinetics: Champaing, IL, USA, 2013. [Google Scholar]
- Jenkinson, C.; Layte, R.; Jenkinson, D.; Lawrence, K.; Petersen, S.; Paice, C.; Stradling, J. A shorter form health survey: Can the SF-12 replicate results from the SF-36 in longitudinal studies? J. Public Health 1997, 19, 179–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandek, B.; Ware, J.E.; Aaronson, N.K.; Apolone, G.; Bjorner, J.B.; Brazier, J.E.; Bullinger, M.; Kaasa, S.; Leplege, A.; Prieto, L.; et al. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: Results from the IQOLA Project. J. Clin. Epidemiol. 1998, 51, 1171–1178. [Google Scholar] [CrossRef]
- Vilagut, G.; Valderas, J.M.; Ferrer, M.; Garin, O.; López-García, E.; Alonso, J. Interpretation of SF-36 and SF-12 questionnaires in Spain: Physical and mental components. Med. Clin. 2008, 130, 726–735. [Google Scholar] [CrossRef] [Green Version]
- Winters-Stone, K.M.; Lyons, K.S.; Dobek, J.; Dieckmann, N.F.; Bennett, J.A.; Nail, L.; Beer, T.M. Benefits of partnered strength training for prostate cancer survivors and spouses: Results from a randomized controlled trial of the Exercising Together project. J. Cancer Surviv. 2016, 10, 633–644. [Google Scholar] [CrossRef]
- Pronk, N.P.; Bender, E.G.; Katz, A.S. Health, function, and performance benefits of workplace strength training programs. ACSM’s Health Fit. J. 2016, 20, 69–71. [Google Scholar] [CrossRef]
- Seguin, R.; Nelson, M.E. The benefits of strength training for older adults. Am. J. Prev. Med. 2003, 25, 141–149. [Google Scholar] [CrossRef]
- Leirós-Rodríguez, R.; Romo-Pérez, V.; Pérez-Ribao, I.; García-Soidán, J.L. A comparison of three physical activity programs for health and fitness tested with older women: Benefits of aerobic activity, aqua fitness, and strength training. J. Women Aging 2019, 31, 419–431. [Google Scholar] [CrossRef]
- Nikendei, C.; Terhoeven, V.; Ehrenthal, J.C.; Maatouk, I.; Wild, B.; Herzog, W.; Friederich, H.C. Depression profile in cancer patients and patients without a chronic somatic disease. Psychooncology 2018, 27, 83–90. [Google Scholar] [CrossRef]
- Zhukova, G.; Shikhlyarova, A.; Shirnina, E.; Zinkovich, M.; Maschenko, N.; Zlatnik, E.; Pyltsin, S.; Anistratov, P.; Bragina, M.I.; Zhadobina, A.; et al. Characteristics of the psychosomatic state of patients with lung cancer. Ann. Oncol. 2018, 29, viii561. [Google Scholar] [CrossRef]
- Boguszewski, D.; Adamczyk, J.G.; Ochal, A. The role of pilates and aquafitness exercises in sustaining the health and fitness of elderly women. Sport Sci. Rev. 2012, 21, 127–138. [Google Scholar] [CrossRef]
- Salmon, M.; Blanchin, M.; Rotonda, C.; Guillemin, F.; Sébille, V. Identifying patterns of adaptation in breast cancer patients with cancer-related fatigue using response shift analyses at subgroup level. Cancer Med. 2017, 6, 2562–2575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyszora, A.; Budzyński, J.; Wójcik, A.; Prokop, A.; Krajnik, M. Physiotherapy programme reduces fatigue in patients with advanced cancer receiving palliative care: Randomized controlled trial. Support. Care Cancer 2017, 25, 2899–2908. [Google Scholar] [CrossRef]
- Vécseyné, M.; Kopkáné, J.; József, B.; Olvasztóné, Z.; Barthalos, I. Effects of pilates and aqua fitness training on older adults’ physical functioning and quality of life. Biomed. Hum. Kinet. 2013, 4, 22–27. [Google Scholar] [CrossRef]
- Kitzman, D.W.; Brubaker, P.; Morgan, T.; Haykowsky, M.; Hundley, G.; Kraus, W.E.; Eggebeen, J.; Nicklas, B.J. Effect of caloric restriction or aerobic exercise training on peak oxygen consumption and quality of life in obese older patients with heart failure with preserved ejection fraction: A randomized clinical trial. JAMA 2016, 315, 36–46. [Google Scholar] [CrossRef]
- Zheng, G.; Xia, R.; Zhou, W.; Tao, J.; Chen, L. Aerobic exercise ameliorates cognitive function in older adults with mild cognitive impairment: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2016, 50, 1443–1450. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strength Group | Aqua Fitness Group | Aerobic Group | Control Group | |||||
|---|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Pre-Test | Post-Test | Pre-Test | Post-Test | Pre-Test | Post-Test | |
| Survival (n) | 79 | 74 | 79 | 65 | 79 | 72 | 79 | 73 |
| Age (years) | 63 ± 7 | 65 ± 7 | 62 ± 6.8 | 64 ± 6.8 | 64 ± 7.1 | 66 ± 7.1 | 63 ± 4.6 | 65 ± 4.6 |
| Weight (kg) | 69 ± 11 | 67.7 ± 10.2 #**+ | 70.5 ± 11 | 71.2 ± 10.9 %%**$$$ | 65.7 ± 9.8 | 66 ± 10.5 &&+$$$ | 69.5 ± 10.6 | 69.7 ± 10.6 #%%&& |
| BMI (kg/m2) | 29.4 ± 8.5 | 28.8 ± 9 #**+ | 29.8 ± 9.6 | 30.2 ± 9.5 %%**$$$ | 27.7 ± 8.3 | 27.9 ± 9.1 &&+$$$ | 28.5 ± 9.4 | 28.6 ± 9.3 #%%&& |
| SF-12 health survey | ||||||||
| PF | 50.8 ± 9.2 | 53.1 ± 6.6 | 49.8 ± 8.1 | 53 ± 7.2 | 51.5 ± 7.7 | 52.7 ± 6.7 | 53.2 ± 9.1 | 53.6 ± 7 |
| PL | 38.7 ± 1.3 | 34.4 ± 19.7 #++ | 38.7 ± 1.4 | 34 ± 21.9 %%%$$$ | 38.7 ± 1.4 | 43.7 ± 23.7 ++$$$ | 38.9 ± 22.9 | 44 ± 21 #%%% |
| Pain | 36 ± 13.7 | 34.1 ± 8.4 ##**++ | 39.4 ± 13.7 | 37.1 ± 1.4 ** | 34.6 ± 11.5 | 37.1 ± 1.4 ++ | 27.2 ± 1.3 | 37.3 ± 1.6 ## |
| GH | 41.8 ± 9.3 | 44.4 ± 13.7 ##**+ | 38.1 ± 8.3 | 39.8 ± 13.7 %%%**$$ | 40.3 ± 9.9 | 43 ± 11.5 &&+$$ | 42.3 ± 9.3 | 25.6 ± 15.2 ##%%%&& |
| Vitality | 41.4 ± 5.8 | 39.2 ± 9.3** | 43.2 ± 12.1 | 46.5 ± 8.3 %%**$$ | 41.6 ± 14.2 | 38.7 ± 9.9 &$$ | 38.3 ± 12.9 | 40.7 ± 9.8 %%& |
| EL | 54.4 ± 6.4 | 39.8 ± 5.8 ##* | 53 ± 4.1 | 41.6 ± 12.1 %%*$ | 54.4 ± 10.9 | 40 ± 14.2 &&$ | 54.5 ± 6.4 | 36.7 ± 13.1 ##%%&& |
| SF | 20.2 ± 3.9 | 52.8 ± 6.4 ###* | 20.7 ± 4.3 | 51.4 ± 4.1 %%%*$ | 21.4 ± 4.5 | 52.8 ± 10.9 &&$ | 20.9 ± 3.9 | 50.9 ± 7 ###%%%&& |
| MH | 49.1 ± 7.8 | 58.6 ± 3.9 ###***+++ | 49.4 ± 7 | 49.1 ± 4.3 %%%***$$$ | 48.9 ± 8.5 | 45.8 ± 4.5 &&+++$$$ | 48.5 ± 7.8 | 49.3 ± 3.6 ###%%%&& |
| SF12-P | 45.6 ± 4.2 | 47.5 ± 7.8 # | 45.1 ± 4.1 | 47.8 ± 7 %% | 44.8 ± 3.8 | 47.3 ± 8.5 & | 43.8 ± 4.5 | 46.9 ± 7.4 #%%& |
| SF12-M | 38.4 ± 1.4 | 44 ± 4.5 #+ | 38.9 ± 4.2 | 43.5 ± 4.1 % | 39 ± 4.5 | 43.2 ± 3.8 + | 38.1 ± 5.4 | 42.2 ± 4.5 # |
| Senior Fitness Test | ||||||||
| LLS | 16.2 ± 0.6 | 18.3 ± 1 | 17.7 ± 4.5 | 18.2 ± 1.4 | 17.1 ± 4.9 | 18.8 ± 1.7 & | 17.6 ± 5.8 | 17.2 ± 1.3 & |
| ULS | 20.2 ± 7.6 | 19.2 ± 0.6 ##**+++ | 20.9 ± 5.5 | 16.7 ± 4.5 ** | 20.2 ± 5.5 | 16.1 ± 4.9 +++ | 19.6 ± 9.6 | 16.6 ± 4.9 ## |
| LLF | −0.7 ± 5.2 | 19.2 ± 7.6 # | 0.2 ± 8.6 | 19.9 ± 5.5 %% | 0.7 ± 8.8 | 19.2 ± 5.5 | −0.1 ± 9 | 18.6 ± 5.8 #%% |
| ULF | −5.5 ± 7.4 | 0 ± 9.4 ##+++ | −5.7 ± 12 | 0.5 ± 10.2 %%$$ | −5.5 ± 13.3 | −6.8 ± 8.8 &&+++$$ | −10.1 ± 4.9 | −2 ± 9.8 ##%%&& |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Soidán, J.L.; Pérez-Ribao, I.; Leirós-Rodríguez, R.; Soto-Rodríguez, A. Long-Term Influence of the Practice of Physical Activity on the Self-Perceived Quality of Life of Women with Breast Cancer: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 4986. https://doi.org/10.3390/ijerph17144986
García-Soidán JL, Pérez-Ribao I, Leirós-Rodríguez R, Soto-Rodríguez A. Long-Term Influence of the Practice of Physical Activity on the Self-Perceived Quality of Life of Women with Breast Cancer: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(14):4986. https://doi.org/10.3390/ijerph17144986
Chicago/Turabian StyleGarcía-Soidán, Jose L., Ignacio Pérez-Ribao, Raquel Leirós-Rodríguez, and Anxela Soto-Rodríguez. 2020. "Long-Term Influence of the Practice of Physical Activity on the Self-Perceived Quality of Life of Women with Breast Cancer: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 14: 4986. https://doi.org/10.3390/ijerph17144986