Multidimensional Geriatric Assessment with MAGIC Questionnaire and Quality of Life in Elderly Primary Care Patients

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
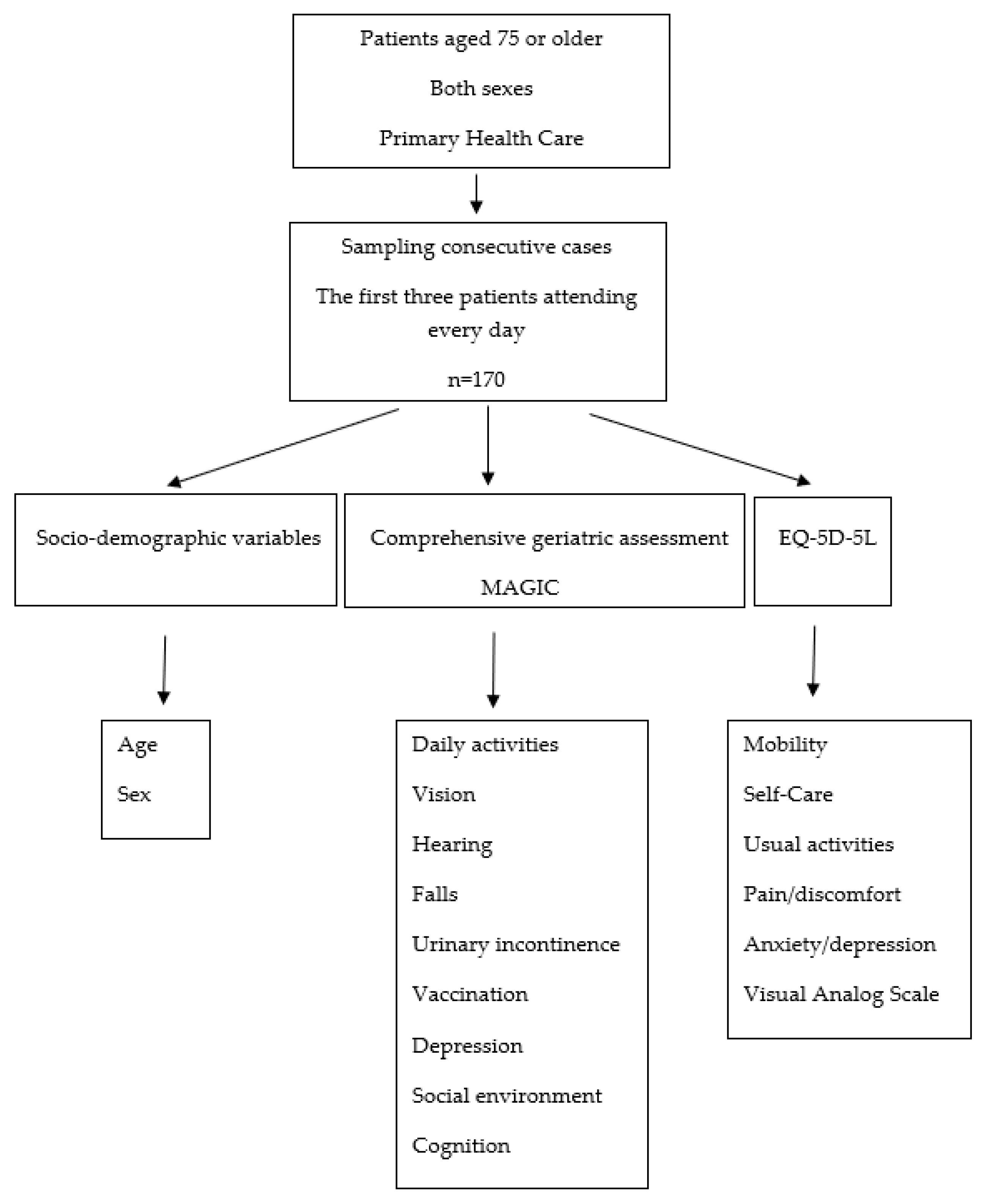
2.1. Design and Location
2.2. Study Population
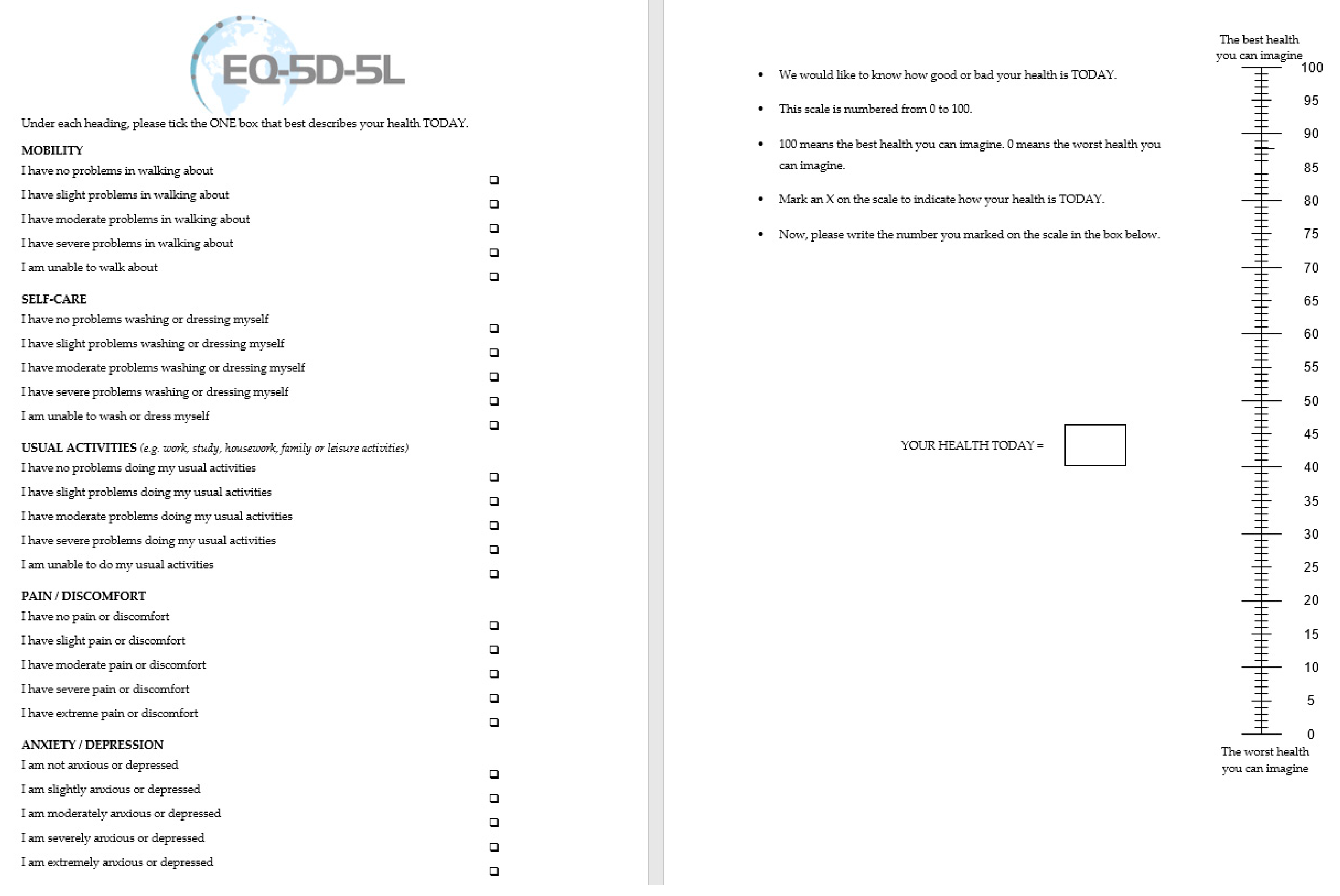
2.3. Measurements
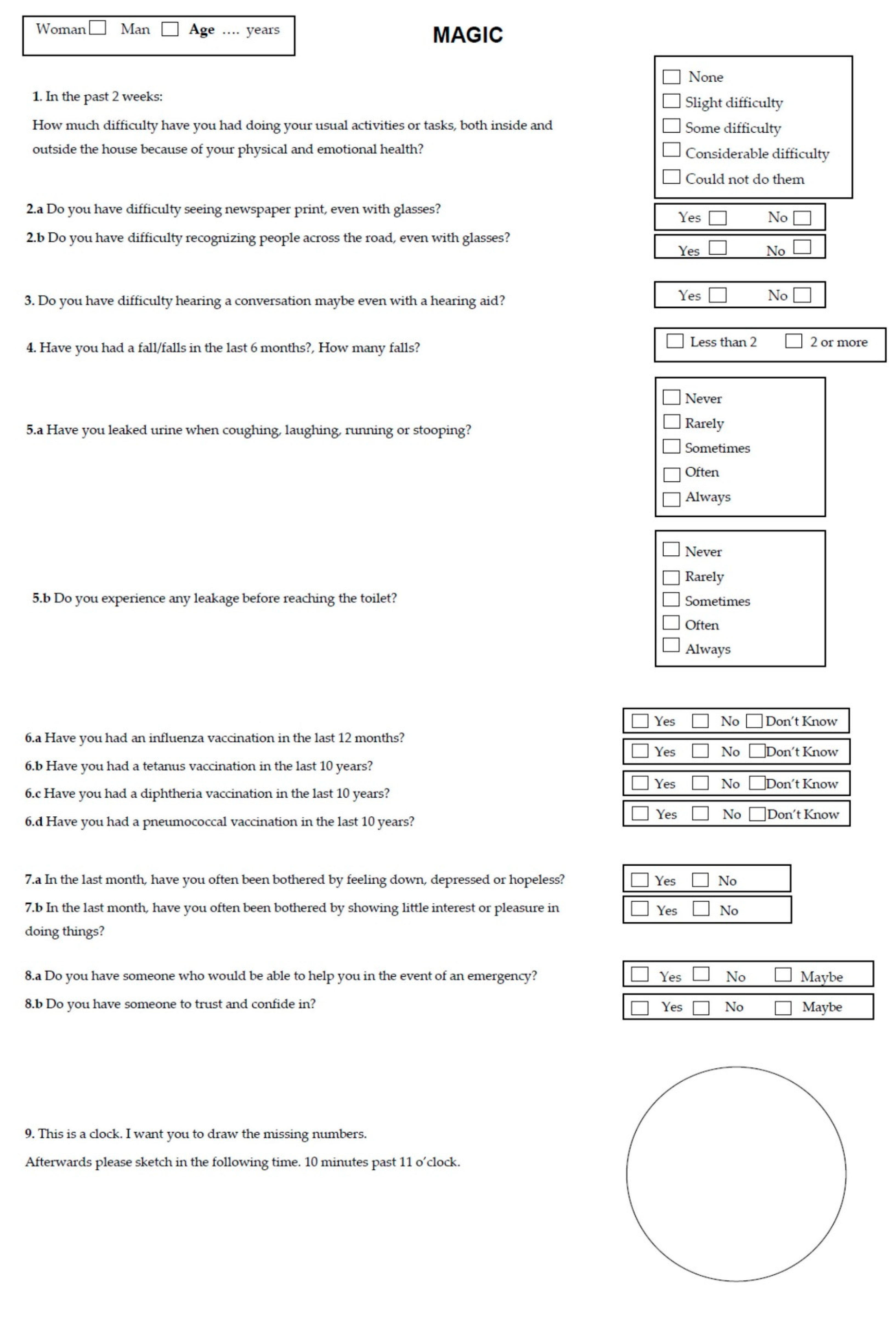
- MAGIC questionnaire [8] with nine domains (daily activities, vision, hearing, falls, urinary incontinence, vaccination, depression, social environment and cognition) and 16 items: 15 categorical response items and one item that includes a question with the clock-drawing test, with scores from 1 to 7. Except for the clock-drawing test, the other items did not score (Table 1).
2.4. Methods
- The wordings in some questions (Do you have someone to trust and confide in? In the past month, have you often been bothered by feeling down, depressed or hopeless? In the past month, have you often been bothered by feeling little interest or pleasure in doing things?) were compared to those used in questionnaires validated in Spanish, such as the Older Americans Resources and Services (OARS) Social Resources Scale [13], the Whooley questions [14] and the COOP/WONCA Functional Assessment Charts [15], respectively;
- Unlike the original instrument, with clock scores ranging from 1 to 7 (without specifying how it was quantified), we followed Thalmann’s assessment [16]. This consists of scoring the following items: 1 point if all 12 numbers are present; 2 points if the number 12 is placed correctly; 2 points if hands are correctly proportional; 2 points if the subject is able to tell the time correctly. The optimal cut-off score was 5 points out of a total of 7;
- “Immunization” has been changed from the original MAGIC questionnaire to “vaccine” to facilitate understanding;
- The question on pneumococcal vaccination was included as this is recommended in Galicia (Spain) [17];
- A cognitive test was performed with 10 patients over 75 years of age to check if wording and font size were acceptable.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

Appendix C

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Woman | Man | p | ||||||||||||||
| N | % | Lost | Median | IQR * | N | % | Lost | Median | IQR * | |||||||
| Age | 106 | 0 | 82.0 | 79.0 | – | 85.0 | 64 | 0 | 81.0 | 77.5 | – | 85.0 | 0.268 | |||
| Daily activities | No difficulty | 34 | 32.1 | 23.8 | – | 41.4 | 32 | 50.0 | 38.0 | – | 62.0 | 0.130 | ||||
| Slight difficulty | 24 | 22.6 | 15.5 | – | 31.3 | 10 | 15.6 | 8.3 | – | 25.9 | ||||||
| Some difficulty | 22 | 20.8 | 13.9 | – | 29.2 | 12 | 18.8 | 10.7 | – | 29.6 | ||||||
| Considerable | 19 | 17.9 | 11.5 | – | 26.0 | 8 | 12.5 | 6.1 | – | 22.2 | ||||||
| Could not do them | 7 | 6.6 | 3.0 | – | 12.5 | 2 | 3.1 | 0.7 | – | 9.6 | ||||||
| Newspaper vision | Yes | 47 | 44.3 | 35.1 | – | 53.8 | 31 | 48.4 | 36.5 | – | 60.5 | 0.611 | ||||
| No | 59 | 55.7 | 46.2 | – | 64.9 | 33 | 51.6 | 39.5 | – | 63.5 | ||||||
| Recognizing people | Yes | 31 | 29.2 | 21.2 | – | 38.4 | 17 | 26.6 | 16.9 | – | 38.2 | 0.632 | ||||
| No | 75 | 70.8 | 61.6 | – | 78.8 | 47 | 73.4 | 61.8 | – | 83.1 | ||||||
| Hearing | Yes | 51 | 48.1 | 38.8 | – | 57.6 | 42 | 65.6 | 53.5 | – | 76.4 | 0.039 | ||||
| No | 55 | 51.9 | 42.4 | – | 61.2 | 22 | 34.4 | 23.6 | – | 46.5 | ||||||
| Falls in the last 6 months | Yes | 34 | 32.1 | 23.8 | – | 41.4 | 13 | 20.3 | 11.9 | – | 31.3 | 0.122 | ||||
| No | 72 | 67.9 | 58.6 | – | 76.2 | 51 | 79.7 | 68.7 | – | 88.1 | ||||||
| Number of falls | 106 | 72 | 1.0 | 1.0 | – | 2.0 | 64 | 51 | 2.0 | 1.0 | – | 2.0 | 0.680 | |||
| Stress urinary incontinence | Never | 34 | 32.1 | 23.8 | – | 41.4 | 39 | 62.9 | 50.5 | – | 74.1 | 0.000 | ||||
| Rarely | 14 | 13.2 | 7.8 | – | 20.6 | 10 | 16.1 | 8.6 | – | 26.7 | ||||||
| Sometimes | 30 | 28.3 | 20.4 | – | 37.4 | 10 | 16.1 | 8.6 | – | 26.7 | ||||||
| Often | 18 | 17.0 | 10.8 | – | 25.0 | 2 | 3.2 | 0.7 | – | 9.9 | ||||||
| Always | 10 | 9.4 | 5.0 | – | 16.1 | 1 | 1.6 | 0.2 | – | 7.3 | ||||||
| Urgency urinary incontinence | Never | 31 | 29.2 | 21.2 | – | 38.4 | 36 | 58.1 | 45.6 | – | 69.7 | 0.001 | ||||
| Rarely | 13 | 12.3 | 7.1 | – | 19.5 | 8 | 12.9 | 6.3 | – | 22.9 | ||||||
| Sometimes | 30 | 28.3 | 20.4 | – | 37.4 | 13 | 21.0 | 12.3 | – | 32.3 | ||||||
| Often | 21 | 19.8 | 13.1 | – | 28.2 | 2 | 3.2 | 0.7 | – | 9.9 | ||||||
| Always | 11 | 10.4 | 5.6 | – | 17.2 | 3 | 4.8 | 1.4 | – | 12.4 | ||||||
| An influenza vaccination in the last 12 months | Yes | 92 | 86.8 | 79.4 | – | 92.2 | 56 | 87.5 | 77.8 | – | 93.9 | 0.955 | ||||
| No | 14 | 13.2 | 7.8 | – | 20.6 | 8 | 12.5 | 6.1 | – | 22.2 | ||||||
| Don’t know | 0 | 0.0 | – | 0 | 0.0 | – | ||||||||||
| A tetanus vaccination in the last 10 years | Yes | 50 | 47.2 | 37.8 | – | 56.6 | 31 | 48.4 | 36.5 | – | 60.5 | 0.444 | ||||
| No | 33 | 31.1 | 22.9 | – | 40.4 | 14 | 21.9 | 13.1 | – | 33.1 | ||||||
| Don’t know | 23 | 21.7 | 14.7 | – | 30.2 | 19 | 29.7 | 19.6 | – | 41.6 | ||||||
| A diphtheria vaccination in the last 10 years | Yes | 46 | 43.4 | 34.2 | – | 52.9 | 29 | 45.3 | 33.5 | – | 57.5 | 0.689 | ||||
| No | 34 | 32.1 | 23.8 | – | 41.4 | 16 | 25.0 | 15.7 | – | 36.5 | ||||||
| Don’t know | 26 | 24.5 | 17.1 | – | 33.3 | 19 | 29.7 | 19.6 | – | 41.6 | ||||||
| A pneumococcal vaccination in the last 10 years | Yes | 48 | 45.3 | 36.0 | – | 54.8 | 28 | 43.8 | 32.1 | – | 56.0 | 0.242 | ||||
| No | 31 | 29.2 | 21.2 | – | 38.4 | 12 | 18.8 | 10.7 | – | 29.6 | ||||||
| Don’t know | 27 | 25.5 | 17.9 | – | 34.3 | 24 | 37.5 | 26.4 | – | 49.7 | ||||||
| Depressed in the past month | Yes | 65 | 61.3 | 51.8 | – | 70.2 | 29 | 45.3 | 33.5 | – | 57.5 | 0.026 | ||||
| No | 41 | 38.7 | 29.8 | – | 48.2 | 35 | 54.7 | 42.5 | – | 66.5 | ||||||
| Little interest in doing things | Yes | 56 | 52.8 | 43.4 | – | 62.2 | 31 | 48.4 | 36.5 | – | 60.5 | 0.449 | ||||
| No | 50 | 47.2 | 37.8 | – | 56.6 | 33 | 51.6 | 39.5 | – | 63.5 | ||||||
| Person to help in an emergency | Yes | 96 | 90.6 | 83.9 | – | 95.0 | 60 | 93.8 | 85.8 | – | 97.9 | 0.600 | ||||
| No | 9 | 8.5 | 4.3 | – | 14.9 | 3 | 4.7 | 1.3 | – | 12.0 | ||||||
| Maybe | 1 | 0.9 | 0.1 | – | 4.3 | 1 | 1.6 | 0.2 | – | 7.1 | ||||||
| Trusted person | Yes | 104 | 98.1 | 94.1 | – | 99.6 | 64 | 100.0 | – | 0.532 | ||||||
| No | 2 | 1.9 | 0.4 | – | 5.9 | 0 | 0.0 | – | ||||||||
| Maybe | 0 | 0.0 | – | 0 | 0.0 | – | ||||||||||
| Clock-drawing test | 106 | 2 | 2.0 | 0.0 | – | 3.0 | 64 | 4 | 3.0 | 1.5 | – | 7.0 | 0.009 | |||
| Mobility | No problem | 24 | 22.6 | 15.5 | – | 31.3 | 26 | 40.6 | 29.2 | – | 52.9 | 0.048 | ||||
| Slight | 26 | 24.5 | 17.1 | – | 33.3 | 14 | 21.9 | 13.1 | – | 33.1 | ||||||
| Moderate | 29 | 27.4 | 19.6 | – | 36.4 | 15 | 23.4 | 14.4 | – | 34.8 | ||||||
| Severe | 24 | 22.6 | 15.5 | – | 31.3 | 8 | 12.5 | 6.1 | – | 22.2 | ||||||
| Could not do | 3 | 2.8 | 0.8 | – | 7.4 | 1 | 1.6 | 0.2 | – | 7.1 | ||||||
| Self-care | No problem | 59 | 55.7 | 46.2 | – | 64.9 | 44 | 68.8 | 56.8 | – | 79.1 | 0.302 | ||||
| Slight | 24 | 22.6 | 15.5 | – | 31.3 | 8 | 12.5 | 6.1 | – | 22.2 | ||||||
| Moderate | 18 | 17.0 | 10.8 | – | 25.0 | 8 | 12.5 | 6.1 | – | 22.2 | ||||||
| Severe | 3 | 2.8 | 0.8 | – | 7.4 | 2 | 3.1 | 0.7 | – | 9.6 | ||||||
| Could not do | 2 | 1.9 | 0.4 | – | 5.9 | 2 | 3.1 | 0.7 | – | 9.6 | ||||||
| Usual activities | No problem | 36 | 34.0 | 25.5 | – | 43.3 | 34 | 53.1 | 41.0 | – | 65.0 | 0.014 | ||||
| Slight | 33 | 31.1 | 22.9 | – | 40.4 | 16 | 25.0 | 15.7 | – | 36.5 | ||||||
| Moderate | 21 | 19.8 | 13.1 | – | 28.2 | 11 | 17.2 | 9.5 | – | 27.8 | ||||||
| Severe | 14 | 13.2 | 7.8 | – | 20.6 | 1 | 1.6 | 0.2 | – | 7.1 | ||||||
| Could not do | 2 | 1.9 | 0.4 | – | 5.9 | 2 | 3.1 | 0.7 | – | 9.6 | ||||||
| Pain/discomfort | No problem | 27 | 25.5 | 17.9 | – | 34.3 | 25 | 39.1 | 27.8 | – | 51.3 | 0.250 | ||||
| Slight | 29 | 27.4 | 19.6 | – | 36.4 | 19 | 29.7 | 19.6 | – | 41.6 | ||||||
| Moderate | 29 | 27.4 | 19.6 | – | 36.4 | 12 | 18.8 | 10.7 | – | 29.6 | ||||||
| Severe | 19 | 17.9 | 11.5 | – | 26.0 | 8 | 12.5 | 6.1 | – | 22.2 | ||||||
| Extreme | 2 | 1.9 | 0.4 | – | 5.9 | 0 | 0.0 | – | ||||||||
| Anxiety/depression | No problem | 36 | 34.0 | 25.5 | – | 43.3 | 37 | 57.8 | 45.6 | – | 69.3 | 0.005 | ||||
| Slight | 29 | 27.4 | 19.6 | – | 36.4 | 13 | 20.3 | 11.9 | – | 31.3 | ||||||
| Moderate | 20 | 18.9 | 12.3 | – | 27.1 | 12 | 18.8 | 10.7 | – | 29.6 | ||||||
| Severe | 18 | 17.0 | 10.8 | – | 25.0 | 2 | 3.1 | 0.7 | – | 9.6 | ||||||
| Extreme | 3 | 2.8 | 0.8 | – | 7.4 | 0 | 0.0 | – | ||||||||
| EQ VAS | 106 | 0 | 60.0 | 50.0 | – | 80.0 | 64 | 0 | 60.0 | 50.0 | – | 80.0 | 0.446 | |||
Appendix D
| N | Median | IQR * | p | ||||
|---|---|---|---|---|---|---|---|
| Daily activities | No difficulty | 66 | 73 | 50 | – | 90 | 0.000 |
| Slight difficulty | 34 | 60 | 50 | – | 70 | ||
| Some difficulty | 34 | 50 | 35 | – | 70 | ||
| Considerable | 27 | 50 | 40 | – | 60 | ||
| Could not do them | 9 | 50 | 30 | – | 70 | ||
| Newspaper vision | Yes | 78 | 50 | 40 | – | 75 | 0.005 |
| No | 92 | 70 | 50 | – | 80 | ||
| Recognizing people | Yes | 48 | 50 | 30 | – | 70 | 0.000 |
| No | 122 | 63 | 50 | – | 80 | ||
| Hearing | Yes | 93 | 60 | 50 | – | 80 | 0.398 |
| No | 77 | 60 | 40 | – | 75 | ||
| Falls in the last 6 months | Yes | 47 | 50 | 35 | – | 80 | 0.093 |
| No | 123 | 60 | 50 | – | 80 | ||
| Stress urinary incontinence | Never | 73 | 70 | 50 | – | 85 | 0.005 |
| Rarely | 24 | 60 | 50 | – | 80 | ||
| Sometimes | 40 | 55 | 50 | – | 78 | ||
| Often | 20 | 50 | 30 | – | 60 | ||
| Always | 11 | 50 | 30 | – | 80 | ||
| Urgency urinary incontinence | Never | 67 | 70 | 50 | – | 80 | 0.049 |
| Rarely | 21 | 50 | 50 | – | 60 | ||
| Sometimes | 43 | 60 | 50 | – | 80 | ||
| Often | 23 | 50 | 30 | – | 70 | ||
| Always | 14 | 70 | 30 | – | 90 | ||
| An influenza vaccination in the last 12 months | Yes | 148 | 60 | 50 | – | 80 | 0.402 |
| No | 22 | 65 | 50 | – | 85 | ||
| Don’t know | 0 | . | . | – | . | ||
| A tetanus vaccination in the last 10 years | Yes | 81 | 60 | 50 | – | 80 | 0.850 |
| No | 47 | 60 | 50 | – | 80 | ||
| Don’t know | 42 | 60 | 50 | – | 80 | ||
| A diphtheria vaccination in the last 10 years | Yes | 75 | 60 | 50 | – | 80 | 0.880 |
| No | 50 | 60 | 50 | – | 80 | ||
| Don’t know | 45 | 60 | 50 | – | 80 | ||
| A pneumococcal vaccination in the last 10 years | Yes | 76 | 60 | 50 | – | 80 | 0.440 |
| No | 43 | 70 | 50 | – | 90 | ||
| Don’t know | 51 | 60 | 50 | – | 75 | ||
| Depressed in the past month | Yes | 94 | 50 | 40 | – | 75 | 0.014 |
| No | 76 | 65 | 50 | – | 80 | ||
| Little interest in doing things | Yes | 87 | 55 | 40 | – | 80 | 0.089 |
| No | 83 | 60 | 50 | – | 80 | ||
| Person to help in an emergency | Yes | 156 | 60 | 50 | – | 80 | 0.055 |
| No | 12 | 50 | 30 | – | 60 | ||
| Maybe | 2 | 43 | 35 | – | 50 | ||
| Trusted person | Yes | 168 | 60 | 50 | – | 80 | 0.014 |
| No | 2 | 15 | 0 | – | 30 | ||
| Maybe | 0 | . | . | – | . | ||
| Mobility | No problem | 50 | 75 | 60 | – | 90 | 0.000 |
| Slight | 40 | 60 | 50 | – | 80 | ||
| Moderate | 44 | 60 | 50 | – | 70 | ||
| Severe | 32 | 45 | 30 | – | 65 | ||
| Could not do | 4 | 30 | 30 | – | 40 | ||
| Self-care | No problem | 103 | 60 | 50 | – | 80 | 0.005 |
| Slight | 32 | 60 | 50 | – | 80 | ||
| Moderate | 26 | 50 | 35 | – | 80 | ||
| Severe | 5 | 30 | 20 | – | 50 | ||
| Could not do | 4 | 35 | 30 | – | 45 | ||
| Usual activities | No problem | 70 | 70 | 55 | – | 80 | 0.000 |
| Slight | 49 | 60 | 50 | – | 80 | ||
| Moderate | 32 | 50 | 38 | – | 70 | ||
| Severe | 15 | 40 | 30 | – | 50 | ||
| Could not do | 4 | 30 | 20 | – | 40 | ||
| Pain/discomfort | No problem | 52 | 80 | 50 | – | 90 | 0.000 |
| Slight | 48 | 60 | 50 | – | 80 | ||
| Moderate | 41 | 60 | 50 | – | 65 | ||
| Severe | 27 | 50 | 30 | – | 55 | ||
| Extreme | 2 | 30 | 30 | – | 30 | ||
| Anxiety/depression | No problem | 73 | 60 | 50 | – | 80 | 0.000 |
| Slight | 42 | 70 | 50 | – | 80 | ||
| Moderate | 32 | 50 | 45 | – | 70 | ||
| Severe | 20 | 40 | 30 | – | 58 | ||
| Extreme | 3 | 35 | 30 | – | 40 | ||
Appendix E

References
- World Health Organization. Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health/ (accessed on 5 February 2018).
- Baraković, S.; Baraković Husić, J.; van Hoof, J.; Krejcar, O.; Maresova, P.; Akhtar, Z.; Melero, F.J. Quality of Life Framework for Personalised Ageing: A Systematic Review of ICT Solutions. Int. J. Environ. Res. Public Health 2020, 17, 2940. [Google Scholar] [CrossRef]
- Morley, J.E.; Arai, H.; Cao, L.; Dong, B.; Merchant, R.A.; Vellas, B.; Visvanathan, R.; Woo, J. Integrated Care: Enhancing the Role of the Primary Health Care Professional in Preventing Functional Decline: A Systematic Review. J. Am. Med. Dir. Assoc. 2017, 18, 489–494. [Google Scholar] [CrossRef] [PubMed]
- OMS. Informe Mundial Sobre El Envejecimiento y La Salud; OMS: Nueva York, NY, USA, 2015; pp. 100–131. [Google Scholar]
- Boeckxstaens, P.; Graff, P. International Exchange Primary Care and Care for Older Persons: Position Paper of the European Forum for Primary Care. Qual. Prim. Care 2011, 19, 369–389. [Google Scholar] [PubMed]
- Sandholzer, H.; Hellenbrand, W.; Renteln-Kruse, W.; Van Weel, C.; Walker, P. STEP—Europäische Leitlinie Für Das Standardisierte Evidenzbasierte Präventive Assessment Älterer Menschen in Der Medizinischen Primärversorgung. DMW-Dtsch. Med. Wochenschr. 2004, 129, S183–S226. [Google Scholar] [CrossRef] [PubMed]
- Seematter-Bagnoud, L.; Büla, C. Brief Assessments and Screening for Geriatric Conditions in Older Primary Care Patients: A Pragmatic Approach. Public Health Rev. 2018, 39, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Barkhausen, T.; Junius-Walker, U.; Hummers-Pradier, E.; Mueller, C.A.; Theile, G. “It’s MAGIC”–Development of a Manageable Geriatric Assessment for General Practice Use. BMC Fam. Pract. 2015, 16, 4. [Google Scholar] [CrossRef] [Green Version]
- EuroQol Research Foundation. EQ-5D-5L User Guide. 2019. Available online: https://euroqol.org/publications/user-guides (accessed on 15 September 2020).
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P.; ISPOR Task Force for Translation and Cultural Adaptation. Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef] [Green Version]
- Guillemin, F.; Bombardier, C.; Beaton, D. Cross-Cultural Adaptation of Health-Related Quality of Life Measures: Literature Review and Proposed Guidelines. J. Clin. Epidemiol. 1993, 46, 1417–1432. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- Grau Fibla, G.; Eiroa Patiño, P.; Cayuela Domínguez, A. Spanish Version of the OARS Multidimensional Functional Assessment Questionnaire: Cross-Cultural Adaptation and Validity Measurement. Atencion Primaria 1996, 17, 486–495. [Google Scholar]
- Whooley, M.A.; Avins, A.L.; Miranda, J.; Browner, W.S. Case-Finding Instruments for Depression. Two Questions Are as Good as Many. J. Gen. Intern. Med. 1997, 12, 439–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López Alonso, S.R.; Martínez Sánchez, C.M.; Romero Cañadillas, A.B.; Angel Rueda, M. Validez y Fiabilidad Del Cuestionario COOP/WONCA Cumplimentado Vía Telefónica En Personas Con Artrosis de Cadera y Rodilla. Index de Enfermería 2005, 14, 24–28. [Google Scholar] [CrossRef]
- Thalmann, B.; Spiegel, R.; Stähelin, H.B. Dementia Screening in General Practice: Optimised Scoring for the Clock Drawing Test. Brain Aging Int. J. 2002, 2, 36–43. [Google Scholar]
- Grupo de trabajo vacunación frente a neumococo en grupos de riesgo 2015 de la Ponencia de Programas y Registro de Vacunaciones. In Utilización de la Vacuna Frente a Neumococo en Grupos de Riesgo; Comisión de Salud Pública del Consejo Interterritorial del Sistema Nacional de Salud; Ministerio de Sanidad, Servicios Sociales e Igualdad: Madrid, Spain, 2015.
- Murphy, M.; Hollinghurst, S.; Salisbury, C. Identification, Description and Appraisal of Generic PROMs for Primary Care: A Systematic Review. BMC Fam. Pract. 2018, 19, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoyos Alonso, M.C.; Gorroñogoitia Iturbe, A.; Martín Lesende, I.; Baena Díez, J.M.; López-Torres Hidalgo, J.; Magán Tapia, P.; Acosta Benito, M.Á.; Herreros Herreros, Y. Actividades Preventivas En Los Mayores. Actualización PAPPS 2018. Atención Primaria 2018, 50, 109–124. [Google Scholar] [CrossRef]
- Cervantes Becerra, R.G.; Villarreal Ríos, E.; Galicia Rodríguez, L.; Vargas Daza, E.R.; Martínez González, L. Estado de Salud En El Adulto Mayor En Atención Primaria a Partir de Una Valoración Geriátrica Integral. Atención Primaria 2015, 47, 329–335. [Google Scholar] [CrossRef] [Green Version]
- Suárez Cardona, M.; Neira León, M.; Pastor Sanz, M.T.; De los Santos Ichaso Hernàndez-Rubio, M. Encuesta Nacional De Salud Serie 2011/2012; Ministerio de sanidad, servicios sociales e igualdad: Madrid, Spain, 2012; pp. 1–46. [Google Scholar]
- Liu, C.; Wang, D.; Liu, C.; Jiang, J.; Wang, X.; Chen, H.; Ju, X.; Zhang, X. What Is the Meaning of Health Literacy? A Systematic Review and Qualitative Synthesis. Fam. Med. Com. Health 2020, 8, e000351. [Google Scholar] [CrossRef]
- Nolasco, A.; Barona, C.; Tamayo-Fonseca, N.; Irles, M.Á.; Más, R.; Tuells, J.; Pereyra-Zamora, P. Alfabetización En Salud: Propiedades Psicométricas Del Cuestionario HLS-EU-Q16. Gac. Sanit. 2020, 34, 399–402. [Google Scholar] [CrossRef]
- Mueller, Y.K.; Monod, S.; Locatelli, I.; Büla, C.; Cornuz, J.; Senn, N. Performance of a Brief Geriatric Evaluation Compared to a Comprehensive Geriatric Assessment for Detection of Geriatric Syndromes in Family Medicine: A Prospective Diagnostic Study. BMC Geriatr. 2018, 18, 72. [Google Scholar] [CrossRef] [Green Version]
- Locatelli, I.; Monod, S.; Cornuz, J.; Büla, C.J.; Senn, N. A Prospective Study Assessing Agreement and Reliability of a Geriatric Evaluation. BMC Geriatr. 2017, 17, 153. [Google Scholar] [CrossRef] [Green Version]
- Sabbagh, M.; Boada, M.; Borson, S.; Chilukuri, M.; Dubois, B.; Ingram, J.; Iwata, A.; Porsteinsson, A.; Possin, K.; Rabinovici, G.; et al. Early Detection of Mild Cognitive Impairment (MCI) in Primary Care. J. Prev. Alzheimer’s Dis. 2020, 7, 1–6. [Google Scholar] [CrossRef]
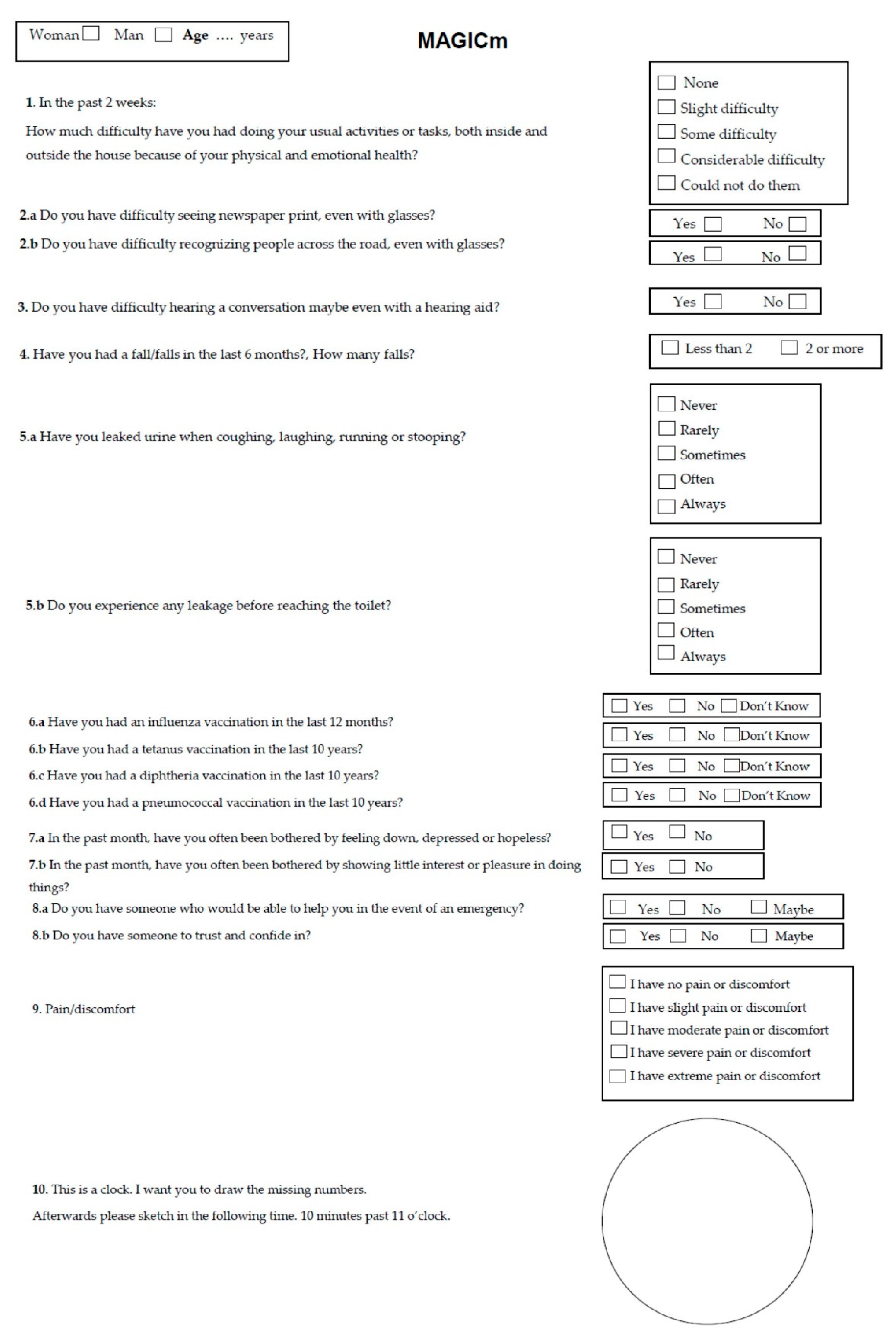
- Clavería, A.; Dios-Quiroga, F.; Pallas, M.; Soliño-Lourido, S.; González-Formoso, C. Effectiveness of a multidimensional geriatric assessment (MAGICm questionnaire) in elderly patients quality of life in primary care. In Proceedings of the Programme Book of the 89th EGPRN Meeting, Vigo, Spain, 17–20 October 2019. [Google Scholar]

| Domains | Items | Response Scale | Scoring | Direction |
|---|---|---|---|---|
| Daily activities | In the past 2 weeks: how much difficulty have you had doing your usual activities or tasks, both inside and outside the house because of your physical and emotional health? | None, slight, some, considerable or could not do them | No | |
| Vision | Do you have difficulty seeing newspaper print, even with glasses? | Yes or No | No | |
| Do you have difficulty recognizing people across the road, even with glasses? | Yes or No | No | ||
| Hearing | Do you have difficulty hearing a conversation maybe even with a hearing aid? | Yes or No | No | |
| Falls | Have you had a fall/falls in the last 6 months? How many falls? | Less than 2 or 2 or more | No | |
| Urinary incontinence | Have you leaked urine when coughing, laughing, running or stooping? | Never, Rarely, Sometimes, Often or Always | No | |
| Do you experience any leakage before reaching the toilet? | Never, Rarely, Sometimes, Often or Always | No | ||
| Immunization | Have you had an influenza vaccination in the last 12 months? | Yes, No or Don’t Know | No | |
| Have you had a tetanus vaccination in the last 10 years? | Yes, No or Don’t Know | No | ||
| Have you had a diphtheria vaccination in the last 10 years? | Yes, No or Don’t Know | No | ||
| Have you had a pneumococcal vaccination in the last 10 years? | Yes, No or Don’t Know | No | ||
| Depression | In the past month, have you often been bothered by feeling down, depressed or hopeless? | Yes or No | No | |
| In the past month, have you often been bothered by showing little interest or pleasure in doing things? | Yes or No | No | ||
| Social environment | Do you have someone who would be able to help you in the event of an emergency? | Yes, No or Maybe | No | |
| Do you have someone to trust and confide in? | Yes, No or Maybe | No | ||
| Cognition | The clock-drawing test | 1–7 points | <5 (Problem) or ≥5 (No Problem) |
| N (%) N = 170 * | 95% CI | ||||
|---|---|---|---|---|---|
| Daily activities | No difficulty | 66 (38.8%) | 31.7 | – | 46.3 |
| A little difficulty | 34 (20.0%) | 14.5 | – | 26.5 | |
| Some difficulty | 34 (20.0%) | 14.5 | – | 26.5 | |
| Considerable | 27 (15.9%) | 11.0 | – | 21.9 | |
| Could not do them | 9 (5.3%) | 2.7 | – | 9.4 | |
| Newspaper vision | Yes | 78 (45.9%) | 38.5 | – | 53.4 |
| No | 92 (54.1%) | 46.6 | – | 61.5 | |
| Recognizing people | Yes | 48 (28.2%) | 21.9 | – | 35.3 |
| No | 122 (71.8%) | 64.7 | – | 78.1 | |
| Hearing | Yes | 93 (54.7%) | 47.2 | – | 62.1 |
| No | 77 (45.3%) | 37.9 | – | 52.8 | |
| Falls in the last 6 months | Yes | 47 (27.6%) | 21.3 | – | 34.7 |
| No | 123 (72.4%) | 65.3 | – | 78.7 | |
| Number of falls | 1.0 | 1.0 | – | 2.0 | |
| Stress urinary incontinence | Never | 73 (43.5%) | 36.1 | – | 51.0 |
| Rarely | 24 (14.3%) | 9.6 | – | 20.2 | |
| Sometimes | 40 (23.8%) | 17.9 | – | 30.7 | |
| Often | 20 (11.9%) | 7.7 | – | 17.4 | |
| Always | 11 (6.5%) | 3.5 | – | 11.0 | |
| Urgency urinary incontinence | Never | 67 (39.9%) | 32.7 | – | 47.4 |
| Rarely | 21 (12.5%) | 8.1 | – | 18.1 | |
| Sometimes | 43 (25.6%) | 19.5 | – | 32.6 | |
| Often | 23 (13.7%) | 9.1 | – | 19.5 | |
| Always | 14 (8.3%) | 4.9 | – | 13.2 | |
| An influenza vaccination in the last 12 months | Yes | 148 (87.1%) | 81.4 | – | 91.5 |
| No | 22 (12.9%) | 8.5 | – | 18.6 | |
| Don’t know | 0 | ||||
| A tetanus vaccination in the last 10 years | Yes | 81 (47.6%) | 40.2 | – | 55.1 |
| No | 47 (27.6%) | 21.3 | – | 34.7 | |
| Don’t know | 42 (24.7%) | 18.7 | – | 31.6 | |
| A diphtheria vaccination in the last 10 years | Yes | 75 (44.1%) | 36.8 | – | 51.6 |
| No | 50 (29.4%) | 23.0 | – | 36.6 | |
| Don’t know | 45 (26.5%) | 20.3 | – | 33.5 | |
| A pneumococcal vaccination in the last 10 years | Yes | 76 (44.7%) | 37.4 | – | 52.2 |
| No | 43 (25.3%) | 19.2 | – | 32.2 | |
| Don’t know | 51 (30%) | 23.5 | – | 37.2 | |
| Depressed in the past month | Yes | 94 (55.3%) | 47.8 | – | 62.6 |
| No | 76 (44.7%) | 37.4 | – | 52.2 | |
| Little interest doing things | Yes | 87 (51.2%) | 43.7 | – | 58.6 |
| No | 83 (48.8%) | 41.4 | – | 56.3 | |
| Person to help in an emergency | Yes | 156 (91.8%) | 86.9 | – | 95.2 |
| No | 12 (7.1%) | 3.9 | – | 11.6 | |
| Maybe | 2 (1.2%) | 0.2 | – | 3.7 | |
| Trusted person | Yes | 168 (98.8%) | 96.3 | – | 99.8 |
| No | 2 (1.2%) | 0.2 | – | 3.7 | |
| Maybe | 0 | ||||
| Clock-drawing test (Median/IQR) | 3 | 1.0 | – | 5.0 | |
| N (%) N = 170 * | 95% CI | ||||
|---|---|---|---|---|---|
| Mobility | No problem | 50 (29.4%) | 23.0 | – | 36.6 |
| Slight | 40 (23.5%) | 17.6 | – | 30.3 | |
| Moderate | 44 (25.9%) | 19.7 | – | 32.8 | |
| Severe | 32 (18.8%) | 13.5 | – | 25.2 | |
| Could not do | 4 (2.4%) | 0.8 | – | 5.5 | |
| Self-care | No problem | 103 (60.6%) | 53.1 | – | 67.7 |
| Slight | 32 (18.8%) | 13.5 | – | 25.2 | |
| Moderate | 26 (15.3%) | 10.5 | – | 21.3 | |
| Severe | 5 (2.9%) | 1.1 | – | 6.3 | |
| Could not do | 4 (2.4%) | 0.8 | – | 5.5 | |
| Usual activities | No problem | 70 (41.2%) | 34.0 | – | 48.7 |
| Slight | 49 (28.8%) | 22.4 | – | 35.9 | |
| Moderate | 32 (18.8%) | 13.5 | – | 25.2 | |
| Severe | 15 (8.8%) | 5.2 | – | 13.8 | |
| Could not do | 4 (2.4%) | 0.8 | – | 5.5 | |
| Pain/discomfort | No problem | 52 (30.6%) | 24.0 | – | 37.8 |
| Slight | 48 (28.2%) | 21.9 | – | 35.3 | |
| Moderate | 41 (24.1%) | 18.2 | – | 30.9 | |
| Severe | 27 (15.9%) | 11.0 | – | 21.9 | |
| Extreme | 2 (1.2%) | 0.2 | – | 3.7 | |
| Anxiety/depression | No problem | 73 (42.9%) | 35.7 | – | 50.4 |
| Slight | 42 (24.7%) | 18.7 | – | 31.6 | |
| Moderate | 32 (18.8%) | 13.5 | – | 25.2 | |
| Severe | 20 (11.8%) | 7.6 | – | 17.2 | |
| Extreme | 3 (1.8%) | 0.5 | – | 4.6 | |
| EQ VAS (Median/IQR) | 60.0 | 50.0 | – | 80.0 | |
| Coefficient | 95% CI | p | |||
|---|---|---|---|---|---|
| Interception | 13.631 | −19.49 | – | 46.753 | 0.418 |
| Daily activities = None and a little difficulty. | 10.468 | 3.464 | – | 17.472 | 0.004 |
| Daily activities = Some, considerable and could not do them. | 0 | ||||
| Stress urinary incontinence = Never. | 13.359 | 3.789 | – | 22.930 | 0.007 |
| Stress urinary incontinence = Rarely and sometimes. | 6.217 | −3.486 | – | 15.920 | 0.208 |
| Stress urinary incontinence = Often and always. | 0 | ||||
| Recognizing people = Yes | −10.014 | −17.64 | – | −2.393 | 0.01 |
| Recognizing people = No | 0 | ||||
| Person to help in an emergency = Yes | 10.332 | −1.804 | – | 22.468 | 0.095 |
| Person to help in an emergency = No | 0 | ||||
| Trusted person = Yes | 26.097 | −5.553 | – | 57.746 | 0.105 |
| Trusted person = No | 0 | ||||
| Coefficient | 95% CI | p | |||
|---|---|---|---|---|---|
| Interception | 29.884 | 19.341 | – | 40.43 | 0.000 |
| Mobility = No problem. | 19.658 | 9.787 | – | 29.53 | 0.000 |
| Mobility = Slight and moderate. | 12.21 | 3.617 | – | 20.8 | 0.006 |
| Mobility = Severe and could not do. | 0 | ||||
| Anxiety/depression = No problem and slight. | 15.329 | 5.420 | – | 25.24 | 0.003 |
| Anxiety/depression = Moderate. | 8.044 | −3.398 | – | 19.46 | 0.167 |
| Anxiety/depression = Severe and extreme. | 0 | ||||
| Pain/discomfort = No problem. | 14.248 | 3.589 | – | 24.91 | 0.009 |
| Pain/discomfort = Slight and moderate. | 4.665 | −4.785 | – | 14.12 | 0.331 |
| Pain/discomfort = Severe and extreme. | 0 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dios-Quiroga, F.; Soliño-Lourido, S.; Pallas-Queijo, C.; González-Formoso, C.; Constenla-Castro, A.; Conde-Freire, S.; Clavería, A. Multidimensional Geriatric Assessment with MAGIC Questionnaire and Quality of Life in Elderly Primary Care Patients. Int. J. Environ. Res. Public Health 2020, 17, 7089. https://doi.org/10.3390/ijerph17197089
Dios-Quiroga F, Soliño-Lourido S, Pallas-Queijo C, González-Formoso C, Constenla-Castro A, Conde-Freire S, Clavería A. Multidimensional Geriatric Assessment with MAGIC Questionnaire and Quality of Life in Elderly Primary Care Patients. International Journal of Environmental Research and Public Health. 2020; 17(19):7089. https://doi.org/10.3390/ijerph17197089
Chicago/Turabian StyleDios-Quiroga, Fátima, Susana Soliño-Lourido, Carmen Pallas-Queijo, Clara González-Formoso, Aurelia Constenla-Castro, Soledad Conde-Freire, and Ana Clavería. 2020. "Multidimensional Geriatric Assessment with MAGIC Questionnaire and Quality of Life in Elderly Primary Care Patients" International Journal of Environmental Research and Public Health 17, no. 19: 7089. https://doi.org/10.3390/ijerph17197089