
Effectiveness of Conservative Treatment According to Severity and Systemic Disease in Carpal Tunnel Syndrome: A Systematic Review

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Register
2.2. Information Sources and Search
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Data Extraction Process
2.6. Risk of Bias in the Individual Studies
3. Results
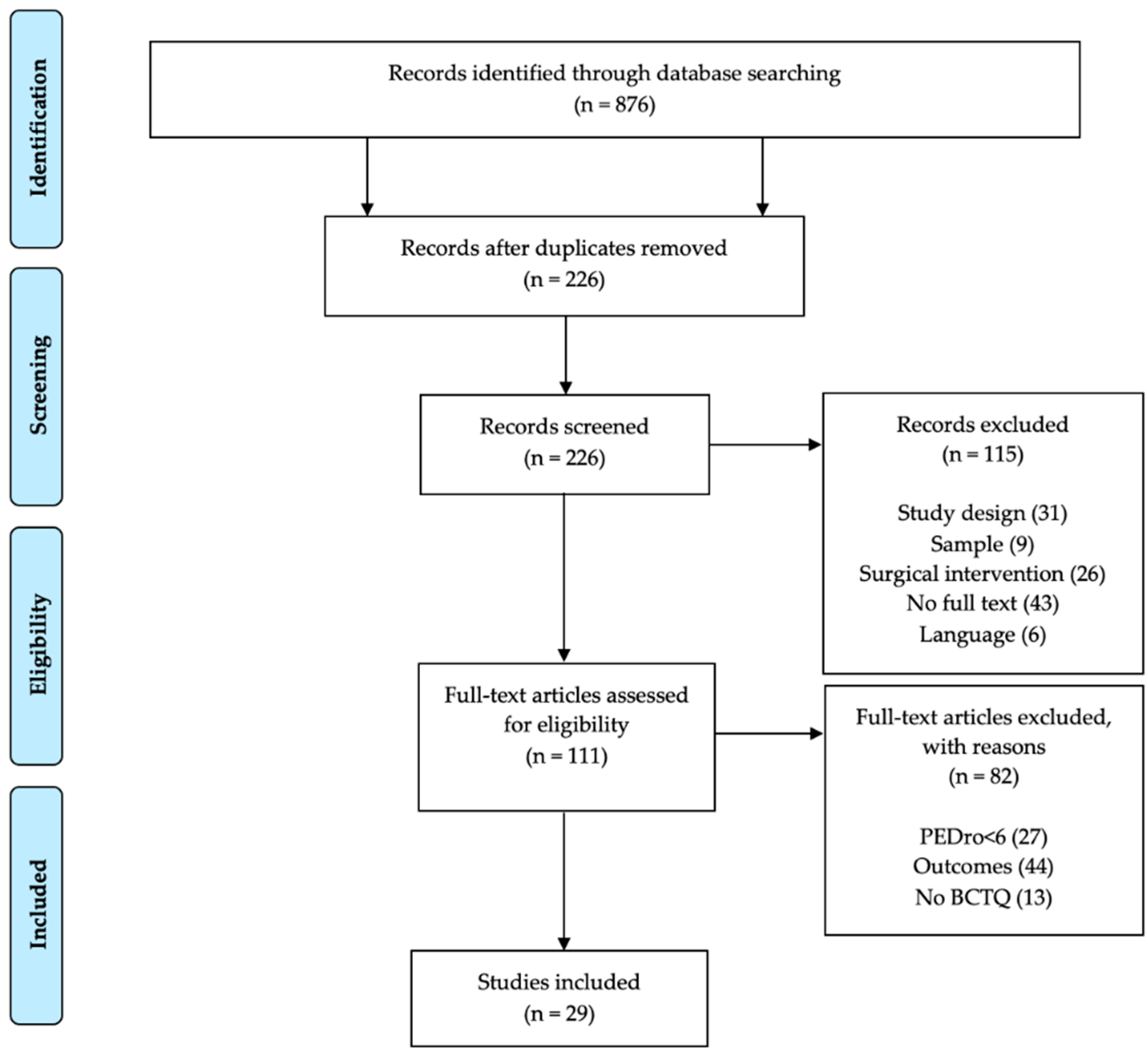
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Sample
3.2.2. Intervention
3.2.3. Variables
3.2.4. Follow-Up
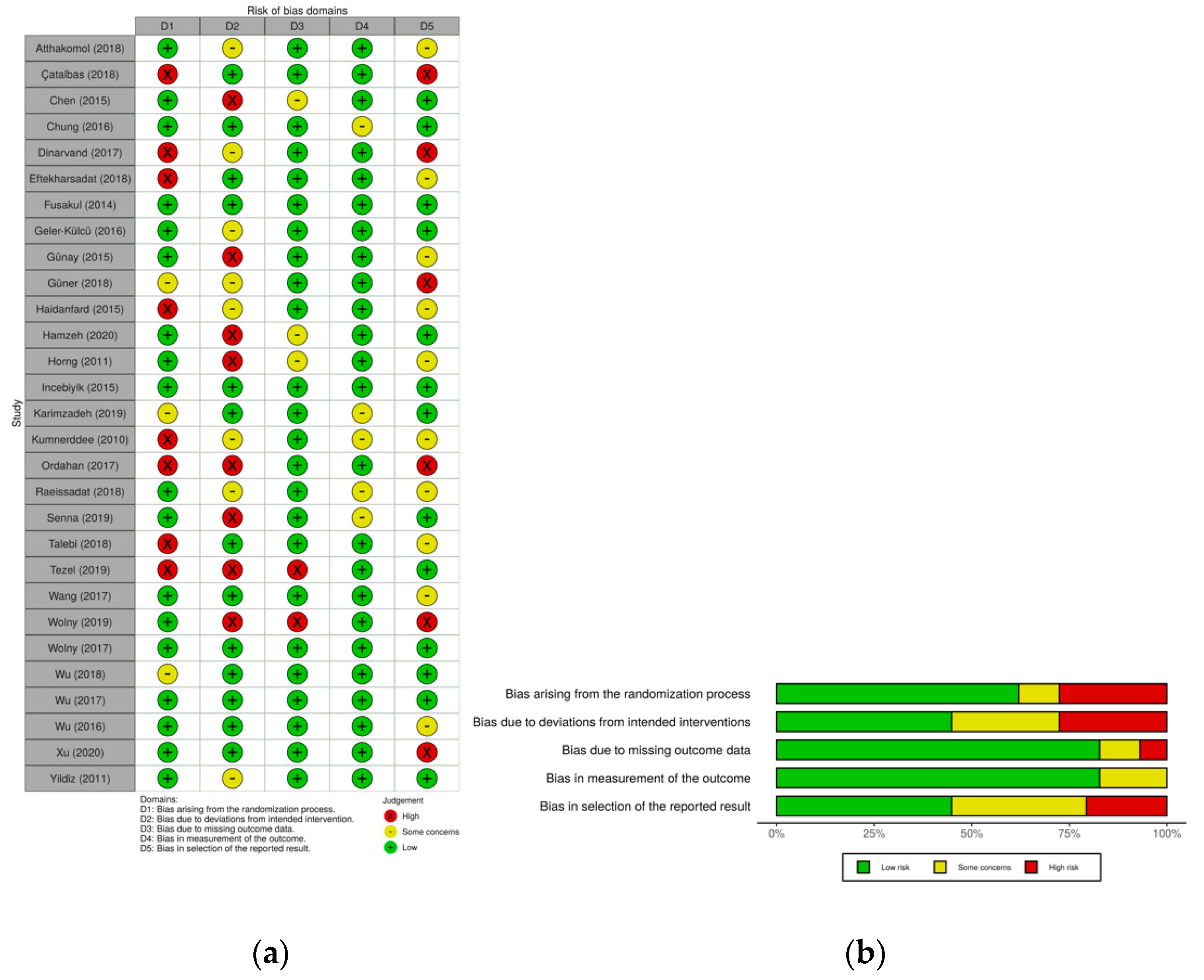
3.2.5. Evaluation of the Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wipperman, J.; Goerl, K. Diagnosis and management of carpal tunnel syndrome. J. Musculoskelet. Med. 2016, 94, 47–60. [Google Scholar]
- Atroshi, I.; Gummesson, C.; Johnsson, R.; Ornstein, E.; Ranstam, J.; Rosén, I. Prevalence of Carpal Tunnel Syndrome in a General Population. JAMA 1999, 282, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, T.; Kortlever, J.T.; Shapiro, L.M.; Baker, L.; Harris, A.H.; Kamal, R.N. The Influence of Cost Information on Treatment Choice: A Mixed-Methods Study. J. Hand Surg. 2020, 45, 899–908.e4. [Google Scholar] [CrossRef] [PubMed]
- Erickson, M.; Lawrence, M.; Stegink Jansen, C.; Coker, D.; Amadio, P.; Cleary, C. Carpal Tunnel Syndrome: A Summary of Clinical Practice Guideline Recommendations-Using the Evidence to Guide Physical Therapist Practice. J. Orthop. Sports Phys. Ther. 2019, 49, 359–360. [Google Scholar]
- Padua, L.; Coraci, D.; Erra, C.; Pazzaglia, C.; Paolasso, I.; Loreti, C.; Caliandro, P.; Hobson-Webb, L.D. Carpal tunnel syndrome: Clinical features, diagnosis, and management. Lancet Neurol. 2016, 15, 1273–1284. [Google Scholar] [CrossRef]
- Lin, Y.-N.; Chiu, C.-C.; Huang, S.-W.; Hsu, W.-Y.; Liou, T.-H.; Chen, Y.-W.; Chang, K.-H. Association between Manual Loading and Newly Developed Carpal Tunnel Syndrome in Subjects with Physical Disabilities: A Follow-Up Study. Arch. Phys. Med. Rehabilit. 2017, 98, 2002–2008. [Google Scholar] [CrossRef] [PubMed]
- Schmid, A.B.; Fundaun, J.; Tampin, B. Entrapment neuropathies: A contemporary approach to pathophysiology, clinical assessment, and management. PAIN Rep. 2020, 5, e829. [Google Scholar] [CrossRef]
- Moradi, A.; Sadr, A.; Ebrahimzadeh, M.H.; Hassankhani, G.G.; Mehrad-Majd, H. Does diabetes mellitus change the carpal tunnel release outcomes? Evidence from a systematic review and meta-analysis. J. Hand Ther. 2020, 1–7. [Google Scholar] [CrossRef]
- Pourmemari, M.H.; Shiri, R. Diabetes as a risk factor for carpal tunnel syndrome: A systematic review and meta-analysis. Diabet. Med. 2016, 33, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, J.; Castro, G.; Rojas, W.; Palacios, E. Frecuencia y evolución de la polineuropatía en pacientes hipotiroideos no controlados. Acta Neurol. Colomb. 2002, 18, 83–87. [Google Scholar]
- Ibrahim, I.; Khan, W.; Goddard, N.; Smitham, P. Carpal Tunnel Syndrome: A Review of the Recent Literature. Open Orthop. J. 2012, 6, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Zyluk-Gadowska, P.; Zyluk, A. Factors Affecting the Outcomes of Carpal Tunnel Surgery: A Review. Handchir. Mikrochir. Plast. Chir. 2016, 48, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Jiménez del Barrio, S.; Bueno Gracia, E.; Hidalgo García, C.; Estébanez de Miguel, E.; Tricás Moreno, J.M.; Rodríguez Marco, S. Tratamiento conservador en pacientes con síndrome del túnel carpiano con intensidad leve o moderada. Revisión sistemática. Neurología 2018, 33, 590–601. [Google Scholar] [CrossRef] [PubMed]
- Zyluk, A.; Strychar, J. Results of the treatment of carpal tunnel syndrome—A review. Chir. Narzadow. Ruch. Ortop. Polska 2005, 70, 439–445. [Google Scholar]
- Perkins, B.A.; Olaleye, D.; Bril, V. Carpal Tunnel Syndrome in Patients with Diabetic Polyneuropathy. Diabetes Care 2002, 25, 565–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afshar, A.; Tabrizi, A.; Tajbakhsh, M.; Navaeifar, N. Subjective Outcomes of Carpal Tunnel Release in Patients with Diabetes and Patients without Diabetes. J. Hand Microsurg. 2020, 12, 183–188. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.; Ioannidis, J. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, 1–2. [Google Scholar] [CrossRef]
- Leite, J.C.D.C.; Jerosch-Herold, C.; Song, F. A systematic review of the psychometric properties of the Boston Carpal Tunnel Questionnaire. BMC Musculoskelet. Disord. 2006, 7, 78–79. [Google Scholar] [CrossRef] [Green Version]
- Herbert, R.; Moseley, A.; Sherrington, C.; Maher, C. Escala PEDro-Español. Physiotherapy 2000, 86, 55. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.-T.; Ke, M.-J.; Chou, Y.-C.; Chang, C.-Y.; Lin, C.-Y.; Li, T.-Y.; Shih, F.-M.; Chen, L.-C. Effect of radial shock wave therapy for carpal tunnel syndrome: A prospective randomized, double-blind, placebo-controlled trial. J. Orthop. Res. 2015, 34, 977–984. [Google Scholar] [CrossRef]
- Chen, L.C.; Ho, C.W.; Sun, C.H.; Lee, J.T.; Li, T.Y.; Shih, F.M. Ultrasound-Guided Pulsed Radiofrequency for Carpal Tunnel Syndrome: A Single-Blinded Randomized Controlled Study. PLoS ONE 2015, 10, e0129918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talebi, G.A.; Saadat, P.; Javadian, Y.; Taghipour, M. Manual therapy in the treatment of carpal tunnel syndrome in diabetic patients: A randomized clinical trial. Casp. J. Intern. Med. 2018, 9, 283–289. [Google Scholar]
- Atthakomol, P.; Manosroi, W.; Phanphaisarn, A.; Phrompaet, S.; Iammatavee, S.; Tongprasert, S. Comparison of single-dose radial extracorporeal shock wave and local corticosteroid injection for treatment of carpal tunnel syndrome including mid-term efficacy: A prospective randomized controlled trial. BMC Musculoskelet. Disord. 2018, 19, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, V.C.H.; Ho, R.S.T.; Liu, S.; Chong, M.K.C.; Leung, A.W.N.; Yip, B.H.K. Electroacupuncture and splinting versus splinting alone to treat carpal tunnel syndrome: A randomized controlled trial. Can. Med. Assoc. J. 2016, 188, 867–875. [Google Scholar] [CrossRef] [Green Version]
- Hamzeh, H.; Madi, M.; Alghwiri, A.A.; Hawamdeh, Z. The long term effect of neurodynamics vs. exercise therapy on pain and function in people with carpal tunnel syndrome: A randomized parallel-group clinical trial. J. Hand Ther. 2020, 20, 30144–30147. [Google Scholar] [CrossRef]
- Horng, Y.S.; Hsieh, S.F.; Tu, Y.K.; Lin, M.C. The comparative effectiveness of tendon and nerve gliding exercises in patients with carpal tunnel syndrome: A randomized trial. Am. J. Phys. Med. Rehabil. 2011, 90, 435–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tezel, N.; Umay, E.; Yılmaz, V.; Cakci, A. Acupuncture plus night splint for quality of life and disability in patients with carpal tunnel syndrome: A randomized controlled trial. Integr. Med. Res. 2019, 8, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-T.T.; Ho, T.-Y.Y.; Chou, Y.-C.C.; Ke, M.-J.J.; Li, T.-Y.Y.; Tsai, C.-K.K. Six-month Efficacy of Perineural Dextrose for Carpal Tunnel Syndrome: A Prospective, Randomized, Double-Blind, Controlled Trial. Mayo Clin. Proc. 2017, 92, 1179–1189. [Google Scholar] [CrossRef]
- Wolny, T.; Saulicz, E.; Linek, P.; Shacklock, M.; Myśliwiec, A.; Wolny, T. Efficacy of Manual Therapy Including Neurodynamic Techniques for the Treatment of Carpal Tunnel Syndrome: A Randomized Controlled Trial. J. Manip. Physiol. Ther. 2017, 40, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-T.; Ho, T.-Y.; Chou, Y.-C.; Ke, M.-J.; Li, T.-Y.; Huang, G.-S.; Chen, L.-C. Six-month efficacy of platelet-rich plasma for carpal tunnel syndrome: A prospective randomized, single-blind controlled trial. Sci. Rep. 2017, 7, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimzadeh, A.; Bagheri, S.; Raeissadat, S.A.; Bagheri, S.; Rayegani, S.M.; Rahimi-Dehgolan, S.; Safdari, F.; Abrishamkarzadeh, H.; Shirzad, H. The comparison of the effectiveness between different doses of local methylprednisolone injection versus triamcinolone in Carpal Tunnel Syndrome: A double-blind clinical trial. J. Pain Res. 2019, 12, 579–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raeissadat, S.A.; Karimzadeh, A.; Hashemi, M.; Bagherzadeh, L. Safety and efficacy of platelet-rich plasma in treatment of carpal tunnel syndrome; a randomized controlled trial. BMC Musculoskelet. Disord. 2018, 19, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senna, M.K.; Shaat, R.M.; Ali, A.A.A. Platelet-rich plasma in treatment of patients with idiopathic carpal tunnel syndrome. Clin. Rheumatol. 2019, 38, 3643–3654. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.C.; Liao, K.K.; Lin, K.-P.; Chou, C.-L.; Yang, T.-F.; Huang, Y.-F. Efficacy of Combined Ultrasound-Guided Steroid Injection and Splinting in Patients with Carpal Tunnel Syndrome: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2017, 98, 947–956. [Google Scholar] [CrossRef]
- Wu, Y.-T.; Ke, M.-J.; Ho, T.-Y.; Li, T.-Y.; Shen, Y.-P.; Chen, L.-C. Randomized double-blinded clinical trial of 5% dextrose versus triamcinolone injection for carpal tunnel syndrome patients. Ann. Neurol. 2018, 84, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Çatalbas, N.; Akkaya, N.; Atalay, N.S.; Sahin, F. Ultrasonographic imaging of the effects of continuous, pulsed or sham ultrasound treatments on carpal tunnel syndrome: A randomized controlled study. J. Back Musculoskelet. Rehabil. 2018, 31, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Fusakul, Y.; Aranyavalai, T.; Saensri, P.; Thiengwittayaporn, S. Low-level laser therapy with a wrist splint to treat carpal tunnel syndrome: A double-blinded randomized controlled trial. Lasers Med. Sci. 2014, 29, 1279–1287. [Google Scholar] [CrossRef]
- Güner, A.; Altan, L.; Aksoy, M.K. The effectiveness of the low-power laser and kinesiotaping in the treatment of carpal tunnel syndrome, a pilot study. Rheumatol. Int. 2018, 38, 895–904. [Google Scholar] [CrossRef]
- Incebiyik, S.; Boyaci, A.; Tutoglu, A. Short-term effectiveness of short-wave diathermy treatment on pain, clinical symptoms, and hand function in patients with mild or moderate idiopathic carpal tunnel syndrome. J. Back Musculoskelet. Rehabil. 2015, 28, 221–228. [Google Scholar] [CrossRef]
- Kumnerddee, W.; Kaewtong, A. Efficacy of acupuncture versus night splinting for carpal tunnel syndrome: A randomized clinical trial. J. Med. Assoc. Thail. 2010, 93, 1463–1469. [Google Scholar]
- Geler Külcü, D.; Bursali, C.; Aktaş, İ.; Bozkurt Alp, S.; Ünlü Özkan, F.; Akpinar, P. Kinesiotaping as an alternative treatment method for carpal tunnel syndrome. Turk. J. Med. Sci. 2016, 46, 1042–1049. [Google Scholar] [CrossRef] [PubMed]
- Gunay, B.; Alp, A. The effectiveness of carpal bone mobilization accompanied by night splinting in idiopathic carpal tunnel syndrome. Turkish. J. Phys. Med. Rehabil. 2015, 61, 45–50. [Google Scholar] [CrossRef]
- Hadianfard, M.; Bazrafshan, E.; Momeninejad, H.; Jahani, N. Efficacies of Acupuncture and Anti-inflammatory Treatment for Carpal Tunnel Syndrome. J. Acupunct. Meridian Stud. 2015, 8, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Wolny, T.; Linek, P. Is manual therapy based on neurodynamic techniques effective in the treatment of carpal tunnel syndrome? A randomized controlled trial. Clin. Rehabil. 2018, 33, 408–417. [Google Scholar] [CrossRef]
- Dinarvand, V.; Abdollahi, I.; Raeissadat, S.A.; Bandpei, M.A.M.; Babaee, M.; Talimkhani, A. The Effect of Scaphoid and Hamate Mobilization on Treatment of Patients with Carpal Tunnel Syndrome. Anesthesiol. Pain Med. 2017, 7, e14621. [Google Scholar] [CrossRef] [Green Version]
- Xu, D.; Ma, W.; Jiang, W.; Hu, X.; Jiang, F.; Mao, C.; Wang, Y.; Fang, L.; Luo, N.; Li, H.; et al. A randomized controlled trial: Comparing extracorporeal shock wave therapy versus local corticosteroid injection for the treatment of carpal tunnel syndrome. Int. Orthop. 2020, 44, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, N.; Atalay, N.S.; Gungen, G.O.; Sanal, E.; Akkaya, N.; Topuz, O. Comparison of ultrasound and ketoprofen phonophoresis in the treatment of carpal tunnel syndrome. J. Back Musculoskelet. Rehabil. 2011, 24, 39–47. [Google Scholar] [CrossRef]
- Eftekharsadat, B.; Roomizadeh, P.; Torabi, S.; Heshmati-Afshar, F.; Jahanjoo, F.; Babaei-Ghazani, A. Effectiveness of Lavendula stoechas essential oil in treatment of mild to moderate carpal tunnel syndrome: A randomized controlled trial. J. Hand Ther. 2018, 31, 437–442. [Google Scholar] [CrossRef]
- Ordahan, B.; Karahan, A.Y. Efficacy of paraffin wax bath for carpal tunnel syndrome: A randomized comparative study. Int. J. Biometeorol. 2017, 61, 2175–2181. [Google Scholar] [CrossRef]
- Hall, B.; Lee, H.C.; Fitzgerald, H.; Byrne, B.; Barton, A.; Lee, A.H. Investigating the effectiveness of full-time wrist splinting and education in the treatment of carpal tunnel syndrome: A randomized controlled trial. Am. J. Occup. Ther. 2013, 67, 448–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, D.T.; Burke, M.M.; Stewart, G.W.; Cambré, A. Splinting for carpal tunnel syndrome: In search of the optimal angle. Arch. Phys. Med. Rehabil. 1994, 75, 1241–1244. [Google Scholar] [CrossRef]
- American Academy of Orthopaedic Surgeons Boards of Directors. Management of carpal tunnel syndrome. Am. Acad. Orthop. Surg. 2016, 35, 1–983. [Google Scholar]
- Huisstede, B.M.; Hoogvliet, P.; Randsdorp, M.S.; Glerum, S.; van Middelkoop, M.; Koes, B.W. Carpal Tunnel Syndrome. Part I: Effectiveness of Nonsurgical Treatments-A Systematic Review. Arch. Phys. Med. Rehabil. 2010, 91, 981–1004. [Google Scholar] [CrossRef]
- Huisstede, B.M.; Fridén, J.; Coert, J.H.; Hoogvliet, P. Carpal tunnel syndrome: Hand surgeons, hand therapists, and physical medicine and rehabilitation physicians agree on a multidisciplinary treatment guidelined-results from the European HANDGUIDE study. Arch. Phys. Med. Rehabil. 2014, 95, 2253–2263. [Google Scholar] [CrossRef]
- Maniquis-Smigel, L.; Reeves, K.D.; Rosen, H.J.; Lyftogt, J.; Graham-Coleman, C.; Cheng, A.-L.; Rabago, D. Short Term Analgesic Effects of 5% Dextrose Epidural Injections for Chronic Low Back Pain: A Randomized Controlled Trial. Anesthesiol. Pain Med. 2016, 7, e42550. [Google Scholar] [CrossRef] [Green Version]
- Rabago, D.; Slattengren, A.; Zgierska, A. Prolotherapy in Primary Care Practice. Prim. Care Clin. Off. Pract. 2010, 37, 65–80. [Google Scholar] [CrossRef] [Green Version]
- Bueno-Gracia, E.; Ruiz-De-Escudero-Zapico, A.; Malo-Urriés, M.; Shacklock, M.; Estébanez-De-Miguel, E.; Fanlo-Mazas, P.; Caudevilla-Polo, S.; Jiménez-Del-Barrio, S. Dimensional changes of the carpal tunnel and the median nerve during manual mobilization of the carpal bones. Musculoskelet. Sci. Pract. 2018, 36, 12–16. [Google Scholar] [CrossRef]
- da Silva, G.L.; Luft, C.; Lunardelli, A.; Amaral, R.H.; da Silva Melo, D.A.; Donadio, M.V.F. Antioxidant, analgesic and anti-inflammatory effects of lavender essential oil. An. Acad. Bras. Cienc. 2015, 87, 1397–1408. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.D.P. A neurophysiological grading scale for carpal tunnel syndrome. Muscle Nerve 2000, 23, 1280–1283. [Google Scholar] [CrossRef]
- Jablecki, C.K.; Andary, M.T.; Floeter, M.K.; Miller, R.G.; Quartly, C.A.; Vennix, M.J. Practice parameter for electrodiagnostic studies in carpal tunnel syndrome: Summary statement. Muscle Nerve 2002, 25, 918–922. [Google Scholar]
- Schmid, A.B.; Bland, J.D.P.; Bhat, M.A.; Bennett, D.L.H. The relationship of nerve fibre pathology to sensory function in entrapment neuropathy. Brain 2014, 137, 3186–3199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karpitskaya, Y.; Novak, C.B.; MacKinnon, S.E. Prevalence of Smoking, Obesity, Diabetes Mellitus, and Thyroid Disease in Patients with Carpal Tunnel Syndrome. Ann. Plast. Surg. 2002, 48, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Collins, J.; Blazar, P.; Earp, B.E. Factors Associated with Advanced Presentation for Carpal Tunnel Release. J. Hand Surg. 2020, 45, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Westenberg, R.F.; Oflazoglu, K.; De Planque, C.A.; Jupiter, J.B.; Eberlin, K.R.; Chen, N.C. Revision Carpal Tunnel Release: Risk Factors and Rate of Secondary Surgery. Plast. Reconstr. Surg. 2020, 145, 1204–1214. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Database | Search Strategy | Filters |
|---|---|---|
| PubMed | “Carpal Tunnel Syndrome” AND (Therapy OR “Physical Therapy” OR “Manual Therapy” OR “Neural mobilization”) AND Treatment outcome | Text availability: Full text. Article type: Clinical Trial; Randomized Controlled Trial. Publication date: 10 years. Language: English, Spanish, French. |
| Web of Science | “Carpal Tunnel Syndrome” AND (Therapy OR “Physical Therapy” OR “Manual Therapy” OR “Neural mobilization”) AND Treatment outcome | Document type: Article Timespan: 2010 to 2020 |
| SCOPUS | “Carpal Tunnel Syndrome” AND (Therapy OR “Physical Therapy” OR “Manual Therapy” OR “Neural mobilization”) AND Treatment outcome | Document type: Article Years: 2010–2020 Language: English, Spanish, French |
| Cochrane Library | “Carpal Tunnel Syndrome” AND (Therapy OR “Physical Therapy” OR “Manual Therapy” OR “Neural mobilization”) AND Treatment outcome | Years: 2010–2020 Trials Language: English, Spanish, French |
| PEDro | “Carpal Tunnel Syndrome” “Therapy” | Published since: 2010. When searching: Match all search terms (AND). Method: Clinical Trial. |
| Study | Sample | Groups | Outcomes | Follow-ups | Results | |
|---|---|---|---|---|---|---|
| No. (M/F) | CTS Characteristics | |||||
| Çatalbas (2018) | 54 (8/46) | Mild and moderate. Idiopathic | G1: Continuous ultrasound continuo (10 sessions × 10 min) + Night splint (2 wks) G2: Pulsed ultrasound (10 sessions × 10 min) + Night splint (2 wks) G3: Placebo (Ultrasound–10 sessions × 10 min) + Night splint (2 wks) | BCTQ, VAS (pain and paraesthesia), Grip strength, DSL, DML, SNCV, MNCV, CSA | 0, 2, 6 weeks | G1: Improvement in all parameters at 2 and 6 wks [<0167] G2: Improvement in all parameters at 2 and 6 wks [<0167] G3: Improvement in all parameters at 2 and 6 wks [<0167] except for grip strength at 6 wks and DML at 2 wks. |
| Dinarvand (2017) | 37 (0/37) | Mild and moderate. Idiopathic | G1: Unciform and scaphoid bone mobilization (10 min, 3 v/wk × 8 wks) + Night splint (8 wks) G2: Control (Night splint—8 wks) | VAS (pain), BCTQ, DSL, DML, SNAP, motor initiation latency. | 0, 10 weeks | G1: Improvement in BCTQ and VAS [<05]; DSL y DML [<05]. G2: Improvement in BCTQ and VAS [<05]; DSL y DML [<05]. G1 vs. G2: Improvement in BCQT and VAS G1 [01]. |
| Eftekharsadat (2018) | 48 (7/21) | Mild and moderate. Idiopathic | G1: Lavender ointment (2 times/day × 40 days) + Night splint (40 d) G2: Placebo (ointment 2 times/day × 40 + night splint (40 d) | BCTQ, VAS (pain), Pinch and grip strength, CMAP, SNAP | 0, 40 days | G1: Improvement in BCTQ, VAS, pinch and grip strength [05]. G2: Improvement in BCTQ, VAS, pinch and grip strength [05]. G1 vs. G2: Improvement in means in G1, ls pinch strength [05]. |
| Fusakul (2014) | 112 (4/108) | Mild and moderate. Idiopathic | G1: Diode laser (15 sessions × 5 wks, 3 times/wk) + Splint (12 wks morning and night) G2: Placebo (Laser–15 sessions x 5 wks, 3 times/wk) + Splint (12 wks morning and night) | VAS (pain), BCTQ, Pinch and grip strength, Treatment evaluation, DSL. SNAP, DML, CMAP | 0, 5 and 12 weeks | G1: Improvement in VAS, BCTQ and grip strength at 5 and 12 wks [05]; Pinch strength and DML at 12 wks [05]. G2: Improvement in VAS and BCTQ at 5 and 12 wks [05]. Pinch strength and DML at 12 wks [05] G1 vs. G2: Improvement in BCTQ-SSS at 5 wks [031]. |
| Geler-Külcü (2016) | 60 (2/58) | Mild and moderate. Idiopathic | G1: Kinesio-tape (1 time/5 days with 2d rest) + Gliding exercises (4 wks) G2: Placebo (kinesio-tape–1 time/5 days with 2 days of rest) + Gliding exercises (4 wks) G3: Night splint (as often as possible) + Gliding exercises (4 wks) | VAS (pain), DN4 Questionnaire, BCTQ, Grip strength. | 0, 4 weeks | G1: Improvement in VAS, DN4, BCTQ [001]. G2: Improvement in VAS, DN4, BCTQ-SSS [001]. G3: Improvement in VAS, DN4, grip strength, BCTQ-SSS [001]. G1 vs. G3: Significant difference in favour of G1 BCTQ [008]. |
| Günay (2015) | 40 (–/–) | Mild and moderate. Idiopathic | G1: Carpal bone mobilization (10 min/day × 3 times/wk × 10 d) + Splint G2: Control (Splint) | NPRS (Pain), BCTQ, Pinch and grip strength, DSL, DML, SNAP, CMAP, MNCV, MCV, EMG. | 0, 3 months | G1: Improvement in all clinical variables [<022]. DSL y SNAP [05]. G2: Improvement in BCTQ-SSS and NPRS [01]. G1 vs. G2: Greatest improvement in G1 grip strength [04] y BCTQ-FSS [01]. |
| Güner (2018) | 63 hands (4/33) | Mild and moderate. Idiopathic | G1: Low-intensity laser (5 times/wk × 3 wks × 12 min) G2: Low intensity laser (5 times/wk × 3 wks × 12 min) + Kinesio-tape (changed every 2d) G3: Placebo (Laser—5 times/wk × 3 wks × 12 min) | VAS (pain), BCTQ, Pinch and grip strength, DML, DSL, SNCV, MA, SA. | 0, 3, 12 weeks | G1: Improvement in VAS, BCTQ, pinch strength at 3 and 12 wks [05]; Grip strength at 3 wks [014]; MA and SNCV at 12 wks [05]. G2: Improvement in VAS, BCTQ, pinch and grip strength at 3 and 12 wks [05]; MA, DSL and SNCV at12 wks [05]. G3: Improvement in VAS and BCTQ (SSS) 3 wks [05]; DSL and SNCV at 12 wks [05]. G1 vs. G2: Greatest improvement in pinch and grip strength at 12 wks [<03] in G2. G1 vs. G3: Greatest Improvement in VAS and BCTQ at 3 and 12 wks [<01]; Grip strength at 3 wks [028] in G1. G2 vs. G3: All parameters at all times [<03] in G2. |
| Hadianfard (2015) | 50 (3/47) | Mildand moderate. Idiopathic | G1: Acupuncture (2 times/wk × 4 wks) + Night splint G2: Control (Night splint+ Ibuprofen–3 times/day × 10 d) | BCTQ, VAS (pain), DSL, DML, SNCV. | 0, 4 weeks | G1: Improvement in VAS, BCTQ, DSL, DML, SNCV [<001] G2: Improvement in VAS, BCTQ, DSL, DML, SNCV [<001] G1 vs. G2: Improvement in VAS [<001], BCTQ [<001], DSL [<001], SNCV [002] |
| Incebiyik (2015) | 52 hands (0/28) | Mild and moderate. Idiopathic | G1: Short wave diathermy (15 min × 5 times/wk × 3 wks) + Gliding exercises G2: Placebo (diathermy off–15 min × 5 times/wk × 3 wks) + Gliding exercises | VAS (pain), BCTQ, clinical parameters. | 0, 3 weeks | G1: Improvement in all variables [<001] G2: No improvement. G1 vs. G2: Improvement in all variables [<05] in G1. |
| Karimzadeh (2019) | 73 (23/50) | Mild and moderate. Idiopathic | G1: 20 mg Triamcinolone G2: 40 mg Triamcinolone G3: 20 mg Methylprednisolone G4: 40 mg Methylprednisolone | VAS (pain), BCTQ, Grip strength, CMAP, SNAP, MNCV. | 0, 3 months | G1: Improvement in all variables [<026] except CMAP. G2: Improvement in all variables [<034]. G3: Improvement in all variables [<017] except grip strength y CMAP. G4: Improvements in all variables [<01] except CMAP. G1 vs. G2 vs. G3 vs. G4: Significant difference only in amount in BCTQ-FSS [005] at 40 mg. |
| Kumnerddee (2010) | 60 (6/54) | Mild and moderate. Idiopathic | G1: Electro-acupuncture (2 times/wk × 5 wks) G2: Control (Night splint—5 wks) | BCTQ, VAS (pain) | 0, 5 weeks | G1: Improvement in all variables [<05]. G2: Improvement in BCTQ-SSS [008]. G1 vs: G2: Significant improvement in VAS [028] in G1. |
| Ordahan (2017) | 60 (0/60) | Mild and moderate. Idiopathic | G1: Paraffin (5 days/wk × 3 wks) + Splint (always for 3 wks) + Exercises (2 times/day) G2: Control (Splint (always for 3 wks) + Exercises (2 times/day)) | BCTQ, VAS (pain), DML, DSL, SNAP, MNCV, CMAP. | 0, 3 weeks | G1: Improvement in all variables [<03] except CMAP. G2: Improvement in VAS y BCTQ-SSS [<02]. G1 vs. G2: Significant improvement BCTQ-FSS [021]; SNAP [028]; MNCV [041] in G1. |
| Raeissadat (2018) | 41 (0/41) | Mild and moderate. Idiopathic | G1: Leukocyte-poor platelet-rich plasma (1 injection) + Night splint (8 wks) G2: Control (Night splint—8 wks) | BCTQ, VAS (pain), SNAP, CMAP | 0, 10 weeks | G1: Improvement in all variables [<01] except CMAP. G2: Improvement in all variables [<01]. G1 vs. G2: No significant differences. |
| Senna (2019) | 85 (14/71) | Mild and moderate. Idiopathic | G1: Platelet-rich plasma (1 dose) G2: 1ml methylprednisolone acetate (1 dose) | BCTQ, VAS (pain and paraesthesia), Phalen, Tinel, DML, CMAP, SL, SNAP, CSA. | 0, 1 and 3 months | G1: Improvement in all variables [<01] at all follow-ups. G2: Improvement in the variables [<01] at all follow-ups. G1 vs. G2: No significant differences a 1 m. Significant improvement to 3 m in VAS-pain [041]; VAS-paraesthesia [040]; Phalen [041]; Tinel [039], BCTQ-SSS [007]; BCTQ-SSS [002]; DML [002]; SL [037]; SC [049] in G1. |
| Wang (2017) | 52 (41/11) | Mild and moderate. Idiopathic | G1: Triamcinolone + lidocaine (1 ultrasound-guided dose) + Splint (as often as possible for 12 wks) G2: Triamcinolone + lidocaine (1 ultrasound-guided dose) | BCTQ, VAS (pain), DML, SNCV, CMAP, SNAP. | 0, 6, 12 weeks | G1: Improvement in all variables except CMAP [<001] 6 and 12 wks. G2: Improvement in all variables except CMAP [<05] 6 and 12 wks. G1 vs. G2: Significant improvement at 12 wks in BCTQ-SSS [0032], BCTQ-FSS [.019] SNCV [015], SNAP [025] in G1. |
| Wolny (2019) | 103 (11/92) | Mild and moderate. Idiopathic | G1: Neurodynamic techniques (20 min × 2 times/wk × 10 wks) G2: Control | BCTQ, NPRS (pain), Pinch and grip strength, SNCV, MNCV, MT. | 0, 10 weeks | G1 vs. G2: Significant improvement SNCV [<01], MT [<01], NPRS [<01], BCTQ-SSS [<01], BCTQ-FSS [<01] in G1. |
| Wolny (2017) | 140 (18/122) | Mild and moderate. Idiopathic | G1: Neurodynamic techniques + Function massage + Joint mobilization (15 × 2 times/wk × 10 wks). G2: Laser + ultrasound (15 × 2 times/wk × 10 wks). | BCTQ, VAS (pain), SNCV, MNCV, MT, SL | 0, 10 weeks | G1: Improvement in all variables [<01] G2: Improvement in all variables [<05] except SNCV and MNCV. G1 vs. G2: Significant improvement in VAS [<01], BCTQ-SSS [<01], BCTQ-FSS [<01] in G1. |
| Wu (2018) | 54 (11/43) | Mild and moderate. Idiopathic | G1: 5mL Dextrose (1 dose) G2: 3mL Triamcinolone | VAS (pain), BCTQ, CSA, SNCV, DML. | 0, 1, 3, 4, 6 months | G1: Improvement in all variables at all times [<03] except DML at 1 and 6 months. G2: Improvement in VAS, BCTQ-SSS, BCTQ-FSS n 1, 3, 4 m [<01] and VAS 6 m [<001] G1 vs. G2: Significant improvement VAS at 4 m [<01] and 6 m [<001]; BCTQ-SSS at 4 m [<01] and 6 m [<001] and BCTQ-FSS at 4 m and 6 m [<001] in G1. |
| Wu (2017) | 60 (10/50) | Mild and moderate. Idiopathic. | G1: Perineural injection of 5% dextrose (1 dose) G2: Placebo (1 dose of perineural injection with saline) | VAS (pain), BCTQ, CSA, SNCV, DML. | 0, 1, 3, 6 months | G1: Improvement in all variables at all times [<05] except DML. G2: Improvement in VAS, BCTQ-SSS, BCTQ-FSS (not at 1 month) and CSA at all times [<05] G1 vs. G2: Significant improvement in VAS 1m [<01], 3m [<05], 6m [<001]; BCTQ-SSS 1m [<05], 3m [<.05], 6m [<.001]; BCTQ-FSS 1 m [<001], 3 m [<001], 6 m [<001]; SNC 1 m [03], 3 m [001], 6 m [006]; DML 1 m [04], 3 m [03]; CSA 3 m [01], 6 m [004]. |
| Xu (2020) | 55 (9/46) | Mild and moderate. Idiopathic | G1: Radial extracorporeal shock waves (1 time/wk × 3 wks) G2: Betamethasone 1 mL (1 dose) | VAS (pain), BCTQ, SNAPa, SNAPdl, CMAPa, CMAPdl | 0, 3, 9 and 12 weeks | G1: Improvement in VAS, BCTQ, SNAPdl and CMAPdl 12 wks [<05]; VAS, BCTQ and SNAPdl 9 wks [<05]; VAS and BCTQ 3 wks [<05]. G2: Improvement in VAS and BCTQ 3 wks [05]; BCTQ 9 wks [05]. G1 vs. G2: Significant improvement VAS 9 wks [<001], 12 wks [<001]; BCTQ 9 wks [<001], 12 wks [<001]; SNAPdl 12 wks [004] in G1. |
| Yildiz (2011) | 44 (8/36) | Mild and moderate. Idiopathic | G1: Ultrasound + Gel with ketoprofen (15 min × 5 times/wk × 2 wks) + Splint (8 wks) G2: Ultrasound + Gel with drugs (15 min × 5 times/wk × 2 wks) + Splint (8 wks) G3: Placebo (ultrasound off + gel without drugs) (15 min × 5 times/wk × 2 wks) + Splint (8 wks) | VAS (pain), BCTQ | 0, 2 and 8 weeks | G1: Improvement in all variables 2 and 8 wks. G2: Improvement in all variables 2 and 8 wks. G3: Improvement in all variables 2 and 8 wks. G1 vs. G2: Significant improvement in VAS 8 wks [004] in G1. G1 vs. G3: Significant improvement in VAS 8 wks [002] in G1. G2 vs. G3: No significant differences. |
| Study | Sample | Groups | Outcomes | Follow-ups | Results | |
|---|---|---|---|---|---|---|
| No. (M/F) | CTS Characteristics | |||||
| Atthakomol (2018) | 25 (6/19) | Mild, moderate and severe. Idiopathic | G1: Radial extracorporeal shock waves (3–7 min + 15 min cold) G2: Local corticosteroid injections (triamcinolone, lidocaine) | BCTQ, VAS (pain), DSL, DML, SNAP, CMAP | 0, 1, 4, 12 and 24 weeks | G1: Improvement in VAS at 12 and 24 wks [05], BCTQ at 4 [05], 12 and 24 wks [01]; DSL at 12 wks [01]. G2: Improvement in BCTQ at 1 and 4 wks [01]; DSL 12 wks [01]. G1 vs. G2: Improvement in BCQT at 12 a 24 wks [01] G1; DSL at 0 and 12 wks [01] G1. |
| Chen (2015) | 36 (1/35) | Mild, moderate and severe. Idiopathic, hypertension (6) and diabetics (6) | G1: Pulsed radiofrequency (32 min) + Night splint (8 h) G2: Control (Night splint–8h) | VAS (pain), BCTQ, CSA, SNCV, Pinch strength | 0, 1, 4, 8, 12 weeks | G1 vs. G2: All parameters following intervention [<05]. Greatest improvement in VAS and BCTQ at all times, except BCTQ-SSS, in G1. All parameters improved in both. |
| Chung (2016) | 181 (158/23) | Mild, moderate and severe. Idiopathic. | G1: Electro-acupuncture (13 sessions × 20 min) + 8 h Night splint G2: Control (8 h Night splint) | BCTQ, DASH, NPRS (pain), Sensitivity, Manual dexterity, Pinch strength. | 0, 1, 2, 5, 17 weeks | G1 vs. G2: Improvement in BCTQ-FSS and DASH [05] at 1 and 17 wks. Improvement in manual dexterity at 17 wks [<01]. |
| Hamzeh (2020) | 52 hands (4/37) | Mild, moderate and severe. Idiopathic | G1: Neurodynamic technique with exercises to do at home (1 h × 1 time/wk × 4 wks) G2: Exercise programme (1h × 1time/wk × 4 wks supervision, 2 v/d) | BCTQ, Quick DASH, NPRS (pain), RDM, Grip strength. | 0, 1, 6 months | G1: Improvement in BCTQ, NPRS, DASH, RDM, grip strength [<05] G2: Improvement in BCTQ, NPRS, DASH, RDM [<05] G1 vs. G2: Improvement in BCTQ-FSS [.004], DASH [004] in G1. |
| Horng (2011) | 53 (3/50) | Mild, moderate and severe. Idiopathic | G1: Tendon gliding exercises (3 times/day) + Paraffin (2 times/wk) + Night splint (8 wks) G2: Nerve gliding exercises (3 times/day) + Paraffin (2 times/wk) + Night splint (8 wks) G3: Paraffin (2 v/wk) + Night splint (8 wks) | BCTQ, VAS (pain), DASH, WHOQOL (4 domains). | 0, 8 weeks | G1: Improvement in BCTQ, VAS, DASH, WHOQOL (2 domains) [05]. G2: Improvement in BCTQ-SSS, VAS, WHOQOL (1 domain) [05]. G3: Improvement in BCTQ-SSS, VAS, WHOQOL (1 domain) [05]. G1 vs. G2 vs. G3: Significant improvement in BCTQ-FSS in G1 [04] |
| Talebi (2018) | 30 (–/–) | Mild, moderate and severe. Diabetic | G1: Manual therapy–Nerve + interface mobilization + neural (25 min × 3 times/wk × 4 wks) G2: TENS (20 min) + Ultrasound (5 min) (3 times/wk × 4 wks) | VAS (pain), BCTQ, TNDM test. | 0, 4 weeks | G1: Improvement in all variables [<009] G2: Improvement in VAS and BCTQ-SSS [<001] G1 vs. G2: Significant improvement in BCTQ-SSS [006]; BCTQ-FSS [043]; TNDM [<001] in G1 |
| Tezel (2019) | 44 (2/42) | Mild, moderate and severe. Idiopathic | G1: Acupuncture (2 times/wk x 5 wks) + Night splint G2: Control (Night splint) | BCTQ, NHP (6 QoL domains), VAS (pain), DML, MNCV, SCV, DSL, SNCV. | 0, 5 weeks | G1 vs. G2: Significant improvement in VAS [007] and NHP-Pain [001] in G1. |
| Wu (2016) | 40 (5/35) | Mild, moderate and severe. Idiopathic, hypertension (8) and diabetics (4) | G1: Radial extracorporeal shock waves + Splint G2: Placebo (shock waves) + Splint | VAS (pain, paraesthesia), BCTQ, CSA, SNCV, Pinch strength. | 1, 4, 8 and 12 weeks | G1: Improvement in all variables at all times [<01] except SNCV 1 wk. G2: Improvement in all variables at all times [<05] except BCTQ-FSS 8 wks and 12 wks. G1 vs. G2: Significant improvement in VAS at 1 wk [<001], 4 wks [<001], 8 wks [003], 12 wks [006]; BCTQ-SSS at 1 wk [017], 4 wks [005], 8 wks [008]; BCTQ-FSS at 1 wk [001], 4 wks [002], 8 wks [002], 12 wks [007]; CSA at 1 wk [07], 8 wks [041], 12 wks [043] in G1. |
| Group | Study | Treatment | Outcome Pain | Outcome BCTQ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SSS | FSS | |||||||||||
| Pharmacological | Karimzadeh (2019) | G1. 20 mg Triamcinolone G2. 40 mg Triamcinolone G3. 20 mg Methylprednisolone G4. 40 mg Methylprednisolone | VAS G1. Pre (5.4 ± 2.4) vs. Post (4 ± 1.8) p = 0.007 G2. Pre (5.4 ± 2.4) vs. Post (3.7 ± 2.2) p = 0.001 G3. Pre (5.6 ± 1.8) vs. Post (4.1 ± 1.9) p = 0.014 G4. Pre (5.3 ± 2.9) vs. Post (3 ± 2.2) p = 0.006 | Triamcinolone vs. Methylprednisolone 3.84 ± 2.1 vs. 3.53 ± 2.1 (p = 0.53) 20 mg vs. 40 mg 4.05 ± 1.8 vs. 3.36 ± 2.2 (p = 0.14) | G1. Pre (32.5 ± 11.8) vs. Post (24.9 ± 10.2) p = 0.002 G2. Pre (31.7 ± 8.6) vs. Post (22.3 ± 1.1) p = 0.001 G3. Pre (31.9 ± 8) vs. Post (.1 ± 1.9) p = 0.001 G4. Pre (5.3 ± 2.9) vs. Post (3 ± 2.2) p = 0.001 Triamcinolone vs. Methylprednisolone 23.5 ± 10.5 vs. 22.6 ± 7.7 (p = 0.67) 20 mg vs. 40 mg 23.88 ± 9.3 vs. 22.44 ± 9.1 (p = 0.50) | G1. Pre (32.5 ± 11.8) vs. Post (24.9 ± 10.2) p = 0.002 G2. Pre (31.7 ± 8.6) vs. Post (22.3 ± 1.1) p = 0.001 G3. Pre (31.9 ± 8) vs. Post (.1 ± 1.9) p = 0.001 G4. Pre (5.3 ± 2.9) vs. Post (3 ± 2.2) p = 0.002 Triamcinolone vs. Methylprednisolone 14.0 ± 4.9 vs. 15.3 ± 5.3 (p = 0.27) 20 mg vs. 40 mg 16.46 ± 5.7 vs. 13.05 ± 4.4 (p =0.005) | ||||||
| Raeissadat (2018) | G1. Leukocyte-poor platelet-rich plasma + Night splint G2. Night splint | VAS G1. Pre (6.82 ± 1.24) vs. Post (4.02 ± 1.92) p < 0.001 G2. Pre (6.24 ± 1.13) vs. Post (3.52 ± 2.02) p < 0.001 G1 vs. G2–2.90 ± 2.1 vs. -2.76 ± 2.4 (p = 0.845; Power = 0.073; p = 0.098 adjusted for age). | G1. Pre (2.43 ± 0.73) vs. Post (17 ± 0.52) p < 0.001 G2. Pre (2.76 ± 0.40) vs. Post (1.90 ± 0.42) p < 0.001 G1 vs. G2. -0.05 ± 0.2 vs. −0.19 ± 0.4 (p = 0.174; Power = 0.393; p = 0.194 adjusted for age). | G1. Pre (2.54 ± 0.63) vs. Post (1.82 ± 0.42) p < 0.001 G2. Pre (2.36 ± 0.83) vs. Post (1.83 ± 0.73) p < 0.001 G1 vs. G2 −0.86 ± 0.5 vs. −0.63 ± 0.8 (p = 0.289; Power = 0.283; p = 0.554 adjusted for age). | ||||||||
| Senna (2019) | G1. Platelet-rich plasma G2: 1 mL methylprednisolone acetate | VAS G1 (F = 150,217; p < 0.001) Pre: 68.1 ± 6.0 1 month: 24.4 ± 7.3 3 months: 21.8 ± 6.5 | G2 (F = 116,217; p < 0.001) Pre: 69.5 ± 4.9 1 month: 25.9 ± 8.3 3 months: 25.2 ± 7.1 | G1 vs. G2 Pre: t = 1.178; p = 0.242 1 month: t = 0.337; p = 0.737 3 months: t = 2.100; p = 0.040 | G1 (F= 94,739; p < 0.001) Pre: 3.5 ± 0.4 1 month: 2.4 ± 0.6 3 months: 2.0 ± 0.7 | G2 (F = 89,111; p < 0.001) Pre: 3.4 ± 0.4 1 month: 2.5 ± 0.5 3 months: 2.4 ± 0.7 | G1 (F=111,916; p < 0.001) Pre: 3.5 ± 0.4 1 month: 2.5 ± 0.5 3 months: 2.1 ± 0.6 | G2 (F = 71,821; p < 0.001) Pre: 3.4 ± 0.5 1 month: 3.0 ± 0.4 3 months: 2.5 ± 0.6 | ||||
| G1 vs. G2 Pre: t = 1.1082; p = 0.274 1 month: t = 0.268; p = 0.790 3 months: t = 2.752; p = 0.007 | G1 vs. G2 Pre: t = 1.282; p = 0.204 1 month: t = 1.283; p = 0.203 3 months: t = 1.385; p = 0.002 | |||||||||||
| Wang (2017) | G1. Triamcinolone + lidocaine + Splint G2. Triamcinolone + lidocaine | VAS. G1 Pre: 3.61 ± 3.27 6 weeks: 0.80 ± 2.00 12 weeks: 1.00 ± 2.05 | G2 Pre: 2.23 ± 2.59 6 weeks: 0.40 ± 0.84 12 weeks: 0.80 ± 1.57 | G1 vs. G2 6 weeks: 0.40 (–0.45 to 1.25) p = 0.993 12 weeks: 0.19 (−0.82 to 1.21) p = 0.898 | G1 Pre: 2.27 ± 0.71 6 weeks: 1.30 ± 0.53 12 weeks: 1.32 ± 0.43 | G2 Pre: 1.96 ± 0.62 6 weeks: 1.28 ± 0.21 12 weeks: 1.49 ± 0.51 | G1 Pre: 1.93 ± 0.78 6 weeks: 1.33 ± 0.56 12 weeks: 1.27 ± 0.50 | G2 Pre: 1.61 ± 0.62 6 weeks: 1.18 ± 0.28 12 weeks: 1.32 ± 0.35 | ||||
| G1 vs. G2 6 weeks: 0.02 (−0.20 to 0.24) p = 0.216 12 weeks: -0.17 (-0.43 to 0.09) p = 0.246 | G1 vs. G2 6 weeks: 0.14 (−0.10 to 0.40) p = 0.654 12 weeks: -0.04 (-0.29 to 0.19) p = 0.134 | |||||||||||
| Wu (2017) | G1: Perineural injection of 5% dextrose G2: Perineural injection with saline | VAS. G1 Pre: 6.67 ± 0.30 1 month: 4.60 ± 0.35 (p < 0.001) 3 months: 3.57 ± 0.30 (p < 0.001) 6 months: 2.43 ± 0.30 (p < 0.001) | G2 Pre: 6.56 ± 0.30 1 month: 5.64 ± 0.35 (p = 0.002) 3 months: 4.70 ± 0.46 (p < 0.001) 6 months: 4.59 ± 0.46 (p < 0.001) | G1 vs. G2 1 month: −2.07 ± 0.24 vs. −0.93 ± 0.21 (p = 0.001) 3 months: −3.10 ± 0.35 vs. −1.86 ± 0.37 (p = 02) 6 months: −4.23 ± 0.33 vs. −1.98 ± 0.37 (p < 0.001) | G1 Pre: 30.20 ± 1.25 1 month: 20.83 ± 1.06 (p < 0.001) 3 months: 17.60 ± 0.80 (p < 0.001) 6 months: 15.30 ± 0.60 (p < 0.001) | G2 Pre: 28.07 ± 1.93 1 month: 22.37 ± 1.76 (p <.001) 3 months: 20.50 ± 2.02 (p < 0.001) 6 months: 21.60 ± 2.06 (p = 0.002) | G1 Pre: 21.87 ± 0.69 1 month: 14.17 ± 0.72 (p < 0.001) 3 months: 12.90 ± 0.52 (p < 0.001) 6 months: 11.43 ± 0.46 (p < 0.001) | G2 Pre: 19.93 ± 0.96 1 month: 18.00 ± 1.05 (p = 09) 3 months: 16.77 ± 1.18 (p = 0.005) 6 months: 17.07 ± 1.23 (p = 03) | ||||
| G1 vs. G2 1 month: −9.37 ± 1.20 vs. -5.70 ± 0.93 (p = 0.02) 3 months: −12.60 ± 1.19 vs. -7.57 ± 1.54 (p = 0.01) 6 months: -14.90 ± 1.24 vs. −6.47 ± 1.46 (p <0.001) | G1 vs. G2 1 month: −7.70 ± 0.97 vs. −1.93 ± 0.65 (p < 0.001) 3 months: −8.97 ± 0.73 vs. −3.17 ± 0.79 (p < 0.001) 6 months: −10.43 ± 0.83 vs. -2.87 ± 0.86 (p < 0.001) | |||||||||||
| Wu (2018) | G1. 5mL Dextrose G2. 3mL Triamcinolone | VAS. G1 Pre: 6.3 ± 0.3 1 month: 4.2 ± 0.3; −2.1 (−1.4 to −2.8) (p < 0.001) 3 months: 3.3 ± 0.2 −3.1 (−2.2 to −3.9) (p < 0.001) 4 months: 2.8 ± 0.3 −3.6 (−2.6 to −4.5) (p < 0.001) 6 months: 2.0 ± 0.3 −4.3 (−3.2 to −5.4) (p < 0.001) | G2 Pre: 6.2 ± 0.2 1 month: 4.2 ± 0.4 −2.1 (−1.0 to −3.2) (p ≤ 0.001) 3 months: 3.57 ± 0.30 −2.6 (−1.7 to −3.5) (p < 0.001) 4 months: 3.57 ± 0.30 −2.3 (−1.4 to −3.3) (p < 0.001) 6 months: 2.43 ± 0.30 −1.7 (−0.7 to −2.7) (p < 0.001) | G1 vs. G2 1 month: (p > 05) 3 months: (p > 05) 4 months (p < 01) 6 months (p > 001) | G1 Pre: 28.2 ± 1.2 1 month: 19.8 ± 0.9; −8.4 (−4.5 to −12.4) (p < 0.001) 3 months: 16.4 ± 0.7; −3.1 (−2.2 to −3.9) (p < 0.001) 4 months: 15.9 ± 0.6; −12.3 (−8.4 to −16.2) (p < 0.001) 6 months: 14.7 ± 0.6; −13.5 (−9.3 to −17.6) (p < 0.001) | G2 Pre: 27.6 ± 1.4 1 month: 22.5 ± 1.7; −5.0 (−0.6 to −9.4) (p = 016) 3 months: 19.8 ± 1.2; −7.8 (−3.5 to −12.0) (p < 0.001) 4 months: 21.2 ± 1.3; −6.4 (−1.8 to −10.9) (p = 0.002) 6 months: 23.7 ± 1.6; −3.9 (0.6 to −8.3) (p = 128) | G1 Pre: 20.7 ± 1.1 1 month: 15.0 ± 0.8; −5.7 (−2.6 to −8.9) (p < 0.001) 3 months: 3.3 ± 0.2; −3.1 (−2.2 to −3.9) (p < 0.001) 4 months: 2.8 ± 0.3; −3.6 (−2.6 to −4.5) (p < 0.001) 6 months: 2.0 ± 0.3; −4.3 (−3.2 to −5.4) (p < 0.001) | G2 Pre: 19.7 ± 0.8 1 month: 16.1 ± 1.0; −3.6 (−0.7 to −6.5) (p < 0.001) 3 months: 15.0 ± 0.8; −4.7 (−2.1 to −7.2) (p < 0.001) 4 months: 15.9 ± 0.8; −3.7 (−1.1 to −6.4) (p < 0.001) 6 months: 16.6 ± 0.8; −3.0 (1.0 to −6.2) (p = 063) | ||||
| G1 vs. G2 1 month: (p > 05) 3 months: (p > 05) 4 months: (p < 01) 6 months: (p < 0.001) | G1 vs. G2 1 month: (p > 05) 3 months: (p > 05) 4 months: (p < 0.001) 6 months: (p < 0.001) | |||||||||||
| Electrotherapy | Çatalbas (2018) | G1. Continuous ultrasound + Night splint G2. Pulsed ultrasound + Night splint G3. Placebo Ultrasound + Night splint | VAS. G1 Pre: 5.5 ± 3.2 2 weeks: 2.8 ± 1.9 (p < 0167) 6 weeks: 2.0 ± 2.2 (p < 0167) vs. pre and post. | G2 Pre: 5.4 ± 2.5 2 weeks: 2.9 ± 2.4 (p < 0167) 6 weeks: 2.1 ± 2.3 (p < 0167) vs. pre. | G3 Pre: 5.0 ± 2.5 2 weeks: 2.6 ± 2.1 (p < 0167) 6 weeks: 2.2 ± 2.0 (p < 0167) vs. pre. | G1 Pre: 2.8 ± 0.8 2 weeks: 1.9 ± 0.7 (p < 0167) 6 weeks: 1.9 ± 0.7 (p < 0167) vs. pre. | G2 Pre: 3.1 ± 0.8 2 weeks: 2.1 ± 0.7 (p < 0167) 6 weeks: 2.1 ± 0.9 (p < 0167) vs. pre. | G3 Pre: 2.8 ± 0.9 2 weeks: 2.2 ± 0.8 (p < 0167) 6 weeks: 2.2 ± 0.7 (p < 0167) vs. pre. | G1 Pre: 2.5 ± 0.9 2 weeks: 1.8 ± 0.7 (p < 0167) 6 weeks: 2.4 ± 0.8 (p < 0167) vs. pre. | G2 Pre: 2.4 ± 0.9 2 weeks: 1.9 ± 0.8 (p < 0167) 6 weeks: 1.9 ± 0.8 (p < 0167) vs. pre. | G3 Pre: 2.4 ± 0.8 2 weeks: 1.9 ± 0.6 (p < 0167) 6 weeks: 1.9 ± 0.7 (p < 0167) vs. pre. | |
| Pre: p = 0.730 2 weeks: p = 0.860 6 weeks: p = 0.850 | Pre: p = 0.380; 2 weeks: p = 0.600; 6 weeks: p = 0.430 | Pre: p = 0.910; 2 weeks: p = 0.580; 6 weeks: p = 0.260 | ||||||||||
| Chen (2015) | G1. Pulsed radiofrequency + Night splint G2. Night splint | VAS. G1 Pre: 5.4 ± 2.1 1 week: 2.5 ± 1.4 −2.9 ± 1.1 (2.4–3.4). 4 weeks: 2.2 ± 1.5 −3.2 ± 1.1 (2.6–3.7). 8 week: 1.8 ± 1.2 −3.6 ± 1.6 (2.8–4.4). 12 weeks: 1.1 ± 0.8 −4.2 ± 2.1 (3.2–5.2). | G2 Pre: 5.0 ± 1.5 1 week: 3.9 ± 1.1 −1.1 ± 1.2 (0.5–1.7). 4 weeks: 3.4 ± 1. −1.6 ± 1.4 (0.9–2.2) 8 week: 3.2 ± 1.1 −1.8 ± 1.5 (1.0–2.5) 12 weeks: -2.0 ± 1.8 (1.1–2.9) | G1 vs. G2 Pre: (p = 552) 1 week: (p = 0.002) 4 weeks: (p = 013) 8 week: (p < 0.001) 12 weeks: (p < 0.001) | G1 Pre: 33.4 ± 6.4 1 week: 21.7 ± 7.3 −11.7 ± 4.7 (9.4–14.1). 4 weeks: 19.6 ± 4.8 −13.9 ± 5.1 (11.3–16.4). 8 week: 17.1 ± 3.6 −16.3 ± 6.3 (13.2–19.4). 12 weeks: 13.7 ± 2.1 −19.7 ± 6.7 (16.4–23.0). | G2 Pre: 33.0 ± 6.5 1 week: 26.0 ± 6.7 −7.0 ± 6.6 (3.7–10.3) 4 weeks: 23.6 ± 6.2 −9.4 ± 7.7 (5.6–13.3) 8 week: 22.8 ± 6.7 −10.2 ± 8.7 (5.9–14.5) 12 weeks: 22.1 ± 6.3 −10.9 ± 9.2 (6.3–15.5) | G1 Pre: 23.3 ± 3.4 1 week: 12.1 ± 3.9 −11.2 ± 4.6 (8.9–13.4) 4 weeks: 11.2 ± 3.8 −12.1 ± 4.3(10–14.3) 8 week: 10.7 ± 3.7 −12.6 ± 5(10.1–15.1). 12 weeks: 9.1 ± 2.2 −14.2 ± 4.1(12.2–16.3). | G2 Pre: 23.2 ± 6.2 1 week: 16.3 ± 6.9 −6.9 ± 6.3 (3.8–10) 4 weeks: 14.6 ± 4.9 −8.6 ± 6.8 (5.2–11.9) 8 week: 14.4 ± 5.0 −8.8 ± 7.0 (5.3–12.2) 12 weeks: 13.9 ± 5.0 −9.3 ± 7.4 (5.6–13.0) | ||||
| G1 vs. G2 Pre: (p = 837) 1 week: (p = 077) 4 weeks: (p = 037) 8 week: (p = 0.004) 12 weeks: (p < 0.001) | G1 vs. G2 Pre: (p = 948) 1 week: (p = 032) 4 weeks: (p = 025) 8 week: (p = 016) 12 weeks: (p = 0.001) | |||||||||||
| Chung (2016) | G1. Electro-acupuncture + Night splint G2. Night splint | NPRS. G1 Pre: 4.38 ± 2.62 1 week: 18 (20.0) –0.22 (–0.68 to 0.23) 2 weeks: 21 (23.3) –0.30 (–0.81 to 0.21) 5 week: 27 (31.0) –0.68 (–1.18 to –0.19) 17 weeks: 34 (40.0) –1.22 (–1.79 to –0.65) | G2 Pre: 4.52 ± 2.78 1 week: 20 (22.0) –0.43 (–0.89 to 0.04) 2 weeks: 24 (26.4) –0.50 (–1.01 to 0.01) 5 week: 28 (31.1) −0.55 (–1.11 to 0.02) 17 weeks: 31 (34.8) –0.61 (–1.22 to 0.00) | G1 vs. G2 1 week: (p = 6) 4 weeks: (p = 7) 8 week: (p = 6) 12 weeks: (p = 03) | G1 Pre: 2.32 ± 0.62 1 week: 11 (12.2) 0.04 (–0.03 to 0.12) 2 weeks: 19 (21.1) –0.01 (–0.09 to 0.07) 5 week: 33 (37.9) 0.17 (–0.28 to –0.06) 17 weeks: 40 (47.1) –0.25 (–0.37 to –0.12) | G2 Pre: 2.40 ± 0.69 1 week: 19 (20.9) 0.01 (–0.08 to 0.10) 2 weeks: 23 (25.3) –0.02 (–0.13 to 0.08) 5 week: 27 (30.0) –0.06 (–0.19 to 0.07) 17 weeks: 32 (36.0) –0.09 (–0.25 to 0.06) | G1 Pre: 4.38 ± 2.62 1 week: 7 (7.8) 0.14 (0.05 to 0.23) 2 weeks: 15 (16.7) 0.11 (0.00 to 0.22) 5 week: 19 (21.8) –0.01 (–0.12 to 0.11) 17 weeks: 30 (35.3) –0.16 (–0.28 to –0.04) | G2 Pre: 4.52 ± 2.78 1 week: 17 (18.7) 0.09 (0.00 to 0.18) 2 weeks: 15 (16.5) 0.07 (–0.04 to 0.17) 5 week: 18 (20.0) 0.06 (–0.07 to 0.18) 17 weeks: 21 (23.6) 0.02 (–0.13 to 0.17) | ||||
| G1 vs. G2 1 week: 0.02 (–0.09 to 0.13) (p = 8) 4 weeks: –0.01 (–0.13 to 0.11) (p = 9) 8 week:–0.15 (–0.29 to –0.01) (p = 0.04) 12 weeks: –0.20 (–0.36 to –0.03) (p = 02) | G1 vs. G2 1 week: 0.05 (–0.08 to 0.17) (p = 03) 4 weeks: 0.03 (–0.12 to 0.17) (p = 1.0) 8 week: –0.09 (–0.24 to 0.06) (p = 8) 12 weeks: –0.22 (–0.38 to –0.05) (p = 09) | |||||||||||
| Fusakul (2014) | G1. Diode laser + Splint G2. Laser Placebo + Splint | VAS. G1 Pre: 6.26 ± 0.27 (p < 0.05) 5 weeks: 4.25 ± 0.34 (p < 0.05) 12 weeks: 3.45 ± 0.38 (p < 0.05) | G2 Pre: 4.83 ± 0.33 (p < 0.05) 5 weeks: 3.15 ± 0.30 (p < 0.05) 12 weeks: 2.48 ± 0.36 (p < 0.05) | G1 vs. G2 Pre: p = 0.174 5 weeks: p = 0.243 12 weeks: p = 0.433 | G1 Pre: 2.10 ± 0.68 (p < 0.05) 5 weeks: 1.68 ± 0.66 (p < 0.05) 12 weeks: 1.49 ± 0.58 (p < 0.05) | G2 Pre: 1.68 ± 0.56 (p < 0.05) 5 weeks: 1.43 ± 0.49 (p < 0.05) 12 weeks: 1.35 ± 0.51 (p < 0.05) | G1 Pre: 2.07 ± 0.67 (p < 0.05) 5 weeks: 1.75 ± 0.62 (p < 0.05) 12 weeks: 1.53 ± 0.57 (p < 0.05) | G2 Pre: 1.77 ± 0.62 (p < 0.05) 5 weeks: 1.54 ± 0.62 (p < 0.05) 12 weeks: 1.37 ± 0.49 (p < 0.05) | ||||
| G1 vs. G2 Pre: p = 0.291 5 weeks: p = 0.031 12 weeks p = 0.886 | G1 vs. G2 Pre: p = 0.712 5 weeks: p = 0.406 12 weeks: p = 0.313 | |||||||||||
| Güner (2018) | G1. Low-intensity laser G2. Low intensity laser + Kinesio-tape G3. Laser Placebo | VAS daytime G1 Post: 6 (3–9) 3 weeks: 1 (0–5) p < 0.001 12 weeks:1 (0–5) p < 0.001 | G2 Post: 6 (4–10) 3 weeks: 1 (0–8) p < 0.001 12 weeks:2 (0–6) p < 0.001 | G3 Post: 6 (2–10) 3 weeks: 5 (1–9) p < 0.001 12 weeks:5 (0–9) p = 085 | G1 vs. G2 0–3 w: p = 879 0–12w: p = 879 G1 vs. G3 0–3 w: p = 0.001 0-12w: p < 0.001 G2 vs. G3 0-3w: p = 0.003 0-12w: p < 0.001 | G1 Post: 3.09 (2.09–4) 3 weeks: 1.36 (1.00–3.27) p < 0.001 12 weeks: 1.90 (1.00–3.00) p < 0.001 | G2 Post: 3.24 (2.63–4.27) 3 weeks: 1.54 (1–2.81) p < 0.001 12 weeks: 1.90 (1–2.90) p < 0.001 | G3 Post: 3.27 (2.09–4.18) 3 weeks: 2.63 (1.54–3.54) p = 0.001 12 weeks: 3.00 (1.36–3.81) p = 054 | G1 Post: 2.63 (1.25–3.75) 3 weeks: 1.63 (1.00–3.25) p < 0.001 12 weeks: 1.63 (1.00–3.25) p < 0.001 | G2 Post: 2.88 (1.38–3.88) 3 weeks: 1.63 (1.25–2.75) p < 0.001 12 weeks: 1.88 (1–3) p < 0.001 | G3 Post: 3.12 (1.13–5.75) 3 weeks: 3 (1–5.75) p = 632 12 weeks: 2.5 (1–4.13) p = 626 | |
| VAS night G1 Post: 8 (4–10) 3 weeks: 2 (0–8) p < 0.001 12 weeks:0 (0–8) p < 0.001 | G2 Post: 8 (3–10) 3 weeks: 0 (0–8) p < 0.001 12 weeks:0 (0–6) p < 0.001 | G3 Post: 7 (5–10) 3 weeks:5 (1–10) p = 0.001 12 weeks: 7 (0–10) p = 273 | G1 vs. G2 0–3w: p = 245 0–12w: p = 577 G1 vs. G3 0–3w: p = 0.004 0–12w: p < 0.001 G2 vs. G3 0–3w: p = 0.001 0–12w: p < 0.001 | G1 vs. G2 0–3w: p = 840 0–12w: p = 659 | G1 vs. G3 0–3w: p = 0.002 0–12w: p = 0.006 | G2 vs. G3 0–3w: p = 020 0–12w: p < 0.001 | G1 vs. G2 0–3w: p = 772 0–12w: p = 970 | G1 vs. G3 0–3w: p = 0.001 0–12w: p = 0.006 | G2 vs. G3 0–3w: p = 0.002 0–12w: p = 0.007 | |||
| Kumnerddee (2010) | G1. Electro-acupuncture G2. Night splint | VAS. G1 Post vs. Post: 22.57 ± 22.27 vs. 7.97 + 14.99 | G2 Post vs. Post: 22.57 ± 22.27 vs. 17.60 + 22.37 | G1 vs. G2 9.63 (1.07 to 18.20) p = 0.028 | G1 Post vs. Post: 2.03 ± 0.61 vs. 1.98 ± 0.56 | G2 Post vs. Post: 0.39 vs. 1.66 ± 0.50 | G1 Post vs. Post: 1.76 ± 0.63 vs. 1.50 ± 0.39 | G2 Post vs. Post: 1.70 ± 0.57 vs. 1.54 ± 0.48 | ||||
| G1 vs. G2 0.11 (−0.10 to 0.33). p = 0.295 | G1 vs. G2 0.05 (−0.16 to 0.25). p = 0.663 | |||||||||||
| Wu (2016) | G1. Radial extracorporeal shock waves + Splint G2. Placebo shock waves + Splint | VAS. G1 Pre: 6.26 ± 0.27 1 week: 3.15 ± 0.98 p < 0.01) 4 weeks: 2.48 ± 1.00 (p < 0.01) 8 weeks: 2.77 ± 1.37 (p < 0.01) 12 weeks: 2.70 ± 1.23 (p < 0.01) | G2 Pre: 5.90 ± 1.22 1 week: 4.47 ± 1.05 (p < 0.05) 4 weeks: 4.12 ± 1.14 (p < 0.05) 8 weeks: 3.80 ± 1.35 (p < 0.05) 12 weeks: 3.59 ± 1.27 (p < 0.05) | G1 vs. G2 1 week: p < 0.001 4 weeks: p < 0.001 8 weeks: p = 0.003 12 weeks: p = 0.006 | G1 Pre: 32.65 ± 7.86 1 week: 20.20 ± 5.0 (p < 0.001) 4 weeks: 18.90 ± 4.76 (p < 0.001) 8 weeks: 17.50 ± 4.11 (p < 0.001) 12 weeks: 18.45 ± 4.76 (p < 0.001) | G2 Pre: 29.95 ± 8.46 1 week: 23.75 ± 6.76 (p = 0.005) 4 weeks: 23.45 ± 7.01 (p = 0.009) 8 weeks: 22.00 ± 6.32 (p = 0.002) 12 weeks: 19.80 ± 5.04 (p = 0.002) | G1 Pre: 17.70 ± 4.21 1 week: 11.75 ± 2.51(p < 0.001) 4 weeks: 10.90 ± 2.81 (p < 0.001) 8 weeks: 10.70 ± 2.52 (p < 0.001) 12 weeks: 10.60 ± 2.28 (p < 0.001) | G2 Pre: 16.65 ± 5.03 1 week: 14.30 ± 4.46 (p = 0.021) 4 weeks: 13.70 ± 4.84 (p < 0.019) 8 weeks: 13.95 ± 5.48 (p = 0.109) 12 weeks: 13.50 ± 5.77 (p = 0.107) | ||||
| G1 vs. G2 1 week: p = 0.017 4 weeks: p = 0.005 8 weeks: p = 0.008 12 weeks: p = 0.171 | G1 vs. G2 1 week: p= 0.001 4 weeks: p= 0.002 8 weeks: p= 0.002 12 weeks: p = 0.007 | |||||||||||
| Manual Therapy | Dinarvand (2017) | G1. Unciform and scaphoid bone mobilization + Night splint G2. Night splint | VAS. G1 Post vs. Post: p < 0.001 5.44 ± 2.35 vs. 1.94 ± 1.34 | G2 Post vs. Post: p < 0.001 6.36 ± 1.16 vs. 3.52 ± 2.06 | G1 Post vs. Post: p < 0.001 2.58 ± 0.57 vs. 1.46 ± 0.37 | G2 Post vs. Post: p < 0.001 6.36 ± 1.16 vs. 3.52 ± 2.06 | G1 Post vs. Post: p < 0.001 2.52 ± 0.4 vs. 1.8 ± 0.44 | G2 Post vs. Post: p < 0.001 2.61 ± 0.57 vs. 1.76 ± 0.45 | ||||
| Geler-Külcu (2016) | G1. Kinesio-tape + Gliding exercises G2. Placebo kinesio-tape + Gliding exercises G3. Night splint + Gliding exercises | VAS. G1 Post vs. Post: p = 0.005 6.6 ± 2.1 vs. 4.1 ± 2.7 | G2 Post vs. Post: p = 0.003 5.8 ± 3.2 vs. 3.9 ± 2.8 | G3 Post vs. Post: p = 0.024 6.1 ± 2.9 vs. 5.7 ± 3.1 | G1 vs. G2 vs. G3 p = 0.269 | G1 Post vs. Post: p < 0.0001 32 ± 8.4 vs. 20 ± 7.5 | G2 Post vs. Post: p < 0.0001 33 ± 10.7 vs. 24.4 ± 8.0 | G3 Post vs. Post: p < 0.036 31.6 ± 8.4 vs. 28.7 ± 11.8 | G1 Post vs. Post: p = 0.001 23.1 ± 6.0 vs. 16.2 ± 5.4 | G2 Post vs. Post: p = 0.077 19.7 ± 8.4 vs. 16.3 ± 5.8 | G3 Post vs. Post: p = 0.090 19.7 ± 7.0 vs. 19.7 ± 19.7 | |
| G1 vs. G2 vs. G3 p = 0.024 | G1 vs. G2 vs. G3 p = 0.017 | |||||||||||
| Günay (2015) | G1. Carpal bone mobilization + Splint G2. Splint | VAS daytime G1 Pre vs. Post: p = 0.003 3 (0–8) vs. 0 (0–8) | G2 Pre vs. Post: p = 0.011 5 (0–7) vs. 1 (0–7) | G1 vs. G2 −2 (−7;2) vs. -3 (−7;4): p = 0.53 | G1 Pre vs. Post: p < 0.001 29 (20–46) vs. 17 (12–44) | G2 Pre vs. Post: p = 0.001 31.5 (18–46) vs. 23 (11–43) | G1 Pre vs. Post: p = 0.001 21 (14–33) vs. 16.5 (8–32) | G2 Pre vs. Post: p = 0.57 19 (9–35) vs. 19 (8–29) | ||||
| VAS night G1 Pre vs. Post: p < 0.001 6 (1–8) vs. 0 (0–8) | G2 Pre vs. Post: p = 0.001 5 (0–9) vs. 0 (0–8) | G1 vs. G2 −5 (−8;2) vs. -4 (−8;2): p = 0.14 | G1 vs. G2 −12.5 (−26;5) vs. −8.0 (−23;5): p = 0.39 | G1 vs. G2 -5.5 (−18;2) vs. 0 (−11;5): p = 0.01 | ||||||||
| Hadianfard (2015) | G1. Acupuncture + Night splint G2. Night splint + Ibuprofen | VAS. G1 Post vs. Post: p < 0.001 7.32 ± 0.94 vs. 3.8 ± 0.78 | G2 Post vs. Post: p < 0.001 7.32 ± 1.06 vs. 4.64 ± 0.7 | G1 vs. G2 p = 0.001 | G1 Post vs. Post: p < 0.001 6.6 ± 2.1 vs. 4.1 ± 2.7 | G2 Post vs. Post: p < 0.001 6.6 ± 2.1 vs. 4.1 ± 2.7 | G1 Post vs. Post: p < 0.001 17.708 ± 2.561 vs. 11.00 ± 0.780 | G2 Post vs. Post: p < 0.001 18.00 ± 3.00 vs. 12.840 ± 1.929 | ||||
| G1 vs. G2 p < 0.001 | G1 vs. G2 p < 0.001 | |||||||||||
| Hamzeh (2020) | G1. Neurodynamic technique with home exercises G2. Exercise programme | NPRS mean G1 Pre: 4.17 ± 2.23 1 month: 1.22 ± 1.59 p < 05 6 months: 1.06 ± 1.75 p < 05 | G2 Pre: 3.17 ± 2.49 1 month: 2.97 ± 2.44 p > 05 6 months: 2.09 ± 2.43 p > 05 | G1 vs. G2 Pre: 1.00 (−0.3 to 2.3) p = 14 1 month: −1.75 (-2.9 to −0.6) p = 0.005 6 months: −1.03 (−2.5 to 0.4) p = 14 | G1 Pre: 3.17 ± 0.86 1 month: 2.04 ± 0.68 p < 05 6 months: 1.64 ± 0.66 p < 05 | G2 Pre: 2.71 ± 0.76 1 month: 2.16 ± 0.74 p < 05 6 months: 1.88 ± 0.60 p < 05 | G1 Pre: 2.80 ± 0.87 1 month: 2.08 ± 0.82 p < 05 6 months: 1.35 ± 0.48 p < 05 | G2 Pre: 2.63 ± 0.84 1 month: 2.17 ± 0.97 p < 05 6 months: 1.84 ± 0.87 p < 05 | ||||
| NPRS worst G1 Pre: 7.52 ± 2.57 1 month: 3.17 ± 2.59 p < 05 6 months: 2.88 ± 3.39 p < 05 | G2 Pre: 7.07 ± 2.19 1 month: 5.10 ± 2.81 p < 05 6 months: 4.82 ± 2.81 p < 05 | G1 vs. G2 Pre: 0.45 (−0.9 to 1.8) p = 50 1 month: −1.93 (−3.5 to −0.4) p = 014 6 months: −1.94 (−4.0 to 0.1) p = 06 | G1 vs. G2 Pre: 0.46 (0.01 to 0.9) p = 0.05 1 month: −0.13 (-0.5 to 0.3) p = 0.53 6 months: −0.24 (-0.7 to 0.2) p = 0.24 | G1 vs. G2 Pre: 0.17 (−0.3 to 0.7) p = 48 1 month: −0.09 (−0.6 to 0.4) p = 73 6 months: −0.49 (−1.0 to −0.01) p = 04 | ||||||||
| Horng (2011) | G1. Tendon gliding exercises + Paraffin + Night splint G2. Nerve gliding exercises + Paraffin + Night splint G3. Paraffin + Night splint | VAS G1 Pre vs. Post: p < 05 −19.7 ± 24.6 | G2 Pre vs. Post: p < 05 −10.5 ± 18.0 | G3 Pre vs. Post: p < 05 −17.2 ± 26.2 | G1 vs. G2 vs. G3 p = 44 | G1 Pre vs. Post: p < 05 −0.7 ± 0.8 | G2 Pre vs. Post: p < 05 −0.3 ± 0.6 | G3 Pre vs. Post: p < 05 −0.6 ± 0.6 | G1 Pre vs. Post: p < 05 −0.4 ± 0.5 | G2 Pre vs. Post: p > 05 0.1 ± 0.5 | G3 Pre vs. Post: p > 05 −0.2 ± 0.7 | |
| G1 vs. G2 vs. G3 p = 56 | G1 vs. G2 vs. G3 p = 04 | |||||||||||
| Ordahan (2017) | G1. Paraffin + Splint + Exercises G2. Splint + Exercises | VAS G1 Pre vs. Post: p = 0.009 7.31 ± 1.41 vs. 3.73 ± 1.19 | G2 Pre vs. Post: p = 0.013 6.95 ± 1.60 vs. 3.80 ± 1.67 | G1 vs. G2 p = 423 | G1 Pre vs. Post: p = 011 3.07 ± 0.63 vs. 2.52 ± 0.59 | G2 Pre vs. Post: p = 018 2.83 ± 0.68 vs. 2.52 ± 0.71 | G1 Pre vs. Post: p = 027 2.83 ± 0.90 vs. 2.32 ± 0.89 | G2 Pre vs. Post: p = 214 2.41 ± 0.83 vs. 2.42 ± 1.05 | ||||
| G1 vs. G2 p = 0.551 | G1 vs. G2 p = 0.021 | |||||||||||
| Tezel (2019) | G1. Acupuncture + Night splint G2. Night splint | VAS G1 Pre vs. Post: 7.4 ± 0.8 vs. 4.8 ± 0.8 | G2 Pre vs. Post: 7.6 ± 0.7 vs. 5.8 ± 0.8 | G1 vs. G2 p = 0.007 | G1 Pre vs. Post: 29.8 ± 5.9 vs. 23.4 ± 7.5 | G2 Pre vs. Post: 28.8 ± 5.4 vs. 22.1 ± 6.5 | G1 Pre vs. Post: 26.8 ± 9.0 vs. 20.7 ± 6.9 | G2 Pre vs. Post: 25.8 ± 8.7 vs. 19.4 ± 6.4 | ||||
| G1 vs. G2 p = 0.54 | G1 vs. G2 p = 0.51 | |||||||||||
| Combined | Atthakomol (2018) | G1. Radial extracorporeal shock waves G2. Local corticosteroid injections | VAS G1 Pre: 2.4 ± 2.5 1 week: 1.3 ± 2.0 (p < 0.18) 4 weeks: 1.3 ± 1.9 (p < 0.15) 12 weeks: 0.65 ± 1.2 (p < 0.022) 24 weeks: 0.35 ± 0.81 (p < 0.0075) | G2 Pre: 2.6 ± 2.0 1 week: 1.6 ± 1.7 (p < 0.08) 4 weeks: 1.3 ± 1.5 (p < 0.08) 12 weeks: 1.9 ± 2.7 (p < 0.52) 24 weeks: 1.7 ± 2.1 (p < 0.19) | G1 vs. G2 Pre vs. 1w: −10 (−1.7 to 1.5) p = 90 1w vs. 4w: 0.049 (−1.6 to 1.7) p = 95 4w vs. 12w: −1.0 (−2.7 to 0.63) p = 23 12w vs. 24w: −1.2 (−2.9 to 0.49) p = 17 | G1 Pre: 21 ± 6.4 1 week: 19 ± 7.4(p = 33) 4 weeks: 17 ± 4.3 p = 031) 12 weeks: 15 ± 4.5 (p = 0.0082) 24 weeks: 13 ± 2.9 (p = 0.0059) | G2 Pre: 22 ± 5.1 1 week: 17 ± 4.5 (p = 0.0047) 4 weeks: 17 ± 5.1 (p = 011) 12 weeks: 18 ± 5.5 (p = 13) 24 weeks: 19 ± 7.9 (p = 20) | G1 Pre: 14 ± 3.2 1 week: 13 ± 4.2 (p = 27) 4 weeks: 13 ± 3.5 (p = 12) 12 weeks: 11 ± 3.0 (p = 0.0065) 24 weeks: 11 ± 2.2 (p = 0.0073) | G2 Pre: 12 ± 4.1 1 week: 11 ± 3.2 (p = 31) 4 weeks: 11 ± 3.3 (p = 39) 12 weeks: 10 ± 3.4 (p = 19) 24 weeks: 13 ± 7.0 (p = 65) | |||
| G1 vs. G2 Pre vs. 1w: 2.6 (−2.0 to 7.2) p = 27 1w vs. 4w: 1.5 (−3.2 to 6.1) p = 53 4w vs. 12w: −1.9 (−2.7 to 2.8) p = 43 12w vs. 24w: −5.1 (−9.8 to −33) p = 036 | G1 vs. G2 Pre vs. 1w: 0.43 (−3.1 to 3.9) p = 81 1w vs. 4w: −20 (−3.7 to 3.3) p = 91 4w vs. 12w: −1.8 (−5.3 to 1.7) p = 32 12w vs. 24w: −4.5 (−8.1 to −87) p = 015 | |||||||||||
| Incebiyik (2015) | G1. Short wave diathermy + Gliding exercises G2. Placebo + Gliding exercises | VAS G1 Pre vs. Post: p < 0.001 5.50 ± 2.53 vs. 2.32 ± 1.80 | G2 Pre vs. Post: p = 1.105 4.83 ± 2.76 vs. 4.20 ± 2.53 | G1 vs. G2 p = 0.003 | G1 Pre vs. Post: p < 0.001 30.78 ± 7.92 vs. 18.53 ± 9.09 | G2 Pre vs. Post: p = 204 29.25 ± 11.41 vs. 27.62 ± 10.63 | G1 Pre vs. Post: p < 0.001 29.8 ± 5.9 vs. 23.4 ± 7.5 | G2 Pre vs. Post: p = 234 28.8 ± 5.4 vs. 22.1 ± 6.5 | ||||
| G1 vs. G2 p = 0.002 | G1 vs. G2 p < 0.001 | |||||||||||
| Talebi (2018) | G1: Manual therapy–Nerve + interface mobilization + neural G2: TENS + Ultrasound | VAS G1 Pre vs. Post: p = 0.000 7.08 ± 1.56 vs. 3.75 ± 2.22 | G2 Pre vs. Post: p = 0.000 6.58 ± 1.37 vs. 4.4 1 ± 1.31 | G1 vs. G2 p = 141 | G1 Pre vs. Post: p = 0.000 29.91 ± 9.65 vs. 19.25 ± 6.25 | G2 Pre vs. Post: p = 0.000 29.91 ± 7.24 vs. 25.41 ± 6.25 | G1 Pre vs. Post: p = 241 4.83 ± 2.76 vs. 4.20 ± 2.53 | G2 Pre vs. Post: p = 0.008 4.83 ± 2.76 vs. 4.20 ± 2.53 | ||||
| G1 vs. G2 p = 0.006 | G1 vs. G2 p = 043 | |||||||||||
| Wolny (2017) | G1: Neurodynamic techniques + Function massage + Joint mobilization G2: Laser + ultrasound | NPRS G1 Pre vs. Post: p < 01 5.72 ± 1.49 vs. 1.47 ± 1.20 | G2 Pre vs. Post: p < 01 5.25 ± 1.75 vs. 3.58 ± 1.93 | G1 vs. G2 p < 01 | G1 Pre vs. Post: 2.97 ± 0.63 vs. 1.78 ± 0.47 | G2 Pre vs. Post: 2.94 ± 0.74 vs. 2.57 ± 0.77 | G1 Pre vs. Post: 2.80 ± 0.94 vs. 1.90 ± 0.62 | G2 Pre vs. Post: 2.77 ± 0.94 vs. 2.55 ± 0.95 | ||||
| G1 vs. G2 p < 0.001 | G1 vs. G2 p < 0.001 | |||||||||||
| Wolny (2019) | G1: Neurodynamic techniques G2: No treatment | NPRS G1 Pre vs. Post: 5.86 ± 1.46 vs. 1.38 ± 0.72 | G2 Pre vs. Post: 5.71 ± 1.34 vs. 5.46 ± 1.05 | G1 vs. G2 p < 0.001 | G1 Pre vs. Post: 3.03 ± 0.65 vs. 1.08 ± 0.68 | G2 Pre vs. Post: 2.92 ± 0.71 vs. 2.87 ± 0.68 | G1 Pre vs. Post: 2.82 ± 0.71 vs. 1.96 ± 0.64 | G2 Pre vs. Post: 2.99 ± 0.67 vs. 2.87 ± 0.71 | ||||
| G1 vs. G2 p < 0.001 | G1 vs. G2 p < 0.001 | |||||||||||
| Xu (2020) | G1: Radial extracorporeal shock waves G2: Betamethasone 1mL | VAS G1 Pre: 2.5 ± 0.3 3 week: 1.4 ± 0.9(p = 0.04) 9 weeks:8 ± 1.1 (p = 0.02) 12 weeks: 0.6 ± 0.7 (p = 0.00) | G2 Pre: 2.6 ± 0.4 3 week: 1.5 ± 1.1(p = 0.04) 9 weeks: 1.7 ± 0.7 (p = 0.21) 12 weeks: 1.9 ± 1.3 (p = 0.17) | G1 vs. G2 3 week: p = 56 9 weeks: p = 0.00 12 weeks p = 0.00 | G1 Pre: 34.1 ± 4.3 3 week: 30.2 ± 3.7 (p = 0.04) 9 weeks: 25.4 ± 4.1 (p = 0.01) 12 weeks: 22.3 ± 2.7 (p = 0.00) | G2 Pre: 34.7 ± 5.6 3 week: 28.1 ± 6.7 (p = 0.03) 9 weeks: 28.9 ± 6.8 (p = 0.05) 12 weeks: 31.8 ± 3.4 (p = 53) | ||||||
| G1 vs. G2–3 week: p = 43; 9 weeks: p = 0.00; 12 weeks p = 0.00 | ||||||||||||
| Yildiz (2011) | G1: Ultrasound + Gel with ketoprofen + Splint G2: Ultrasound + Gel with drugs + Splint G3: Placebo ultrasound + Splint | VAS G1 Pre: 5.76 ± 2.45 2weeks: 2.72 ± 2.07 8 weeks: 3.48 ± 2.74 | G2 Pre: 4.96 ± 2.50 2weeks: 2.41 ± 2.43 8 weeks: 2.77 ± 2.74 | G3 Pre: 2.5 ± 0.3 2weeks: 3.03 ± 1.96 8 weeks: 0.98 ± 1.65 | G1 < G3 p = 0.002 G2 < G3 p = 0.004 | G1 Pre: 2.88 ± 0.55 2weeks: 1.94 ± 0.57 8 weeks: 2.08 ± 0.82 | G2 Pre: 2.96 ± 0.62 2weeks: 2.04 ± 0.61 8 weeks: 1.97 ± 0.65 | G3 Pre: 2.93 ± 1.04 2weeks: 1.78 ± 0.75 8 weeks: 1.63 ± 0.73 | G1 Pre: 2.73 ± 0.73 2weeks: 2.08 ± 0.78 8 weeks: 2.19 ± 0.89 | G2 Pre: 2.56 ± 0.64 2weeks: 1.93 ± 0.55 8 weeks: 1.98 ± 0.78 | G3 Pre: 2.79 ± 1.05 2weeks: 2.16 ± 0.80 8 weeks: 1.79 ± 0.80 | |
| Other | Eftekharsadat (2018) | G1: Lavender ointment + Night splint G2: Placebo ointment + Night splint | VAS G1 Pre vs. Post: p = 049 6.96 ± 1.30 vs. 3.58 ± 1.59 | G2 Pre vs. Post: 6.12 ± 1.54 vs. 4.79 ± 2.36 | G1 vs. G2 p < 0.001 | G1 Pre vs. Post: p < 0.001 2.20 ± 0.48 vs. 1.59 ± 0.29 | G2 Pre vs. Post: p < 0.001 2.18 ± 0.49 vs. 1.78 ± 0.53 | |||||
| G1 vs. G2 p = 0.003 | ||||||||||||
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Atthakomol (2018) | X | X | X | X | X | X | X | 7 | ||||
| Çatalbas (2018) | X | X | X | X | X | X | X | 7 | ||||
| Chen (2015) | X | X | X | X | X | X | X | 7 | ||||
| Chung (2016) | X | X | X | X | X | X | X | X | X | X | 10 | |
| Dinarvand (2017) | X | X | X | X | X | X | 6 | |||||
| Eftekharsadat (2018) | X | X | X | X | X | X | X | X | 8 | |||
| Fusakul (2014) | X | X | X | X | X | X | X | X | 8 | |||
| Geler-Külcü (2016) | X | X | X | X | X | X | X | X | 8 | |||
| Günay (2015) | X | X | X | X | X | X | X | 7 | ||||
| Güner (2018) | X | X | X | X | X | X | X | 7 | ||||
| Hadianfard (2015) | X | X | X | X | X | X | X | X | 8 | |||
| Hamzeh (2020) | X | X | X | X | X | X | X | 7 | ||||
| Horng (2011) | X | X | X | X | X | X | 6 | |||||
| Incebiyik (2015) | X | X | X | X | X | X | X | X | 8 | |||
| Karimzadeh (2019) | X | X | X | X | X | X | 7 | |||||
| Kumnerddee (2010) | X | X | X | X | X | X | 6 | |||||
| Ordahan (2017) | X | X | X | X | X | X | 6 | |||||
| Raeissadat (2018) | X | X | X | X | X | X | X | X | 8 | |||
| Senna (2019) | X | X | X | X | X | X | X | X | 8 | |||
| Talebi (2018) | X | X | X | X | X | X | X | X | 8 | |||
| Tezel (2019) | X | X | X | X | X | X | 6 | |||||
| Wang (2017) | X | X | X | X | X | X | X | X | X | 9 | ||
| Wolny (2019) | X | X | X | X | X | X | 6 | |||||
| Wolny (2017) | X | X | X | X | X | X | X | 7 | ||||
| Wu (2018) | X | X | X | X | X | X | X | X | 8 | |||
| Wu (2017) | X | X | X | X | X | X | X | X | X | 9 | ||
| Wu (2016) | X | X | X | X | X | X | X | X | X | 9 | ||
| Xu (2020) | X | X | X | X | X | X | X | X | 8 | |||
| Yildiz (2011) | X | X | X | X | X | X | X | X | 8 | |||
| Mean | 7.5 | |||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Secorún, M.; Montaña-Cortés, R.; Hidalgo-García, C.; Rodríguez-Sanz, J.; Corral-de-Toro, J.; Monti-Ballano, S.; Hamam-Alcober, S.; Tricás-Moreno, J.M.; Lucha-López, M.O. Effectiveness of Conservative Treatment According to Severity and Systemic Disease in Carpal Tunnel Syndrome: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 2365. https://doi.org/10.3390/ijerph18052365
Hernández-Secorún M, Montaña-Cortés R, Hidalgo-García C, Rodríguez-Sanz J, Corral-de-Toro J, Monti-Ballano S, Hamam-Alcober S, Tricás-Moreno JM, Lucha-López MO. Effectiveness of Conservative Treatment According to Severity and Systemic Disease in Carpal Tunnel Syndrome: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(5):2365. https://doi.org/10.3390/ijerph18052365
Chicago/Turabian StyleHernández-Secorún, Mar, Raquel Montaña-Cortés, César Hidalgo-García, Jacobo Rodríguez-Sanz, Jaime Corral-de-Toro, Sofia Monti-Ballano, Sami Hamam-Alcober, José Miguel Tricás-Moreno, and María Orosia Lucha-López. 2021. "Effectiveness of Conservative Treatment According to Severity and Systemic Disease in Carpal Tunnel Syndrome: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 5: 2365. https://doi.org/10.3390/ijerph18052365