
The Course of Posterior Antebrachial Cutaneous Nerve: Anatomical and Sonographic Study with a Clinical Implication

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ultrasonography Study
2.2. Anatomical Study
3. Results
3.1. Ultrasonography Study
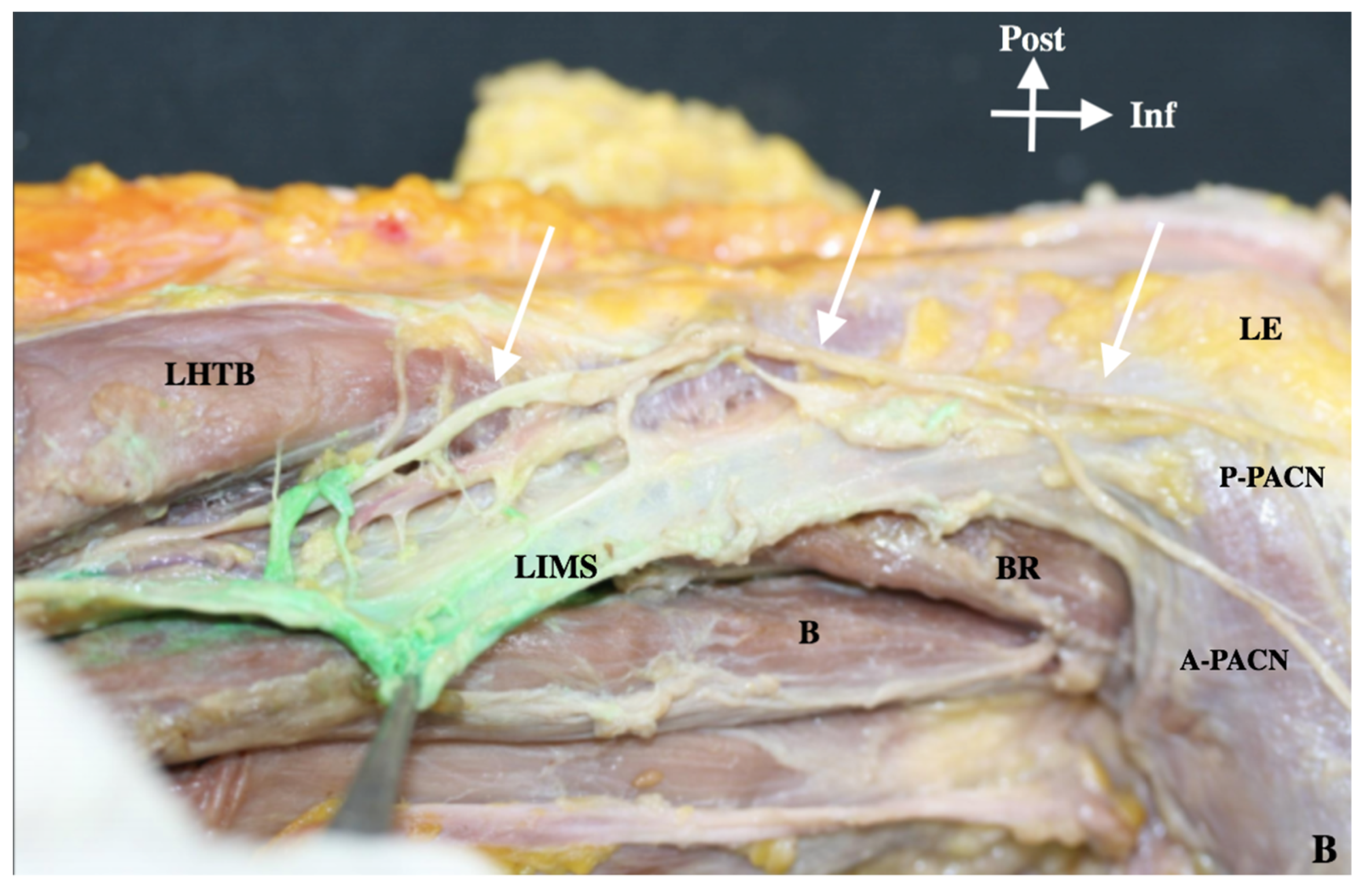
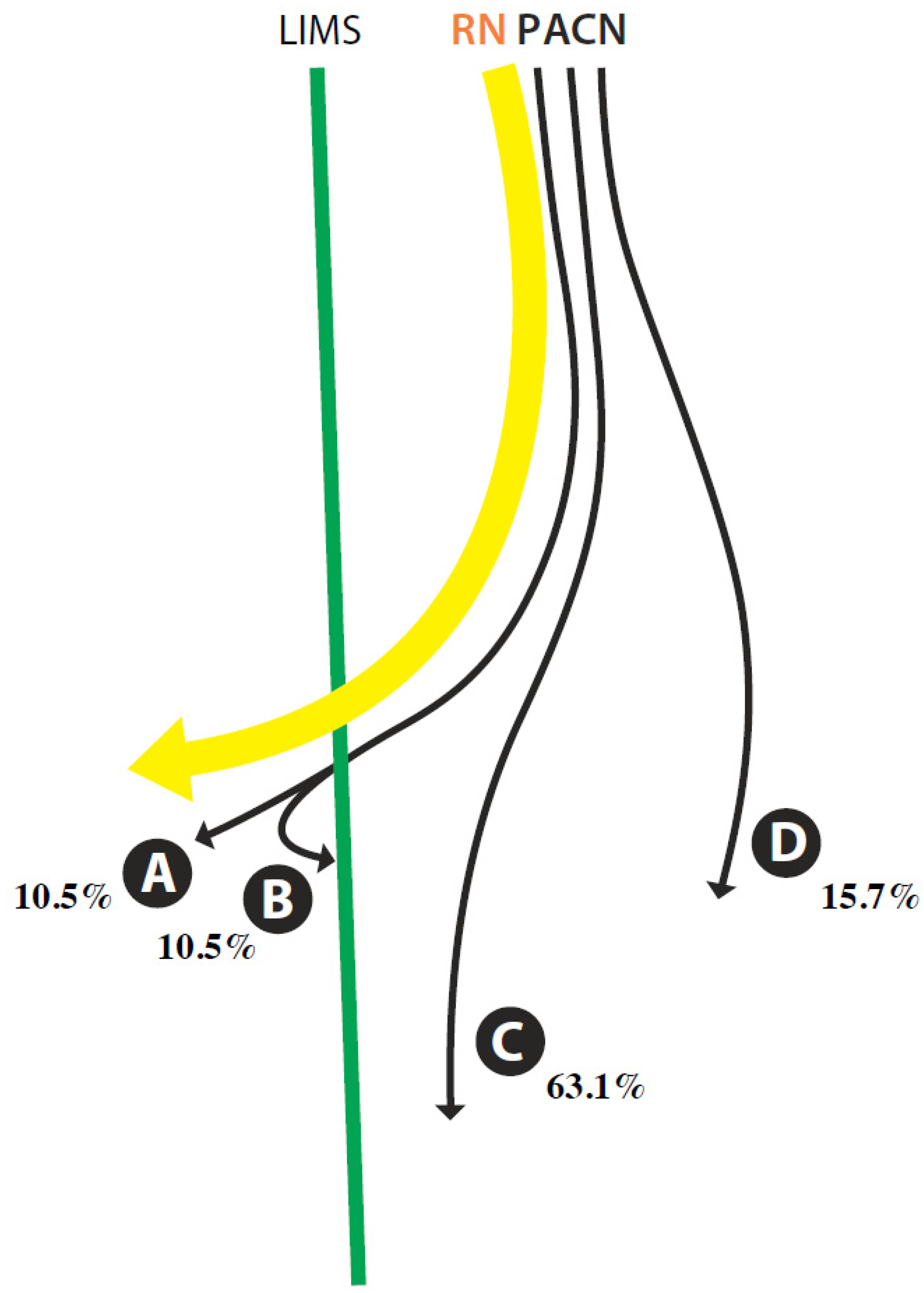
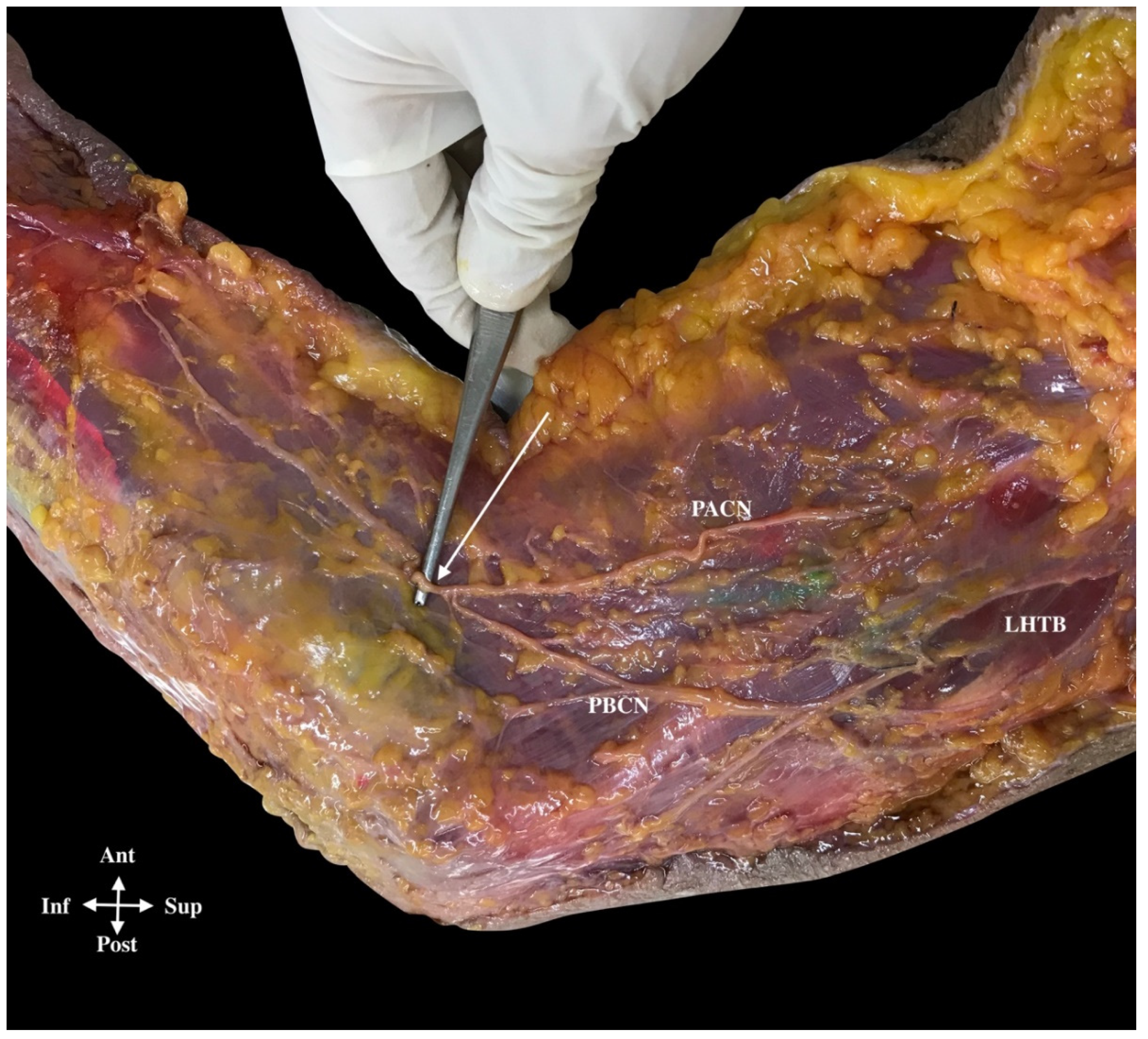
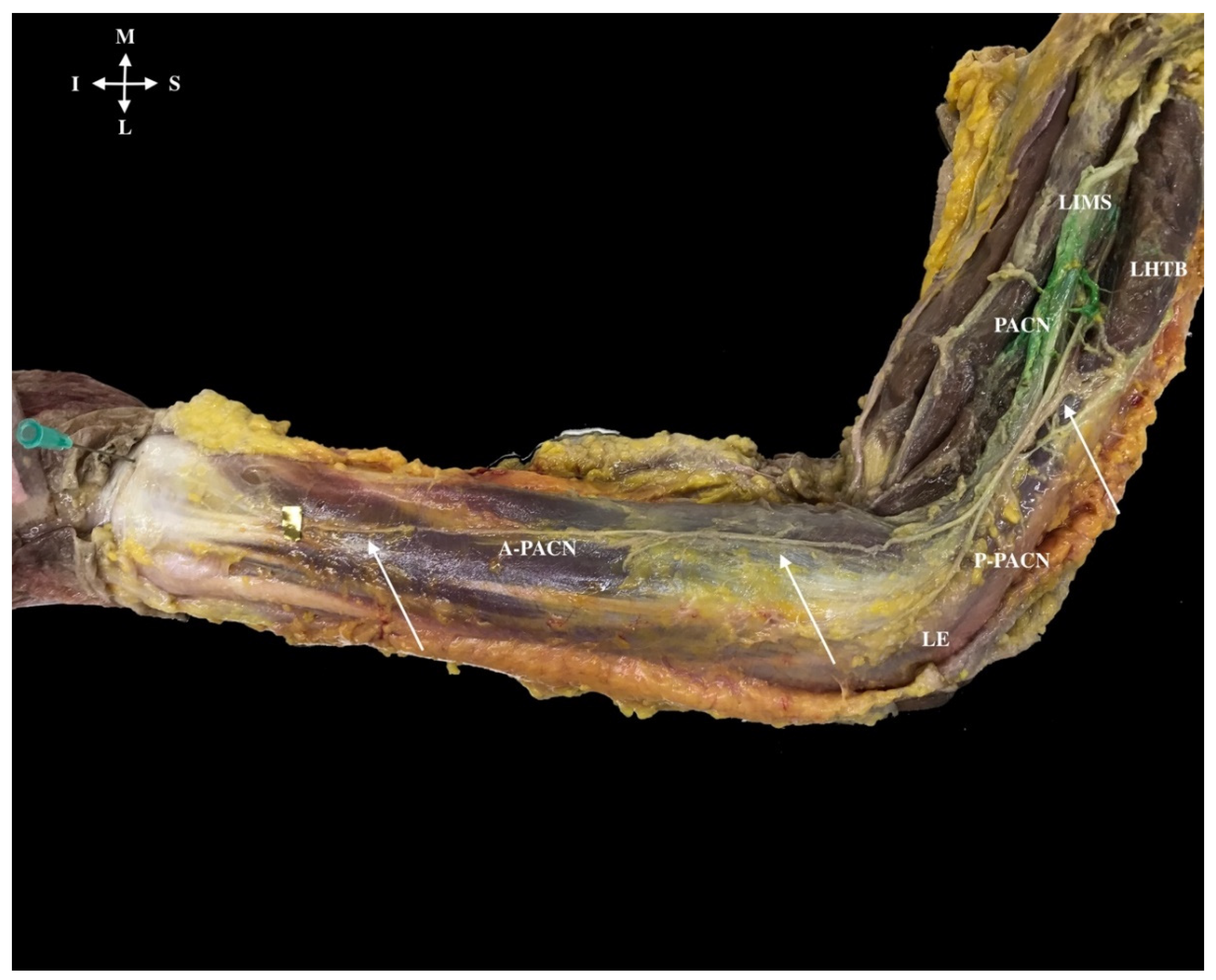
3.2. Anatomical Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smidt, N.; Lewis, M.; Windt, D.A.V.D.; Hay, E.M.; Bouter, L.M.; Croft, P. Lateral epicondylitis in general practice: Course and prognostic indicators of outcome. J. Rheumatol. 2006, 33, 2053–2059. [Google Scholar] [PubMed]
- Rettig, A.C.; Patel, D.V. Epidemiology of elbow, forearm, and wrist injuries in the athlete. Clin. Sports Med. 1995, 14, 289–297. [Google Scholar] [CrossRef]
- Walker-Bone, K.; Palmer, K.T.; Reading, I.; Cooper, C. Soft-tissue rheumatic disorders of the neck and upper limb: Prevalence and risk factors. Semin. Arthritis Rheum. 2003, 33, 185203. [Google Scholar] [CrossRef]
- Doyle, J.J.; David, W.S. Posterior antebrachial cutaneous neuropathy associated with lateral elbow pain. Muscle Nerve 1993, 16, 1417–1418. [Google Scholar] [PubMed]
- Kotnis, N.A.; Chiavaras, M.M.; Harish, S. Lateral epicondylitis and beyond: Imaging of lateral elbow pain with clinical-radiologic correlation. Skelet. Radiol. 2012, 41, 369–386. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.V.; Mezian, K.; Naňka, O.; Wu, W.T.; Lou, Y.M.; Wang, J.C.; Martinoli, C.; Özçakar, L. Ultrasound Imaging for the Cutaneous Nerves of the Extremities and Relevant Entrapment Syndromes: From Anatomy to Clinical Implications. J. Clin. Med. 2018, 21, 457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wee, T.C.; Wu, C.H.; Chen, W.S.; Wang, T.G. Sonographic Evaluation of the Posterior Interosseous Nerve in a Patient with Wrist Drop. Am. J. Phys. Med. Rehabil. 2018, 97, e68. [Google Scholar] [CrossRef] [PubMed]
- Martinoli, C.; Bianchi, S.; Pugliese, F.; Bacigalupo, L.; Gauglio, C.; Valle, M.; Derchi, L.E. Sonography of entrapment neuropathies in the upper limb (wrist excluded). J. Clin. Ultrasound 2004, 32, 438–450. [Google Scholar] [CrossRef]
- Wu, C.H.; Boudier-Revéret, M. Ultrasound-guided steroid injections for lateral antebrachial cutaneous nerve entrapment within postsurgical scar. Am. J. Phys. Med. Rehabil. 2019, 98, e106. [Google Scholar] [CrossRef] [PubMed]
- Schmid, A.B.; Nee, R.J.; Coppieters, M.W. Reapparaising entrapment neuropathies—mechanisms, diagnosis and management. Man. Ther. 2013, 18, 449–457. [Google Scholar] [CrossRef]
- Yildiz, N.; Ardic, F. A rare cause of forearm pain: Anterior branch of the medial antebrachial cutaneous nerve injury: A case report. J. Brachial Plex. Peripher. Nerve Inj. 2008, 3, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belzile, E.; Cloutier, D. Entrapment of the lateral antebrachial cutaneous nerve exiting through the forearm fascia. J. Hand Surg. Am. 2001, 26, 64–67. [Google Scholar] [CrossRef]
- Patl, A.; Pierce, P.; Chiu, D. A facial band implicatd in Wartenberg syndrome. Plast Reconstr. Surg. 2014, 133, 440–442. [Google Scholar] [CrossRef]
- Testut, L.; Latarjet, A. Tratado de Anatomía Humana; Salvat: Barcelona, Spain, 1984; p. 678. [Google Scholar]
- Dellon, A.L.; Kim, J.; Ducic, I. Painful neuroma of the posterior cutaneous nerve of the forearm after surgery for lateral humeral epicondylitis. J. Hand Surg. Am. 2004, 29, 387–390. [Google Scholar] [CrossRef] [PubMed]
- Rose, N.E.; Forman, S.K.; Dellon, A.L. Denervation of the lateral humeral epicondyle for treatment of chronic lateral epicondylitis. J. Hand Surg. Am. 2013, 38, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Moritz, T.; Prosch, H.; Pivec, C.H.; Sachs, A.; Pretterklieber, M.L.; Kriechbaumer, L.; Happak, W.; Bodner, G. High-resolution ultrasound visualization of the subcutaneous nerves of the forearm: A feasibility study in anatomic specimens. Muscle Nerve 2014, 49, 676–679. [Google Scholar] [CrossRef] [PubMed]
- Chodewaratham, P.; Chentanez, V.; Agthong, S.; Huanmanop, T. Anatomy of Posterior Antebrachial Cutaneous Nerve Related to the Lateral Epicondyle and Interepicondylar Line. Int. J. Morphol. 2016, 34, 953–957. [Google Scholar] [CrossRef] [Green Version]
- Finneran, J.J.; Sandhu, N. Ultrasound-guided posterior antebrachial cutaneous nerve block: Technical description and block distribution in healthy volunteers. J. Ultrasound Med. 2019, 38, 239–242. [Google Scholar] [CrossRef] [Green Version]
- Hannouche, D.; Ballis, R.; Raould, A. A lateral approach to the distal humerus following identification of the cutaneous branches of the radial nerve. J. Bone Jt. Surg. Br. 2009, 91, 552–556. [Google Scholar] [CrossRef] [PubMed]
- Stecco, A.; Stern, R.; Fantoni, I.; De Caro, R.; Stecco, C. Fascial Disorders: Implications for Treatment. PM R 2016, 8, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Maida, E.; Chiavaras, M.M.; Jelsing, E.J.; O’Driscoll, S.W.; Pawlina, W.; Smith, J. Sonographic Visualization of the Posterior Cutaneous Nerve of the Forearm: Technique and Validation Using Perineural Injections in a Cadaveric Model. J. Ultrasound Med. 2017, 36, 2395–2399. [Google Scholar] [CrossRef] [PubMed]
- Vicenzino, B.; Paungmali, A.; Buratowski, S. Specific manipulative therapy treatment for chronic lateral epicondylalgia produces uniquely characteristic hypoalgesia. Man. Ther. 2001, 6, 205–212. [Google Scholar] [CrossRef] [Green Version]
- Tubbs, R.S. Anatomy of the lateral intermuscular septum of the arm and its relationships to the radial nerve and its proximal branches: Laboratory investigation. J. Neurosurg. 2009, 111, 336–339. [Google Scholar] [CrossRef]
- MacAvoy, M.C.; Rust, S.S.; Green, D.P. Anatomy of the Posterior Antebrachial Cutaneous Nerve: Practical Information for the Surgeon Operating on the Lateral Aspect of the Elbow. J. Hand Surg. Am. 2006, 31, 908–911. [Google Scholar] [CrossRef] [PubMed]
- Luomala, T.; Pihlman, M.; Heiskanen, J.; Stecco, C. Case study: Could ultrasound and elastrography visualized densified areas inside the deep fascia? J. Dodyw. Mov. Ther. 2014, 18, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Wright, T.W.; Glowczewskie Jr, F.; Cowin, D.; Wheeler, D.L. Radial nerve excursion and strain at the elbow and wrist associated with upper-extremity motion. J. Hand Surg. Am. 2005, 30, 990–996. [Google Scholar] [CrossRef]
- Beldner, S.; Zlotolow, D.A.; Melone, C.P. Anatomy of the lateral antebrachial cutaneous and superficial radial nervesin the forearm: A cadaveric and clinical study. J. Hand Surg. Am. 2005, 30, 1226–1230. [Google Scholar] [CrossRef] [PubMed]
- Shmushkevich, Y.; Kalichman, L. Myofascial pain in lateral epicondylalgia: A review. J. Bodyw. Mov. Ther. 2013, 17, 434–439. [Google Scholar] [CrossRef]
- Chakravarthy Marx, S.; Kumar, P.; Dhalapathy, S. Distribution of sympathetic fiber areas in the sensory nerves of forearm: An immunohistochemical study in cadavers. Rom. J. Morphol. Embryol. 2011, 52, 605–611. [Google Scholar]
- Pavan, P.G.; Stecco, A.; Stern, R.; Stecco, C. Painful connections: Densification versus fibrosis of fascia. Curr. Pain Headache Rep. 2014, 18, 441. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A (US) | A (A) | B (US) | B(A) | C | D | E | F | |
|---|---|---|---|---|---|---|---|---|
| Mean (mm) | 105 | 113 | 74 | 83 | 1.2 | 57 | 36 | 27 |
| SD (mm) | 8 | 11 | 13 | 13 | 2 | 12 | 8 | 6 |
| Range (mm) | 123–84 | 138–99 | 116–50 | 113–58 | 16–7 | 86–37 | 58–23 | 33–17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Martínez, J.; Miguel-Pérez, M.; Pérez-Bellmunt, A.; Ortiz-Miguel, S.; Viscor, G. The Course of Posterior Antebrachial Cutaneous Nerve: Anatomical and Sonographic Study with a Clinical Implication. Int. J. Environ. Res. Public Health 2021, 18, 7733. https://doi.org/10.3390/ijerph18157733
García-Martínez J, Miguel-Pérez M, Pérez-Bellmunt A, Ortiz-Miguel S, Viscor G. The Course of Posterior Antebrachial Cutaneous Nerve: Anatomical and Sonographic Study with a Clinical Implication. International Journal of Environmental Research and Public Health. 2021; 18(15):7733. https://doi.org/10.3390/ijerph18157733
Chicago/Turabian StyleGarcía-Martínez, Jose, Maribel Miguel-Pérez, Albert Pérez-Bellmunt, Sara Ortiz-Miguel, and Ginés Viscor. 2021. "The Course of Posterior Antebrachial Cutaneous Nerve: Anatomical and Sonographic Study with a Clinical Implication" International Journal of Environmental Research and Public Health 18, no. 15: 7733. https://doi.org/10.3390/ijerph18157733