
Self-Learning Methodology in Simulated Environments (MAES©) as a Learning Tool in Perioperative Nursing. An Evidence-Based Practice Model for Acquiring Clinical Safety Competencies


 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
- 1.
- Self-directed and collaborative learning, as the students work in 2–3 person teams, design a scenario, and search for information about the selected case to share with their colleagues afterwards.
- 2.
- Experience-based learning, given that the students come into contact with a situation that is very close to reality, and this training conditions them so that they can appropriately respond to a clinical situation.
- 3.
- Reflective learning, as the participating students’ weak points are worked on, and their strong ones are strengthened. Through a structured debriefing, the participants reflect on the practice and a debate is established, which is very productive for learning. It should be highlighted that the autonomy of the students does not imply that the role of the facilitator is not important. In this sense, the facilitator is the pillar and the guide during the entire learning process.
2. Materials and Methods
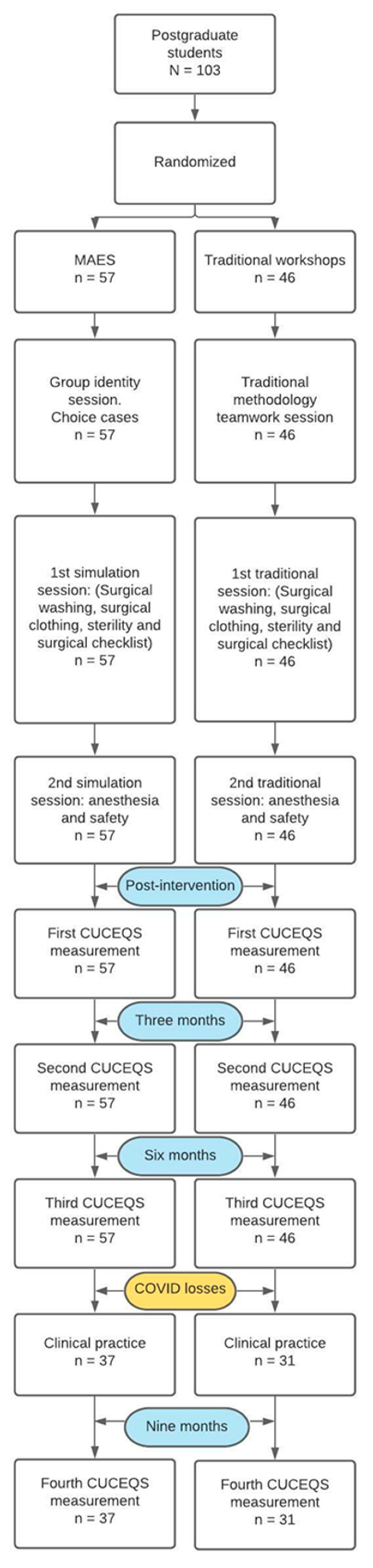
2.1. Design
2.2. Participants
2.3. Procedure
2.3.1. Experimental Group (Learning with MAES©)
- Session 1 (in-person).
- Sessions 2 and 3 (in-person).
2.3.2. Control Group (Learning with Traditional Practical Seminars of Clinical Skills)
- Session 1 (in-person).
- Sessions 2 and 3.
2.4. Instrument and Data Collection
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Description of the Sample
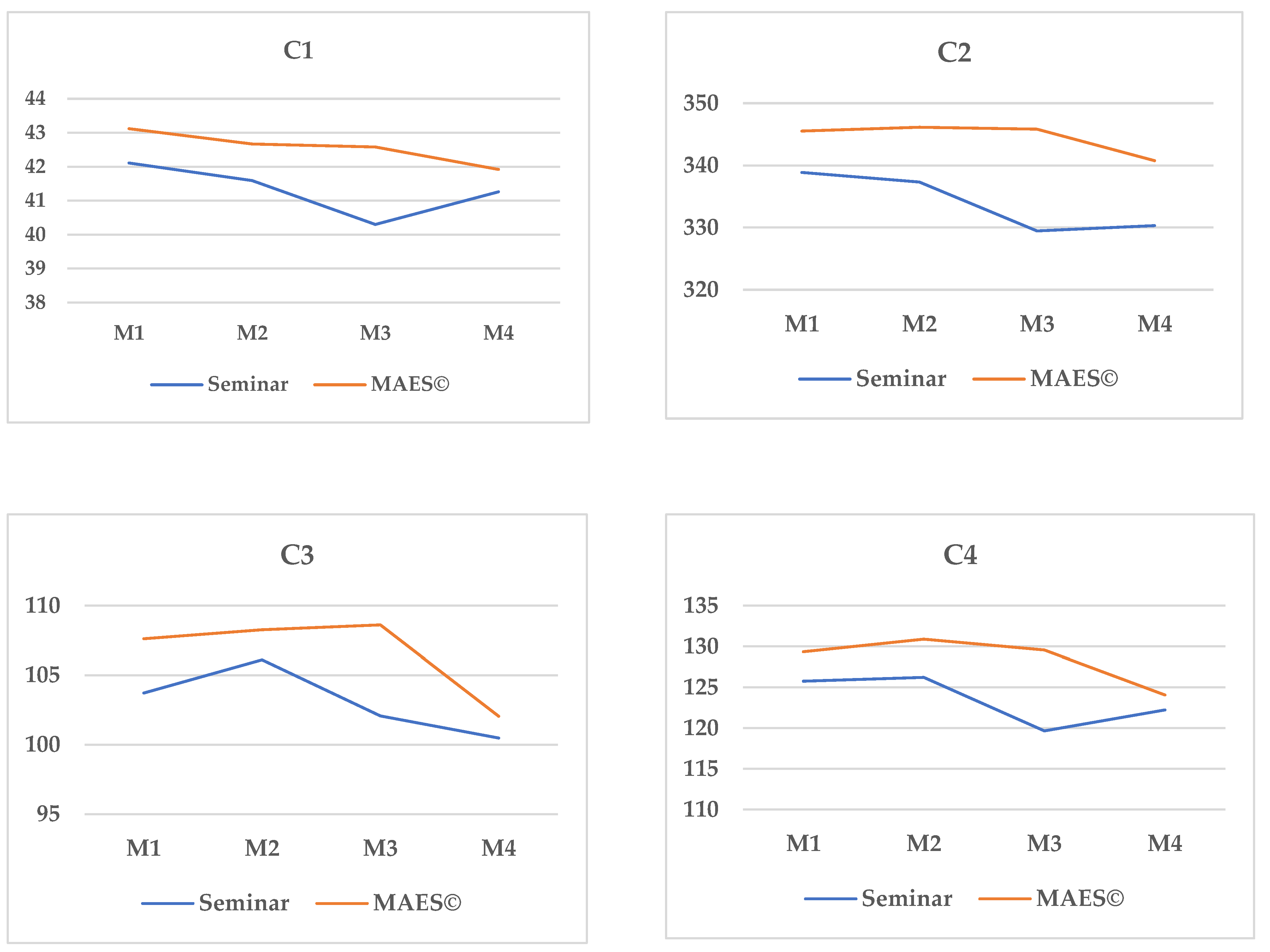
3.2. Competencies in Surgical Safety
4. Discussion
5. Conclusions
6. Strengths, Limitations, and Areas for Further Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Institute of Medicine (US) Commitee on Quality of Health Care in America. To Err Is Human: Building a Safer Health System; National Academies Press: Washington, DC, USA, 2000.
- Collins, S.J.; Newhouse, R.; Porter, J.; Talsma, A. Effectiveness of the Surgical Safety Checklist in Correcting Errors: A Literature Review Applying Reason’s Swiss Cheese Model. AORN J. 2014, 100, 65–79. [Google Scholar] [CrossRef] [PubMed]
- Van Delft, E.A.K.; Schepers, T.; Bonjer, H.J.; Kerkhoffs, G.M.M.J.; Goslings, J.C.; Schep, N.W.L. Safety in the operating room during orthopedic trauma surgery—incidence of adverse events related to technical equipment and logistics. Arch. Orthop. Trauma Surg. 2018, 138, 459–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haynes, A.B.; Weiser, T.G.; Berry, W.R.; Lipsitz, S.R.; Breizat, A.-H.S.; Dellinger, E.P.; Herbosa, T.; Joseph, S.; Kibatala, P.L.; Lapitan, M.C.M.; et al. A Surgical Safety Checklist to Reduce Morbidity and Mortality in a Global Population. N. Engl. J. Med. 2009, 360, 491–499. [Google Scholar] [CrossRef]
- World Health Organization. Implementation Manual WHO Surgical Safety Checklist 2009; Safe Surgery Saves Lives; WHO Library Cataloguing; WHO Press: Geneva, Switzerland, 2009; Available online: https://apps.who.int/iris/bitstream/handle/10665/44186/9789241598590_eng.pdf;sequence=1 (accessed on 7 September 2020).
- Fudickar, A.; Hörle, K.; Wiltfang, J.; Bein, B. The Effect of the WHO Surgical Safety Checklist on Complication Rate and Communication. Dtsch. Arztebl. Int. 2012, 109, 695–701. [Google Scholar] [CrossRef]
- Papadakis, M.; Meiwandi, A.; Grzybowski, A. The WHO safer surgery checklist time out procedure revisited: Strategies to optimise compliance and safety. Int. J. Surg. 2019, 69, 19–22. [Google Scholar] [CrossRef]
- Hosny El-Shafei, A.M.; Yassin Ibrahim, S.; Mahmoud Tawfik, A.; Abd El Fatah, S.A.M. World Health Organization Surgical Safety Checklist with Addition of Infection Control Items: Intervention Study in Egypt. Open Access Maced. J. Med. Sci. 2019, 7, 3691–3697. [Google Scholar] [CrossRef] [Green Version]
- Association of periOperative Registered Nurses (AORN). Guidelines for Perioperative Practice, 2015th ed.; AORN Publications Department: Denver, CO, USA, 2015; p. 771. [Google Scholar]
- European Operating Room Nurses Association (EORNA). EORNA Common Core Curriculum for Perioperative Nursing, 2019 ed. Available online: https://eorna.eu/wp-content/uploads/2020/09/EORNA-Common-Core-Curriculum-for-Perioperative-Nursing-Third-Edition-2019.pdf (accessed on 7 September 2020).
- Michel, N.; Cater, J.J.; Varela, O. Active versus passive teaching styles: An empirical study of student learning outcomes. Hum. Resour. Dev. Q. 2009, 20, 397–418. [Google Scholar] [CrossRef]
- Curran, M.K. Examination of the Teaching Styles of Nursing Professional Development Specialists, Part I: Best Practices in Adult Learning Theory, Curriculum Development, and Knowledge Transfer. J. Contin. Educ. Nurs. 2014, 45, 233–240. [Google Scholar] [CrossRef]
- Taylor, D.C.M.; Hamdy, H. Adult learning theories: Implications for learning and teaching in medical education: AMEE Guide No. 83. Med. Teach. 2013, 35, e1561–e1572. [Google Scholar] [CrossRef]
- Roussin, C.J.; Weinstock, P. SimZones: An Organizational Innovation for Simulation Programs and Centers. Acad. Med. J. Assoc. Am. Med. Coll. 2017, 92, 1114–1120. [Google Scholar] [CrossRef]
- Sittner, B.J.; Aebersold, M.L.; Paige, J.B.; Graham, L.L.M.; Schram, A.P.; Decker, S.I.; Lioce, B. INACSL Standards of Best Practice for Simulation: Past, Present, and Future. Nurs. Educ. Perspect. 2015, 36, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, W.; Sensenig, K. The Sourcebook for Self-Directed Learning; Human Resource Development Press, Inc.: Amherst, MA, USA, 1999; p. 248. [Google Scholar]
- Barrows, H.; Tamblyn, R. Problem-Based Learning: An Approach to Medical Education; Springer Publishing Company: New York City, NY, USA, 1980. [Google Scholar]
- Barkley, E.; Major, C.H.; Cross, K.P. Collaborative Learning Techniques: A Handbook for College Faculty, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2014. [Google Scholar]
- Damon, W. Peer education: The untapped potential. J. Appl. Dev. Psychol. 1984, 5, 331–343. [Google Scholar] [CrossRef]
- Díaz, J.L.; Leal, C.; García, J.A.; Hernández, E.; Adánez, M.G.; Sáez, A. Self-Learning Methodology in Simulated Environments (MAES©): Elements and Characteristics. Clin. Simul. Nurs. 2016, 12, 268–274. [Google Scholar] [CrossRef]
- Díaz Agea, J.L.; Megías Nicolás, A.; García Méndez, J.A.; Adánez-Martínez, M.G.; Leal Costa, C. Improving simulation performance through Self-Learning Methodology in Simulated Environments (MAES©). Nurse Educ. Today 2019, 76, 62–67. [Google Scholar] [CrossRef]
- Arrogante, O.; González-Romero, G.M.; Carrión-García, L.; Polo, A. Reversible causes of cardiac arrest: Nursing competency acquisition and clinical simulation satisfaction in undergraduate nursing students. Int. Emerg. Nurs. 2021, 54, 100938. [Google Scholar] [CrossRef]
- Díaz Agea, J.L.; Ramos-Morcillo, A.J.; Amo Setien, F.J.; Ruzafa-Martínez, M.; Hueso-Montoro, C.; Leal-Costa, C. Perceptions about the Self-Learning Methodology in Simulated Environments in Nursing Students: A Mixed Study. Int. J. Environ. Res. Public Health 2019, 16, 4646. [Google Scholar] [CrossRef] [Green Version]
- Leal Costa, C.; Megías Nicolás, A.; García Méndez, J.A.; Adánez Martínez, M.; Díaz Agea, J.L. Enseñando con metodología de autoaprendizaje en entornos simulados (MAES©). Un estudio cualitativo entre profesores y alumnos de grado en Enfermería. Educ. Med. 2019, 20, 52–58. [Google Scholar] [CrossRef]
- Pardo Merino, A.; Ruíz Díaz, M.A.; San Martín Castellanos, R. Análisis de Datos en Ciencias Sociales y de la Salud I; MCCS; Editorial Síntesis: Madrid, Spain, 2009. [Google Scholar]
- Castillo, J.; Gallart, A.; Rodríguez, E.; Castillo, J.; Gomar, C. Basic life support and external defibrillation competences after instruction and at 6 months comparing face-to-face and bleended training. Randomised trial. Nurse Educ. Today 2018, 65, 232–238. [Google Scholar] [CrossRef]
- Urbach, D.R.; Govindarajan, A.; Saskin, R.; Wilton, A.S.; Baxter, N.N. Introduction of Surgical Safety Checklists in Ontario, Canada. N. Engl. J. Med. 2014, 370, 1029–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahtinen, P.; Leino-Kilpi, H.; Salminen, L. Nursing education in the European higher education area—Variations in implementation. Nurse Educ. Today 2014, 34, 1040–1047. [Google Scholar] [CrossRef] [PubMed]
- Lavoie, P.; Clarke, S.P. Simulation in nursing education. Nurs. Manag. 2017, 48, 16–17. [Google Scholar] [CrossRef] [Green Version]
- Church, C.D. Defining Competence in Nursing and Its Relevance to Quality Care. J. Nurses Prof. Dev. 2016, 32, E9–E14. [Google Scholar] [CrossRef]
- Zenobia, C.Y.C. A systematic review of critical thinking in nursing education. Nurse Educ. Today 2013, 33, 236–240. [Google Scholar] [CrossRef]
- Cook, D.A.; Artino, A.R. Motivation to learn: An overview of contemporary theories. Med. Educ. 2016, 50, 997–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díaz-Agea, J.L.; Pujalte-Jesús, M.J.; Leal-Costa, C.; García-Méndez, J.A.; Adánez-Martínez, M.G.; Jiménez-Rodríguez, D. Motivation: Bringing up the rear in nursing education. Motivational elements in simulation. The participants’ perspective. Nurse Educ. Today 2021, 103, 104925. [Google Scholar] [CrossRef]
- Brandon, A.F.; All, C.A. Constructivism Theory Analysis and Application to Curricula. Nurs. Educ. Perspect. 2010, 31, 89–92. [Google Scholar] [PubMed]
- Agra, G.; Soares Formiga, N.; Simplicío de Oliveira, P.; Lopes Costa, M.M.; Melo Fernandes, M.M.; Lima deNóbrega, M.M. Analysis of the concept of Meaningful Learning in light of the Ausubel’s Theory. Rev. Bras. Enferm. 2019, 72, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Mackey, A.; Bassendowski, S. The History of Evidence-Based Practice in Nursing Education and Practice. J. Prof. Nurs. 2017, 33, 51–55. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Situation Proposed | Knowledge and Skills Chosen by the Group to Conduct Research On |
|---|---|
| Perioperative nurse https://www.youtube.com/watch?v=uBMdgprsmSA (Access date: 2 and 13 November 2018; 13 and 20 November 2019) | Knowledge of surgical scrubbing and sterile surgical clothing. Development of skills. |
| The ring https://www.youtube.com/watch?v=OgfJhOKmXog (Access date: 2 and 13 November 2018; 13 and 20 November 2019) | Knowledge of the correct putting on of gloves through the identification of an error. Development of skills. |
| Emergency https://www.youtube.com/watch?v=naSKwEYVfOM (Access date: 2 and 13 November 2018; 13 and 20 November 2019) | Surgical checklist (phases, development, nurse leadership, and multidisciplinary communication). Practice of WHO standards. |
| The mistake https://www.youtube.com/watch?v=HHD8mNhwG_I (Access date: 2 and 13 November 2018; 13 and 20 November 2019) | Learning about an error. Erroneous surgery. Practice of WHO standards. |
| News https://www.youtube.com/watch?v=_dKxcaTKDnE (Access date: 2 and 13 November 2018; 13 and 20 November 2019) | Learning about an error. Ethical problem when facing the death of a patient in surgery. |
| Awake https://www.youtube.com/watch?v=CTFEz2RPsWE (Access date: 2 and 13 November 2018; 13 and 20 November 2019) | Learning about the care and monitoring of a patient who receives general anesthesia. Development of the necessary skills. |
| They ruined his life https://www.youtube.com/watch?v=WxVTWOt0h00 (Access date: 2 and 13 November 2018; 13 and 20 November 2019) | Learning through different mistakes in surgery or anesthesia. Development of skills after the identification of a drug-related allergy. |
| How do you know if you are tired? https://www.youtube.com/watch?v=rK2Yh2GXE78 (Access date: 2 and 13 November 2018; 13 and 20 November 2019) | Learning about the importance of coordination and teamwork in an operating room. |
| Communication/respect https://www.youtube.com/watch?v=HS-Johhbl0s (Access date: 2 and 13 November 2018; 13 and 20 November 2019) | Development of the importance of the confidentiality of the patient and respect of intimacy. |
| Communication/respect https://www.youtube.com/watch?v=BSMF6JhW0tE (Access date: 2 and 13 November 2018; 13 and 20 November 2019) | Development of the importance of the confidentiality of the patient and respect of intimacy. |
| Session 1 (2 h) | Session 2 (4 h) | Session 3 (4 h) |
|---|---|---|
| Prebriefing | Briefing (10′) Simulation experience (20′) Debriefing (30–35′) | Briefing (10′) Simulation experience (20′) Debriefing (30–35′) |
| Creation of simulation groups | Case 1 Simulation (1 h): Development of safe and quality care of perioperative nursing | Case 4 Simulation (1 h): Error/Perioperative nursing care related to general anesthesia |
| Presentation of learning objectives according to competencies. Selection of cases. | Case 2 Simulation (1 h): Surgery errors/ Surgical checklist | Case 5 Simulation (1 h): Perioperative nurse/Safe general anesthesia. |
| Definition of learning interests by the students. | Case 3 Simulation (1 h): Teamwork/Efficient communication/Nurse leadership in the perioperative process. | Case 6 Simulation (1 h): Error in postoperative analgesia administration/Pharmacological allergy. |
| Competence | Sub-Competence |
|---|---|
|
|
|
|
|
|
|
|
| Seminars (n = 46) | MAES© (n = 57) | Total (n = 103) | Statistic Value a | p | |
|---|---|---|---|---|---|
| Age (M (SD)) | 32.11 (7.63) | 30.32 (7.28) | 31.12 (7.46) | 1.22 | 0.23 |
| Sex (n (%)) | - | - | - | 4.16 | 0.04 |
| Female | 33 (71.70) | 50 (87.70) | 83 (80.60) | - | - |
| Male | 13 (28.30) | 7 (12.30) | 20 (19.40) | - | |
| Years of experience (M (SD)) | 6.09 (6.57) | 5.49 (5.70) | 5.76 (6.08) | 0.49 | 0.62 |
| Years of experience, operating room (M (SD)) | 0.78 (2.24) | 1.14 (2.71) | 0.98 (2.51) | −0.72 | 0.47 |
| Posterior studies (%) | - | - | - | 2.58 | 0.46 |
| Masters | 19 (41.30) | 19 (30.30) | 38 (36.90) | - | - |
| Postgraduate course | 19 (41.30) | 28 (49.10) | 47 (45.60) | - | - |
| Doctorate | 0 (0) | 2 (3.50) | 2 (1.90) | - | - |
| Others | 8 (17.40) | 8 (14.00) | 16 (15.50) | - | - |
| M1 | M2 | M3 | M4 | n = 46 | n = 46 | n = 31 | n = 46 | n = 31 | n = 31 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | t1 | p | t2 | p | t3 | p | t4 | p | t5 | p | t6 | p | |
| C1 | 42.11 | 41.59 | 40.30 | 41.26 | 1.12 | 0.27 | 3.39 | 0.00 | 1.70 | 0.10 | 3.04 | 0.00 | 0.12 | 0.91 | 1.45 | 0.16 |
| (2.30) | (2.47) | (3.18) | (2.50) | |||||||||||||
| C2 | 338.87 | 337.33 | 329.46 | 330.32 | 0.52 | 0.61 | 2.93 | 0.01 | 1.66 | 0.11 | 2.62 | 0.01 | 0.93 | 0.36 | 0.00 | 1.00 |
| (13.75) | (18.52) | (18.86) | (28.23) | |||||||||||||
| C3 | 103.72 | 106.11 | 102.07 | 100.48 | −1.45 | 0.15 | 1.12 | 0.27 | 0.85 | 0.40 | 3.56 | 0.00 | 1.83 | 0.08 | 0.57 | 0.57 |
| (10.95) | (9.45) | (8.81) | (14.01) | |||||||||||||
| C4 | 125.76 | 126.22 | 119.65 | 122.22 | −0.25 | 0.81 | 2.95 | 0.01 | 1.25 | 0.22 | 4.23 | 0.00 | 0.71 | 0.48 | −1.26 | 0.22 |
| (11.39) | (10.06) | (11.59) | (16.00) |
| M1 | M2 | M3 | M4 | n = 57 | n = 57 | n = 37 | n = 57 | n = 37 | n = 37 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | t1 | p | t2 | p | t3 | p | t4 | p | t5 | p | t6 | p | |
| C1 | 43.12 | 42.67 | 42.58 | 41.92 | 1.65 | 0.10 | 1.86 | 0.07 | 2.67 | 0.01 | 0.28 | 0.78 | 0.57 | 0.57 | 1.07 | 0.29 |
| (1.46) | (1.95) | (2.33) | (2.66) | |||||||||||||
| C2 | 345.53 | 346.14 | 345.84 | 340.76 | −0.27 | 0.79 | −0.12 | 0.90 | 0.24 | 0.81 | 0.15 | 0.88 | 0.42 | 0.68 | 0.77 | 0.45 |
| (17.07) | (14.12) | (13.54) | (19.69) | |||||||||||||
| C3 | 107.61 | 108.26 | 108.61 | 102.05 | −0.49 | 0.63 | −0.83 | 0.41 | 1.03 | 0.31 | −0.25 | 0.80 | 1.36 | 0.18 | 2.66 | 0.01 |
| (10.39) | (11.06) | (9.69) | (12.56) | |||||||||||||
| C4 | 129.33 | 130.88 | 129.56 | 124.06 | −0.98 | 0.33 | −0.17 | 0.86 | 0.32 | 0.75 | 0.95 | 0.35 | 1.18 | 0.25 | 1.18 | 0.25 |
| (11.08) | (10.92) | (10.44) | (14.36) |
| M1 | M2 | M3 | M4 | Intergroup A × B | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| M | (SD) | M | (SD) | M | (SD) | M | (SD) | F | p | η2 | |
| C1 | |||||||||||
| Seminar (n = 31) | 42.11 | (2.30) | 41.59 | (2.47) | 40.30 | (3.18) | 41.26 | (2.50) | 3311.57 | <0.001 | 0.98 |
| MAES© (n = 37) | 43.12 | (1.46) | 42.67 | (1.95) | 42.58 | (2.33) | 41.92 | (2.66) | |||
| C2 | |||||||||||
| Seminar (n = 31) | 338.87 | (13.75) | 337.33 | (18.52) | 329.46 | (18.86) | 330.32 | (28.23) | 4225.01 | <0.001 | 0.99 |
| MAES© (n = 37) | 345.53 | (17.07) | 346.14 | (14.12) | 345.84 | (13.54) | 340.76 | (19.69) | |||
| C3 | |||||||||||
| Seminar (n = 31) | 103.72 | (10.95) | 106.11 | (9.45) | 102.07 | (8.81) | 100.48 | (14.01) | 898.18 | <0.001 | 0.93 |
| MAES© (n = 37) | 107.61 | (10.39) | 108.26 | (11.06) | 108.61 | (9.69) | 102.05 | (12.56) | |||
| C4 | |||||||||||
| Seminar (n = 31) | 125.76 | (11.39) | 126.22 | (10.06) | 119.65 | (11.59) | 122.22 | (16.00) | 949.62 | <0.001 | 0.94 |
| MAES© (n = 37) | 129.33 | (11.08) | 130.88 | (10.92) | 129.56 | (10.44) | 124.06 | (14.36) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peñataro-Pintado, E.; Díaz-Agea, J.L.; Castillo, I.; Leal-Costa, C.; Ramos-Morcillo, A.J.; Ruzafa-Martínez, M.; Rodríguez-Higueras, E. Self-Learning Methodology in Simulated Environments (MAES©) as a Learning Tool in Perioperative Nursing. An Evidence-Based Practice Model for Acquiring Clinical Safety Competencies. Int. J. Environ. Res. Public Health 2021, 18, 7893. https://doi.org/10.3390/ijerph18157893
Peñataro-Pintado E, Díaz-Agea JL, Castillo I, Leal-Costa C, Ramos-Morcillo AJ, Ruzafa-Martínez M, Rodríguez-Higueras E. Self-Learning Methodology in Simulated Environments (MAES©) as a Learning Tool in Perioperative Nursing. An Evidence-Based Practice Model for Acquiring Clinical Safety Competencies. International Journal of Environmental Research and Public Health. 2021; 18(15):7893. https://doi.org/10.3390/ijerph18157893
Chicago/Turabian StylePeñataro-Pintado, Ester, José Luis Díaz-Agea, Isabel Castillo, César Leal-Costa, Antonio Jesús Ramos-Morcillo, María Ruzafa-Martínez, and Encarna Rodríguez-Higueras. 2021. "Self-Learning Methodology in Simulated Environments (MAES©) as a Learning Tool in Perioperative Nursing. An Evidence-Based Practice Model for Acquiring Clinical Safety Competencies" International Journal of Environmental Research and Public Health 18, no. 15: 7893. https://doi.org/10.3390/ijerph18157893