
Physiotherapy Rehabilitation in Subjects Diagnosed with Subacromial Impingement Syndrome Does Not Normalize Periscapular and Rotator Cuff Muscle Onset Time of Activation

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
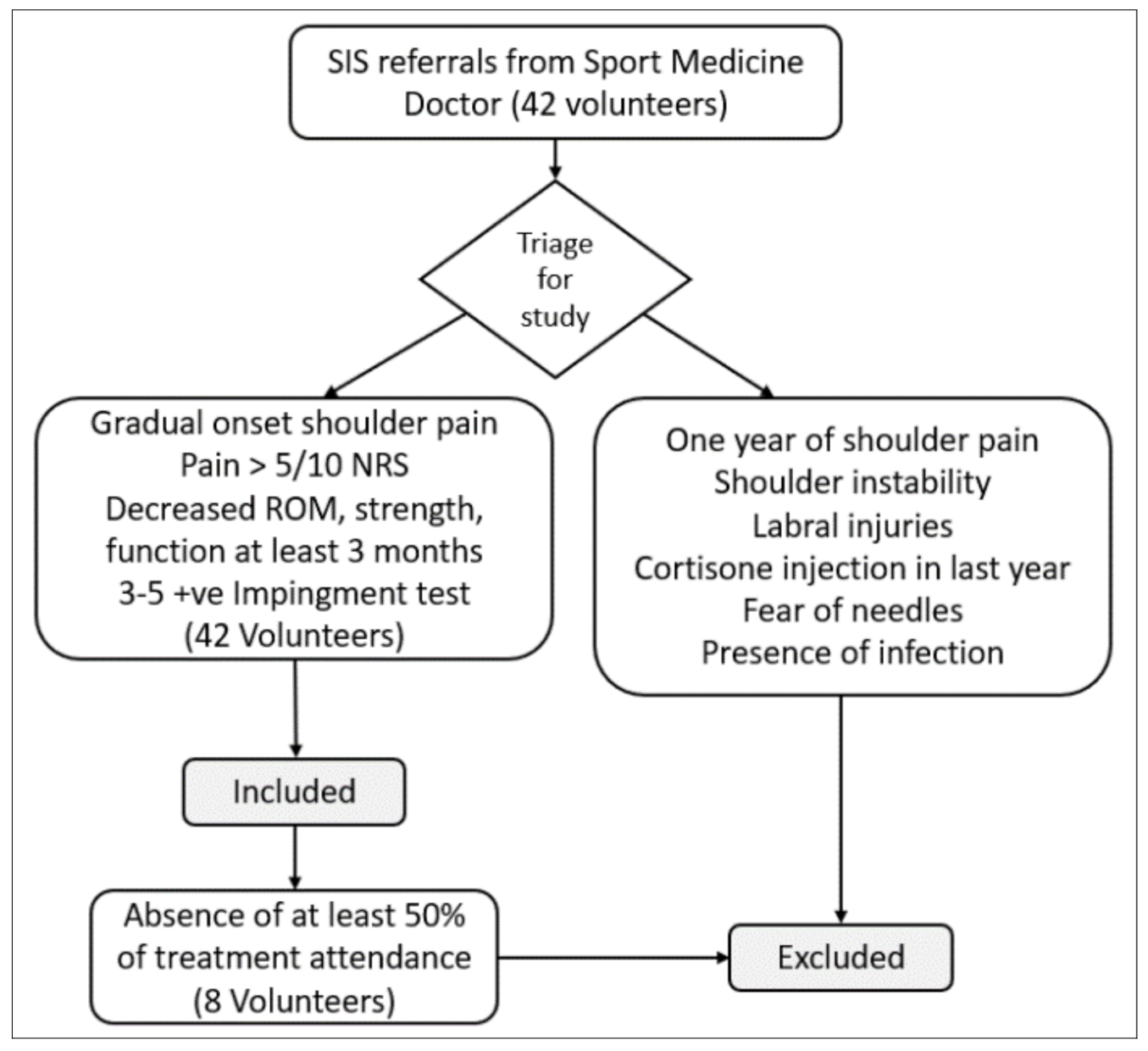
2.1. Settings and Participants
2.2. Variables and Measurements
2.3. Testing Procedure and Instrumentation
2.4. Sample Size
2.5. Signal Processing and Data Analysis
3. Results
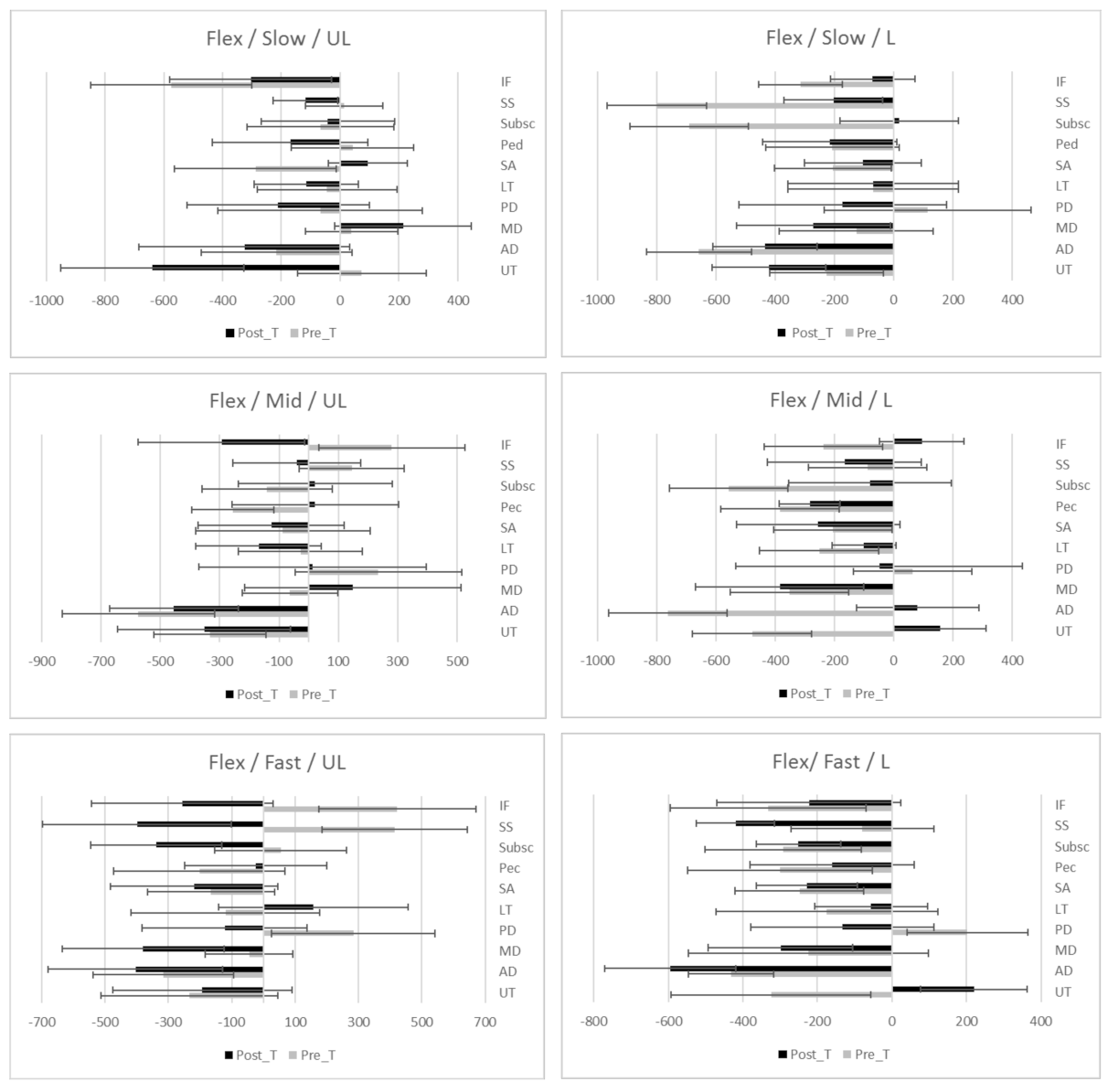
3.1. Flexion Movement
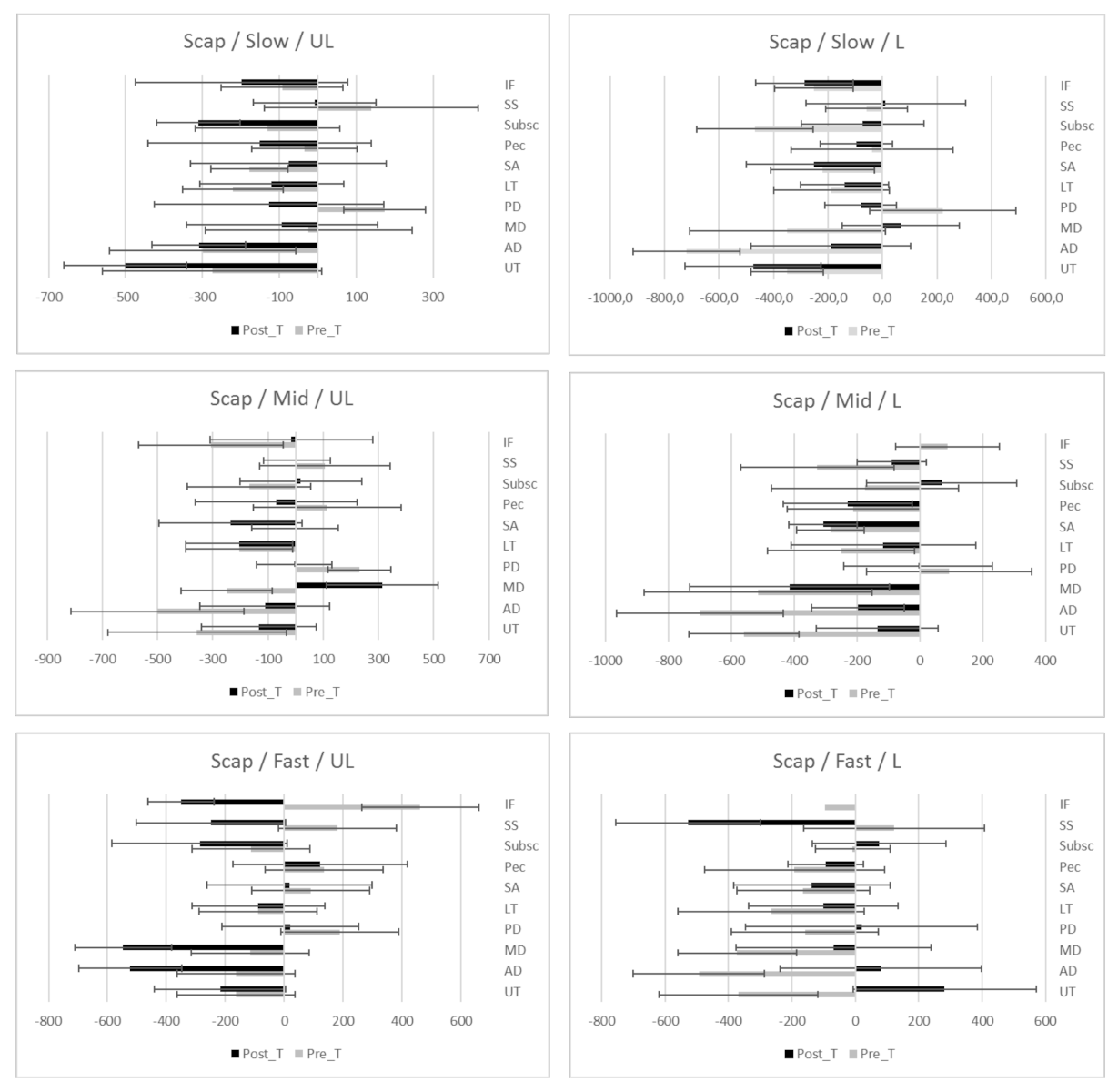
3.2. Scaption Movement
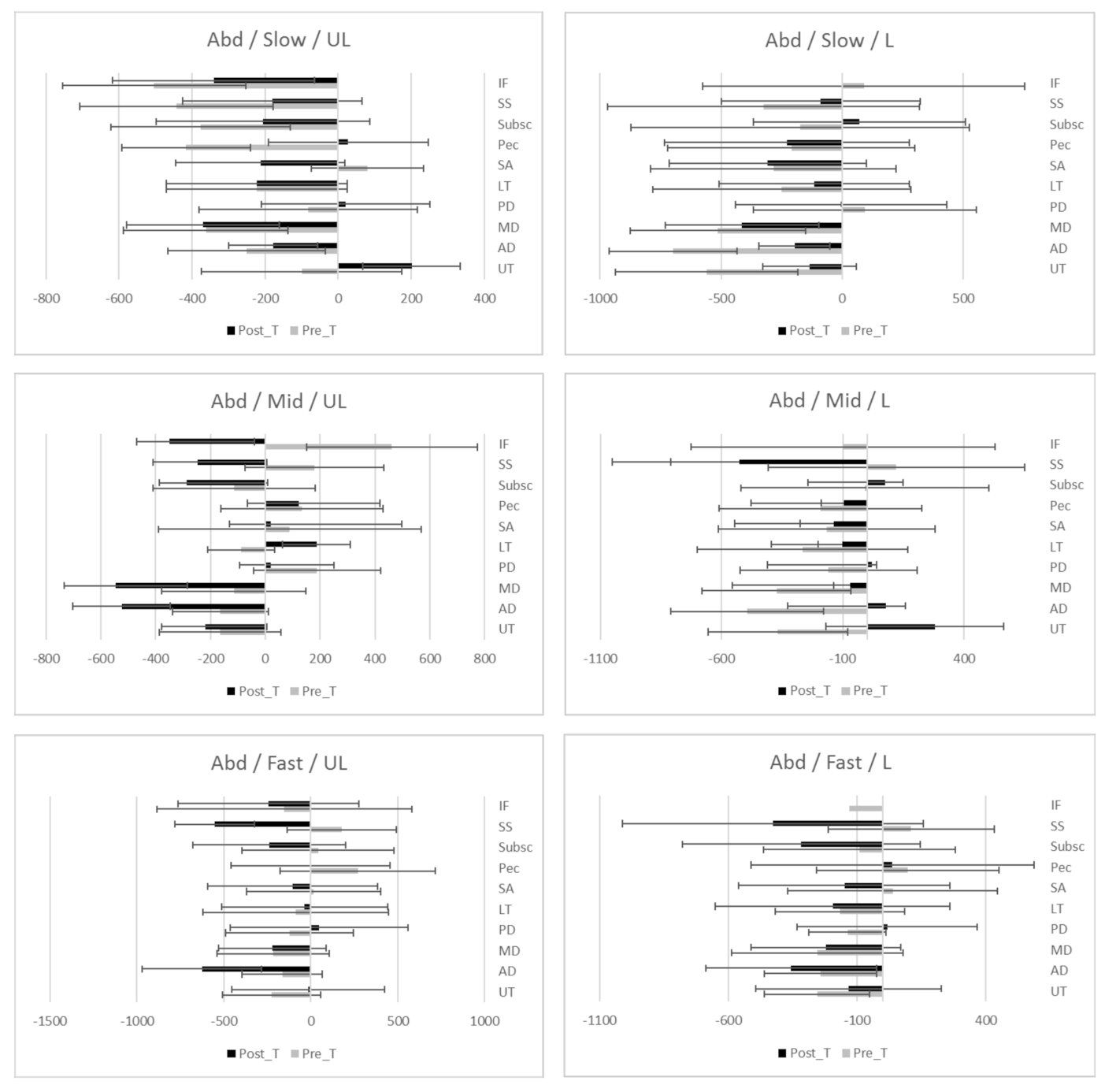
3.3. Abduction Movement
3.4. Post-Hoc Sample Size Calculation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A. Diagram of the Inclusive and Exclusive Criteria

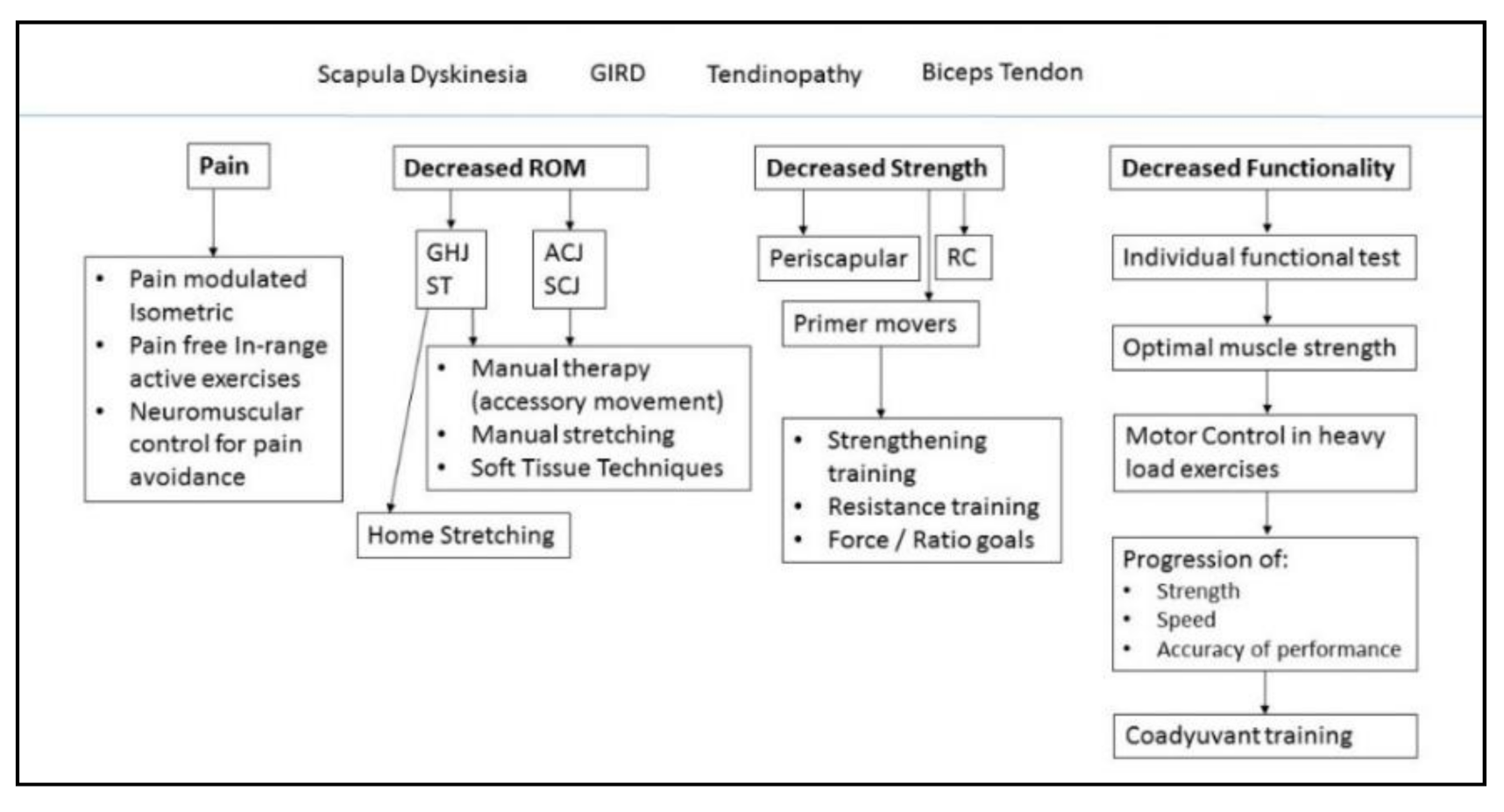
Appendix B. Subacromial Impingement Syndrome Individual Physiotherapy Approach

References
- Jaravay, J. Sur la luxation du tendon de la longue portion du muscle biceps humeral: Sur la luxation de tendons des muscles peroniers latercux. Gaz. Hebd. Med. Chir. 1867, 21, 325. [Google Scholar]
- Neer, C.S. Anterior Acromioplasty for the Chronic Impingement Syndrome in the JBJS Classics Anterior Acromioplasty for the Chronic Impingement Syndrome in the Shoulder. J. Bone Jt. Surg. 1972, 87, 1399. [Google Scholar] [CrossRef]
- Park, H.B.; Yokota, A.; Gill, H.S.; El Rassi, G.; McFarland, E.G. Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. J. Bone Jt. Surg. Am. 2005, 87, 1446–1455. [Google Scholar]
- Hegedus, E.J.; Goode, A.P.; Cook, C.E.; Michener, L.; Myer, C.A.; Myer, D.M.; Wright, A.A. Which physical examination tests provide clinicians with the most value when examining the shoulder? Update of a systematic review with meta-analysis of individual tests. Br. J. Sports Med. 2012, 46, 964–978. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.; Hsieh, S.-C.; Cheng, W.-C.; Chen, W.C.; Lai, Y. Adaptive patterns of movement during arm elevation test in patients with shoulder impingement syndrome. J. Orthop. Res. 2011, 29, 653–657. [Google Scholar] [CrossRef]
- Castelein, B.; Cagnie, B.; Cools, A. Scapular muscle dysfunction associated with subacromial pain syndrome. J. Hand Ther. 2017, 30, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Roy, J.-S.; Moffet, H.; McFadyen, B.J. Upper limb motor strategies in persons with and without shoulder impingement syndrome across different speeds of movement. Clin. Biomech. 2008, 23, 1227–1236. [Google Scholar] [CrossRef]
- Ngomo, S.; Mercier, C.; Bouyer, L.J.; Savoie, A.; Roy, J.-S. Alterations in central motor representation increase over time in individuals with rotator cuff tendinopathy. Clin. Neurophysiol. 2015, 126, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Castelein, B.; Cools, A.; Parlevliet, T.; Cagnie, B. The influence of induced shoulder muscle pain on rotator cuff and scapulothoracic muscle activity during elevation of the arm. J. Shoulder Elb. Surg. 2017, 26, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Ellenbecker, T.S.; Cools, A. Rehabilitation of shoulder impingement syndrome and rotator cuff injuries: An evidence-based review. Br. J. Sports Med. 2010, 44, 319–327. [Google Scholar] [CrossRef] [Green Version]
- Myers, J.; Lephart, S. The Role of the Sensorimotor System in the Athletic Shoulder. J. Athl. Train. 2000, 35, 351–363. [Google Scholar] [PubMed]
- Riemann, B.; Myers, J.; Lephart, S. Sensorimotor System Measurement Techniques. J. Athl. Train. 2002, 37, 85–98. [Google Scholar] [PubMed]
- Seitz, A.L.; McClure, P.W.; Finucane, S.; Boardman, N.D.; Michener, L.A. Mechanisms of rotator cuff tendinopathy: Intrinsic, extrinsic, or both? Clin. Biomech. 2011, 26, 1–12. [Google Scholar] [CrossRef]
- Tucker, W.S.; Armstrong, C.W.; Gribble, P.A.; Timmons, M.K.; Yeasting, R.A. Scapular Muscle Activity in Overhead Athletes With Symptoms of Secondary Shoulder Impingement During Closed Chain Exercises. Arch. Phys. Med. Rehabil. 2010, 91, 550–556. [Google Scholar] [CrossRef]
- Zech, A.; Hübscher, M.; Vogt, L.; Banzer, W.; Hänsel, F.; Pfeifer, K. Neuromuscular Training for Rehabilitation of Sports Injuries: A Systematic Review. Med. Sci. Sports Exerc. 2009, 41, 1831–1841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hübscher, M.; Zech, A.; Pfeifer, K.; Hänsel, F.; Vogt, L.; Banzer, W. Neuromuscular Training for Sports Injury Prevention: A Systematic Review. Med. Sci. Sports Exerc. 2009, 42, 413–421. [Google Scholar] [CrossRef]
- Kibler, W.B.; Sciascia, A. The Shoulder at Risk: Scapular Dyskinesis and Altered Glenohumeral Rotation. Oper. Tech. Sports Med. 2016, 24, 162–169. [Google Scholar] [CrossRef]
- Worsley, P.; Warner, M.; Mottram, S.; Gadola, S.; Veeger, H.E.J.; Hermens, H.; Morrissey, D.; Little, P.; Cooper, C.; Carr, A.; et al. Motor control retraining exercises for shoulder impingement: Effects on function, muscle activation, and biomechanics in young adults. J. Shoulder Elb. Surg. 2013, 22, e11–e19. [Google Scholar] [CrossRef] [Green Version]
- Michener, L.A.; Sharma, S.; Cools, A.M.; Timmons, M.K. Relative scapular muscle activity ratios are altered in subacromial pain syndrome. J. Shoulder Elb. Surg. 2016, 25, 1861–1867. [Google Scholar] [CrossRef]
- Castelein, B.; Cagnie, B.; Parlevliet, T.; Cools, A. Scapulothoracic muscle activity during elevation exercises measured with surface and fine wire EMG: A comparative study between patients with subacromial impingement syndrome and healthy controls. Man. Ther. 2016, 23, 33–39. [Google Scholar] [CrossRef]
- Phadke, V.; Ludewig, P.M. Study of the scapular muscle latency and deactivation time in people with and without shoulder impingement. J. Electromyogr. Kinesiol. 2013, 23, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Wattanaprakornkul, D.; Halaki, M.; Boettcher, C.; Cathers, I.; Ginn, K.A. A comprehensive analysis of muscle recruitment patterns during shoulder flexion: An electromyographic study. Clin. Anat. 2011, 24, 619–626. [Google Scholar] [CrossRef]
- Cools, A.M.; Dewitte, V.; Lanszweert, F.; Notebaert, D.; Roets, A.; Soetens, B.; Cagnie, B.; Witvrouw, E.E. Rehabilitation of Scapular Muscle Balance: Which Exercises to Prescribe? Am. J. Sports Med. 2007, 35, 1744–1751. [Google Scholar] [CrossRef]
- Littlewood, C.; Cools, A.M.J. Scapular dyskinesis and shoulder pain: The devil is in the detail. Br. J. Sports Med. 2018, 52, 72–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangwan, S.; Green, R.A.; Taylor, N.F. Stabilizing characteristics of rotator cuff muscles: A systematic review. Disabil. Rehabil. 2014, 37, 1–11. [Google Scholar] [CrossRef]
- Ortega-Cebrián, S.; Bagur-Cadafal, C.; Whiteley, R.; Navarro, R.; Monné-Guasch, L.; Girabent-Farrés, M. Subacromial Impingment Syndrome does not alter muscle onset activation patterns during shoulder cardinal movement at different speed and load. Musculoskelet. Sci. Pract. 2020, 48, 102. [Google Scholar] [CrossRef] [PubMed]
- Alqunaee, M.; Galvin, R.; Fahey, T. Diagnostic Accuracy of Clinical Tests for Subacromial Impingement Syndrome: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2012, 93, 229–236. [Google Scholar] [CrossRef]
- Hermans, J.; Luime, J.J.; Meuffels, D.E.; Reijman, M.; Simel, D.L.; Bierma-Zeinstra, S.M.A. Does This Patient With Shoulder Pain Have Rotator Cuff Disease?: The Rational Clinical Examination Systematic Review. JAMA 2013, 310, 837. [Google Scholar] [CrossRef]
- Heron, S.R.; Woby, S.R.; Thompson, D.P. Comparison of three types of exercise in the treatment of rotator cuff tendinopathy/shoulder impingement syndrome: A randomized controlled trial. Physiotherapy (UK) 2017, 103, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Drew, M.; Cook, J.; Finch, C. Sports-related workload and injury risk: Simply knowing the risks will not prevent injuries. Br. J. Sports Med. 2016, 50. [Google Scholar] [CrossRef]
- Kadaba, M.P.; Cole, A.; Wootten, M.E.; McCann, P.; Reid, M.; Mulford, G.; April, E.; Bigliani, L. Intramuscular wire electromyography of the subscapularis. J. Orthop. Res. 1992, 10, 394–397. [Google Scholar] [CrossRef] [PubMed]
- Geiringer, S.R. Anatomic Localization for Needle Electromyography; Hanley and Belfus: Philadelphia, PA, USA; Mosby: St. Louis, MO, USA, 1994; ISBN 1-56053-068-5/978-1-56053-068-8. [Google Scholar]
- Bakeman, R. Recommended effect size statistics for repeated measures designs. Behav. Res. Methods 2005, 37, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Hambly, K. The use of the Tegner Activity Scale for articular cartilage repair of the knee: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2010, 19, 604–614. [Google Scholar] [CrossRef]
- Hanratty, C.E.; McVeigh, J.G.; Kerr, D.P.; Basford, J.R.; Finch, M.B.; Pendleton, A.; Sim, J. The Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-Analysis. Semin. Arthritis Rheum. 2012, 42, 297–316. [Google Scholar] [CrossRef]
- De Mey, K.; Danneels, L.; Cagnie, B.; Cools, A.M. Scapular Muscle Rehabilitation Exercises in Overhead Athletes With Impingement Symptoms: Effect of a 6-Week Training Program on Muscle Recruitment and Functional Outcome. Am. J. Sports Med. 2012, 40, 1906–1915. [Google Scholar] [CrossRef]
- Chester, R.; Shepstone, L.; Lewis, J.S.; Jerosch-Herold, C. Predicting response to physiotherapy treatment for musculoskeletal shoulder pain: Protocol for a longitudinal cohort study. BMC Musculoskelet. Disord. 2013, 14, 192. [Google Scholar] [CrossRef] [Green Version]
- Crow, J.; Pizzari, T.; Buttifant, D. Muscle onset can be improved by therapeutic exercise: A systematic review. Phys. Ther. Sport 2011, 12, 199–209. [Google Scholar] [CrossRef]
- Struyf, F.; Nijs, J.; Baeyens, J.P.; Mottram, S.; Meeusen, R. Scapular positioning and movement in unimpaired shoulders, shoulder impingement syndrome, and glenohumeral instability. Scand. J. Med. Sci. Sport. 2011, 21, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.J.; Belangero, W.D.; Almeida, G.L. The effect of joint instability on latency and recruitment order of the shoulder muscles. J. Electromyogr. Kinesiol. 2007, 17, 167–175. [Google Scholar] [CrossRef]
- de Oliveira, F.C.L.; Bouyer, L.J.; Ager, A.L.; Roy, J.-S. Electromyographic analysis of rotator cuff muscles in patients with rotator cuff tendinopathy: A systematic review. J. Electromyogr. Kinesiol. 2017, 35, 100–114. [Google Scholar] [CrossRef] [PubMed]
- Ebaugh, D.D.; Spinelli, B.A. Scapulothoracic motion and muscle activity during the raising and lowering phases of an overhead reaching task. J. Electromyogr. Kinesiol. 2010, 20, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Mark Burden, A.; Lewis, S.E.; Willcox, E. The effect of manipulating root mean square window length and overlap on reliability, inter-individual variability, statistical significance and clinical relevance of electromyograms. Man. Ther. 2014, 19, 595–601. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Pre_Treatment | Post_ Treatment |
|---|---|---|
| Mean [SD] | ||
| Age [years] | 29.1 [5.5] | 28.4 [2.1] |
| Height [cm] | 178 [9.5] | 177 [3] |
| Weight [Kg] | 78.2 [8.7] | 79.1 [7.6] |
| Affected Side | % | |
| R | 83% | 87% |
| L | 17% | 13% |
| Physical Activity * | [n] | |
| 0–3 | 0 | 0 |
| 4–7 | 3 | 2 |
| 8–10 | 31 | 24 |
| Speed | Muscle | Flexion LOADED | Flexion UNLOADED | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Hedges’s g Effect Size | 95% CI Sup Lim | 95% CI Inf Lim | p-Value | Hedges’s g Effect Size | 95% CI Sup Lim | 95% CI Inf Lim | p-Value | ||
| Slow | UT | 1.97 | 243.58 | −96.73 | 0.01 | 3.08 | −30.74 | −424.60 | 0.37 |
| AD | 0.33 | −51.00 | −381.30 | 0.00 | 3.11 | −506.23 | −807.97 | 0.00 | |
| MD | −0.35 | 224.31 | −146.96 | 0.07 | 0.35 | 41.59 | −294.28 | 0.53 | |
| PD | 0.44 | 372.24 | −507.82 | 0.68 | 0.62 | 399.07 | −172.41 | 0.33 | |
| LT | 0.20 | 293.93 | −384.34 | 0.72 | 0.92 | 164.51 | −304.01 | 0.58 | |
| SA | −0.73 | 236.14 | −812.27 | 0.05 | 0.16 | 44.61 | −455.55 | 0.43 | |
| Pec | −0.05 | 243.94 | −375.96 | 0.11 | 5.75 | −485.13 | −896.82 | 0.07 | |
| Subsc | 0.51 | 306.96 | −222.74 | 0.79 | 1.08 | 9.89 | −423.90 | 0.45 | |
| SS | 0.38 | 500.48 | −471.55 | 0.18 | 0.72 | −638.30 | −960.74 | 0.18 | |
| IF | −0.69 | −117.60 | 0.38 | 0.34 | 2.85 | 125.11 | −755.86 | 0.07 | |
| Medium | UT | 0.06 | −191.31 | −475.17 | 0.26 | 3.38 | −330.17 | −626.43 | 0.00 |
| AD | −0.39 | −457.93 | −691.93 | 0.21 | 5.94 | −657.01 | −865.40 | 0.00 | |
| MD | −0.53 | 69.68 | −195.54 | 0.00 | 0.40 | −250.48 | −450.86 | 0.44 | |
| PD | 0.62 | 407.07 | 64.14 | 0.02 | 2.73 | 267.85 | −141.67 | 0.44 | |
| LT | 0.36 | 164.40 | −220.02 | 0.02 | 0.16 | −35.26 | −468.21 | 0.65 | |
| SA | 0.12 | 135.42 | −308.99 | 0.65 | 0.47 | 3.59 | −415.05 | 0.88 | |
| Pec | −0.60 | −74.37 | −435.43 | 0.05 | 1.43 | −176.90 | −590.82 | 0.06 | |
| Subsc | −0.37 | 204.64 | −485.64 | 0.11 | 1.23 | −295.80 | −815.91 | 0.40 | |
| SS | 0.39 | 415.42 | −124.71 | 0.22 | 3.59 | 262.48 | −440.58 | 0.59 | |
| IF | 1.93 | 634.81 | −73.13 | 0.78 | 0.07 | 113.23 | −585.61 | 0.91 | |
| Fast | UT | −0.11 | −133.38 | −333.97 | 0.59 | 4.62 | −191.86 | −457.84 | 0.00 |
| AD | 0.20 | −217.80 | −413.58 | 0.59 | 0.68 | −319.26 | −543.20 | 0.09 | |
| MD | 0.92 | 45.96 | −136.59 | 0.20 | 0.14 | −109.47 | −338.57 | 0.39 | |
| PD | 0.85 | 421.60 | 145.51 | 0.53 | 2.00 | 346.78 | 58.02 | 0.05 | |
| LT | −0.55 | 21.82 | −261.87 | 0.69 | 0.48 | −30.66 | −318.45 | 0.72 | |
| SA | 0.12 | −64.88 | −267.09 | 0.86 | 0.06 | −110.84 | −385.73 | 0.90 | |
| Pec | −0.38 | −45.61 | −358.90 | 0.05 | 1.15 | −135.25 | −465.33 | 0.79 | |
| Subsc | 0.77 | 329.02 | −219.99 | 0.59 | 1.15 | 24.74 | −610.74 | 0.18 | |
| SS | 2.03 | 614.74 | 213.51 | 0.14 | 2.60 | 240.71 | −399.26 | 0.65 | |
| IF | 1.51 | 634.52 | 210.54 | 0.76 | 0.18 | −28.50 | −636.61 | 0.56 | |
| Speed | Muscle | Scaption LOADED | Scaption UNLOADED | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Hedges’s g Effect Size | 95% CI Sup Lim | 95% CI Inf Lim | p-Value | Hedges’s g Effect Size | 95% CI Sup Lim | 95% CI Inf Lim | p-Value | ||
| Slow | UT | 0.60 | −81.23 | −468.09 | 0.03 | 0.31 | −186.93 | −513.17 | 0.74 |
| AD | 0.04 | −133.55 | −465.09 | 0.00 | 5.40 | −615.21 | −823.03 | 0.77 | |
| MD | 0.22 | 155.91 | −203.27 | 0.00 | 5.85 | −198.25 | −499.14 | 0.01 | |
| PD | 0.67 | 412.94 | −65.66 | 0.05 | 0.48 | 443.25 | 1.34 | 0.11 | |
| LT | −0.23 | 0.77 | −440.89 | 0.66 | 0.39 | 36.29 | −410.56 | 0.88 | |
| SA | −0.19 | −212.7 | 531.7 | 0.75 | 0.05 | −10.31 | −429.51 | 0.46 | |
| Pec | 0.28 | 226.47 | −297.15 | 0.12 | 0.43 | 174.11 | −250.25 | 0.78 | |
| Subsc | 0.37 | 251.52 | −512.41 | 0.35 | 0.46 | −219.16 | −719.62 | 0.89 | |
| SS | 0.34 | 450.91 | −171.47 | 0.65 | 7.59 | 520.09 | −636.19 | 0.89 | |
| IF | 0.26 | 550.06 | −735.56 | 0.56 | 1.27 | 285.45 | −788.83 | 0.09 | |
| Medium | UT | −0.82 | −238.30 | −476.33 | 0.10 | 1.41 | −418.91 | −700.89 | 0.00 |
| AD | −1.09 | −387.98 | −610.87 | 0.99 | 2.24 | −604.29 | −793.14 | 0.00 | |
| MD | −1.30 | −117.75 | −382.60 | 0.00 | 0.64 | −382.35 | −645.01 | 0.19 | |
| PD | 0.58 | 399.19 | 62.49 | 0.00 | 0.85 | 277.01 | −90.69 | 0.72 | |
| LT | 0.00 | −3.80 | −405.18 | 0.72 | 0.50 | −45.79 | −453.84 | 0.33 | |
| SA | 0.57 | −65.3 | −404.6 | 0.30 | 0.47 | −97.70 | −471.59 | 0.16 | |
| Pec | 0.43 | 314.00 | −84.76 | 0.23 | 0.15 | −19.23 | −402.52 | 0.37 | |
| Subsc | −0.35 | 236.92 | −574.35 | 0.72 | 0.23 | 203.98 | −550.98 | 0.87 | |
| SS | −0.89 | 149.30 | −762.87 | −0.55 | |||||
| IF | 0.24 | 437.49 | −224.71 | 0.18 | 0.09 | 71.81 | −723.41 | 0.65 | |
| Fast | UT | 0.18 | −33.49 | −295.51 | 0.64 | 5.22 | −263.87 | −472.63 | 0.00 |
| AD | 1.09 | −28.20 | −299.16 | 0.89 | 8.06 | −379.26 | −608.43 | 0.52 | |
| MD | 1.10 | 25.62 | −254.84 | 0.91 | 4.94 | −262.05 | −484.09 | 0.05 | |
| PD | 0.32 | 338.62 | 39.16 | 0.83 | 1.66 | −21.38 | −295.84 | 0.66 | |
| LT | 0.00 | 77.69 | −254.02 | 1.00 | 1.35 | −105.10 | −425.37 | 0.07 | |
| SA | 0.14 | 119.7 | −331.1 | 1.00 | 0.42 | 0.37 | −329.44 | 0.02 | |
| Pec | 0.03 | 277.43 | −7.34 | 0.35 | 1.07 | −34.64 | −348.51 | 0.21 | |
| Subsc | 0.35 | 211.24 | −438.56 | 0.65 | 0.16 | 220.14 | −236.64 | 0.69 | |
| SS | 0.79 | 375.25 | −15.59 | 0.08 | 0.01 | 387.78 | −144.20 | 0.24 | |
| IF | 1.91 | 681.00 | 242.95 | −0.61 | |||||
| Speed | Muscle | Abduction LOADED | Abduction UNLOADED | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Hedges’s g Effect Size | 95% CI Sup Lim | 95% CI Inf Lim | p-Value | Hedges’s g Effect Size | 95% CI Sup Lim | 95% CI Inf Lim | p-Value | ||
| Slow | UT | −0.74 | 81.61 | −281.80 | 0.18 | 0.38 | −166.55 | −562.20 | 0.02 |
| AD | −0.34 | −460.94 | −725.36 | 0.00 | −0.04 | −94.91 | −406.38 | 0.37 | |
| MD | 0.35 | −196.33 | −528.36 | 0.01 | 0.87 | −427.25 | −703.21 | 0.02 | |
| PD | −0.24 | 155.77 | −320.73 | 0.98 | 2.33 | −60.46 | −440.32 | 0.69 | |
| LT | 0.00 | 93.61 | −538.11 | 0.92 | 1.56 | 247.04 | −228.33 | 1.00 | |
| SA | 0.60 | −36.8 | 477.7 | 0.22 | 0.75 | −55.81 | −458.80 | 0.39 | |
| Pec | −0.92 | −107.60 | −726.33 | 0.13 | −0.19 | 345.71 | −270.93 | 0.21 | |
| Subsc | −0.34 | −0.05 | −752.03 | 0.11 | 1.08 | 300.60 | −260.25 | 0.60 | |
| SS | −0.61 | −52.37 | −833.87 | 0.11 | 8.02 | 112.64 | −671.91 | 0.65 | |
| IF | 3.05 | 247.2 | −261.9 | 0.09 | |||||
| Medium | UT | 0.46 | −126.72 | −403.28 | 0.44 | 0.01 | −397.59 | −662.30 | 0.04 |
| AD | −0.86 | −517.35 | −754.55 | 0.00 | 1.37 | −240.20 | −489.40 | 0.01 | |
| MD | −1.18 | −308.06 | −557.18 | 0.09 | −0.19 | −497.22 | −744.51 | 0.01 | |
| PD | −0.67 | −60.95 | −391.66 | 0.05 | 0.63 | −118.99 | −448.76 | 0.02 | |
| LT | 0.00 | 158.87 | −324.17 | 0.01 | 0.06 | 243.00 | −159.20 | 0.36 | |
| SA | 0.27 | 80.4 | 554.1 | 0.42 | 0.08 | −35.62 | −429.65 | 0.30 | |
| Pec | 0.39 | 315.75 | −110.53 | 0.06 | −0.35 | 328.09 | −236.08 | 0.08 | |
| Subsc | −0.12 | 195.30 | −497.48 | 1.00 | 0.06 | 296.63 | −394.43 | 0.59 | |
| SS | 0.76 | 297.10 | −404.20 | 0.14 | 4.11 | 297.10 | −404.20 | 0.67 | |
| IF | |||||||||
| Fast | UT | −0.61 | −124.09 | −332.30 | 0.28 | 1.62 | −124.69 | −385.77 | 0.43 |
| AD | −0.70 | −119.55 | −364.55 | 0.00 | −0.74 | −79.90 | −251.20 | 0.04 | |
| MD | 0.01 | −99.16 | −333.90 | 0.04 | 1.48 | −148.94 | −363.17 | 0.69 | |
| PD | −0.31 | 15.38 | −261.90 | 0.93 | 0.21 | −3.95 | −271.96 | 0.57 | |
| LT | 0.00 | 116.06 | −290.59 | 0.17 | 1.14 | 216.20 | −0.04 | 0.92 | |
| SA | 0.22 | 15.4 | −261.9 | 0.88 | 0.81 | 195.40 | −118.82 | 0.03 | |
| Pec | 0.55 | 444.55 | 95.92 | 0.50 | 0.45 | 315.09 | −123.54 | 0.47 | |
| Subsc | 0.74 | 298.86 | −215.43 | 0.59 | 0.03 | 158.55 | −342.04 | 0.72 | |
| SS | 3.04 | 340.88 | 13.58 | 0.12 | 1.19 | 414.72 | −194.27 | 0.89 | |
| IF | 0.16 | 277.57 | −582.88 | 0.35 | |||||
| Descriptive Data Physical Outcome Measures | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Condition | n | Mean | SD | Variance | 95% IC Sup Lim | 95% IC Inf Inf | p-Value | Hedges’s g Effect Size |
| ROM IR | Pre_T | 34 | 33.03 | 13.03 | 26.1 | 39.3 | 169.8 | 0.00 | −0.61 |
| Post_T | 26 | 52.1 | 15.2 | 44.6 | 57.9 | 230.2 | |||
| ROM ER | Pre_T | 34 | 96.3 | 1.31 | 88.8 | 99.2 | 169.4 | 0.00 | −0.33 |
| Post_T | 26 | 104.5 | 7.7 | 101.2 | 108.1 | 58.9 | |||
| ROM IR 90°Flex | Pre_T | 34 | 23.5 | 9.2 | 18.7 | 28.1 | 84.9 | 0.00 | −0.50 |
| Post_T | 26 | 38.5 | 17.9 | 30.4 | 46.6 | 320.1 | |||
| S Kg ER | Pre_T | 34 | 10.6 | 3.0 | 9.7 | 12.5 | 9.0 | 0.00 | −0.51 |
| Post_T | 26 | 17.2 | 2.4 | 16.1 | 18.2 | 5.7 | |||
| S Kg IR | Pre_T | 34 | 18.4 | 4.8 | 17.2 | 21.4 | 22.7 | 0.00 | −1.06 |
| Post_T | 26 | 23.6 | 4.2 | 21.8 | 25.6 | 17.9 | |||
| PSFS | Pre_T | 34 | 21 | 5.9 | 18.3 | 23.5 | 35.9 | 0.00 | −1.84 |
| Post_T | 26 | 44.1 | 5.0 | 41.7 | 46.1 | 25.3 | |||
| NRS | Pre_T | 34 | 6.7 | 1 | 6.3 | 7.3 | 1.2 | 0.00 | 2.23 |
| Post_T | 26 | 1.4 | 1.2 | 0.9 | 2.0 | 1.5 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega-Cebrián, S.; Girabent-Farrés, M.; Whiteley, R.; Bagur-Calafat, C. Physiotherapy Rehabilitation in Subjects Diagnosed with Subacromial Impingement Syndrome Does Not Normalize Periscapular and Rotator Cuff Muscle Onset Time of Activation. Int. J. Environ. Res. Public Health 2021, 18, 8952. https://doi.org/10.3390/ijerph18178952
Ortega-Cebrián S, Girabent-Farrés M, Whiteley R, Bagur-Calafat C. Physiotherapy Rehabilitation in Subjects Diagnosed with Subacromial Impingement Syndrome Does Not Normalize Periscapular and Rotator Cuff Muscle Onset Time of Activation. International Journal of Environmental Research and Public Health. 2021; 18(17):8952. https://doi.org/10.3390/ijerph18178952
Chicago/Turabian StyleOrtega-Cebrián, Silvia, Monserrat Girabent-Farrés, Rodney Whiteley, and Caritat Bagur-Calafat. 2021. "Physiotherapy Rehabilitation in Subjects Diagnosed with Subacromial Impingement Syndrome Does Not Normalize Periscapular and Rotator Cuff Muscle Onset Time of Activation" International Journal of Environmental Research and Public Health 18, no. 17: 8952. https://doi.org/10.3390/ijerph18178952