
Four Decades of COPD Mortality Trends: Analysis of Trends and Multiple Causes of Death

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Statistical Analysis
- (a)
- Assessment of mortality with COPD as underlying cause of death.
- (b)
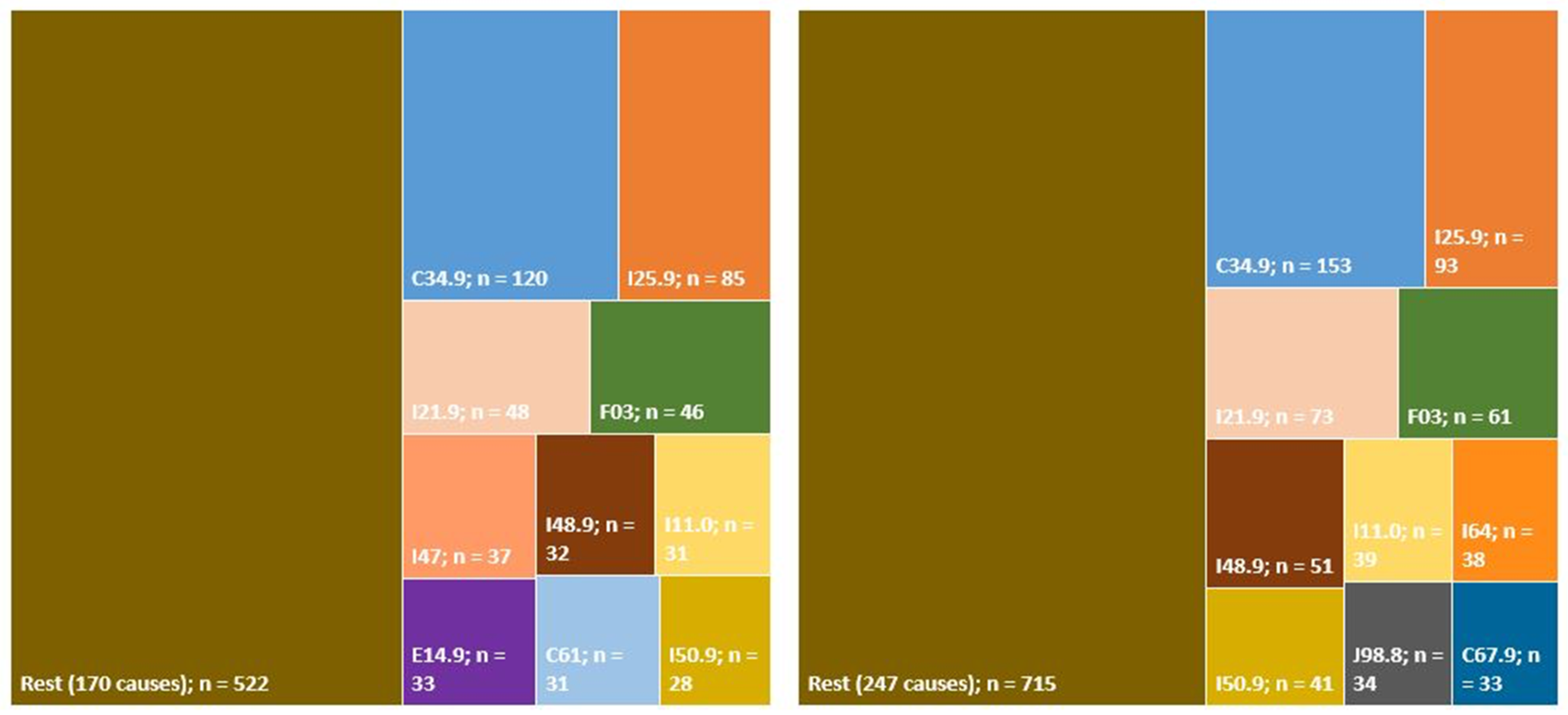
- Analysis of multiple causes of mortality due to COPD as a contributing cause of death.
- (c)
- Analysis of trends.
3. Results
3.1. COPD Mortality Trend: Period 1980–2017
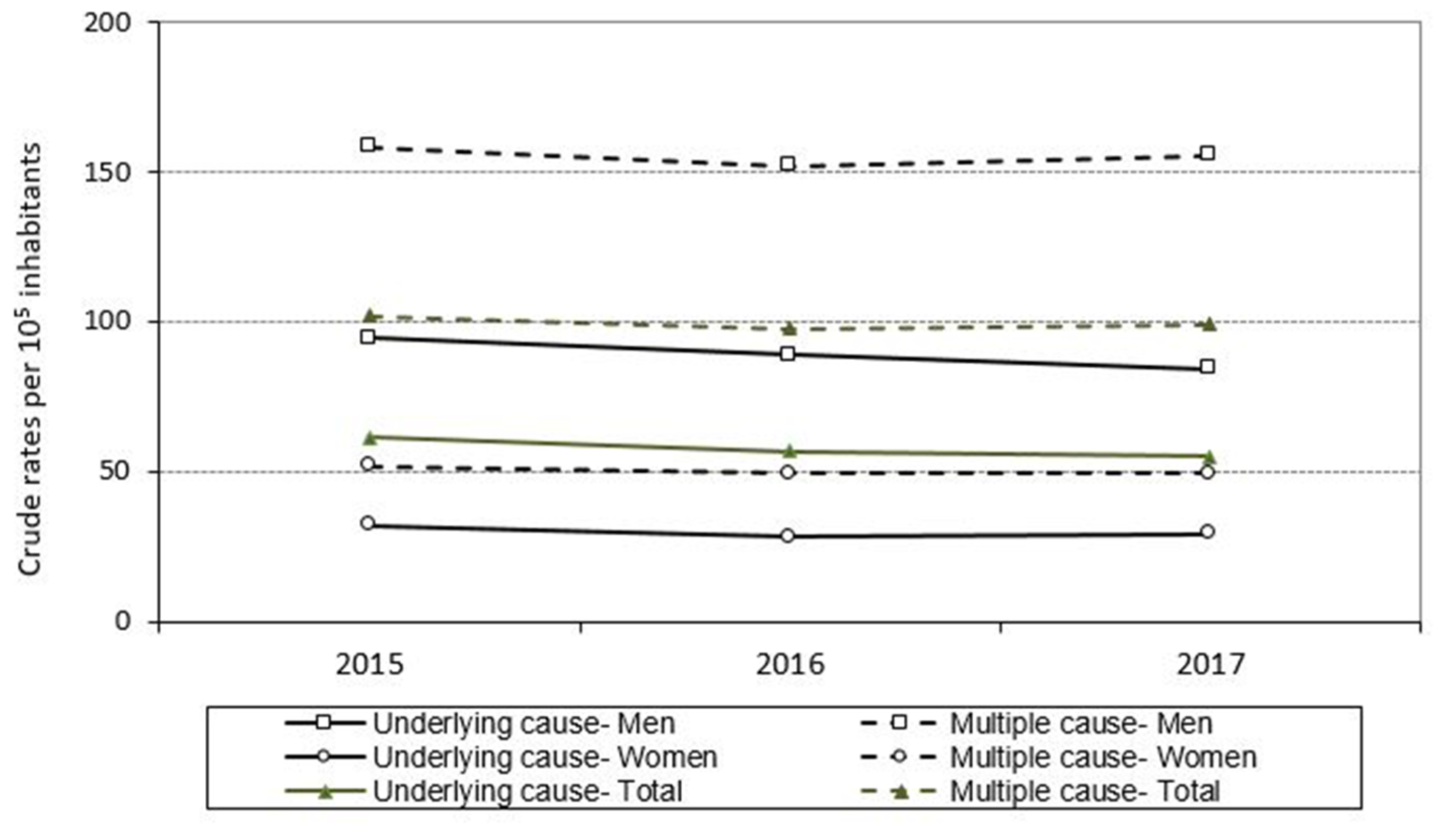
3.2. Trend in Mortality Due to COPD and with COPD: Period 2015–2017
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Working Group of the GesEPOC. Clinical Practice Guideline for the Diagnosis and Treatment of Patients with Chronic Obstructive Pulmonary disease (COPD)-The Spanish COPD Guideline (GesEPOC). Arch. Bronconeumol. 2017, 53 (Suppl. 1), 1–64. [Google Scholar]
- 2020 GOLD Report. Global Strategy for Prevention, Diagnosis and Management of COPD. Available online: https://goldcopd.org (accessed on 20 December 2020).
- Soriano, J.B.; Alfageme, I.; Miravitlles, M.; de Lucas, P.; Soler-Cataluña, J.J.; García-Río, F.; Casanova, C.; Rodríguez González-Moro, J.M.; Cosío, B.G.; Sánchez, G.; et al. Prevalence and Determinants of COPD in Spain: EPISCAN II. Arch. Bronconeumol. 2021, 57, 61–69, Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef] [Green Version]
- López-Campos, J.L.; Ruiz-Ramos, M.; Soriano, J.B. Mortality trends in chronic obstructive pulmonary disease in Europe, 1994–2010: A joinpoint regression analysis. Lancet Respir. Med. 2014, 2, 54–62. [Google Scholar] [CrossRef]
- Lortet-Tieulent, J.; Soerjomataram, I.; López-Campos, J.L.; Ancochea, J.; Coebergh, J.W.; Soriano, J.B. International trends in COPD mortality, 1995–2017. Eur. Respir. J. 2019, 54, 1901791. [Google Scholar] [CrossRef] [PubMed]
- López-Campos, J.L.; Ruiz-Ramos, M.; Soriano, J.B. COPD mortality rates in Andalusia, Spain, 1975–2010: A joinpoint regression analysis. Int. J. Tuberc. Lung Dis. 2013, 17, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Estadística de Mortalidad Según Causas Multiples. Instituto de Estadística de la Comunidad de Madrid. Available online: http://www.madrid.org/iestadis/fijas/estructu/demograficas/mnp/descarga/mor06_1.pdf (accessed on 15 September 2020).
- Obi, J.; Mehari, A.; Gillum, R. Mortality Related to Chronic Obstructive Pulmonary Disease and Co-morbidities in the United States, A Multiple Causes of Death Analysis. COPD J. Chronic Obstr. Pulm. Dis. 2018, 15, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.B.; Wise, R.A.; John, M.; Zvarich, M.T.; McGarvey, L.P. Accuracy of death certificates in COPD: Analysis from the TORCH trial. COPD J. Chronic Obstr. Pulm. Dis. 2010, 7, 179–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- May, K.L. Death certificates in asthma and COPD patients (survey of statistical data in Warsaw). Monaldi. Arch. Chest Dis. 2002, 57, 253–257. [Google Scholar] [PubMed]
- Marcon, A.; Saugo, M.; Fedeli, U. COPD-Related Mortality and Co-morbidities in Northeastern Italy, 2008–2012: A Multiple Causes of Death Analysis. COPD J. Chronic Obstr. Pulm. Dis. 2016, 13, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Represas Represas, C.; Ruano Raviña, A.; Fernández Villar, A. Changes in chronic obstructive pulmonary disease mortality trends: Fact or fiction? Arch. Bronconeumol. 2014, 50, 311–312. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation test for joinpoint regression with applications to cancer rates. Statist. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Joinpoint Regression Program. Version 4.0.4. May 2013; Statistical Research and Applications Branch, National Cancer Institute. Available online: http://surveillance.cancer.gov/joinpoint (accessed on 20 June 2020).
- Almagro, P.; Salvadó, M.; Garcia-Vidal, C.; Rodriguez-Carballeira, M.; Delgado, M.; Barreiro, B.; Heredia, J.L.; Soriano, J.B. Recent improvement in long-term survival after a COPD hospitalisation. Thorax 2010, 65, 298–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartl, S.; Lopez-Campos, J.L.; Pozo-Rodriguez, F.; Castro-Acosta, A.; Studnicka, M.; Kaiser, B.; Roberts, C.M. Risk of death and readmission of hospital-admitted COPD exacerbations: European COPD Audit. Eur. Respir. J. 2016, 47, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Cano-Serral, G.; Perez, G.; Borrell, C.; COMPARA Group. Comparability between ICD-9 and ICD-10 for the leading causes of death in Spain. Rev. Epidemiol. Sante Publique 2006, 54, 355–365. [Google Scholar] [CrossRef]
- Salmeron, D.; Cirera, L.; Saez, M.; Navarro, C. Influence of the introduction of the ICD-10 on tendencies of mortality by causes (1980–2004). Gac. Sanit. 2009, 23, 144–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celli, B.R.; Wedzicha, J.A. Update on Clinical Aspects of Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2019, 381, 1257–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soriano, J.B.; Ancochea, J.; Celli, B.R. The most beautiful COPD chart in the world: All together to end COPD. Eur. Respir. J. 2019, 54, 1902047. [Google Scholar] [CrossRef] [PubMed]
- Fernández-García, S.; Represas-Represas, C.; Ruano-Raviña, A.; Mouronte-Roibás, C.; Botana-Rial, M.; Ramos-Hernández, C.; Fernández-Villar, A. Social and clinical predictors of short- and long-term readmission after a severe exacerbation of COPD. PLoS ONE 2020, 15, e0229257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno, A.; Montón, C.; Belmonte, Y.; Gallego, M.; Pomares, X.; Real, J. Causes of death and risk factors for mortality in patients with severe chronic obstructive pulmonary disease. Arch. Bronconeumol. 2009, 45, 181–186. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Men | Women | Total | |||
|---|---|---|---|---|---|
| Number of deaths | 1980–1989 | 5740 | 2609 | 8349 | |
| 1990–1999 | 9289 | 4028 | 13,317 | ||
| 2000–2009 | 8823 | 3633 | 12,456 | ||
| 2010–2017 | 6531 | 2581 | 9112 | ||
| Total | 30,383 | 12,851 | 43,234 | ||
| Age | Mean | 1980–1989 | 76.0 | 79.6 | 77.1 |
| 1990–1999 | 78.2 | 82.7 | 79.5 | ||
| 2000–2009 | 80.7 | 85.5 | 82.1 | ||
| 2010–2017 | 82.3 | 87.0 | 83.6 | ||
| Total | 79.4 | 83.7 | 80.7 | ||
| 25th percentile | 1980–1989 | 71 | 75 | 72 | |
| 1990–1999 | 72 | 78 | 74 | ||
| 2000–2009 | 76 | 81 | 77 | ||
| 2010–2017 | 78 | 83 | 79 | ||
| Total | 74 | 79 | 75 | ||
| 50th percentile | 1980–1989 | 77 | 81 | 78 | |
| 1990–1999 | 79 | 84 | 81 | ||
| 2000–2009 | 82 | 87 | 83 | ||
| 2010–2017 | 84 | 88 | 85 | ||
| Total | 81 | 85 | 82 | ||
| 75th percentile | 1980–1989 | 82 | 85.5 | 84 | |
| 1990–1999 | 85 | 88 | 86 | ||
| 2000–2009 | 87 | 91 | 88 | ||
| 2010–2017 | 89 | 92 | 90 | ||
| Total | 86 | 90 | 87 |
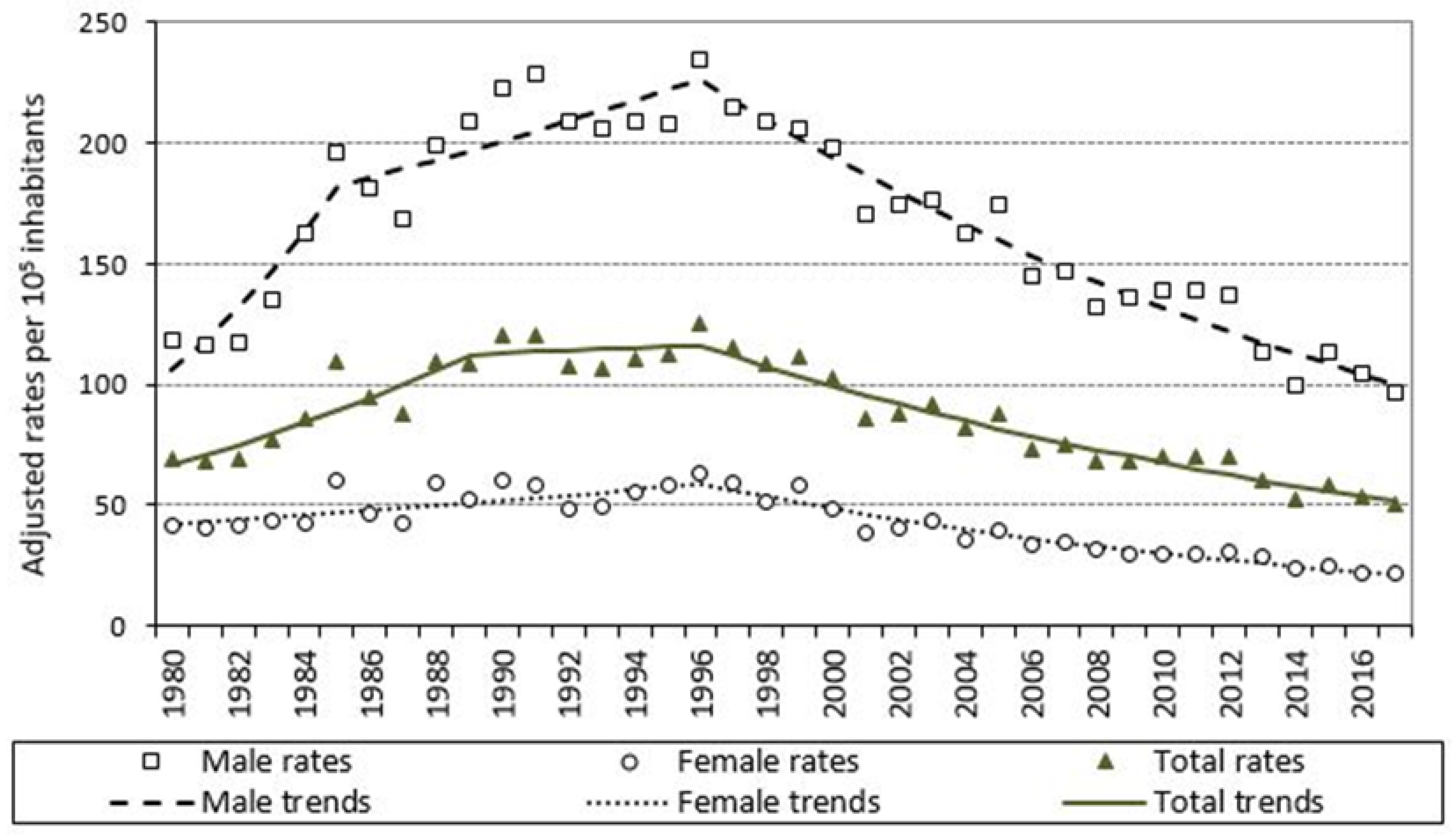
| Sex | Change Points (95% CI) | Period | APC (95% CI) | Interpretation | |
|---|---|---|---|---|---|
| 1980–1985 | 11.5 | (6.6; 16.6) | Rising | ||
| 1985 (1983; 1992) | |||||
| Men | 1985–1996 | 2.0 | (0.4; 3.6) | Rising | |
| 1996 (1992; 2006) | |||||
| 1996–2017 | −3.8 | (−4.3; −3.3) | Falling | ||
| 1980–1996 | 2.1 | (1.0; 3.2) | Rising | ||
| Women | 1996 (1993; 1998) | ||||
| 1996–2017 | −4.7 | (−5.4; −4.1) | Falling | ||
| 1980–1989 | 6.0 | (4.0; 8.0) | Rising | ||
| 1989 (1983; 1992) | |||||
| Total | 1989–1996 | 0.5 | (−3.0; 4.0) | Slightly rising | |
| 1996 (1993; 2002) | |||||
| 1996–2017 | −3.8 | (−4.3; −3.3) | Falling | ||
| Year | Deaths Due to COPD Considered as Underlying Cause | COPD Shown as Immediate or Intermediate Cause but Not as Underlying Cause | COPD Shown in Other Processes, but Not as Immediate, Intermediate, or Underlying Cause | Total |
|---|---|---|---|---|
| 2015 | 1135 | 310 | 447 | 1892 |
| 2016 | 1064 | 327 | 429 | 1820 |
| 2017 | 1028 | 376 | 455 | 1859 |
| Sum | 3227 | 1013 | 1331 | 5571 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-García, A.; Pérez-Ríos, M.; Fernández-Villar, A.; Naveira, G.; Candal-Pedreira, C.; Santiago-Pérez, M.I.; Represas-Represas, C.; Malvar-Pintos, A.; Cerdeira-Caramés, S.; Ruano-Raviña, A. Four Decades of COPD Mortality Trends: Analysis of Trends and Multiple Causes of Death. J. Clin. Med. 2021, 10, 1117. https://doi.org/10.3390/jcm10051117
Fernández-García A, Pérez-Ríos M, Fernández-Villar A, Naveira G, Candal-Pedreira C, Santiago-Pérez MI, Represas-Represas C, Malvar-Pintos A, Cerdeira-Caramés S, Ruano-Raviña A. Four Decades of COPD Mortality Trends: Analysis of Trends and Multiple Causes of Death. Journal of Clinical Medicine. 2021; 10(5):1117. https://doi.org/10.3390/jcm10051117
Chicago/Turabian StyleFernández-García, Alberto, Mónica Pérez-Ríos, Alberto Fernández-Villar, Gael Naveira, Cristina Candal-Pedreira, María Isolina Santiago-Pérez, Cristina Represas-Represas, Alberto Malvar-Pintos, Sara Cerdeira-Caramés, and Alberto Ruano-Raviña. 2021. "Four Decades of COPD Mortality Trends: Analysis of Trends and Multiple Causes of Death" Journal of Clinical Medicine 10, no. 5: 1117. https://doi.org/10.3390/jcm10051117