
Safety and Feasibility of MitraClip Implantation in Patients with Acute Mitral Regurgitation after Recent Myocardial Infarction and Severe Left Ventricle Dysfunction

 , , , , , , , , , , , , ,
, , , , , , , , , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Echocardiographic Evaluation
2.3. MitraClip
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Procedural and Safety Outcomes
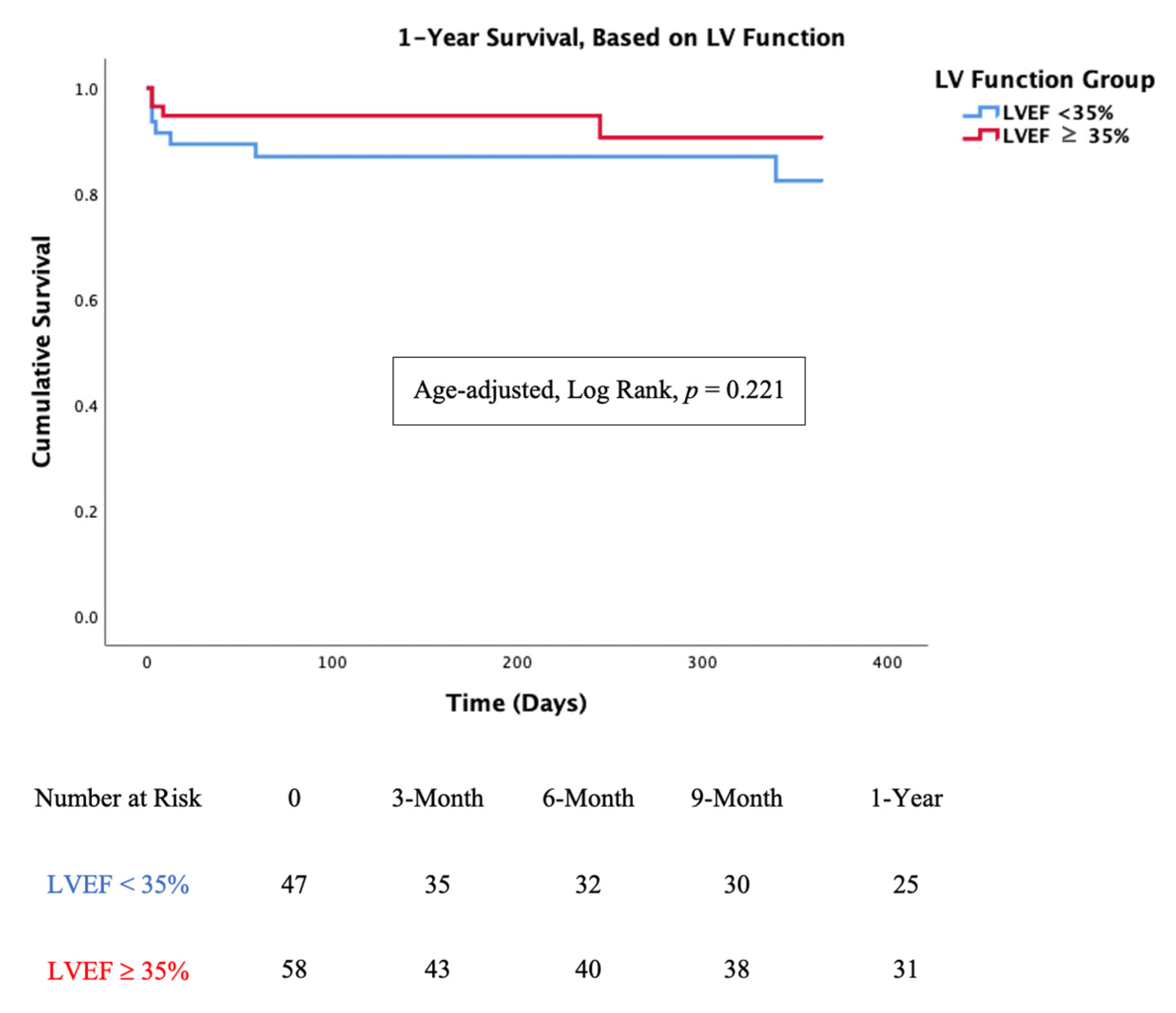
3.3. Mortality Analysis
3.4. Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhardwaj, B.; Sidhu, G.; Balla, S.; Kumar, V.; Kumar, A.; Aggarwal, K.; Dohrmann, M.L.; Alpert, M.A. Outcomes and Hospital Utilization in Patients with Papillary Muscle Rupture Associated with Acute Myocardial Infarction. Am. J. Cardiol. 2020, 125, 1020–1025. [Google Scholar] [CrossRef]
- Rossi, A.; Dini, F.L.; Faggiano, P.; Agricola, E.; Cicoira, M.; Frattini, S.; Simioniuc, A.; Gullace, M.; Ghio, S.; Enriquez-Sarano, M.; et al. Independent prognostic value of functional mitral regurgitation in patients with heart failure. A quantitative analysis of 1256 patients with ischaemic and non-ischaemic dilated cardiomyopathy. Heart 2011, 97, 1675–1680. [Google Scholar] [CrossRef] [PubMed]
- Grigioni, F.; Enriquez-Sarano, M.; Zehr, K.J.; Bailey, K.R.; Tajik, A.J. Ischemic mitral regurgitation: Long-term outcome and prognostic implications with quantitative Doppler assessment. Circulation 2001, 103, 1759–1764. [Google Scholar] [CrossRef] [Green Version]
- Maisano, F.; Franzen, O.; Baldus, S.; Schafer, U.; Hausleiter, J.; Butter, C.; Ussia, G.P.; Sievert, H.; Richardt, G.; Widder, J.D.; et al. Percutaneous mitral valve interventions in the real world: Early and 1-year results from the ACCESS-EU, a prospective, multicenter, nonrandomized post-approval study of the MitraClip therapy in Europe. J. Am. Coll. Cardiol. 2013, 62, 1052–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar]
- Geis, N.A.; Puls, M.; Lubos, E.; Zuern, C.S.; Franke, J.; Schueler, R.; von Bardeleben, R.S.; Boekstegers, P.; Ouarrak, T.; Zahn, R.; et al. Safety and efficacy of MitraClip therapy in patients with severely impaired left ventricular ejection fraction: Results from the German transcatheter mitral valve interventions (TRAMI) registry. Eur. J. Heart Fail. 2018, 20, 598–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalbacher, D.; Schafer, U.; RS, V.B.; Eggebrecht, H.; Sievert, H.; Nickenig, G.; Butter, C.; May, A.E.; Bekeredjian, R.; Ouarrak, T.; et al. Long-term outcome, survival and predictors of mortality after MitraClip therapy: Results from the German Transcatheter Mitral Valve Interventions (TRAMI) registry. Int. J. Cardiol. 2019, 277, 35–41. [Google Scholar] [CrossRef]
- Stone, G.W.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.; Grayburn, P.A.; Rinaldi, M.; Kapadia, S.R.; et al. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. N. Engl. J. Med. 2018, 379, 2307–2318. [Google Scholar] [CrossRef] [PubMed]
- Obadia, J.F.; Messika-Zeitoun, D.; Leurent, G.; Iung, B.; Bonnet, G.; Piriou, N.; Lefevre, T.; Piot, C.; Rouleau, F.; Carrie, D.; et al. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation. N. Engl. J. Med. 2018, 379, 2297–2306. [Google Scholar] [CrossRef] [PubMed]
- Pascual, I.; Benito-González, T.; Hernandez-Vaquero, D.; Estévez-Loureiro, R.; Lorca, R.; Garrote-Coloma, C.; Avanzas, P.; Gualis, J.; Adeba, A.; de Prado, A.P.; et al. Percutaneous treatment with Mitraclip for functional mitral regurgitation: Medium-term follow up according to left ventricular function. Ann. Transl. Med. 2020, 8, 959. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e72–e227. [Google Scholar]
- Pighi, M.; Estevez-Loureiro, R.; Maisano, F.; Ussia, G.P.; Dall’Ara, G.; Franzen, O.; Laroche, C.; Settergren, M.; Winter, R.; Nickenig, G.; et al. Immediate and 12-Month Outcomes of Ischemic Versus Nonischemic Functional Mitral Regurgitation in Patients Treated with MitraClip (from the 2011 to 2012 Pilot Sentinel Registry of Percutaneous Edge-To-Edge Mitral Valve Repair of the European Society of Cardiology). Am. J. Cardiol. 2017, 119, 630–637. [Google Scholar] [PubMed]
- Haberman, D.; Taramasso, M.; Czarnecki, A.; Kerner, A.; Chrissoheris, M.; Spargias, K.; Poles, L.; Agmon, Y.; Scianna, S.; Beeri, R.; et al. Salvage MitraClip in severe secondary mitral regurgitation complicating acute myocardial infarction: Data from a multicentre international study. Eur. J. Heart Fail. 2019, 21, 1161–1164. [Google Scholar] [CrossRef] [PubMed]
- Estevez-Loureiro, R.; Adamo, M.; Arzamendi, D.; Denti, P.; Freixa, X.; Nombela-Franco, L.; Pascual, I.; Melica, B.; Attias, D.; Serrador, A.; et al. Transcatheter mitral valve repair in patients with acute myocardial infarction: Insights from the European Registry of MitraClip in Acute Mitral Regurgitation following an acute myocardial infarction (EREMMI). Eurointerv. J. Eur. Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2020, 15, 1248–1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estévez-Loureiro, R.; Shuvy, M.; Taramasso, M.; Benito-Gonzalez, T.; Denti, P.; Arzamendi, D.; Adamo, M.; Freixa, X.; Villablanca, P.; Krivoshei, L.; et al. Use of MitraClip for mitral valve repair in patients with acute mitral regurgitation following acute myocardial infarction: Effect of cardiogenic shock on outcomes (IREMMI Registry). Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv. 2021. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [Green Version]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef]
- Stone, G.W.; Adams, D.H.; Abraham, W.T.; Kappetein, A.P.; Généreux, P.; Vranckx, P.; Mehran, R.; Kuck, K.H.; Leon, M.B.; Piazza, N.; et al. Clinical trial design principles and endpoint definitions for transcatheter mitral valve repair and replacement: Part 2: Endpoint definitions: A consensus document from the Mitral Valve Academic Research Consortium. Eur. Heart J. 2015, 36, 1878–1891. [Google Scholar] [CrossRef] [PubMed]
- Bursi, F.; Enriquez-Sarano, M.; Nkomo, V.T.; Jacobsen, S.J.; Weston, S.A.; Meverden, R.A.; Roger, V.L. Heart failure and death after myocardial infarction in the community: The emerging role of mitral regurgitation. Circulation 2005, 111, 295–301. [Google Scholar] [CrossRef] [Green Version]
- Hillis, G.S.; Moller, J.E.; Pellikka, P.A.; Bell, M.R.; Casaclang-Verzosa, G.C.; Oh, J.K. Prognostic significance of echocardiographically defined mitral regurgitation early after acute myocardial infarction. Am. Heart J. 2005, 150, 1268–1275. [Google Scholar] [CrossRef]
- Nishino, S.; Watanabe, N.; Kimura, T.; Enriquez-Sarano, M.; Nakama, T.; Furugen, M.; Koiwaya, H.; Ashikaga, K.; Kuriyama, N.; Shibata, Y. The Course of Ischemic Mitral Regurgitation in Acute Myocardial Infarction after Primary Percutaneous Coronary Intervention: From Emergency Room to Long-Term Follow-Up. Circ. Cardiovasc. Imaging 2016, 9, e004841. [Google Scholar] [CrossRef] [Green Version]
- Tcheng, J.E.; Jackman, J.D., Jr.; Nelson, C.L.; Gardner, L.H.; Smith, L.R.; Rankin, J.S.; Califf, R.M.; Stack, R.S. Outcome of patients sustaining acute ischemic mitral regurgitation during myocardial infarction. Ann. Intern. Med. 1992, 117, 18–24. [Google Scholar] [CrossRef]
- Valuckiene, Z.; Budrys, P.; Jurkevicius, R. Predicting ischemic mitral regurgitation in patients with acute ST-elevation myocardial infarction: Does time to reperfusion really matter and what is the role of collateral circulation? Int. J. Cardiol. 2016, 203, 667–671. [Google Scholar] [CrossRef] [Green Version]
- Dunlay, S.M.; Roger, V.L. Gender differences in the pathophysiology, clinical presentation, and outcomes of ischemic heart failure. Curr. Heart Fail. Rep. 2012, 9, 267–276. [Google Scholar] [CrossRef]
- Sutton, N.R.; Li, S.; Thomas, L.; Wang, T.Y.; de Lemos, J.A.; Enriquez, J.R.; Shah, R.U.; Fonarow, G.C. The association of left ventricular ejection fraction with clinical outcomes after myocardial infarction: Findings from the Acute Coronary Treatment and Intervention Outcomes Network (ACTION) Registry-Get with the Guidelines (GWTG) Medicare-linked database. Am. Heart J. 2016, 178, 65–73. [Google Scholar] [CrossRef]
- Gerber, Y.; Weston, S.A.; Enriquez-Sarano, M.; Berardi, C.; Chamberlain, A.M.; Manemann, S.M.; Jiang, R.; Dunlay, S.M.; Roger, V.L. Mortality Associated with Heart Failure after Myocardial Infarction: A Contemporary Community Perspective. Circ. Heart Fail. 2016, 9, e002460. [Google Scholar] [CrossRef] [Green Version]
- Funaro, S.; La Torre, G.; Madonna, M.; Galiuto, L.; Scara, A.; Labbadia, A.; Canali, E.; Mattatelli, A.; Fedele, F.; Alessandrini, F.; et al. Incidence, determinants, and prognostic value of reverse left ventricular remodelling after primary percutaneous coronary intervention: Results of the Acute Myocardial Infarction Contrast Imaging (AMICI) multicenter study. Eur. Heart J. 2009, 30, 566–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agricola, E.; Oppizzi, M.; Pisani, M.; Meris, A.; Maisano, F.; Margonato, A. Ischemic mitral regurgitation: Mechanisms and echocardiographic classification. Eur. J. Echocardiogr. 2008, 9, 207–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mentias, A.; Raza, M.Q.; Barakat, A.F.; Hill, E.; Youssef, D.; Krishnaswamy, A.; Desai, M.Y.; Griffin, B.; Ellis, S.; Menon, V.; et al. Outcomes of ischaemic mitral regurgitation in anterior versus inferior ST elevation myocardial infarction. Open Heart 2016, 3, e000493. [Google Scholar] [CrossRef]
- Chan, K.M.; Punjabi, P.P.; Flather, M.; Wage, R.; Symmonds, K.; Roussin, I.; Rahman-Haley, S.; Pennell, D.J.; Kilner, P.J.; Dreyfus, G.D.; et al. Coronary artery bypass surgery with or without mitral valve annuloplasty in moderate functional ischemic mitral regurgitation: Final results of the Randomized Ischemic Mitral Evaluation (RIME) trial. Circulation 2012, 126, 2502–2510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estevez-Loureiro, R.; Arzamendi, D.; Freixa, X.; Cardenal, R.; Carrasco-Chinchilla, F.; Serrador-Frutos, A.; Pan, M.; Sabate, M.; Diaz, J.; Hernandez, J.M.; et al. Percutaneous Mitral Valve Repair for Acute Mitral Regurgitation after an Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2015, 66, 91–92. [Google Scholar] [CrossRef] [PubMed]
- Wolff, R.; Cohen, G.; Peterson, C.; Wong, S.; Hockman, E.; Lo, J.; Strauss, B.H.; Cohen, E.A. MitraClip for papillary muscle rupture in patient with cardiogenic shock. Can. J. Cardiol. 2014, 30, 1461.e13–1461.e14. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Santamarta, M.; Estevez-Loureiro, R.; Gualis, J.; Alonso, D.; Perez de Prado, A.; Fernandez-Vazquez, F. Percutaneous mitral valve repair with MitraClip system in a patient with acute mitral regurgitation after myocardial infarction. Rev. Esp. Cardiol. 2015, 68, 259–261. [Google Scholar] [CrossRef] [PubMed]
- Adamo, M.; Curello, S.; Chiari, E.; Fiorina, C.; Chizzola, G.; Magatelli, M.; Locantore, E.; Cuminetti, G.; Lombardi, C.; Manzato, A.; et al. Percutaneous edge-to-edge mitral valve repair for the treatment of acute mitral regurgitation complicating myocardial infarction: A single centre experience. Int. J. Cardiol. 2017, 234, 53–57. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | 1 | 2 | |||
|---|---|---|---|---|---|
| Total Population | LVEF < 35% | LVEF ≥ 35% | p-Value | ||
| n | 105 | 47 | 58 | ||
| Demographics | |||||
| Age, years | 70.5 ± 10.3 | 68.4 ± 9.1 | 72.4 ± 11.0 | 0.05 | |
| Sex, Female, % (n) | 50 (53) | 43 (20) | 57 (33) | 0.17 | |
| BMI (Kg/M2) | 26.5 ± 5.2 | 27.9 ± 4.7 | 25.5 ± 5.3 | 0.04 | |
| Hypertension, % (n) | 70.5 (74) | 68.1 (32) | 70.7 (41) | 0.83 | |
| Diabetes, % (n) | 45.7 (48) | 51.1 (24) | 41.4 (24) | 0.33 | |
| Dyslipidemia, % (n) | 62.9 (66) | 70.0 (31) | 60.3 (35) | 0.69 | |
| COPD, % (n) | 17.1 (18) | 19.1 (9) | 15.5 (9) | 0.80 | |
| CKD ≥ grade 2, % (n) | 29.5 (31) | 25.5 (12) | 32.8 (19) | 0.82 | |
| Prior stroke, % (n) | 13.3 (14) | 6.4 (3) | 19.0 (11) | 0.08 | |
| Prior MI, % (n) | 55.2 (58) | 61.7 (29) | 50 (29( | 0.24 | |
| Prior CABG, % (n) | 26.7 (28) | 23.4 (11) | 29.3 (17) | 0.51 | |
| Euroscore 2, % | 17.2 ± 16.7 | 20.1 ± 18.5 | 14.9 ± 15.0 | 0.14 | |
| Presentation | |||||
| STEMI, % (n) | 71.4 (75) | 66.0 (31) | 75.9 (44) | 0.25 | |
| Killip Class 3+, % (n) | 68.6 (72) | 78.7 (37) | 60.3 (35) | 0.06 | |
| Echocardiographic | |||||
| MR Grade 4+, % (n) | 81.0 (85) | 83.0 (39) | 79.3 (46) | 0.80 | |
| Papillary muscle rapture, % (n) | 5.7 (6) | 2.1 (1) | 8.6 % (5) | 0.22 | |
| Ejection Fraction (%) | 35.8 ± 11.9 | 25.8 ± 5.7 | 44 ± 8.9 | <0.01 | |
| sPAP, mmHg | 53.6 ± 18.6 | 54.4 ± 16.1 | 53.1 ± 20.3 | 0.75 | |
| Coronary Angiography | |||||
| Multivessel disease, % (n) | 80 (84) | 83.0 (39) | 77.6 (45) | 0.63 | |
| Infarct Related Artery (IRA) | RCA, % (n) | 11 (5) | 41 (24) | <0.01 | |
| LCX, % (n) | 32 (15) | 33 (19) | |||
| LAD, % (n) | 53 (25) | 22 (13) | |||
| PCI, % (n) | 94.3 (99) | 95.7 (45) | 95.7 (54) | 0.69 | |
| Wall Involved | Anterior | 51 (24) | 19 (11) | <0.01 | |
| Inferior | 30 (14) | 59 (34) | |||
| Lateral and/or Posterior | 19 (9) | 22 (13) | |||
| ICCU Status and Treatment | |||||
| Cardiogenic Shock | 54.3 (57) | 63.8 (30) | 46.6 (27) | 0.12 | |
| Mechanical Ventilation | 42.9 (45) | 46.8 (22) | 39.7 (23) | 0.55 | |
| Vasoactive medication | 42.9 (45) | 48.9 (23) | 37.9 (22) | 0.32 | |
| Any MSD | 37.1 (39) | 42.6 (20) | 32.8 (19) | 0.32 | |
| Parameter | 1 | 2 | ||
|---|---|---|---|---|
| Total Population | LVEF < 35% | LVEF ≥ 35% | p-Value | |
| n | 105 | 47 | 58 | |
| Procedure | ||||
| Procedure Time, min | 115 ± 90 | 122 ± 84 | 109 ± 95 | 0.51 |
| Major Complications | 6.7 (7) | 8.5 (4) | 5.2 (3) | 0.70 |
| MI to Procedure, days | 27 ± 22 | 35 ± 26 | 20 ± 17 | <0.01 |
| Clips Implanted, mean | 1.7 ± 0.7 | 1.8 ± 0.7 | 1.6 ± 0.6 | 0.22 |
| MR > 2 at discharge, % (n) | 8.6 (9) | 8.5 (4) | 8.6 (5) | 1 |
| MV Gradient post | 3.7 ± 1.7 | 3.7 ± 1.6 | 3.7 ± 1.8 | 0.91 |
| Outcomes | ||||
| Procedure success | 91.4 (96) | 93.6 (44) | 89.7 (52) | 0.73 |
| In hospital mortality | 8.6 (9) | 10.6 (5) | 6.9 (4) | 0.51 |
| Major Complications | 6.7 (7) | 8.5 (4) | 5.2 (3) | 0.70 |
| Mortality at 3 months | 11.4 (12) | 14.9 (7) | 8.6 (5) | 0.50 |
| Rehospitalizations at 3 months | 13.3 (14) | 19.1 (9) | 15.5 (9) | 0.77 |
| 1-year mortality | 15.2 (16) | 19.1 (9) | 12.1 (7) | 0.49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haberman, D.; Estévez-Loureiro, R.; Benito-Gonzalez, T.; Denti, P.; Arzamendi, D.; Adamo, M.; Freixa, X.; Nombela-Franco, L.; Villablanca, P.; Krivoshei, L.; et al. Safety and Feasibility of MitraClip Implantation in Patients with Acute Mitral Regurgitation after Recent Myocardial Infarction and Severe Left Ventricle Dysfunction. J. Clin. Med. 2021, 10, 1819. https://doi.org/10.3390/jcm10091819
Haberman D, Estévez-Loureiro R, Benito-Gonzalez T, Denti P, Arzamendi D, Adamo M, Freixa X, Nombela-Franco L, Villablanca P, Krivoshei L, et al. Safety and Feasibility of MitraClip Implantation in Patients with Acute Mitral Regurgitation after Recent Myocardial Infarction and Severe Left Ventricle Dysfunction. Journal of Clinical Medicine. 2021; 10(9):1819. https://doi.org/10.3390/jcm10091819
Chicago/Turabian StyleHaberman, Dan, Rodrigo Estévez-Loureiro, Tomas Benito-Gonzalez, Paolo Denti, Dabit Arzamendi, Marianna Adamo, Xavier Freixa, Luis Nombela-Franco, Pedro Villablanca, Lian Krivoshei, and et al. 2021. "Safety and Feasibility of MitraClip Implantation in Patients with Acute Mitral Regurgitation after Recent Myocardial Infarction and Severe Left Ventricle Dysfunction" Journal of Clinical Medicine 10, no. 9: 1819. https://doi.org/10.3390/jcm10091819