
Inflammatory and Hypercoagulable Biomarkers and Clinical Outcomes in COVID-19 Patients

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
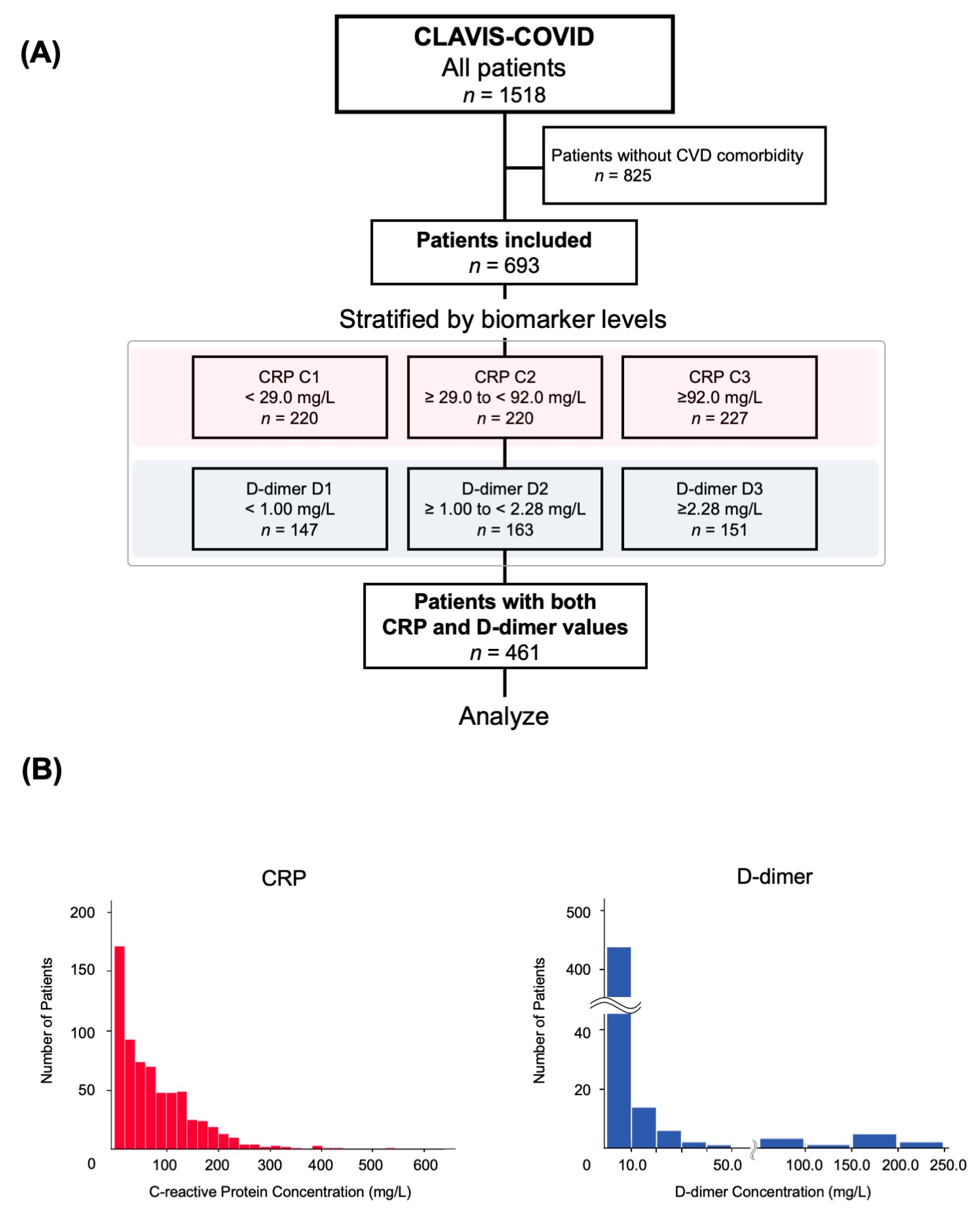
2.1. Study Design and Patient Population
2.2. Data Collection
2.3. Decision of Hospitalization and Discharge in Patients with COVID-19
2.4. Biomarker Measurement
2.5. Study Outcome
2.6. Statistical Analysis
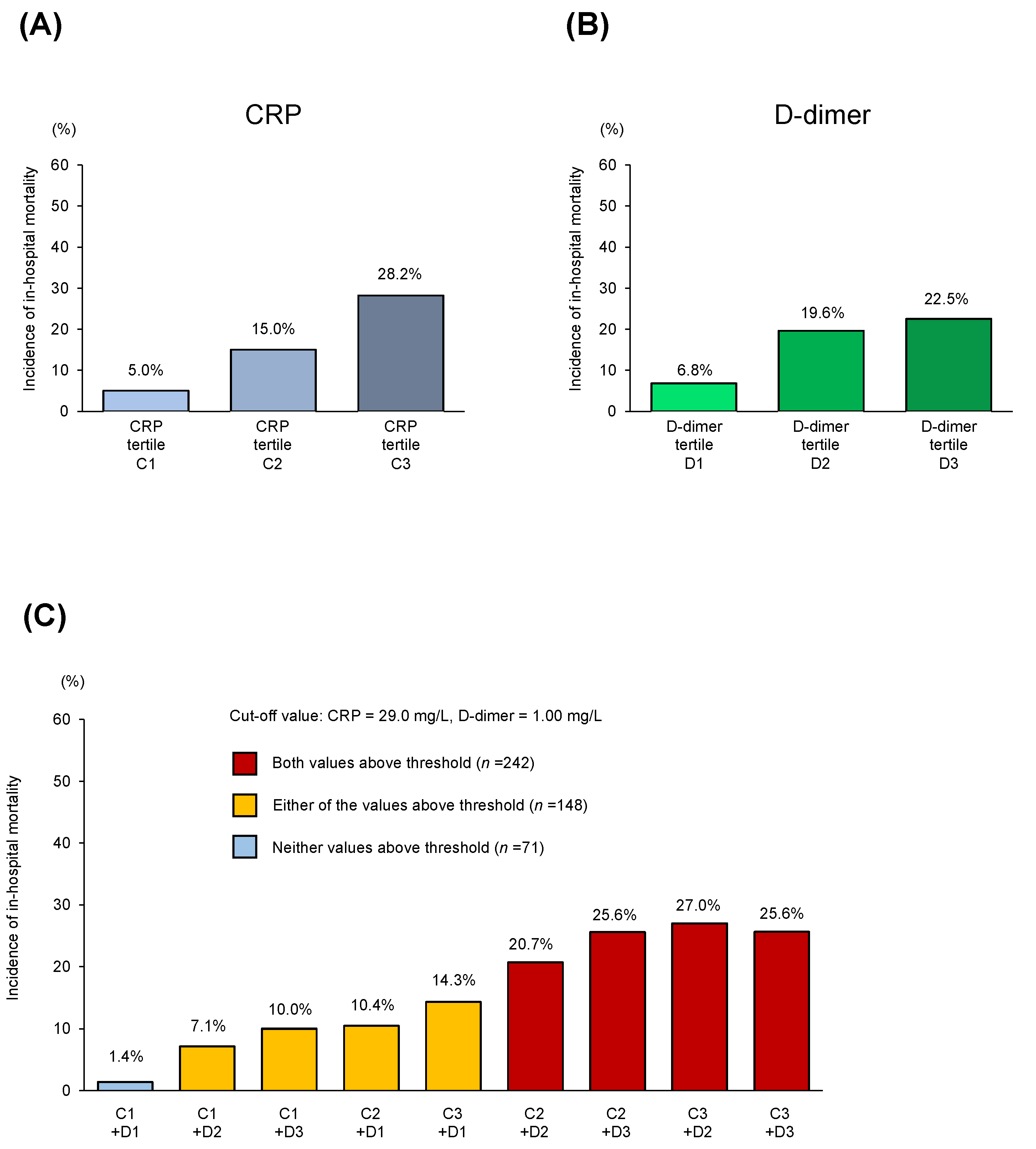
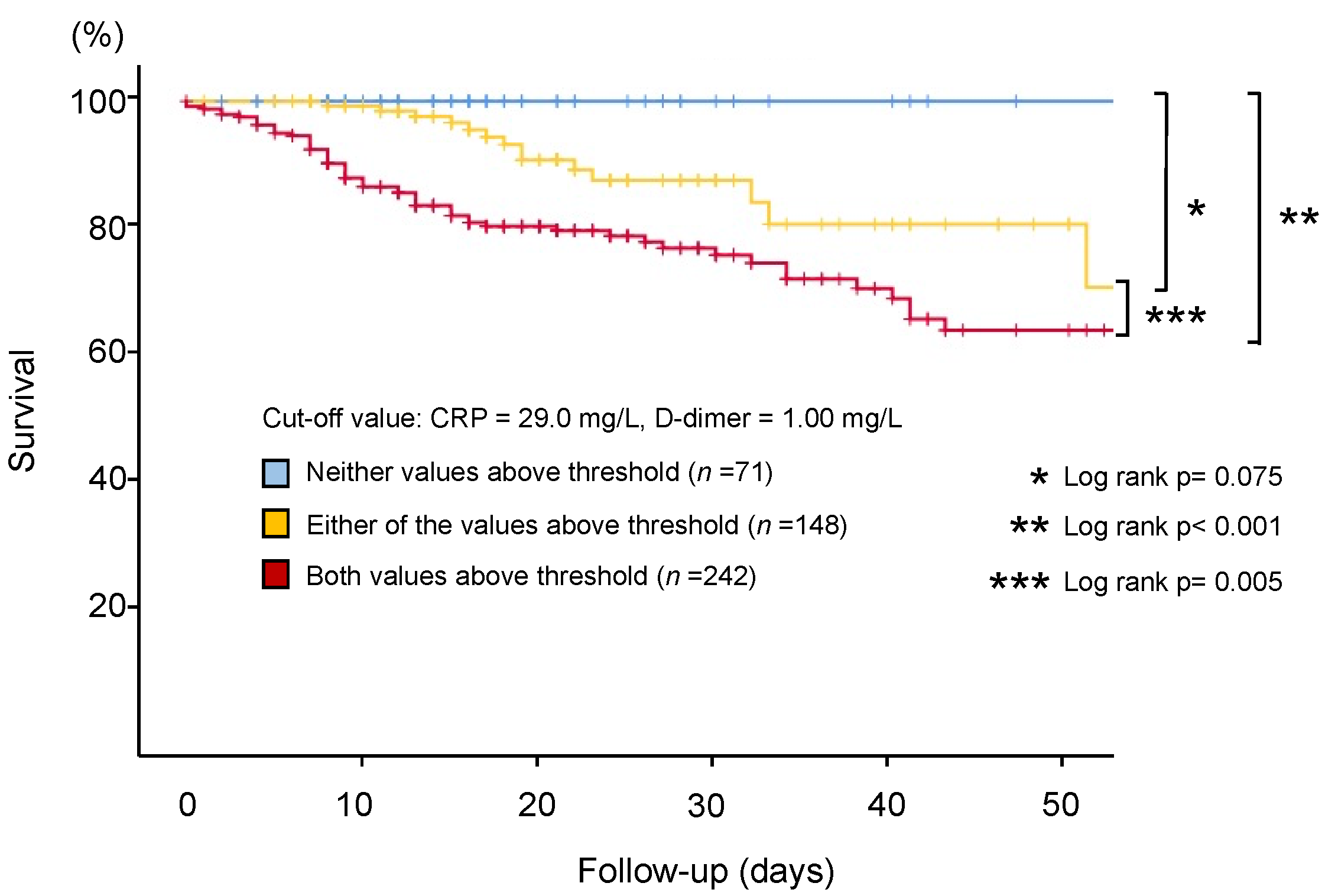
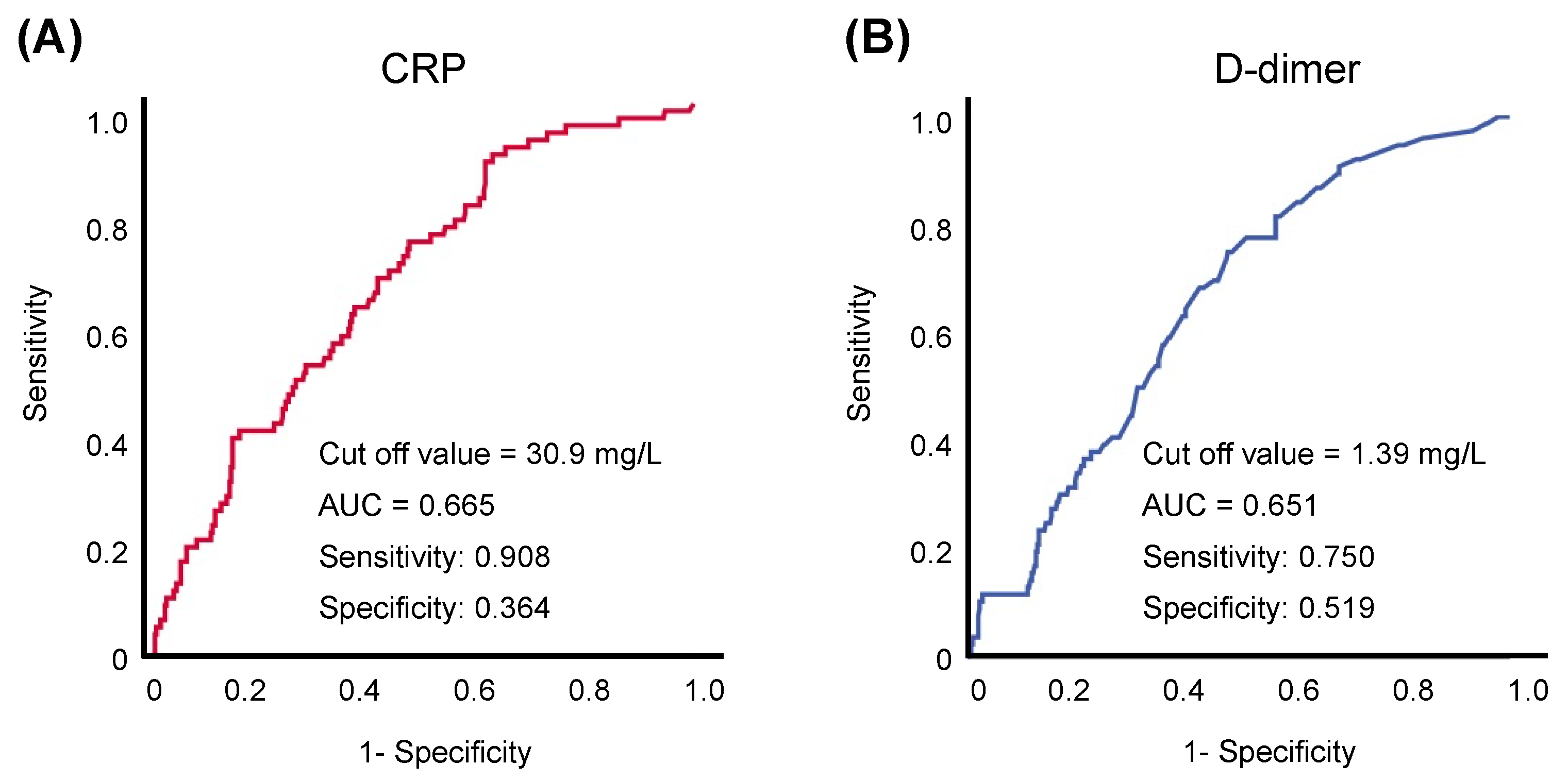
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 14 February 2021).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Li, X.; Guan, B.; Su, T.; Liu, W.; Chen, M.; Waleed, K.B.; Guan, X.; Gary, T.; Zhu, Z. Impact of cardiovascular disease and cardiac injury on in-hospital mortality in patients with COVID-19: A systematic review and meta-analysis. Heart 2020, 106, 1142–1147. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.; Kim, S.R.; Kim, M.N.; Shim, W.J.; Park, S.M. Impact of cardiovascular disease and risk factors on fatal outcomes in patients with COVID-19 according to age: A systematic review and meta-analysis. Heart 2021, 107, 373–380. [Google Scholar] [CrossRef]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients With Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury With Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [Green Version]
- Levi, M.; Thachil, J.; Iba, T.; Levy, J.H. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Haematol. 2020, 7, e438–e440. [Google Scholar] [CrossRef]
- Malik, P.; Patel, U.; Mehta, D.; Patel, N.; Kelkar, R.; Akrmah, M.; Gabrilove, J.L.; Sacks, H. Biomarkers and outcomes of COVID-19 hospitalisations: Systematic review and meta-analysis. BMJ Evid. Based Med. 2020, 3, 107–108. [Google Scholar] [CrossRef]
- Liu, F.; Li, L.; Xu, M.; Wu, J.; Luo, D.; Zhu, Y.; Li, B.; Song, X.; Zhou, X. Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. J. Clin. Virol. 2020, 127, 104370. [Google Scholar] [CrossRef]
- Luo, X.; Zhou, W.; Yan, X.; Guo, T.; Wang, B.; Xia, H.; Ye, L.; Xiong, J.; Jiang, Z.; Liu, Y.; et al. Prognostic Value of C-Reactive Protein in Patients With Coronavirus 2019. Clin. Infect. Dis. 2020, 71, 2174–2179. [Google Scholar] [CrossRef]
- Zhang, L.; Yan, X.; Fan, Q.; Liu, H.; Liu, X.; Liu, Z.; Zhang, Z. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J. Thromb. Haemost. 2020, 18, 1324–1329. [Google Scholar] [CrossRef]
- Matsumoto, S.; Kuroda, S.; Sano, T.; Kitai, T.; Yonetsu, T.; Kohsaka, S.; Torii, S.; Kishi, T.; Komuro, I.; Hirata, K.I.; et al. Clinical and Biomarker Profiles and Prognosis of Elderly Patients With Coronavirus Disease 2019 (COVID-19) With Cardiovascular Diseases and/or Risk Factors. Circ. J. 2021, 85, 921–928. [Google Scholar] [CrossRef]
- International Severe Acute Respiratory and emerging Infection Consortium. Clinical data collection: The COVID-19 case report forms (CRF). Available online: https://isaric.org/ (accessed on 1 December 2020).
- Ministry of Health, Labour and Welfare. Clinical management of patients with COVID-19 [in Japanese]. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000121431_00111.html (accessed on 1 June 2020).
- Daniels, J.M.; Schoorl, M.; Snijders, D.; Knol, D.L.; Lutter, R.; Jansen, H.M.; Boersma, W.G. Procalcitonin vs C-reactive protein as predictive markers of response to antibiotic therapy in acute exacerbations of COPD. Chest 2010, 138, 1108–1115. [Google Scholar] [CrossRef] [PubMed]
- Komiya, K.; Ishii, H.; Teramoto, S.; Takahashi, O.; Eshima, N.; Yamaguchi, O.; Ebi, N.; Murakami, J.; Yamamoto, H.; Kadota, J. Diagnostic utility of C-reactive protein combined with brain natriuretic peptide in acute pulmonary edema: A cross sectional study. Respir. Res. 2011, 12, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Zhang, G.; Zhang, J.; Wang, B.; Zhu, X.; Wang, Q.; Qiu, S. Analysis of clinical characteristics and laboratory findings of 95 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A retrospective analysis. Respir. Res. 2020, 21, 74. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Jaramillo, N.; Low, N.; Franco, O.H. The double burden of disease of COVID-19 in cardiovascular patients: Overlapping conditions could lead to overlapping treatments. Eur. J. Epidemiol. 2020, 35, 335–337. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Li, T.; Han, M.; Li, X.; Wu, D.; Xu, Y.; Zhu, Y.; Liu, Y.; Wang, X.; Wang, L. Diagnostic utility of clinical laboratory data determinations for patients with the severe COVID-19. J. Med. Virol. 2020, 92, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Levy, J.H.; Levi, M.; Connors, J.M.; Thachil, J. Coagulopathy of Coronavirus Disease 2019. Crit. Care Med. 2020, 48, 1358–1364. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Bansal, A.; Singh, A.D.; Jain, V.; Aggarwal, M.; Gupta, S.; Padappayil, R.P.; Nadeem, M.; Joshi, S.; Mian, A.; Greathouse, T.; et al. The association of D-dimers with mortality, intensive care unit admission or acute respiratory distress syndrome in patients hospitalized with coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. Heart Lung. 2021, 50, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk stratification of patients admitted to hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Development and validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Kunichoff, D.; Garshick, M.; Shah, B.; Pillinger, M.; Hochman, J.S.; Berger, J.S. C-reactive protein and clinical outcomes in patients with COVID-19. Eur. Heart J. 2021, 23, 2270–2279. [Google Scholar] [CrossRef] [PubMed]
- Teigell Muñoz, F.J.; García-Guijarro, E.; García-Domingo, P.; Pérez-Nieto, G.; Roque Rojas, F.; García-Peña, M.; Nieto Gallo, M.A.; Melero Bermejo, J.A.; de Guzman García-Monge, M.T.; Granizo, J.J. A safe protocol to identify low-risk patients with COVID-19 pneumonia for outpatient management. Intern Emerg. Med. 2021, 1–9. [Google Scholar]
- Yamamoto, N.; Bauer, G. Apparent difference in fatalities between Central Europe and East Asia due to SARS-COV-2 and COVID-19: Four hypotheses for possible explanation. Med. Hypotheses. 2020, 144, 110160. [Google Scholar] [CrossRef]
- Li, L.; Zhang, S.; He, B.; Chen, X.; Wang, S.; Zhao, Q. Risk factors and electrocardiogram characteristics for mortality in critical inpatients with COVID-19. Clin. Cardiol. 2020, 43, 1624–1630. [Google Scholar] [CrossRef]
- Goldstein, J.R.; Lee, R.D. Demographic perspectives on the mortality of COVID-19 and other epidemics. Proc. Natl. Acad. Sci. USA 2020, 117, 22035–22041. [Google Scholar] [CrossRef]
- Biamonte, F.; Botta, C.; Mazzitelli, M.; Rotundo, S.; Trecarichi, E.M.; Foti, D.; Torti, C.; Viglietto, G.; Torella, D.; Costanzo, F. Combined lymphocyte/monocyte count, D-dimer and iron status predict COVID-19 course and outcome in a long-term care facility. J. Transl. Med. 2021, 19, 79. [Google Scholar] [CrossRef] [PubMed]
- Manocha, K.K.; Kirzner, J.; Ying, X.; Yeo, I.; Peltzer, B.; Ang, B.; Li, H.A.; Lerman, B.B.; Safford, M.M.; Goyal, P.; et al. Troponin and Other Biomarker Levels and Outcomes Among Patients Hospitalized with COVID-19: Derivation and Validation of the HA(2)T(2) COVID-19 Mortality Risk Score. J. Am. Heart. Assoc. 2020, 6, e018477. [Google Scholar]
- Sharifpour, M.; Rangaraju, S.; Liu, M.; Alabyad, D.; Nahab, F.B.; Creel-Bulos, C.M.; Jabaley, C.S. C-Reactive protein as a prognostic indicator in hospitalized patients with COVID-19. PLoS ONE 2020, 15, e0242400. [Google Scholar] [CrossRef]
- Escadafal, C.; Incardona, S.; Fernandez-Carballo, B.L.; Dittrich, S. The good and the bad: Using C reactive protein to distinguish bacterial from non-bacterial infection among febrile patients in low-resource settings. BMJ Glob. Health 2020, 5, e002396. [Google Scholar] [CrossRef] [PubMed]
- Crawford, F.; Andras, A.; Welch, K.; Sheares, K.; Keeling, D.; Chappell, F.M. D-dimer test for excluding the diagnosis of pulmonary embolism. Cochrane Database Syst. Rev. 2016, 2016, Cd010864. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, Y.; Hosogaya, S.; Osawa, S.; Ichihara, K.; Onuma, T.; Saito, A.; Banba, K.; Araki, H.; Nagamine, Y.; Shinohara, K.; et al. Nationwide multicenter study aimed at the establishment of common reference intervals for standardized clinical laboratory tests in Japan. Clin. Chem. Lab. Med. 2013, 51, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Oi, M.; Yamashita, Y.; Toyofuku, M.; Morimoto, T.; Motohashi, Y.; Tamura, T.; Kaitani, K.; Amano, H.; Takase, T.; Hiramori, S.; et al. D-dimer levels at diagnosis and long-term clinical outcomes in venous thromboembolism: From the COMMAND VTE Registry. J. Thromb. Thrombolysis. 2020, 49, 551–561. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Neither above Threshold (n = 71) | Either above Threshold (n = 148) | Both above Threshold (n = 242) | p Value |
|---|---|---|---|---|
| Demographics | ||||
| Age, years | 62.0 ± 14.3 | 69.5 ± 16.3 | 70.6 ± 13.0 | <0.001 |
| Male, % | 53.5 | 64.9 | 69.4 | 0.045 |
| Japanese, % | 94.4 | 98.8 | 98.8 | 0.079 |
| BMI, kg/m2 | 25.2 ± 4.7 | 23.9 ± 4.9 | 23.9 ± 5.1 | 0.006 |
| Comorbidities and medical history | ||||
| Hypertension, % | 74.6 | 75.0 | 68.2 | 0.282 |
| Diabetes mellitus, % | 22.5 | 35.8 | 48.8 | <0.001 |
| Dyslipidemia, % | 49.3 | 35.1 | 41.7 | 0.124 |
| Heart failure, % | 7.0 | 11.5 | 9.9 | 0.589 |
| Coronary artery disease,% | 7.0 | 11.5 | 9.5 | 0.573 |
| Myocardial infarction, % | 0.0 | 5.4 | 5.8 | 0.120 |
| CI/TIA, % | 4.2 | 6.8 | 10.3 | 0.188 |
| COPD, % | 4.2 | 3.4 | 7.4 | 0.206 |
| CKD, % | 5.6 | 7.4 | 9.5 | 0.528 |
| Cancer, % | 4.2 | 8.1 | 10.7 | 0.218 |
| Symptoms | ||||
| Fever (>38.0 °C), % | 55.1 | 61.9 | 69.5 | 0.062 |
| Cough, % | 47.9 | 45.3 | 53.7 | 0.248 |
| Pharyngitis, % | 16.9 | 14.2 | 8.7 | 0.087 |
| Rhinorrhea, % | 7.0 | 4.1 | 3.7 | 0.472 |
| Dyspnea, % | 15.5 | 33.8 | 47.5 | <0.001 |
| Arthritis, % | 7.0 | 4.1 | 2.5 | 0.192 |
| Headache, % | 9.9 | 8.8 | 5.8 | 0.374 |
| Olfactory dysfunction, % | 9.9 | 10.1 | 5.4 | 0.167 |
| Asymptom, % | 9.9 | 9.5 | 3.7 | 0.038 |
| 4C Mortality Score | 8 (6–11) | 12 (9–14) | 14 (11–15) | < 0.001 |
| Physical findings | ||||
| Max body temperature | 38.0 (37.5–38.3) | 38.0 (37.6–38.5) | 38.0 (37.7–38.6) | 0.005 |
| Herat rate (bpm) | 85.0 (76.0–95.0) | 82.0 (73.0–95.0) | 88.0 (75.0–101.0) | 0.028 |
| Systolic BP (mmHg) | 140.0 (119.0–154.0) | 130.0 (117.0–150.0) | 130.0 (115.0–142.5) | 0.042 |
| Respiratory rate (/min) | 18.0 (16.0–22.0) | 20.0 (17.0–24.0) | 20.0 (18.0–25.3) | 0.001 |
| SpO2, % | 97.0 (96.0–98.0) | 96.0 (95.0–98.0) | 95.0 (92.0–97.0) | <0.001 |
| Laboratory data at admission | ||||
| White blood cell, /μL | 4800 (3760–5900) | 5400 (4400–7400) | 6600 (5000–8800) | <0.001 |
| Lymphocyte, % | 24.0 (17.9–28.5) | 18.3 (12.9–25.4) | 12.3 (8.4–17.5) | <0.001 |
| Neutrocyte, % | 65.2 (60.7–73.4) | 72.3 (63.8–80.7) | 80.3 (73.7–86.2) | <0.001 |
| Eosinocyte, % | 0.50 (0.00–1.20) | 0.30 (0.00–1.15) | 0.00 (0.00–0.500) | <0.001 |
| Hemoglobin, g/dl | 14.0 (12.8–15.1) | 13.4 (11.6–14.9) | 13.0 (11.5–14.5) | 0.003 |
| Platelet, 103/μL | 184.0 (149.0–238.0) | 178.0 (140.0–235.0) | 196.0 (140.0–251.0) | 0.657 |
| Creatinin, mg/dL | 0.77 (0.62–0.88) | 0.85 (0.65–1.10) | 0.87 (0.65–1.14) | 0.012 |
| eGFR, mL/min/1.73 m2 | 94.6 (77.4–105.5) | 86.1 (64.1–106.6) | 82.6 (60.3–109.2) | 0.058 |
| LDH, IU/L | 219.0 (183.5–256.0) | 276.5 (216.0–344.5) | 380.0 (265.0–501.0) | <0.001 |
| HbA1c, % | 6.1 (5.9–6.8) | 6.2 (5.7–6.8) | 6.5 (6.1–7.4) | 0.001 |
| CK, U/L | 73.5 (49.0–108.3) | 84.5 (43.5–142.5) | 88.0 (55.0–189.0) | 0.089 |
| Serum Alb, gL | 4.0 (3.7–4.2) | 3.4 (3.0–3.8) | 3.0 (2.6–3.3) | <0.001 |
| Specific biomarker at admission | ||||
| CRP, mg/L | 7.8 (2.5–14.7) | 30.5 (11.9–74.9) | 106.0 (66.0–159.0) | <0.001 |
| D-dimer, mg/L | 0.60 (0.50–0.70) | 0.90 (0.60–1.70) | 2.24 (1.49–5.31) | <0.001 |
| FDP, μg/mL | 2.50 (1.60–2.95) | 5.25 (3.42–6.40) | 6.6 (5.0–12.9) | <0.001 |
| Ferritin, ng/mL | 234.0 (105.5–460.0) | 476.0 (175.8–1000.8) | 752.0 (312.0–1395.0) | <0.001 |
| Procalcitonin, ng/mL | 0.050 (0.020–0.750) | 0.100 (0.058–0.193) | 0.160 (0.080–0.570) | <0.001 |
| KL-6, U/mL | 277.0 (187.5–398.8) | 276.0 (204.0–490.5) | 332.0 (234.3–471.5) | 0.071 |
| BNP, pg/mL | 11.0 (5.8–34.9) | 29.1 (11.7–134.0) | 58.9 (15.6–169.3) | 0.001 |
| Length of Stay, days | 15.0 (11.0–25.0) | 19.0 (13.0–27.8) | 19.5 (10.0–32.0) | 0.097 |
| Variables | HR | CI | p Value |
|---|---|---|---|
| Age | 1.08 | 1.04–1.11 | <0.000 |
| Male | 1.60 | 0.85–3.01 | 0.147 |
| BMI | 1.11 | 1.04–1.18 | 0.001 |
| Hypertension | 0.97 | 0.51–1.86 | 0.930 |
| Diabetes mellitus | 1.06 | 0.60–1.89 | 0.833 |
| Dyslipidemia | 0.94 | 0.52–1.68 | 0.831 |
| Coronary artery disease | 2.09 | 1.05–4.15 | 0.035 |
| Cancer | 1.26 | 0.60–2.62 | 0.541 |
| COPD | 2.56 | 1.23–5.34 | 0.012 |
| CKD | 1.28 | 0.60–2.75 | 0.524 |
| Both values above threshold (CRP = 29.0 mg/L, D-dimer = 1.00 mg/L) | 2.97 | 1.57–5.60 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitakata, H.; Kohsaka, S.; Kuroda, S.; Nomura, A.; Kitai, T.; Yonetsu, T.; Torii, S.; Matsue, Y.; Matsumoto, S. Inflammatory and Hypercoagulable Biomarkers and Clinical Outcomes in COVID-19 Patients. J. Clin. Med. 2021, 10, 3086. https://doi.org/10.3390/jcm10143086
Kitakata H, Kohsaka S, Kuroda S, Nomura A, Kitai T, Yonetsu T, Torii S, Matsue Y, Matsumoto S. Inflammatory and Hypercoagulable Biomarkers and Clinical Outcomes in COVID-19 Patients. Journal of Clinical Medicine. 2021; 10(14):3086. https://doi.org/10.3390/jcm10143086
Chicago/Turabian StyleKitakata, Hiroki, Shun Kohsaka, Shunsuke Kuroda, Akihiro Nomura, Takeshi Kitai, Taishi Yonetsu, Sho Torii, Yuya Matsue, and Shingo Matsumoto. 2021. "Inflammatory and Hypercoagulable Biomarkers and Clinical Outcomes in COVID-19 Patients" Journal of Clinical Medicine 10, no. 14: 3086. https://doi.org/10.3390/jcm10143086