Anesthetic Agents and Cardiovascular Outcomes of Noncardiac Surgery after Coronary Stent Insertion

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Study Outcomes
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Rabbitts, J.A.; Nuttall, G.A.; Brown, M.J.; Hanson, A.C.; Oliver, W.C.; Holmes, D.R.; Rihal, C.S. Cardiac risk of noncardiac surgery after percutaneous coronary intervention with drug-eluting stents. Anesthesiology 2008, 109, 596–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcock, R.F.; Kouzios, D.; Naoum, C.; Hillis, G.S.; Brieger, D.B. Perioperative myocardial necrosis in patients at high cardiovascular risk undergoing elective non-cardiac surgery. Heart 2012, 98, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger, C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients with Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2016, 68, 1082–1115. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.; Guilera, N.; Mases, A.; Sierra, P.; Oliva, J.C.; Colilles, C.; REGISTRESTENTS Group. Management of antiplatelet therapy in patients with coronary stents undergoing noncardiac surgery: Association with adverse events. Br. J. Anaesth. 2018, 120, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Albaladejo, P.; Marret, E.; Samama, C.M.; Collet, J.P.; Abhay, K.; Loutrel, O.; Charbonneau, H.; Jaber, S.; Thoret, S.; Bosson, J.L.; et al. Non-cardiac surgery in patients with coronary stents: The RECO study. Heart 2011, 97, 1566–1572. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Gupta, N.; Ramakrishna, H.; Guo, Y.; Berger, J.S.; Bangalore, S. Perioperative Major Adverse Cardiovascular and Cerebrovascular Events Associated with Noncardiac Surgery. JAMA Cardiol. 2017, 2, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Cho, Y.J.; Kim, W.H. Perioperative Cardioprotection by Remote Ischemic Conditioning. Int. J. Mol. Sci. 2019, 20, 4839. [Google Scholar] [CrossRef] [Green Version]
- Park, S.K.; Hur, M.; Yoo, S.; Choi, J.Y.; Kim, W.H.; Kim, J.T.; Bahk, J.H. Effect of remote ischaemic preconditioning in patients with ischaemic heart disease undergoing orthopaedic surgery: A randomized controlled trial. Br. J. Anaesth. 2018, 120, 198–200. [Google Scholar] [CrossRef] [Green Version]
- Marouli, D.; Stylianou, K.; Papadakis, E.; Kroustalakis, N.; Kolyvaki, S.; Papadopoulos, G.; Ioannou, C.; Papaioannou, A.; Daphnis, E.; Georgopoulos, D.; et al. Preoperative Albuminuria and Intraoperative Chloride Load: Predictors of Acute Kidney Injury Following Major Abdominal Surgery. J. Clin. Med. 2018, 7, 431. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.; Fang, X.; Ottosson, J.; Naslund, E.; Stenberg, E. A Comparative Study of Machine Learning Algorithms in Predicting Severe Complications after Bariatric Surgery. J. Clin. Med. 2019, 8, 668. [Google Scholar] [CrossRef] [Green Version]
- Piriou, V.; Chiari, P.; Lhuillier, F.; Bastien, O.; Loufoua, J.; Raisky, O.; David, J.S.; Ovize, M.; Lehot, J.J. Pharmacological preconditioning: Comparison of desflurane, sevoflurane, isoflurane and halothane in rabbit myocardium. Br. J. Anaesth. 2002, 89, 486–491. [Google Scholar] [CrossRef]
- Kersten, J.R.; Schmeling, T.J.; Pagel, P.S.; Gross, G.J.; Warltier, D.C. Isoflurane mimics ischemic preconditioning via activation of K(ATP) channels: Reduction of myocardial infarct size with an acute memory phase. Anesthesiology 1997, 87, 361–370. [Google Scholar] [CrossRef]
- Lutz, M.; Liu, H. Inhaled sevoflurane produces better delayed myocardial protection at 48 versus 24 hours after exposure. Anesth. Analg. 2006, 102, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Runzer, T.D.; Ansley, D.M.; Godin, D.V.; Chambers, G.K. Tissue antioxidant capacity during anesthesia: Propofol enhances in vivo red cell and tissue antioxidant capacity in a rat model. Anesth. Analg. 2002, 94, 89–93. [Google Scholar] [PubMed]
- Javadov, S.A.; Lim, K.H.; Kerr, P.M.; Suleiman, M.S.; Angelini, G.D.; Halestrap, A.P. Protection of hearts from reperfusion injury by propofol is associated with inhibition of the mitochondrial permeability transition. Cardiovasc. Res. 2000, 45, 360–369. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.J.; Bae, J.; Kwon, Y.; Jang, H.S.; Yoo, S.; Jeong, C.W.; Kim, J.T.; Kim, W.H. General Anesthetic Agents and Renal Function after Nephrectomy. J. Clin. Med. 2019, 8, 1530. [Google Scholar] [CrossRef] [Green Version]
- Udelsman, R.; Norton, J.A.; Jelenich, S.E.; Goldstein, D.S.; Linehan, W.M.; Loriaux, D.L.; Chrousos, G.P. Responses of the hypothalamic-pituitary-adrenal and renin-angiotensin axes and the sympathetic system during controlled surgical and anesthetic stress. J. Clin. Endocrinol. Metab. 1987, 64, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, B.A.; Beattie, C.; Christopherson, R.; Norris, E.J.; Frank, S.M.; Breslow, M.J.; Rock, P.; Parker, S.D.; Gottlieb, S.O.; Perler, B.A.; et al. The effects of different anesthetic regimens on fibrinolysis and the development of postoperative arterial thrombosis. Perioperative Ischemia Randomized Anesthesia Trial Study Group. Anesthesiology 1993, 79, 435–443. [Google Scholar] [CrossRef]
- Cruickshank, A.M.; Fraser, W.D.; Burns, H.J.; Van Damme, J.; Shenkin, A. Response of serum interleukin-6 in patients undergoing elective surgery of varying severity. Clin. Sci. 1990, 79, 161–165. [Google Scholar] [CrossRef] [Green Version]
- Bassuoni, A.S.; Amr, Y.M. Cardioprotective effect of sevoflurane in patients with coronary artery disease undergoing vascular surgery. Saudi. J. Anaesth. 2012, 6, 125–130. [Google Scholar]
- Lurati Buse, G.A.; Schumacher, P.; Seeberger, E.; Studer, W.; Schuman, R.M.; Fassl, J.; Kasper, J.; Filipovic, M.; Bolliger, D.; Seeberger, M.D. Randomized comparison of sevoflurane versus propofol to reduce perioperative myocardial ischemia in patients undergoing noncardiac surgery. Circulation 2012, 126, 2696–2704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindholm, E.E.; Aune, E.; Noren, C.B.; Seljeflot, I.; Hayes, T.; Otterstad, J.E.; Kirkeboen, K.A. The anesthesia in abdominal aortic surgery (ABSENT) study: A prospective, randomized, controlled trial comparing troponin T release with fentanyl-sevoflurane and propofol-remifentanil anesthesia in major vascular surgery. Anesthesiology 2013, 119, 802–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landoni, G.; Lomivorotov, V.V.; Nigro Neto, C.; Monaco, F.; Pasyuga, V.V.; Bradic, N.; Lembo, R.; Gazivoda, G.; Likhvantsev, V.V.; Lei, C.; et al. Volatile Anesthetics versus Total Intravenous Anesthesia for Cardiac Surgery. N. Engl. J. Med. 2019, 380, 1214–1225. [Google Scholar] [CrossRef] [PubMed]
- Hawn, M.T.; Graham, L.A.; Richman, J.S.; Itani, K.M.; Henderson, W.G.; Maddox, T.M. Risk of major adverse cardiac events following noncardiac surgery in patients with coronary stents. JAMA 2013, 310, 1462–1472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardi, T.; Kayali, A.; Trimaille, A.; Marchandot, B.; Ristorto, J.; Hoang, V.A.; Hess, S.; Kibler, M.; Jesel, L.; Ohlmann, P.; et al. Prognostic Value of Incomplete Revascularization after Percutaneous Coronary Intervention Following Acute Coronary Syndrome: Focus on CKD Patients. J. Clin. Med. 2019, 8, 810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleisher, L.A.; Fleischmann, K.E.; Auerbach, A.D.; Barnason, S.A.; Beckman, J.A.; Bozkurt, B.; Davila-Roman, V.G.; Gerhard-Herman, M.D.; Holly, T.A.; Kane, G.C.; et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J. Am. Coll. Cardiol. 2014, 64, e77–e137. [Google Scholar] [CrossRef] [Green Version]
- Kristensen, S.D.; Knuuti, J.; Saraste, A.; Anker, S.; Botker, H.E.; Hert, S.D.; Ford, I.; Gonzalez-Juanatey, J.R.; Gorenek, B.; Heyndrickx, G.R.; et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: Cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: Cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur. Heart J. 2014, 35, 2383–2431. [Google Scholar]
- Glance, L.G.; Lustik, S.J.; Hannan, E.L.; Osler, T.M.; Mukamel, D.B.; Qian, F.; Dick, A.W. The Surgical Mortality Probability Model: Derivation and validation of a simple risk prediction rule for noncardiac surgery. Ann. Surg. 2012, 255, 696–702. [Google Scholar] [CrossRef] [Green Version]
- Devereaux, P.J.; Mrkobrada, M.; Sessler, D.I.; Leslie, K.; Alonso-Coello, P.; Kurz, A.; Villar, J.C.; Sigamani, A.; Biccard, B.M.; Meyhoff, C.S.; et al. Aspirin in patients undergoing noncardiac surgery. N. Engl. J. Med. 2014, 370, 1494–1503. [Google Scholar] [CrossRef] [Green Version]
- Novalija, E.; Varadarajan, S.G.; Camara, A.K.; An, J.; Chen, Q.; Riess, M.L.; Hogg, N.; Stowe, D.F. Anesthetic preconditioning: Triggering role of reactive oxygen and nitrogen species in isolated hearts. Am. J. Physiol. Heart Circ. Physiol. 2002, 283, H44–H52. [Google Scholar] [CrossRef]
- Tanguay, M.; Blaise, G.; Dumont, L.; Beique, G.; Hollmann, C. Beneficial effects of volatile anesthetics on decrease in coronary flow and myocardial contractility induced by oxygen-derived free radicals in isolated rabbit hearts. J. Cardiovasc. Pharmacol. 1991, 18, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; McPherson, B.C.; Yao, Z. Preconditioning attenuates apoptosis and necrosis: Role of protein kinase C epsilon and -delta isoforms. Am. J. Physiol. Heart Circ. Physiol. 2001, 281, H404–H410. [Google Scholar] [CrossRef] [PubMed]
- Hemmings, H.C., Jr.; Adamo, A.I. Activation of endogenous protein kinase C by halothane in synaptosomes. Anesthesiology 1996, 84, 652–662. [Google Scholar] [CrossRef]
- de Ruijter, W.; Musters, R.J.; Boer, C.; Stienen, G.J.; Simonides, W.S.; de Lange, J.J. The cardioprotective effect of sevoflurane depends on protein kinase C activation, opening of mitochondrial K(+)(ATP) channels, and the production of reactive oxygen species. Anesth. Analg. 2003, 97, 1370–1376. [Google Scholar] [CrossRef] [PubMed]
- Piriou, V.; Chiari, P.; Gateau-Roesch, O.; Argaud, L.; Muntean, D.; Salles, D.; Loufouat, J.; Gueugniaud, P.Y.; Lehot, J.J.; Ovize, M. Desflurane-induced preconditioning alters calcium-induced mitochondrial permeability transition. Anesthesiology 2004, 100, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Fleisher, L.A.; Beckman, J.A.; Brown, K.A.; Calkins, H.; Chaikof, E.L.; Fleischmann, K.E.; Freeman, W.K.; Froehlich, J.B.; Kasper, E.K.; Kersten, J.R.; et al. ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) Developed in Collaboration With the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J. Am. Coll. Cardiol. 2007, 50, 1707–1732. [Google Scholar] [PubMed]
- Landoni, G.; Fochi, O.; Bignami, E.; Calabro, M.G.; D’Arpa, M.C.; Moizo, E.; Mizzi, A.; Pappalardo, F.; Morelli, A.; Zangrillo, A. Cardiac protection by volatile anesthetics in non-cardiac surgery? A meta-analysis of randomized controlled studies on clinically relevant endpoints. HSR Proc. Intensive Care Cardiovasc. Anesth. 2009, 1, 34–43. [Google Scholar]
- Zangrillo, A.; Testa, V.; Aldrovandi, V.; Tuoro, A.; Casiraghi, G.; Cavenago, F.; Messina, M.; Bignami, E.; Landoni, G. Volatile agents for cardiac protection in noncardiac surgery: A randomized controlled study. J. Cardiothorac. Vasc. Anesth. 2011, 25, 902–907. [Google Scholar] [CrossRef]
- Kwon, J.H.; Park, J.; Lee, S.H.; Oh, A.R.; Lee, J.H.; Min, J.J. Effects of Volatile versus Total Intravenous Anesthesia on Occurrence of Myocardial Injury after Non-Cardiac Surgery. J. Clin. Med. 2019, 8, 1999. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Lin, W.; Shen, S.; Wang, H.; Feng, X.; Sun, J. Randomized comparison of sevoflurane versus propofol-remifentanil on the cardioprotective effects in elderly patients with coronary heart disease. BMC Anesthesiol. 2017, 17, 104. [Google Scholar] [CrossRef]
- Landoni, G.; Biondi-Zoccai, G.G.; Zangrillo, A.; Bignami, E.; D’Avolio, S.; Marchetti, C.; Calabro, M.G.; Fochi, O.; Guarracino, F.; Tritapepe, L.; et al. Desflurane and sevoflurane in cardiac surgery: A meta-analysis of randomized clinical trials. J. Cardiothorac. Vasc. Anesth. 2007, 21, 502–511. [Google Scholar] [CrossRef] [PubMed]
- Landoni, G.; Greco, T.; Biondi-Zoccai, G.; Nigro Neto, C.; Febres, D.; Pintaudi, M.; Pasin, L.; Cabrini, L.; Finco, G.; Zangrillo, A. Anaesthetic drugs and survival: A Bayesian network meta-analysis of randomized trials in cardiac surgery. Br. J. Anaesth. 2013, 111, 886–896. [Google Scholar] [CrossRef] [Green Version]
- Uhlig, C.; Bluth, T.; Schwarz, K.; Deckert, S.; Heinrich, L.; De Hert, S.; Landoni, G.; Serpa Neto, A.; Schultz, M.J.; Pelosi, P.; et al. Effects of Volatile Anesthetics on Mortality and Postoperative Pulmonary and Other Complications in Patients Undergoing Surgery: A Systematic Review and Meta-analysis. Anesthesiology 2016, 124, 1230–1245. [Google Scholar] [CrossRef] [PubMed]
- Howell, S.J.; Hoeks, S.E.; West, R.M.; Wheatcroft, S.B.; Hoeft, A. Prospective observational cohort study of the association between antiplatelet therapy, bleeding and thrombosis in patients with coronary stents undergoing noncardiac surgery. Br. J. Anaesth. 2019, 122, 170–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, B.B.; Warner, M.A.; Warner, N.S.; Hanson, A.C.; Smith, M.M.; Rihal, C.S.; Gulati, R.; Bell, M.R.; Nuttall, G.A. Cardiac Risk of Noncardiac Surgery After Percutaneous Coronary Intervention With Second-Generation Drug-Eluting Stents. Anesth. Analg. 2019, 128, 621–628. [Google Scholar] [CrossRef]
- Kurth, T.; Walker, A.M.; Glynn, R.J.; Chan, K.A.; Gaziano, J.M.; Berger, K.; Robins, J.M. Results of multivariable logistic regression, propensity matching, propensity adjustment, and propensity-based weighting under conditions of nonuniform effect. Am. J. Epidemiol. 2006, 163, 262–270. [Google Scholar] [CrossRef]
- Oprea, A.D.; Fontes, M.L.; Onaitis, M.W.; Kertai, M.D. Comparison Between the 2007 and 2014 American College of Cardiology/American Heart Association Guidelines on Perioperative Evaluation for Noncardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2015, 29, 1639–1650. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | TIVA (n = 975) | SEVO (n = 439) | DES (n = 216) | p-Value |
|---|---|---|---|---|
| Demographic data | ||||
| Age, years, median (IQR) | 69 (61–76) | 70 (61–77) | 71 (62–78) | 0.307 |
| Female, n | 322 (33.0) | 174 (39.6) | 82 (38.0) | 0.040 |
| Body-mass index, kg/m2 | 23.4 (21.7–24.9) | 23.4 (21.0–24.9) | 23.4 (21.3–25.7) | 0.305 |
| Body-mass index >30 kg/m2, n | 33 (3.4) | 12 (2.7) | 8 (3.7) | 0.950 |
| Medical history | ||||
| Hypertension, n | 590 (60.5) | 286 (65.1) | 128 (59.3) | 0.190 |
| Diabetes mellitus, n | 382 (39.2) | 173 (39.4) | 70 (32.4) | 0.156 |
| Stroke, n | 21 (2.2) | 16 (3.6) | 4 (1.9) | 0.203 |
| Chronic kidney disease*, n | 106 (10.9) | 62 (14.1) | 21 (9.7) | 0.137 |
| ASA physical status classification, 2/3/4 n | 620 (63.6)/334 (34.3)/21 (2.2) | 279 (63.6)/151 (34.4)/9 (2.1) | 138 (63.9)/73 (33.8)/5 (2.3) | 0.970 |
| Coronary intervention type | ||||
| First generation drug-eluting stent, n | 394 (40.4) | 164 (37.4) | 88 (40.7) | 0.520 |
| Sirolimus-eluting stent (Cypher), n | 181 (18.6) | 78 (17.8) | 39 (18.1) | 0.934 |
| Paclitaxel-eluting stent (Taxus), n | 222 (22.8) | 87 (19.8) | 54 (25.0) | 0.273 |
| Second generation drug-eluting stent (Xience, Endeavor, Resolute, Coroflex), n | 581 (59.6) | 275 (62.6) | 129 (59.7) | 0.540 |
| Time from PCI to surgery, days | 548 (132–1438) | 647 (150–1456) | 638 (144–1461) | 0.595 |
| Time from PCI to surgery | ||||
| <30 days | 140 (14.4) | 62 (14.1) | 35 (16.2) | 0.753 |
| 30–180 days | 133 (13.6) | 55 (12.5) | 23 (10.6) | 0.473 |
| 181–365 days | 107 (11.0) | 38 (8.7) | 22 (10.2) | 0.413 |
| >1 year | 595 (61.0) | 284 (64.7) | 136 (63.0) | 0.410 |
| Maintenance of aspirin until surgery without discontinuation, n | 299 (30.7) | 107 (24.4) | 57 (26.4) | 0.041 |
| Maintenance of clopidogrel until surgery without discontinuation, n | 139 (14.3) | 53 (12.1) | 34 (15.7) | 0.379 |
| Maintenance of dual antiplatelet agent, n | 101 (10.4) | 35 (8.0) | 21 (9.7) | 0.420 |
| Preoperative other medications | ||||
| Beta-blocker, n | 185 (19.0) | 82 (18.7) | 44 (20.4) | 0.737 |
| ACE inhibitor, n | 65 (6.7) | 31 (7.1) | 15 (6.9) | 0.817 |
| Angiotensin receptor blocker, n | 147 (15.1) | 61 (13.9) | 38 (17.6) | 0.592 |
| Calcium channel blocker, n | 248 (25.4) | 109 (24.8) | 57 (26.4) | 0.888 |
| Statin, n | 273 (28.0) | 121 (27.6) | 59 (27.3) | 0.813 |
| Diuretics, n | 78 (8.0) | 35 (8.0) | 19 (8.8) | 0.755 |
| Oral hypoglycemic agent, n | 361 (37.0) | 163 (37.1) | 65 (30.1) | 0.118 |
| Preoperative laboratory finding | ||||
| Hematocrit, % | 38.3 (34.8–42.1) | 38.2 (33.9–42.1) | 39.4 (35.3–41.6) | 0.303 |
| Albumin, g/dL | 4.1 (3.8–4.4)/n = 937 | 4.2 (3.9–4.4)/n = 428 | 4.2 (3.9–4.4)/n = 213 | 0.248 |
| Surgery-related parameter | ||||
| High-risk surgery | ||||
| Emergency surgery, n | 27 (2.8) | 13 (3.0) | 0 (0.0) | 0.043 |
| Vascular surgery, n | 99 (10.2) | 36 (8.2) | 12 (5.6) | 0.080 |
| Intermediate-risk surgery | ||||
| Nose, mouth, and pharynx surgery, n | 96 (9.8) | 51 (11.6) | 5 (2.3) | <0.001 |
| Abdominal surgery, n | 392 (40.2) | 119 (27.1) | 61 (28.2) | <0.001 |
| Musculoskeletal surgery, n | 128 (13.1) | 78 (17.8) | 15 (6.9) | 0.001 |
| Neurosurgery, n | 27 (2.8) | 20 (4.6) | 8 (3.7) | 0.218 |
| Low-risk surgery | ||||
| Urologic surgery, n | 112 (11.5) | 35 (8.0) | 56 (25.9) | <0.001 |
| Gynecologic surgery, n | 16 (1.6) | 13 (3.0) | 8 (3.7) | 0.096 |
| Miscellaneous, n | 105 (10.8) | 87 (19.8) | 51 (23.6) | <0.001 |
| Surgery time, min | 130 (65–200)/n = 942 | 120 (65–209)/n = 422 | 120 (60–183)/n = 212 | 0.152 |
| Anesthesia time, min | 170 (100–255)/n = 941 | 170 (100–265)/n = 422 | 155 (95–235)/n = 212 | 0.056 |
| Intraoperative colloid administration, n | 171 (17.5) | 83 (18.9) | 22 (10.2) | 0.015 |
| Intraoperative colloid administration, mL | 500 (500–900) | 500 (500–1000) | 500 (500–900) | 0.240 |
| Intraoperative red blood cell transfusion, n | 66 (6.8) | 35 (8.0) | 11 (5.1) | 0.384 |
| Intraoperative fresh frozen plasma transfusion, n | 57 (5.8) | 29 (6.6) | 10 (4.6) | 0.598 |
| Outcome | Definition |
|---|---|
| Myocardial infarction | Diagnosis of myocardial infarction required any one of the followings: 1. A typical rise of troponin or a typical fall of an elevated troponin detected at its peak post-surgery in a patient without a documented other explanation for the troponin change (e.g., pulmonary embolism) OR a rapid rise and fall of creatinine kinase-myocardial band (CK-MB). This finding should accompany one of the following: a. ischemic sign or symptom b. development of pathologic Q wave c. ECG changes indicative of ischemia d. coronary intervention (i.e., PCI or CABG surgery) e. new or presumed new cardiac wall motion abnormality on echocardiography or new or presumed new fixed defect on radionuclide myocardial imaging 2. Development of new pathological Q wave on an ECG if troponin levels were not obtained or were obtained at times that could have missed the clinical event. |
| Non-fatal myocardial infarction | Non-fatal myocardial infarction was defined as successful patient treatment and resuscitation from either documented or presumed myocardial infarction. |
| Coronary revascularization | Cardiac revascularization procedure was defined as PCI or CABG surgery. |
| Pulmonary embolism | The diagnosis of pulmonary embolism required any one of the following: 1. Diagnosis suggested with a high probability by ventilation/perfusion lung scan 2. An intraluminal filling defect on pulmonary angiography 3. An intraluminal filling defect of segmental or larger pulmonary artery on a helical CT scan 4. A positive diagnostic test for deep vein thrombosis and one of the following a. non-diagnostic ventilation/perfusion lung scan (i.e., low or intermediate probability suggested) b. non-diagnostic helical CT scan (i.e., subsegmental defect or technically inadequate study) |
| Non-hemorrhagic stroke | Stroke was defined as a new focal neurological deficit thought to be vascular in origin with signs or symptoms lasting more than 24 hours. Non-hemorrhagic stroke was identified by lack of hemorrhage in the brain imaging study including CT or MRI. |
| Before Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| Characteristics | TIVA (n = 975) | Volatile (n = 655) | p-Value | TIVA (n = 642) | Volatile (n = 642) | p-Value |
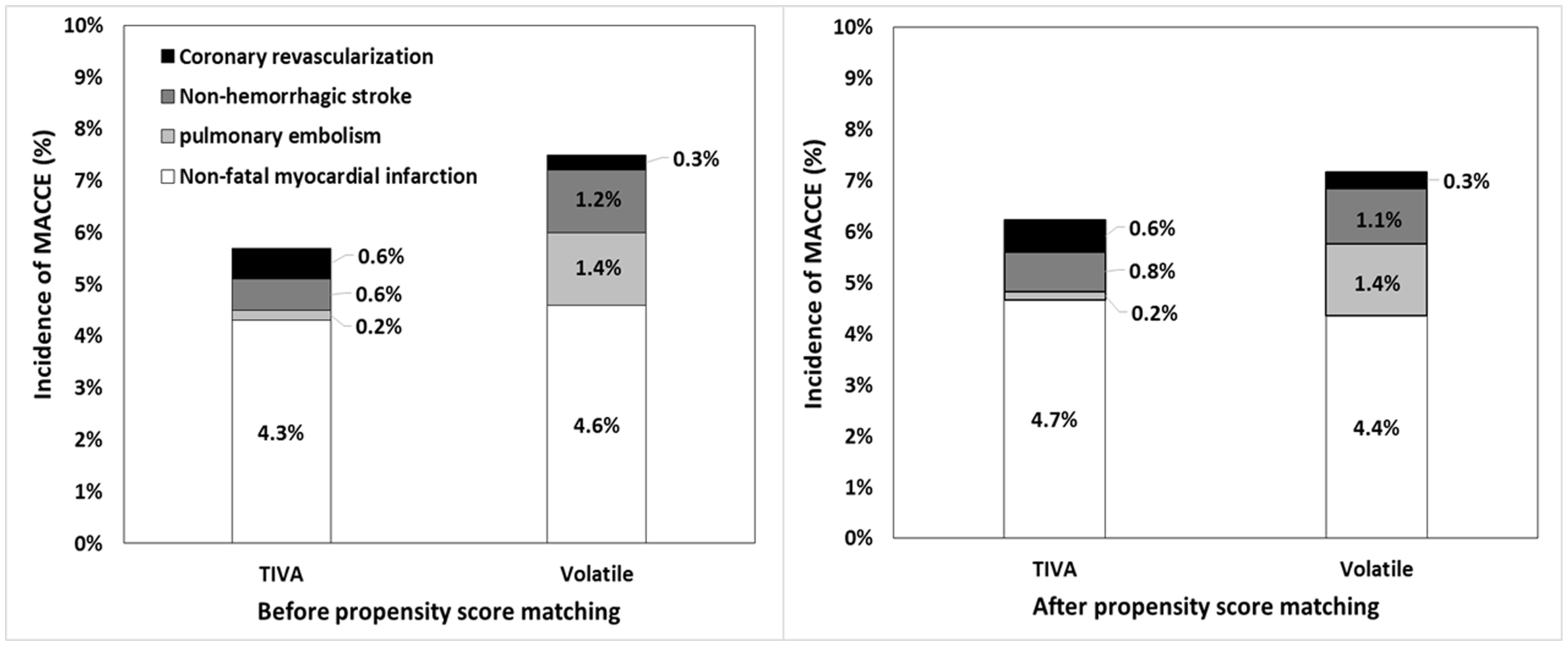
| MACCE | 50 (5.1) | 47 (7.2) | 0.087 | 36 (5.6) | 44 (6.9) | 0.356 |
| Fatal myocardial infarction | - | - | - | - | - | - |
| Non-fatal myocardial infarction | 42 (4.3) | 30 (4.6) | 0.793 | 30 (4.7) | 28 (4.4) | 0.788 |
| Pulmonary embolism | 2 (0.2) | 9 (1.4) | 0.009 | 1 (0.2) | 9 (1.4) | 0.021 |
| Non-hemorrhagic stroke | 6 (0.6) | 8 (1.2) | 0.273 | 5 (0.8) | 7 (1.1) | 0.733 |
| Coronary revascularization | 6 (0.6) | 2 (0.3) | 0.487 | 4 (0.6) | 2 (0.3) | 0.687 |
| Major bleeding | 35 (3.6) | 30 (4.6) | 0.316 | 22 (3.4) | 28 (4.4) | 0.387 |
| Variable | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Age, year | 1.00 (0.98–1.03) | 0.708 |
| Female | 0.70 (0.42–1.17) | 0.174 |
| Body-mass index > 30 kg/m2 | 0.68 (0.16–2.98) | 0.612 |
| Interval between PCI and surgery | ||
| <30 days | 2.10 (1.18–3.72) | 0.011 |
| 30–180 days | 1.02 (0.49–2.13) | 0.963 |
| 181–365 days | 0.86 (0.40–1.86) | 0.697 |
| >1 year | reference | |
| Hypertension | 0.86 (0.54–1.39) | 0.545 |
| Diabetes mellitus | 1.20 (0.77–1.88) | 0.428 |
| Chronic kidney disease | 2.46 (1.39–4.35) | 0.002 |
| Stroke | 0.86 (0.19–3.99) | 0.847 |
| Preoperative beta-blocker | 0.89 (0.67–1.94) | 0.435 |
| Preoperative ACE inhibitor or ARB | 0.95 (0.38–2.48) | 0.514 |
| Calcium channel blocker | 1.35 (0.57–1.95) | 0.774 |
| Statin | 0.91 (0.44–1.84) | 0.614 |
| Diuretics | 1.13 (0.34–2.57) | 0.546 |
| Oral hypoglycemic agent | 1.23 (0.60–1.74) | 0.517 |
| Second vs. first generation drug-eluting stent | 0.97 (0.61–1.56) | 0.906 |
| Surgery time, hour | 1.14 (1.03–1.26) | 0.013 |
| Preoperative hemoglobin, g/dL | 0.91 (0.56–1.64) | 0.400 |
| Preoperative albumin, g/dL | 0.92 (0.41–1.83) | 0.205 |
| Emergency surgery | 1.39 (0.44–4.37) | 0.575 |
| Vascular surgery | 2.84 (1.44–5.60) | 0.003 |
| Musculoskeletal surgery | 2.59 (1.34–5.34) | 0.002 |
| Intraoperative colloid administration | 1.00 (1.00–1.00) | 0.327 |
| Intraoperative red blood cell transfusion | 1.41 (0.58–3.46) | 0.448 |
| Maintenance of aspirin until surgery without discontinuation | 0.74 (0.36–1.39) | 0.415 |
| Maintenance of clopidogrel until surgery without discontinuation | 0.52 (0.23–1.30) | 0.245 |
| Maintenance of dual antiplatelet therapy | 0.83 (0.71–0.98) | 0.041 |
| Volatile anesthetics vs. total intravenous anesthesia | 1.49 (0.91–2.39) | 0.213 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, H.-K.; Jun, K.; Park, S.-K.; Ji, S.-H.; Jang, Y.-E.; Yoo, S.; Kim, J.-T.; Kim, W.H. Anesthetic Agents and Cardiovascular Outcomes of Noncardiac Surgery after Coronary Stent Insertion. J. Clin. Med. 2020, 9, 429. https://doi.org/10.3390/jcm9020429
Yoon H-K, Jun K, Park S-K, Ji S-H, Jang Y-E, Yoo S, Kim J-T, Kim WH. Anesthetic Agents and Cardiovascular Outcomes of Noncardiac Surgery after Coronary Stent Insertion. Journal of Clinical Medicine. 2020; 9(2):429. https://doi.org/10.3390/jcm9020429
Chicago/Turabian StyleYoon, Hyun-Kyu, Kwanghoon Jun, Sun-Kyung Park, Sang-Hwan Ji, Young-Eun Jang, Seokha Yoo, Jin-Tae Kim, and Won Ho Kim. 2020. "Anesthetic Agents and Cardiovascular Outcomes of Noncardiac Surgery after Coronary Stent Insertion" Journal of Clinical Medicine 9, no. 2: 429. https://doi.org/10.3390/jcm9020429