Major Bleeding Predictors in Patients with Left Atrial Appendage Closure: The Iberian Registry II

 ,
,
Abstract
:1. Introduction
2. Methods
Patients and Procedures
3. Statistical Analysis
4. Results
5. Discussion
5.1. The Importance of GIB, Major Bleeding History and Follow-up Time
5.2. The Importance of Age
5.3. Post-Implantation Treatment is an Important Variable
6. Conclusions
6.1. What is Known about the Topic?
- -
- LAAC is an effective therapeutic option for atrial fibrillation patients with a contraindication for the use of anticoagulants.
- -
- However, these patients present a high bleeding risk even in the absence of antiplatelet treatment.
- -
- Age influences the emergence of complications during follow-up of LAAC patients.
6.2. What does this Study add?
- -
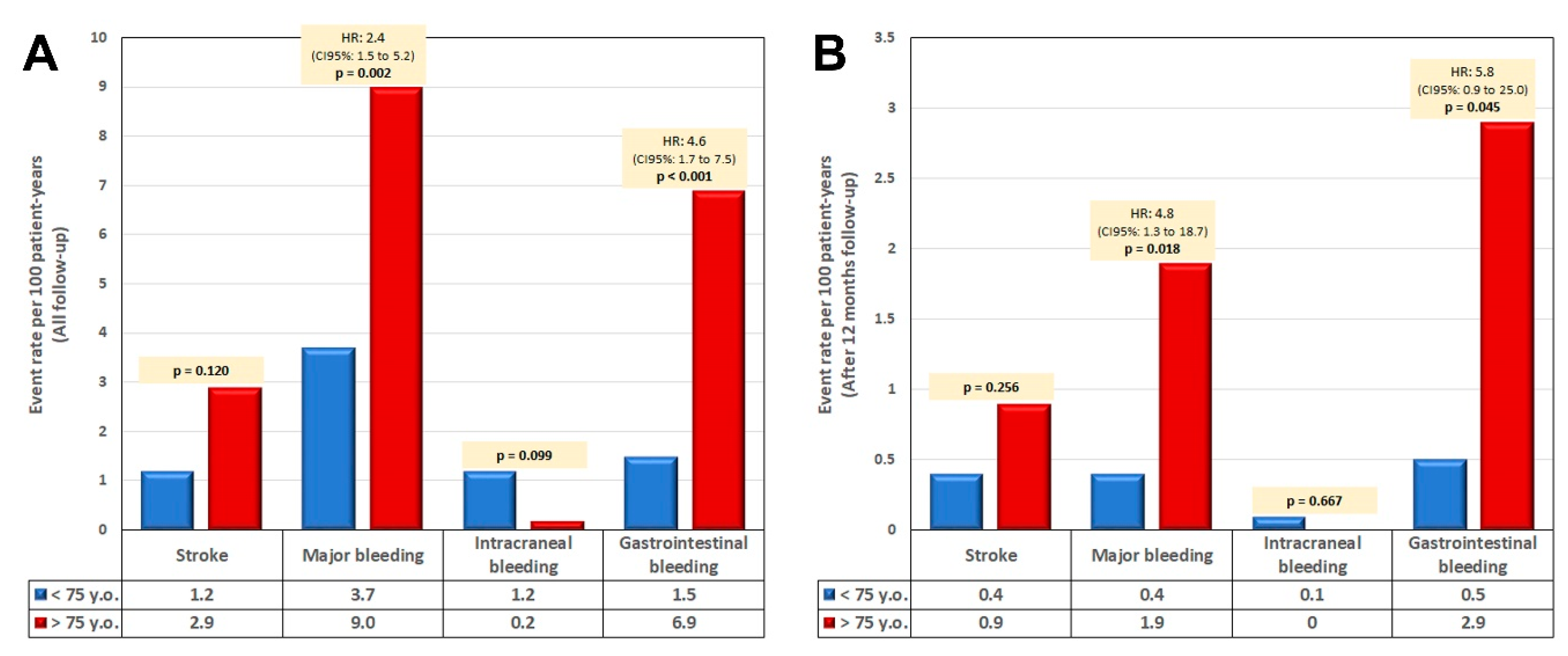
- This study shows that age has a greater influence on the occurrence of major bleedings than on thromboembolic events.
- -
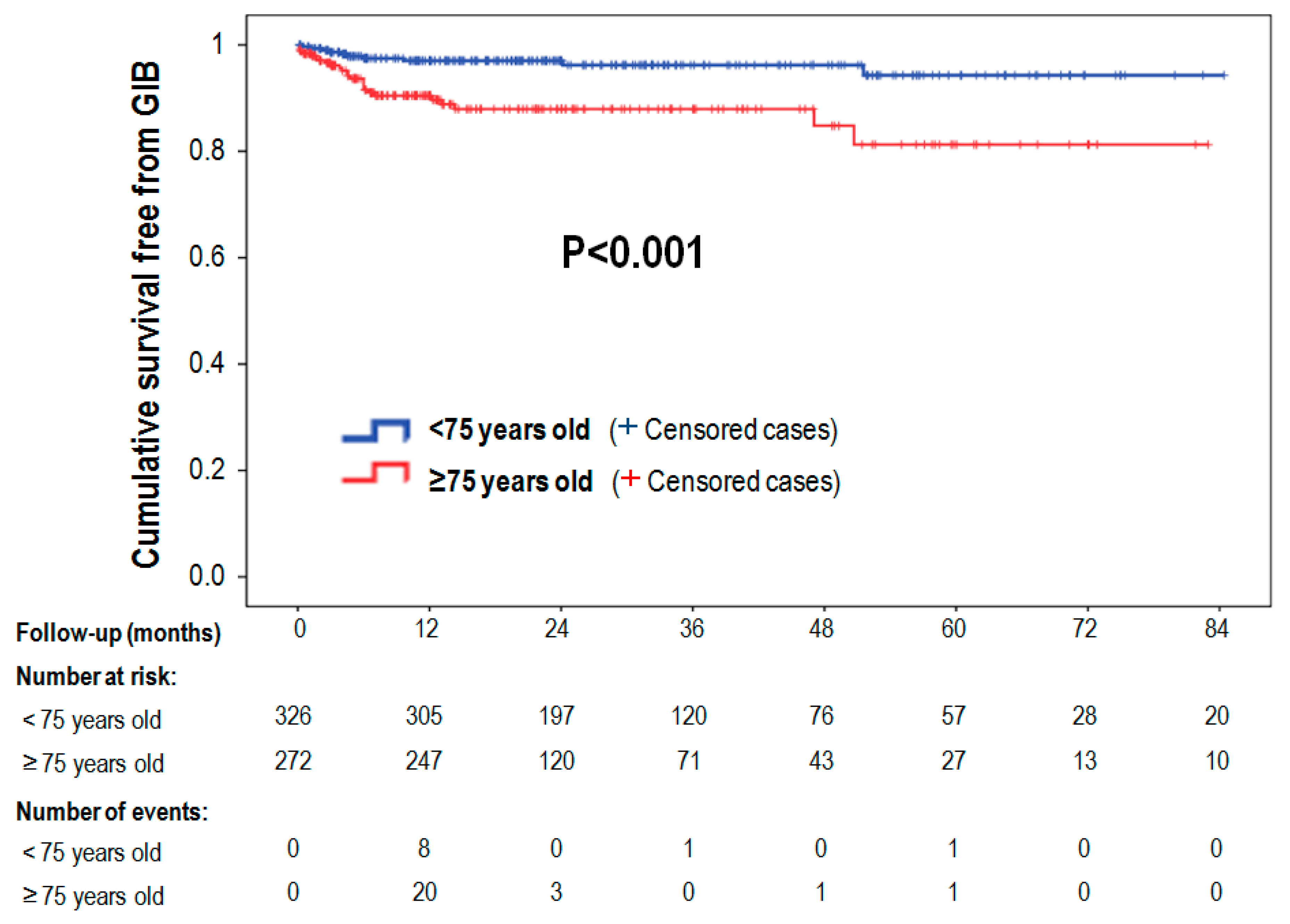
- Our analysis also shows that GIB history is the main predictive factor of major bleeding events during the first year of follow-up after LAAC.
- -
- Differences in the rates of major bleeding events reported in different series of LAAC patients may be due to the number of patients ≥ 75 years and the percentage of patients with GIB history included in those series.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| LAAC | left atrial appendage closure |
| GIB | gastrointestinal bleeding |
| OAC | oral anticoagulants |
| NOAC | new oral anticoagulants |
| NVAF | non-valvular atrial fibrillation |
References
- Sharma, D.; Reddy, V.Y.; Sandri, M.; Schulz, P.; Majunke, N.; Hala, P.; Wiebe, J.; Mraz, T.; Miller, M.A.; Neuzil, P.; et al. Left Atrial Appendage Closure in Patients With Contraindications to Oral Anticoagulation. J. Am. Coll. Cardiol. 2016, 67, 2190–2192. [Google Scholar] [CrossRef] [PubMed]
- Landmesser, U.; Tondo, C.; Camm, J.; Diener, H.C.; Paul, V.; Schmidt, B.; Settergren, M.; Teiger, E.; Nielsen-Kudsk, J.E.; Hildick-Smith, D. Left atrial appendage occlusion with the AMPLATZER Amulet device: One-year follow-up from the prospective global Amulet observational registry. EuroIntervention 2018, 14, e590–e597. [Google Scholar] [CrossRef] [PubMed]
- Phillips, K.P.; Santoso, T.; Sanders, P.; Alison, J.; Chan, J.L.K.; Pak, H.N.; Chandavimol, M.; Stein, K.M.; Gordon, N.; Razali, O.B. Left atrial appendage closure with WATCHMAN in Asian patients: 2 year outcomes from the WASP registry. Int. J. Cardiol Heart Vasc. 2019, 23, 100358. [Google Scholar] [CrossRef] [PubMed]
- Freixa, X.; Gafoor, S.; Regueiro, A.; Cruz-Gonzalez, I.; Shakir, S.; Omran, H.; Berti, S.; Santoro, G.; Kefer, J.; Landmesser, U.; et al. Comparison of Efficacy and Safety of Left Atrial Appendage Occlusion in Patients Aged <75 to >/= 75 Years. Am. J. Cardiol. 2016, 117, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Minguez, J.R.; Nogales-Asensio, J.M.; Infante De Oliveira, E.; De Gama Ribeiro, V.; Ruiz-Salmeron, R.; Arzamendi-Aizpurua, D.; Costa, M.; Gutierrez-Garcia, H.; Fernandez-Diaz, J.A.; Martin-Yuste, V.; et al. Long-term Event Reduction After Left Atrial Appendage Closure. Results of the Iberian Registry II. Rev. Esp. Cardiol. 2019, 72, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Friberg, L.; Rosenqvist, M.; Lip, G.Y. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182 678 patients with atrial fibrillation: The Swedish Atrial Fibrillation cohort study. Eur. Heart J. 2012, 33, 1500–1510. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.; Frison, L.; Halperin, J.L.; Lane, D.A. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fibrillation: The HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/Alcohol Concomitantly) score. J. Am. Coll. Cardiol. 2011, 57, 173–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kappetein, A.P.; Head, S.J.; Genereux, P.; Piazza, N.; van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document. EuroIntervention 2012, 8, 782–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez Minguez, J.R.; Asensio, J.M.; Gragera, J.E.; Costa, M.; Gonzalez, I.C.; de Carlos, F.G.; Diaz, J.A.; Martin Yuste, V.; Gonzalez, R.M.; Dominguez-Franco, A.; et al. Two-year clinical outcome from the Iberian registry patients after left atrial appendage closure. Heart 2015, 101, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef]
- Boersma, L.V.; Ince, H.; Kische, S.; Pokushalov, E.; Schmitz, T.; Schmidt, B.; Gori, T.; Meincke, F.; Protopopov, A.V.; Betts, T.; et al. Efficacy and safety of left atrial appendage closure with WATCHMAN in patients with or without contraindication to oral anticoagulation: 1-Year follow-up outcome data of the EWOLUTION trial. Heart Rhythm 2017, 14, 1302–1308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzikas, A.; Shakir, S.; Gafoor, S.; Omran, H.; Berti, S.; Santoro, G.; Kefer, J.; Landmesser, U.; Nielsen-Kudsk, J.E.; Cruz-Gonzalez, I.; et al. Left atrial appendage occlusion for stroke prevention in atrial fibrillation: Multicentre experience with the AMPLATZER Cardiac Plug. EuroIntervention 2016, 11, 1170–1179. [Google Scholar] [CrossRef] [PubMed]
- Berti, S.; Santoro, G.; Brscic, E.; Montorfano, M.; Vignali, L.; Danna, P.; Tondo, C.; D’Amico, G.; Stabile, A.; Sacca, S.; et al. Left atrial appendage closure using AMPLATZER devices: A large, multicenter, Italian registry. Int. J. Cardiol. 2017, 248, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Boersma, L.V.; Ince, H.; Kische, S.; Pokushalov, E.; Schmitz, T.; Schmidt, B.; Gori, T.; Meincke, F.; Protopopov, A.V.; Betts, T.; et al. Evaluating Real-World Clinical Outcomes in Atrial Fibrillation Patients Receiving the WATCHMAN Left Atrial Appendage Closure Technology. Circ. Arrhythm Electrophysiol. 2019, 12, e006841. [Google Scholar] [CrossRef] [PubMed]
- Hylek, E.M.; Evans-Molina, C.; Shea, C.; Henault, L.E.; Regan, S. Major hemorrhage and tolerability of warfarin in the first year of therapy among elderly patients with atrial fibrillation. Circulation 2007, 115, 2689–2696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, C.H.; Kim, M.; Kim, J.; Nam, G.B.; Choi, K.J.; Kim, Y.H. Real-world comparison of non-vitamin K antagonist oral anticoagulants and warfarin in Asian octogenarian patients with atrial fibrillation. J. Geriatr. Cardiol. 2016, 13, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Kato, E.T.; Giugliano, R.P.; Ruff, C.T.; Koretsune, Y.; Yamashita, T.; Kiss, R.G.; Nordio, F.; Murphy, S.A.; Kimura, T.; Jin, J.; et al. Efficacy and Safety of Edoxaban in Elderly Patients With Atrial Fibrillation in the ENGAGE AF-TIMI 48 Trial. J. Am. Heart Assoc. 2016, 5, e003432. [Google Scholar] [CrossRef] [PubMed]
- Lauw, M.N.; Eikelboom, J.W.; Coppens, M.; Wallentin, L.; Yusuf, S.; Ezekowitz, M.; Oldgren, J.; Nakamya, J.; Wang, J.; Connolly, S.J. Effects of dabigatran according to age in atrial fibrillation. Heart 2017, 103, 1015–1023. [Google Scholar] [CrossRef] [PubMed]
- Patti, G.; Lucerna, M.; Pecen, L.; Siller-Matula, J.M.; Cavallari, I.; Kirchhof, P.; De Caterina, R. Thromboembolic Risk, Bleeding Outcomes and Effect of Different Antithrombotic Strategies in Very Elderly Patients With Atrial Fibrillation: A Sub-Analysis From the PREFER in AF (PREvention oF Thromboembolic Events-European Registry in Atrial Fibrillation). J. Am. Heart Assoc. 2017, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Gonzalez, I.; Ince, H.; Kische, S.; Schmitz, T.; Schmidt, B.; Gori, T.; Foley, D.; De Potter, T.; Tschishow, W.; Vireca, E.; et al. Left atrial appendage occlusion in patients older than 85 years. Safety and efficacy in the EWOLUTION registry. Rev. Esp. Cardiol. 2019. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| <75 (n = 326) | ≥75 (n = 272) | p-Value | |
|---|---|---|---|
| Age | 67.3 ± 5.8 | 80.3 ± 3.5 | <0.001 |
| Female | 112 (34.4%) | 116 (42.6%) | 0.038 |
| Hypertension | 255 (78.2%) | 213 (78.3%) | 0.979 |
| Diabetes | 106 (32.5%) | 98 (36.0%) | 0.367 |
| Permanent AF | 149 (45.7%) | 159 (58.5%) | 0.002 |
| Previous stroke | 111 (34.0%) | 77 (28.3%) | 0.132 |
| Previous bleeding | 170 (52.1%) | 221 (81.3%) | <0.001 |
| Previous ICH | 95 (29.1%) | 65 (23.9%) | 0.149 |
| Previous GI bleeding | 106 (32.5%) | 132 (48.5%) | <0.001 |
| Previous major bleeding | 130 (39.9%) | 145 (53.3%) | 0.001 |
| CHA2DS2-VASc * | 4 [2] | 5 [2] | <0.001 |
| HAS-BLED * | 3 [1] | 3 [1] | 0.007 |
| Anemia | 63 (19.3%) | 102 (37.5%) | <0.001 |
| Renal failure | 42 (12.9%) | 85 (31.3%) | <0.001 |
| <75 (n = 326) | ≥75 (n = 272) | HR (<75 vs. ≥75) | p-Value | |
|---|---|---|---|---|
| Death | 3.9 | 11.8 | 3.0 | <0.001 |
| Stroke | 1.2 | 2.9 | 2.4 | 0.120 |
| ICH | 1.2 | 0.2 | 0.2 | 0.099 |
| GI bleeding | 1.5 | 6.9 | 4.6 | <0.001 |
| Major bleeding | 3.7 | 9.0 | 2.4 | 0.002 |
| Expected events (×100 patient-years) in ≥75 years | Observed events (×100 patient-years) in ≥75 years | Expected events (×100 patient-years) in <75 years | Observed events (×100 patient-years) in <75 years | |
|---|---|---|---|---|
| Ischemic stroke | 7.2 CHADs-VASc score | 2.9 Reduction, 59.7% p ≤ 0.001 | 5.1 CHADs-VASc score | 1.2 Reduction, 76.5% p ≤ 0.001 |
| ICH | 1.0 HAS-BLED score | 0.3 Reduction, 70.8% p = 0.220 | 0.9 HAS-BLED score | 1.2 Increase, 33.3% p = 0.642 |
| GI bleeding | 6.9 | 1.5 | ||
| Major bleeding | 6.6 HAS-BLED score (Friberg Registry) | 9.0 Increase, 26.7% p < 0.001 | 6.2 HAS-BLED score (Friberg Registry) | 3.7 Reduction, 40.3%) p = 0.007 |
| <75 (n = 326) | ≥75 (n = 272) | p-Value | |
|---|---|---|---|
| AAS | 208 (63.8%) | 166 (61.0%) | 0.485 |
| Clopidogrel | 207 (63.5%) | 164 (60.3%) | 0.422 |
| AAS + Clopidogrel | 185 (56.7%) | 138 (50.7%) | 0.142 |
| Anticoagulants (acenocumarol or LMWH) | 45 (13.8%) | 40 (14.7%) | 0.753 |
| NOAC | 9 (2.8%) | 9 (3.3%) | 0.696 |
| GIB (n = 35) | No GIB (n = 563) | p-Value | |
|---|---|---|---|
| Age | 77.0 ± 8.2 | 74.0 ± 8.0 | 0.029 |
| Female | 15 (42.9%) | 213 (37.8%) | 0.553 |
| Hypertension | 23 (65.7%) | 445 (79.0%) | 0.064 |
| Diabetes | 14 (40.0%) | 190 (33.7%) | 0.449 |
| Permanent AF | 19 (54.3%) | 289 (51.3%) | 0.734 |
| Previous stroke | 7 (20.0%) | 181 (32.1%) | 0.133 |
| Previous bleeding | 26 (74.3%) | 365 (64.8%) | 0.254 |
| Previous ICH | 4 (11.4%) | 156 (27.7%) | 0.035 |
| Previous GI bleeding | 26 (74.3%) | 212 (37.7%) | <0.001 |
| Previous major bleeding | 16 (45.7%) | 259 (56.0%) | 0.973 |
| CHA2DS2-VASc * | 5 [1] | 4 [2] | 0.390 |
| HAS-BLED * | 4 [2] | 3 [1] | 0.016 |
| Anemia | 13 (37.1%) | 152 (27.0%) | 0.269 |
| Renal failure | 10 (28.6%) | 117 (20.8%) | 0.766 |
| AAS at discharge | 23 (65.7%) | 352 (62.3%) | 0.689 |
| Clopidogrel at discharge | 21 (60.0%) | 350 (62.2%) | 0.798 |
| AAS + Clopidogrel at discharge | 19 (54.3%) | 304 (54.0%) | 0.973 |
| Acenocumarol at discharge | 1 (2.9%) | 28 (5.0%) | 0.572 |
| LMWH at discharge | 2 (5.7%) | 54 (9.6%) | 0.445 |
| NOAC | 1 (2.9%) | 17 (3.0%) | 0.956 |
| Death in follow-up | 9 (25.7%) | 71 (12.6%) | 0.027 |
| Registry | EWOLUTION Registry | Multicenter Amplatzer | Amulet Registry | Ii Iberian Registry | Italian Registry |
|---|---|---|---|---|---|
| Population (n) | n = 1025 | n = 1047 | n = 1088 | n = 598 | n = 613 |
| Mean age | 73.4 ± 8.9 | 75 ± 8 | 74 ± 8 | 75.4 ± 8.6 | 75.1 ± 8.0 |
| Follow up (months) | 12 | 13 | 12 | 22.9 | 20 |
| CHA2DS2-VASc score (mean ± SD) | 4.5 ± 1.6 | 4.5 ± 1.6 | 4.5 ± 1.6 | 4.4 ± 1.5 | 4.2 ± 1.5 |
| HAS-BLED score (mean ± SD) | 2.3 ± 1.2 | 3.1 ± 1.2 | 3.3 ± 1.1 | 3.4 ± 1.2 | 3.2 ± 1.1 |
| Rate of events per 100 patient-years | |||||
| Deaths | 9.8% | 4.3% | 8.4% | 7% | 7.4% |
| History of Stroke | 30.5% | 39% | 28% | 39% | 36.3% |
| History of major Bleeding | 31% | 47.7% | 72% | 46% | 41.6% |
| Observed vs. Expected | |||||
| Stroke | 1.1% vs. 7.2% (CHA2DS2-VASc) RRR, 83% | 1.8% vs. 5.62% (CHA2DS2-VASc) RRR, 59% | 2.9 vs. 6.7% (CHA2DS2-VASc) RRR, 57% | 1.6% vs. 8.5% (CHA2DS2-VASc) RRR, 81% | 2.9% vs. 8.6% (CHA2DS2-VASc) RRR, 66% |
| Major bleeding | 2.7% vs. 5% (HAS-BLED) RRR, 46% | 2.1% vs. 5.34% (HAS-BLED) RRR, 46% | 7.1% vs. 10.3% | 3.9% vs. 6.4% (HAS-BLED) RRR, 39% | 4.5% vs. 6.3% (HAS-BLED) RRR, 29% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Mínguez, J.R.; Nogales-Asensio, J.M.; Infante De Oliveira, E.; Santos, L.; Ruiz-Salmerón, R.; Arzamendi-Aizpurua, D.; Costa, M.; Gutiérrez-García, H.; Fernández-Díaz, J.A.; Freixa, X.; et al. Major Bleeding Predictors in Patients with Left Atrial Appendage Closure: The Iberian Registry II. J. Clin. Med. 2020, 9, 2295. https://doi.org/10.3390/jcm9072295
López-Mínguez JR, Nogales-Asensio JM, Infante De Oliveira E, Santos L, Ruiz-Salmerón R, Arzamendi-Aizpurua D, Costa M, Gutiérrez-García H, Fernández-Díaz JA, Freixa X, et al. Major Bleeding Predictors in Patients with Left Atrial Appendage Closure: The Iberian Registry II. Journal of Clinical Medicine. 2020; 9(7):2295. https://doi.org/10.3390/jcm9072295
Chicago/Turabian StyleLópez-Mínguez, José Ramón, Juan Manuel Nogales-Asensio, Eduardo Infante De Oliveira, Lino Santos, Rafael Ruiz-Salmerón, Dabit Arzamendi-Aizpurua, Marco Costa, Hipólito Gutiérrez-García, Jose Antonio Fernández-Díaz, Xavier Freixa, and et al. 2020. "Major Bleeding Predictors in Patients with Left Atrial Appendage Closure: The Iberian Registry II" Journal of Clinical Medicine 9, no. 7: 2295. https://doi.org/10.3390/jcm9072295