Spread of ST348 Klebsiella pneumoniae Producing NDM-1 in a Peruvian Hospital

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Bacterial Samples and Study Population
2.2. Antimicrobial Susceptibility Testing
2.3. Detection and Characterization of Carbapenem Resistance Genes
2.4. Transferability and Epidemiological Studies
3. Results
3.1. Ethical Approval
3.2. Bacterial Samples and Study Population
3.3. Antimicrobial Susceptibility and Characterization of Carbapenem Resistance
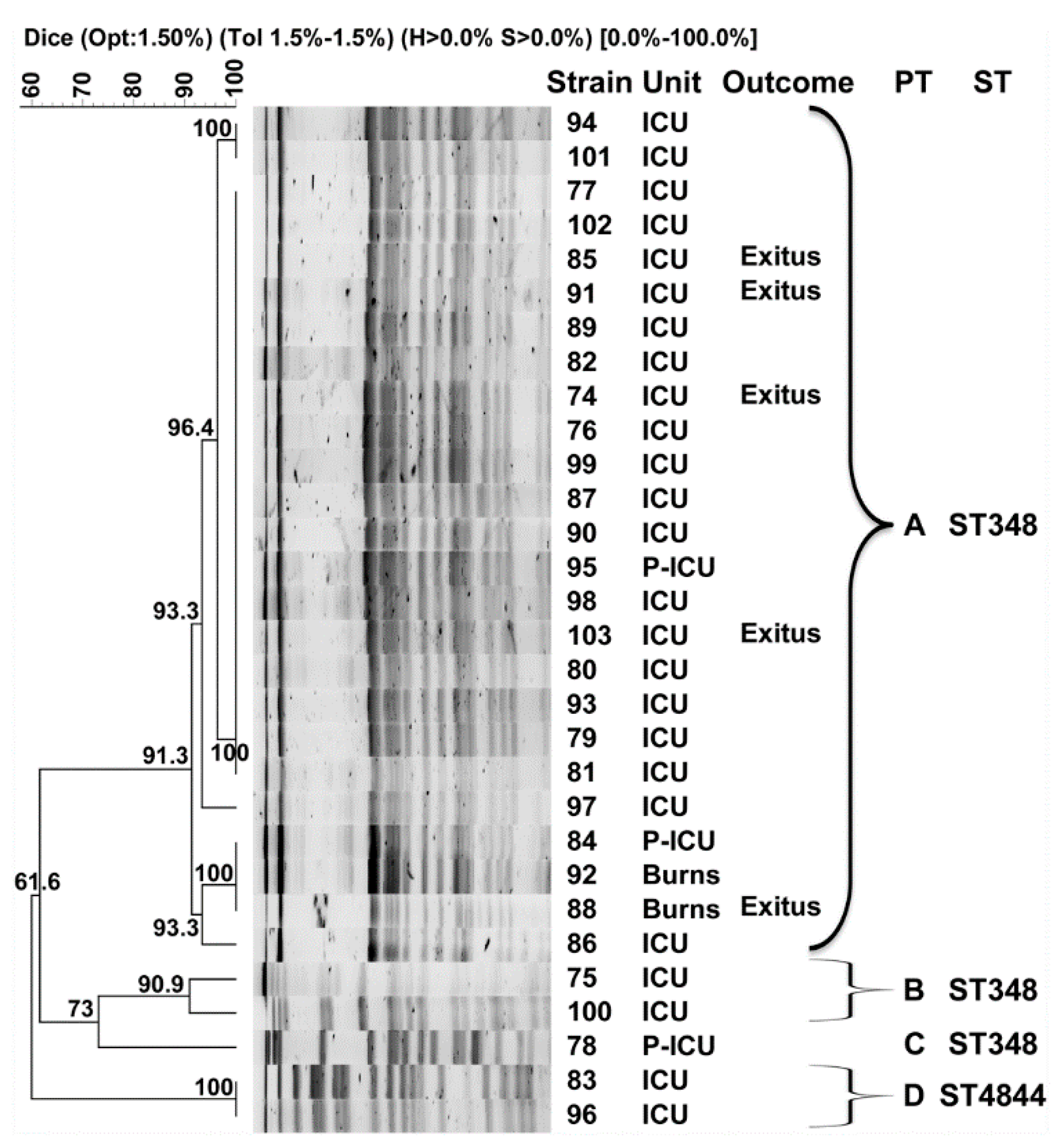
3.4. Transferability and Epidemiological Studies
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wyres, K.L.; Holt, K.E. Klebsiella pneumoniae as a key trafficker of drug resistance genes from environmental to clinically important bacteria. Curr. Opin. Microbiol. 2018, 45, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- De Rosa, F.G.; Corcione, S.; Cavallo, R.; Di Perri, G.; Bassetti, M. Critical issues for Klebsiella pneumoniae KPC-carbapenemase producing K. pneumoniae infections: A critical agenda. Future Microbiol. 2015, 10, 283–294. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Feng, Y.; Tang, G.; Qiao, F.; McNally, A.; Zong, Z. NDM Metallo-beta-Lactamases and Their Bacterial Producers in Health Care Settings. Clin. Microbiol. Rev. 2019, 32. [Google Scholar] [CrossRef] [Green Version]
- Iregui, A.; Ha, K.; Meleney, K.; Landman, D.; Quale, J. Carbapenemases in New York City: The continued decline of KPC-producing Klebsiella pneumoniae, but a new threat emerges. J. Antimicrob. Chemother. 2018, 73, 2997–3000. [Google Scholar] [CrossRef]
- Savov, E.; Politi, L.; Spanakis, N.; Trifonova, A.; Kioseva, E.; Tsakris, A. NDM-1 Hazard in the Balkan States: Evidence of the First Outbreak of NDM-1-Producing Klebsiella pneumoniae in Bulgaria. Microb. Drug Resist. 2018, 24, 253–259. [Google Scholar] [CrossRef]
- Hernandez-Garcia, M.; Perez-Viso, B.; Leon-Sampedro, R.; Navarro-San Francisco, C.; Lopez-Fresnena, N.; Diaz-Agero, C.; Morosini, M.I.; Ruiz-Garbajosa, P.; Canton, R. Outbreak of NDM-1+CTX-M-15+DHA-1-producing Klebsiella pneumoniae high-risk clone in Spain owing to an undetectable colonised patient from Pakistan. Int. J. Antimicrob. Agents 2019, 54, 233–239. [Google Scholar] [CrossRef]
- Chang, J.; Lee, J.Y.; Joo, J.Y.; Kim, K.; Park, H.Y.; Kim, S.H.; Choi, S.H.; Sung, H.; Kim, M.N. Emergence of NDM-4-producing Klebsiella pneumoniae in a Korean hospital due to a patient hospitalized in Vietnam and case review. J. Infect. Chemother. 2019, 25, 909–912. [Google Scholar] [CrossRef]
- Monteiro, J.; Inoue, F.M.; Lobo, A.P.T.; Ibanes, A.S.; Tufik, S.; Kiffer, C.R.V. A major monoclonal hospital outbreak of NDM-1-producing Klebsiella pneumoniae ST340 and the first report of ST2570 in Brazil. Infect. Control Hosp. Epidemiol. 2019, 40, 492–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanegas, J.M.; Parra, O.L.; Jimenez, J.N. Molecular epidemiology of carbapenem resistant gram-negative bacilli from infected pediatric population in tertiary—Care hospitals in Medellin, Colombia: An increasing problem. BMC Infect. Dis. 2016, 16, 463. [Google Scholar] [CrossRef] [Green Version]
- Pasteran, F.; Albornoz, E.; Faccone, D.; Gomez, S.; Valenzuela, C.; Morales, M.; Estrada, P.; Valenzuela, L.; Matheu, J.; Guerriero, L.; et al. Emergence of NDM-1-producing Klebsiella pneumoniae in Guatemala. J. Antimicrob. Chemother. 2012, 67, 1795–1797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Resurreccion-Delgado, C.; Montenegro-Idrogo, J.J.; Chiappe-Gonzalez, A.; Vargas-Gonzales, R.; Cucho-Espinoza, C.; Mamani-Condori, D.H.; Huaroto-Valdivia, L.M. Klebsiella pneumoniae New Delhi metallo-lactamase in a peruvian National hospital. Rev. Peru. Med. Exp. Salud Publica 2017, 34, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Levy-Blitchtein, S.; Roca, I.; Plasencia-Rebata, S.; Vicente-Taboada, W.; Velasquez-Pomar, J.; Muñoz, L.; Moreno-Morales, J.; Pons, M.J.; Del Valle-Mendoza, J.; Vila, J. Emergence and spread of carbapenem-resistant Acinetobacter baumannii international clones II and III in Lima, Peru. Emerg. Microbes Infect. 2018, 7, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, C.; Astocondor, L.; Rojo-Bezares, B.; Jacobs, J.; Saenz, Y. Molecular Characterization of Extended-Spectrum beta-Lactamase-Producer Klebsiella pneumoniae Isolates Causing Neonatal Sepsis in Peru. Am. J. Trop. Med. Hyg. 2016, 94, 285–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adrianzen, D.; Arbizu, A.; Ortiz, J.; Samalvides, F. Mortality caused by bacteremia Escherichia coli and Klebsiella spp. extended-spectrum beta-lactamase- producers: A retrospective cohort from a hospital in Lima, Peru. Rev. Peru. Med. Exp. Salud Publica 2013, 30, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Turlej-Rogacka, A.; Xavier, B.B.; Janssens, L.; Lammens, C.; Zarkotou, O.; Pournaras, S.; Goossens, H.; Malhotra-Kumar, S. Evaluation of colistin stability in agar and comparison of four methods for MIC testing of colistin. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 345–353. [Google Scholar] [CrossRef] [Green Version]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST). Recommendations for MIC Determination of Colistin (Polymyxin E) as Recommended by the Joint CLSI-EUCAST Polymyxin Breakpoints Working Group; EUCAST: Växjö, Sweden, 2016. [Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing; Twenty-Nine Informational Supplement, M100-S29; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2019. [Google Scholar]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST). Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 10.0; EUCAST: Växjö, Sweden, 2020. [Google Scholar]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Solé, M.; Pitart, C.; Roca, I.; Fàbrega, A.; Salvador, P.; Muñoz, L.; Oliveira, I.; Gascón, J.; Marco, F.; Vila, J. First Description of an Escherichia coli Strain Producing NDM-1 Carbapenemase in Spain. Antimicrob. Agents Chemother. 2011, 55, 4402–4404. [Google Scholar] [CrossRef] [Green Version]
- Bogaerts, P.; de Castro, R.R.; de Mendonca, R.; Huang, T.D.; Denis, O.; Glupczynski, Y. Validation of carbapenemase and extended-spectrum beta-lactamase multiplex endpoint PCR assays according to ISO 15189. J. Antimicrob. Chemother. 2013, 68, 1576–1582. [Google Scholar] [CrossRef] [Green Version]
- Siguier, P.; Perochon, J.; Lestrade, L.; Mahillon, J.; Chandler, M. ISfinder: The reference centre for bacterial insertion sequences. Nucleic Acids Res. 2006, 34, D32–D36. [Google Scholar] [CrossRef] [Green Version]
- Durmaz, R.; Otlu, B.; Koksal, F.; Hosoglu, S.; Ozturk, R.; Ersoy, Y.; Aktas, E.; Gursoy, N.C.; Caliskan, A. The optimization of a rapid pulsed-field gel electrophoresis protocol for the typing of Acinetobacter baumannii, Escherichia coli and Klebsiella spp. Jpn. J. Infect. Dis. 2009, 62, 372–377. [Google Scholar] [PubMed]
- Diancourt, L.; Passet, V.; Verhoef, J.; Grimont, P.A.; Brisse, S. Multilocus sequence typing of Klebsiella pneumoniae nosocomial isolates. J. Clin. Microbiol. 2005, 43, 4178–4182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacsaquispe-Contreras, R.; Bailon-Calderon, H. Identification of carbapenem-resistant genes in enterobacteria from peruvian hospitals, 2013-2017. Rev. Peru. Med. Exp. Salud Publica 2018, 35, 259–264. [Google Scholar] [CrossRef]
- Tamariz, J.; Llanos, C.; Seas, C.; Montenegro, P.; Lagos, J.; Fernandes, M.R.; Cerdeira, L.; Lincopan, N. Draft Genome Sequence of the First New Delhi Metallo-beta-Lactamase (NDM-1)-Producing Escherichia coli Strain Isolated in Peru. Genome Announc. 2018, 6. [Google Scholar] [CrossRef] [Green Version]
- Rocha, C.; Bernal, M.; Canal, E.; Rios, P.; Meza, R.; Lopez, M.; Burga, R.; Abadie, R.; Pizango, M.; Diaz, E.; et al. First Report of New Delhi Metallo-beta-Lactamase Carbapenemase-Producing Acinetobacter baumannii in Peru. Am. J. Trop. Med. Hyg. 2019, 100, 529–531. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Mathema, B.; Chavda, K.D.; DeLeo, F.R.; Bonomo, R.A.; Kreiswirth, B.N. Carbapenemase-producing Klebsiella pneumoniae: Molecular and genetic decoding. Trends Microbiol. 2014, 22, 686–696. [Google Scholar] [CrossRef] [Green Version]
- Vubil, D.; Figueiredo, R.; Reis, T.; Canha, C.; Boaventura, L.; Da Silva , G.J. Outbreak of KPC-3-producing ST15 and ST348 Klebsiella pneumoniae in a Portuguese hospital. Epidemiol. Infect. 2017, 145, 595–599. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, C.; Bavlovic, J.; Machado, E.; Amorim, J.; Peixe, L.; Novais, A. KPC-3-Producing Klebsiella pneumoniae in Portugal Linked to Previously Circulating Non-CG258 Lineages and Uncommon Genetic Platforms (Tn4401d-IncFIA and Tn4401d-IncN). Front. Microbiol. 2016, 7, 1000. [Google Scholar] [CrossRef] [Green Version]
- Fasciana, T.; Gentile, B.; Aquilina, M.; Ciammaruconi, A.; Mascarella, C.; Anselmo, A.; Fortunato, A.; Fillo, S.; Petralito, G.; Lista, F.; et al. Co-existence of virulence factors and antibiotic resistance in new Klebsiella pneumoniae clones emerging in south of Italy. BMC Infect. Dis. 2019, 19, 928. [Google Scholar] [CrossRef] [Green Version]
- Prado-Vivar, M.B.; Ortiz, L.; Reyes, J.; Villacis, E.; Fornasini, M.; Baldeon, M.E.; Cardenas, P.A. Molecular typing of a large nosocomial outbreak of KPC-producing bacteria in the biggest tertiary-care hospital of Quito, Ecuador. J. Glob. Antimicrob. Resist. 2019, 19, 328–332. [Google Scholar] [CrossRef]
- Wang, Z.; Li, M.; Shen, X.; Wang, L.; Liu, L.; Hao, Z.; Duan, J.; Yu, F. Outbreak of blaNDM-5-Harboring Klebsiella pneumoniae ST290 in a Tertiary Hospital in China. Microb. Drug Resist. 2019, 25, 1443–1448. [Google Scholar] [CrossRef] [PubMed]
- Seara, N.; Oteo, J.; Carrillo, R.; Perez-Blanco, V.; Mingorance, J.; Gomez-Gil, R.; Herruzo, R.; Perez-Vazquez, M.; Astray, J.; Garcia-Rodriguez, J.; et al. Interhospital spread of NDM-7-producing Klebsiella pneumoniae belonging to ST437 in Spain. Int. J. Antimicrob. Agents 2015, 46, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Hopkins, K.L.; Turton, J.; Doumith, M.; Hill, R.; Loy, R.; Meunier, D.; Pike, R.; Livermore, D.M.; Woodford, N. NDM carbapenemases in the United Kingdom: An analysis of the first 250 cases. J. Antimicrob. Chemother. 2014, 69, 1777–1784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haller, S.; Kramer, R.; Becker, K.; Bohnert, J.A.; Eckmanns, T.; Hans, J.B.; Hecht, J.; Heidecke, C.D.; Hubner, N.O.; Kramer, A.; et al. Extensively drug-resistant Klebsiella pneumoniae ST307 outbreak, north-eastern Germany, June to October 2019. Eurosurveillance 2019, 24, 1900734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, T.A.; Marr, C.M. Hypervirulent Klebsiella pneumoniae. Clin. Microbiol. Rev. 2019, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Strain | MIC (mg/L) | PT | ST | NDM | CTX-M | Inc | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IPM | MEM | CAZ | CZA | CTX | FEP | ATM | GEN | AMK | TOB | CIP | LVX | TGC | CST a | ||||||
| 79 | 8 | 16 | >256 | >256 | >32 | 16 | 96 | 32 | 3 | 16 | 2 | 0.5 | 2 | 2 | A | 348 | + | + | A/C, FIIk, FIB-KN, FIB-M |
| 100 | 12 | 16 | >256 | >256 | >32 | 16 | 16 | 64 | 3 | 32 | >32 | 12 | 1 | 2 | B | 348 | + | + | A/C, FIA, FIB, FIB-M |
| 78 | 16 | 16 | >256 | >256 | >32 | 24 | 24 | 64 | 3 | 16 | 4 | 1 | 1 | 2 | C | 348 | + | + | A/C, FIIk, FIB-KN, FIB-M |
| 83 | 4 | 8 | >256 | >256 | >32 | 16 | 32 | 48 | 2 | 16 | 6 | 2 | 4 | 2 | D | 4844 | + | + | A/C, FIIk, FIB-KN, FIB-M |
| 79t | 4 | 8 | >256 | >256 | >32 | 16 | 16 | 48 | 4 | 16 | 1 | 0.25 | 0.25 | ND | NA | NA | + | + | FIB-M |
| 100t | 8 | 6 | >256 | >256 | >32 | 12 | 12 | 64 | 6 | 16 | 1 | 0.25 | 0.25 | ND | NA | NA | + | + | FIB-M |
| 78t | 4 | 4 | >256 | >256 | >32 | 16 | 8 | 96 | 6 | 16 | 0.75 | 0.25 | 0.25 | ND | NA | NA | + | + | FIB-M |
| 83t | 8 | 8 | >256 | >256 | >32 | 24 | 8 | 64 | 4 | 24 | 1 | 0.25 | 0.25 | ND | NA | NA | + | + | FIB-M |
| MC1061 | 0.19 | 0.012 | 0.125 | ND | 0.047 | 0.023 | 0.094 | 0.25 | 2 | 0.25 | 0.008 | 0.023 | 0.25 | ND | NA | NA | - | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pons, M.J.; Marí-Almirall, M.; Ymaña, B.; Moya-Salazar, J.; Muñoz, L.; Sauñe, S.; Salazar-Hernández, R.; Vila, J.; Roca, I. Spread of ST348 Klebsiella pneumoniae Producing NDM-1 in a Peruvian Hospital. Microorganisms 2020, 8, 1392. https://doi.org/10.3390/microorganisms8091392
Pons MJ, Marí-Almirall M, Ymaña B, Moya-Salazar J, Muñoz L, Sauñe S, Salazar-Hernández R, Vila J, Roca I. Spread of ST348 Klebsiella pneumoniae Producing NDM-1 in a Peruvian Hospital. Microorganisms. 2020; 8(9):1392. https://doi.org/10.3390/microorganisms8091392
Chicago/Turabian StylePons, Maria J., Marta Marí-Almirall, Barbara Ymaña, Jeel Moya-Salazar, Laura Muñoz, Sharon Sauñe, Richard Salazar-Hernández, Jordi Vila, and Ignasi Roca. 2020. "Spread of ST348 Klebsiella pneumoniae Producing NDM-1 in a Peruvian Hospital" Microorganisms 8, no. 9: 1392. https://doi.org/10.3390/microorganisms8091392