Sodium and Salt Consumption in Latin America and the Caribbean: A Systematic-Review and Meta-Analysis of Population-Based Studies and Surveys

Abstract
:1. Introduction
2. Methods
2.1. Protocol
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Study Selection
2.5. Data Collation
2.6. Risk of Bias
2.7. Synthesis of Results
2.8. Ethics
3. Results
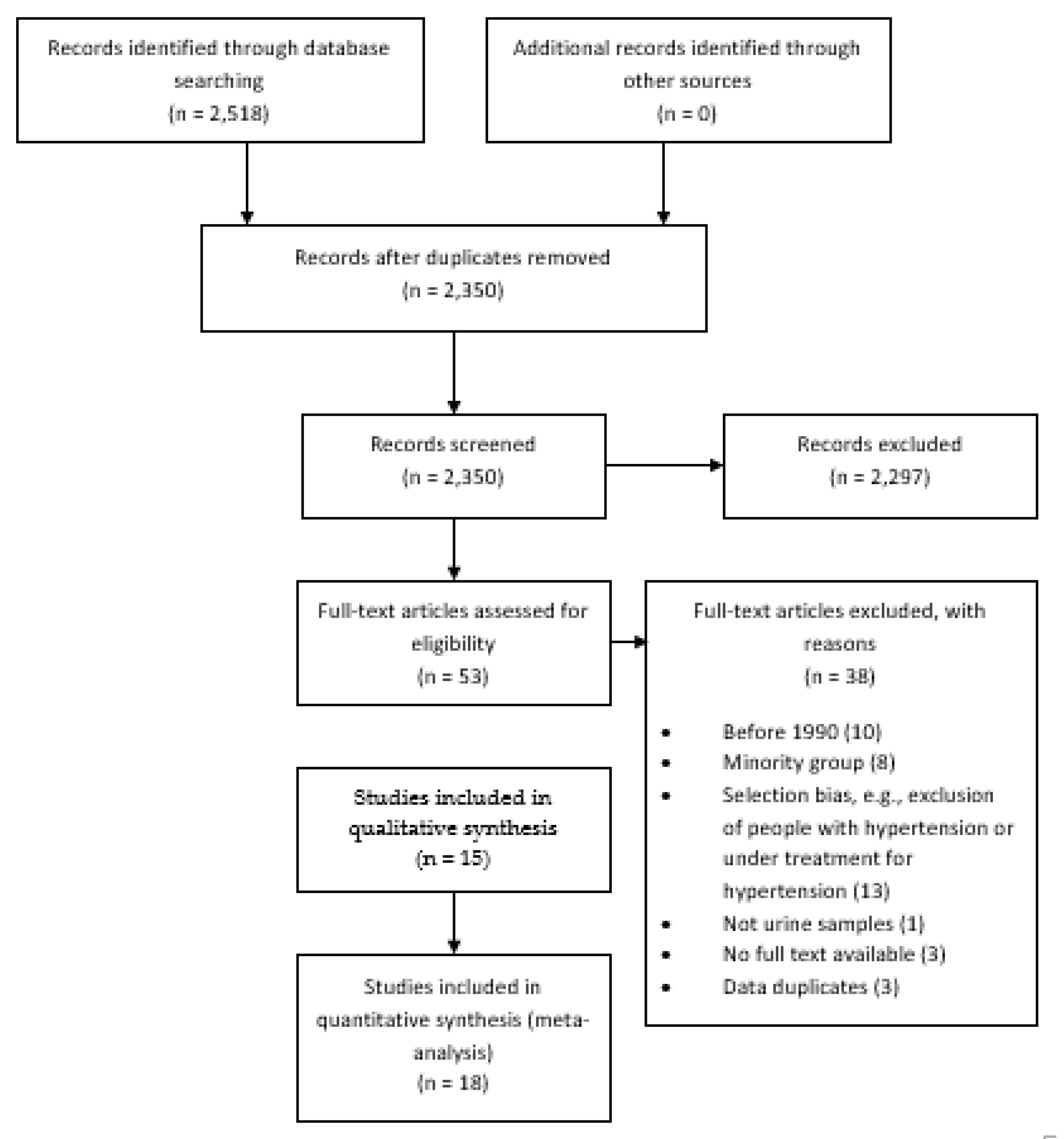
3.1. Study Selection
3.2. Study Characteristics
3.3. Quantitative Synthesis of Results
3.4. Risk of Bias
4. Discusion
4.1. Summary of Evidence
4.2. Results in Context
4.3. Limitations
4.4. Public Health Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- He, F.J.; Li, J.; Macgregor, G.A. Effect of longer-term modest salt reduction on blood pressure. Cochrane Database Syst. Rev. 2013, CD004937. [Google Scholar] [CrossRef] [PubMed]
- Poggio, R.; Gutierrez, L.; Matta, M.G.; Elorriaga, N.; Irazola, V.; Rubinstein, A. Daily sodium consumption and cvd mortality in the general population: Systematic review and meta-analysis of prospective studies. Public Health Nutr. 2015, 18, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Fahimi, S.; Singh, G.M.; Micha, R.; Khatibzadeh, S.; Engell, R.E.; Lim, S.; Danaei, G.; Ezzati, M.; Powles, J. Global sodium consumption and death from cardiovascular causes. N. Engl. J. Med. 2014, 371, 624–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the global burden of disease study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 acc/aha guideline on the primary prevention of cardiovascular disease: Executive summary: A report of the american college of cardiology/american heart association task force on clinical practice guidelines. J. Am. Coll. Cardiol. 2019, 74, 1376–1414. [Google Scholar] [CrossRef]
- World Health Organization. Salt Reduction. Available online: Https://www.Who.Int/news-room/fact-sheets/detail/salt-reduction (accessed on 19 February 2020).
- Powles, J.; Fahimi, S.; Micha, R.; Khatibzadeh, S.; Shi, P.; Ezzati, M.; Engell, R.E.; Lim, S.S.; Danaei, G.; Mozaffarian, D. Global, regional and national sodium intakes in 1990 and 2010: A systematic analysis of 24 h urinary sodium excretion and dietary surveys worldwide. BMJ Open 2013, 3, e003733. [Google Scholar] [CrossRef] [Green Version]
- Thout, S.R.; Santos, J.A.; McKenzie, B.; Trieu, K.; Johnson, C.; McLean, R.; Arcand, J.; Campbell, N.R.C.; Webster, J. The science of salt: Updating the evidence on global estimates of salt intake. J. Clin. Hypertens. (Greenwich) 2019, 21, 710–721. [Google Scholar] [CrossRef] [Green Version]
- Harris, R.M.; Rose, A.M.C.; Hambleton, I.R.; Howitt, C.; Forouhi, N.G.; Hennis, A.J.M.; Samuels, T.A.; Unwin, N. Sodium and potassium excretion in an adult caribbean population of african descent with a high burden of cardiovascular disease. BMC Public Health 2018, 18, 998. [Google Scholar] [CrossRef]
- Carbajal, H.A.; Salazar, M.R.; Riondet, B.; Rodrigo, H.F.; Quaini, S.M.; Rechifort, V.; Aizpurua, M.; Echeverria, R.F. [Associated variables to hypertension in a region of Argentina]. Medicina 2001, 61, 801–809. [Google Scholar]
- Lamelas, P.M.; Mente, A.; Diaz, R.; Orlandini, A.; Avezum, A.; Oliveira, G.; Lanas, F.; Seron, P.; Lopez-Jaramillo, P.; Camacho-Lopez, P.; et al. Association of urinary sodium excretion with blood pressure and cardiovascular clinical events in 17,033 Latin Americans. Am. J. Hypertens. 2016, 29, 796–805. [Google Scholar] [CrossRef] [Green Version]
- Moliterno, P.; Álvarez-Vaz, R.; Pécora, M.; Luzardo, L.; Borgarello, L.; Olascoaga, A.; Marino, C.; Noboa, O.; Staessen, J.A.; Boggia, J. Blood pressure in relation to 24-hour urinary sodium and potassium excretion in a uruguayan population sample. Int. J. Hypertens. 2018, 2018, 6956078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Pozo, G.; Davalos, P.; Yamori, Y. Cardiovascular risk factors in two Ecuadorian urban and rural populations. The ecuadorian-japan cooperative cardiac study group. J. Cardiovasc. Pharmacol. 1990, 16, S24–S25. [Google Scholar] [CrossRef] [PubMed]
- Perin, M.S.; Cornelio, M.E.; Oliveira, H.C.; Sao-Joao, T.M.; Rheaume, C.; Gallani, M.-C.B.J. Dietary sources of salt intake in adults and older people: A population-based study in a brazilian town. Public Health Nutr. 2019, 22, 1388–1397. [Google Scholar] [CrossRef] [PubMed]
- Mill, J.G.; Malta, D.C.; Machado, I.E.; Pate, A.; Pereira, C.A.; Jaime, P.C.; Szwarcwald, C.L.; Rosenfeld, L.G. Estimation of salt intake in the brazilian population: Results from the 2013 national health survey. Rev. Bras. Epidemiol. 2019, 22, E190009.SUPL. [Google Scholar]
- López-Rodríguez, G.; Galván-García, M.; Muzzo, B.S. Excreción urinaria de sodio en niños y adultos de una comuna de la región metropolitana de Santiago de Chile. Rev. Chil. Nutr. 2009, 36, 1139–1143. [Google Scholar] [CrossRef] [Green Version]
- Bisi Molina, M.d.C.; Cunha, R.d.S.; Herkenhoff, L.F.; Mill, J.G. [Hypertension and salt intake in an urban population]. Rev. Saude Publica 2003, 37, 743–750. [Google Scholar] [CrossRef] [Green Version]
- Cipullo, J.P.; Martin, J.F.; Vilela, O.; Ciorlia, L.A.d.S.; Godoy, M.R.P.d.; Cacao, J.C.; Loureiro, A.A.C.; Cesarino, C.B.; Carvalho, A.C.; Cordeiro, J.A.; et al. [Hypertension prevalence and risk factors in a Brazilian urban population]. Arq. Bras. Cardiol. 2010, 94, 519–526. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, S.L.; Souza Júnior, P.R.; Pimentel, E.B.; Baldo, M.P.; Malta, D.C.; Mill, J.G.; Szwarcwald, C.L. Relationship between salt consumption measured by 24-h urine collection and blood pressure in the adult population of vitória (Brazil). Braz. J. Med Biol. Res. 2015, 48, 728–735. [Google Scholar] [CrossRef]
- Costa, E.d.A.; Rose, G.A.; Kelin, C.H.; Leal, M.d.C.; Szwarcwald, C.L.; Bassanesi, S.L.; Achutti, A.C.; Fischman, A. Salt and blood pressure in rio grande do sul, Brasil. Bull. Pan Am. Health Organ. 1990, 24, 159–176. [Google Scholar]
- Petermann-Rocha, F.; Sillars, A.; Brown, R.; Sweeney, L.; Troncoso, C.; Garcia-Hermoso, A.; Leiva, A.M.; Martinez, M.A.; Diaz-Martinez, X.; Poblete-Valderrama, F.; et al. Sociodemographic patterns of urine sodium excretion and its association with hypertension in chile: A cross-sectional analysis. Public Health Nutr. 2019, 22, 2012–2021. [Google Scholar] [CrossRef] [Green Version]
- Carrillo-Larco, R.M.; Saavedra-Garcia, L.; Miranda, J.J.; Sacksteder, K.A.; Diez-Canseco, F.; Gilman, R.H.; Bernabe-Ortiz, A. Sodium and potassium consumption in a semi-urban area in peru: Evaluation of a population-based 24-hour urine collection. Nutrients 2018, 10, 245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campino, C.; Hill, C.; Baudr, R.; Martinez-Aguayo, A.; Aglony, M.; Carrasco, C.A.; Ferrada, C.; Loureiro, C.; Vecchiola, A.; Bancalari, R.; et al. Usefulness and pitfalls in sodium intake estimation: Comparison of dietary assessment and urinary excretion in Chilean children and adults. Am. J. Hypertens. 2016, 29, 1212–1217. [Google Scholar] [CrossRef] [PubMed]
- The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: Http://www.Ohri.Ca/programs/clinical_epidemiology/oxford.Asp (accessed on 7 January 2020).
- Kawasaki, T.; Itoh, K.; Uezono, K.; Sasaki, H. A simple method for estimating 24 h urinary sodium and potassium excretion from second morning voiding urine specimen in adults. Clin. Exp. Pharmacol. Physiol. 1993, 20, 7–14. [Google Scholar] [CrossRef]
- Tanaka, T.; Okamura, T.; Miura, K.; Kadowaki, T.; Ueshima, H.; Nakagawa, H.; Hashimoto, T. A simple method to estimate populational 24-h urinary sodium and potassium excretion using a casual urine specimen. J. Hum. Hypertens. 2002, 16, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Intersalt Co-Operative Research Group. Appendix tables. Centre-specific results by age and sex. J. Hum. Hypertens. 1989, 3, 331–407. [Google Scholar]
- Arcand, J.; Blanco-Metzler, A.; Benavides Aguilar, K.; L’Abbe, M.R.; Legetic, B. Sodium levels in packaged foods sold in 14 Latin American and Caribbean countries: A food label analysis. Nutrients 2019, 11, 369. [Google Scholar] [CrossRef] [Green Version]
- Webster, J.; Trieu, K.; Dunford, E.; Hawkes, C. Target salt 2025: A global overview of national programs to encourage the food industry to reduce salt in foods. Nutrients 2014, 6, 3274–3287. [Google Scholar] [CrossRef] [Green Version]
- Menyanu, E.; Russell, J.; Charlton, K. Dietary sources of salt in low- and middle-income countries: A systematic literature review. Int. J. Environ. Res. Public Health 2019, 16, 2082. [Google Scholar] [CrossRef] [Green Version]
- Pan American Health Organization. Technical Documents on Salt Reduction. Available online: Https://www.Paho.Org/hq/index.Php?Option=com_content&view=article&id=8669:Salt-reduction-technical-documents&itemid=39988&lang=en (accessed on 7 January 2020).
- World Health Organization. Shake the Salt Habit. The Shake Technical Package for Salt Reduction. Available online: Https://apps.Who.Int/iris/bitstream/handle/10665/250135/9789241511346-eng.Pdf?Sequence=1 (accessed on 7 January 2020).
- World Health Organization. NCD Global Monitoring Framework. Available online: Https://www.Who.Int/nmh/global_monitoring_framework/en/ (accessed on 7 January 2020).
- Brown, I.J.; Dyer, A.R.; Chan, Q.; Cogswell, M.E.; Ueshima, H.; Stamler, J.; Elliott, P. Estimating 24-hour urinary sodium excretion from casual urinary sodium concentrations in western populations: The intersalt study. Am. J. Epidemiol. 2013, 177, 1180–1192. [Google Scholar] [CrossRef] [Green Version]
- Mill, J.G.; Rodrigues, S.L.; Baldo, M.P.; Malta, D.C.; Szwarcwald, C.L. Validation study of the tanaka and kawasaki equations to estimate the daily sodium excretion by a spot urine sample. Rev. Bras. Epidemiol. 2015, 18 (Suppl. 2), 224–237. [Google Scholar] [CrossRef] [Green Version]
- Mente, A.; O’Donnell, M.J.; Dagenais, G.; Wielgosz, A.; Lear, S.A.; McQueen, M.J.; Jiang, Y.; Xingyu, W.; Jian, B.; Calik, K.B.; et al. Validation and comparison of three formulae to estimate sodium and potassium excretion from a single morning fasting urine compared to 24-h measures in 11 countries. J. Hypertens. 2014, 32, 1005–1014, discussion 1015. [Google Scholar] [CrossRef] [PubMed]
- Ji, C.; Sykes, L.; Paul, C.; Dary, O.; Legetic, B.; Campbell, N.R.; Cappuccio, F.P. Systematic review of studies comparing 24-hour and spot urine collections for estimating population salt intake. Rev. Panam. Salud Pública 2012, 32, 307–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidal-Petiot, E.; Joseph, A.; Resche-Rigon, M.; Boutten, A.; Mullaert, J.; d’Ortho, M.P.; Vrtovsnik, F.; Steg, P.G.; Flamant, M. External validation and comparison of formulae estimating 24-h sodium intake from a fasting morning urine sample. J. Hypertens. 2018, 36, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Campbell, N.R.C.; He, F.J.; Tan, M.; Cappuccio, F.P.; Neal, B.; Woodward, M.; Cogswell, M.E.; McLean, R.; Arcand, J.; MacGregor, G.; et al. The international consortium for quality research on dietary sodium/salt (true) position statement on the use of 24-hour, spot, and short duration (<24 hours) timed urine collections to assess dietary sodium intake. J. Clin. Hypertens. (Greenwich) 2019, 21, 700–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Author | Country | Type | Sample | Mean Age (Years) | Proportion Men (%) | Proportion HTN* (%) | Sodium Assessment | Collection Time |
|---|---|---|---|---|---|---|---|---|
| Carbajal, 2001 [10] | ARG | Community | 1225 | 37.06 | 35.83 | Results were multiplied by 3 (i.e., 24 h) | Overnight (from 23 h to 7 h) | |
| Lamelas, 2016 [11] | ARG | Community | 6529 | 51.10 | 39.00 | 51.60 | Kawasaki formula was used to estimate 24 h sodium excretion, surrogate of daily sodium consumption | Morning fasting midstream urine sample |
| Lamelas, 2016 [11] | BRA | Community | 5323 | 52.20 | 45.20 | 52.50 | Kawasaki formula was used to estimate 24 h sodium excretion, surrogate of daily sodium consumption | Morning fasting midstream urine sample |
| Lamelas, 2016 [11] | CHL | Community | 668 | 52.00 | 33.70 | 41.30 | Kawasaki formula was used to estimate 24 h sodium excretion, surrogate of daily sodium consumption | Morning fasting midstream urine sample |
| Lamelas, 2016 [11] | COL | Community | 4513 | 50.80 | 37.10 | 37.70 | Kawasaki formula was used to estimate 24 h sodium excretion, surrogate of daily sodium consumption | Morning fasting midstream urine sample |
| Moliterno 2018 [12] | URY | Community | 149 | 52.69 | 40.30 | 36.23 | As per urine samples | Participants were instructed to collect a 24 h urine sample |
| Del Pozo, 1990 [13] | ECU | Community | 332 | 47.59 | ~110/75 | |||
| Perin, 2018 [14] | BRA | Community | 517 | 53.50 | 41.60 | 44.50 | As per urine samples | Participants were instructed to collect a 24 h urine sample |
| Mill, 2019 [15] | BRA | National | 8083 | Tanaka formula was used to estimate the 24 h sodium excretion | Random sample (as long as the participant had gone at least 2 h without urinating | |||
| Lopez-Rodrigez, 2009 [16] | CHL | Community | 48 | 39.00 | 121.5/79.5 | Tanaka formula was used to estimate the 24 h sodium excretion | Random sample | |
| Bisi, 2003 [17] | BRA | Community | 1663 | 44.97 | 45.90 | 42.69 | As per urine samples (here multiplied by 2) | 12 h urine collection |
| Cipullo, 2010 [18] | BRA | Community | 1717 | 55.00 | 48.80 | 44.38 | As per urine samples | 12 h urine collection |
| Rodrigues, 2015 [19] | BRA | Community | 272 | 44.00 | 47.43 | 31.25 | As per urine samples | Participants were instructed to collect a 24 h urine sample |
| Costa, 1990 [20] | BRA | Community | 4565 | 11.75 | Grams of NaCl per day were estimated by the antilogarithm of the average log(Na/creatinine) of spot urine samples times 1.60 (adjustment for daily creatinine) times 0.058 | Random sample | ||
| Petermann-Rocha, 2019 [21] | CHL | National | 2913 | 46.47 | 41.74 | 128.4/76.5 | Tanaka formula was used to estimate the 24 h sodium excretion | Random sample |
| Carrillo-Larco, 2018 [22] | PER | Community | 409 | 45.70 | 44.00 | 17.00 | As per urine samples | Participants were instructed to collect a 24 h urine sample |
| Harris, 2018 [9] | BRB | National | 364 | 44.23 | 34.10 | As per urine samples | Participants were instructed to collect a 24 h urine sample | |
| Campino, 2016 [23] | CHL | Community | 135 | 41.2 | 48.15 | As per urine samples | Participants were instructed to collect a 24 h urine sample |
| Author | Country | Sodium (g/Day) | Salt (g/Day) |
|---|---|---|---|
| Carbajal, 2001 [10] | ARG | 3.02 | 7.68 |
| Lamelas, 2016 [11] | ARG | 4.66 | 11.84 |
| Lamelas, 2016 [11] | BRA | 4.57 | 11.61 |
| Lamelas, 2016 [11] | CHL | 4.88 | 12.40 |
| Lamelas, 2016 [11] | COL | 4.89 | 12.42 |
| Moliterno 2018 [12] | URY | 3.52 | 8.93 |
| Del Pozo, 1990 [13] | ECU | 4.63 | 11.75 |
| Perin, 2018 [14] | BRA | 4.13 | 10.50 |
| Mill, 2019 [15] | BRA | 3.68 | 9.34 |
| Lopez-Rodrigez, 2009 [16] | CHL | 4.10 | 10.41 |
| Bisi, 2003 [17] | BRA | 4.55 | 11.57 |
| Cipullo, 2010 [18] | BRA | Urinary sodium in normotensive: <100 mEq/L = 55.1%; 100–149 mEq/L = 25.8%; ≥150 mEq/L = 19.1%. Urinary sodium in hypertensive: <100 mEq/L = 43.5%; 100–149 mEq/L = 29.8%; ≥150 mEq/L = 26.7%. | |
| Rodrigues, 2015 [19] | BRA | 4.06 | 10.31 |
| Costa, 1990 [20] | BRA | 5.09 | 12.93 |
| Petermann-Rocha, 2019 [21] | CHL | 3.88 | 9.86 |
| Carrillo-Larco, 2018 [22] | PER | 4.40 | 11.18 |
| Harris, 2018 [9] | BRB | 2.66 | 6.76 |
| Campino, 2016 [23] | CHL | 4.16 | 10.57 |
| Coef | 95% confidence interval (p-value) | |
|---|---|---|
| Sodium analysis (ref: as per urine samples) | n = 12 | |
| Formula-based | 0.60 | −0.14; 1.36 (0.102) |
| Survey scope (ref: national) | n = 12 | |
| Community | 0.96 | 0.23; 1.68 (0.015) |
| Urine collection (ref: 24 h) | n = 12 | |
| Different than 24 h | 0.61 | −0.14; 1.36 (0.102) |
| Proportion of men (continuous) n = 11 | −0.06 | −0.17; 0.04 (0.196) |
| Mean age (continuous) n = 10 | 0.03 | −0.06; 0.11 (0.519) |
| Proportion of hypertension (continuous) n = 9 | 0.02 | −0.04; 0.08 (0.476) |
| Publication year (continuous) n = 12 | −0.26 | −0.53; −0.00 (0.049) |
| Author | Country | Representativeness | Selection | Ascertainment | Assessment |
|---|---|---|---|---|---|
| Carbajal, 2001 [10] | ARG | ||||
| Lamelas, 2016 [11] | ARG | ||||
| Lamelas, 2016 [11] | BRA | ||||
| Lamelas, 2016 [11] | CHL | ||||
| Lamelas, 2016 [11] | COL | ||||
| Moliterno 2018 [12] | URY | ||||
| Del Pozo, 1990 [13] | ECU | ||||
| Perin, 2018 [14] | BRA | ||||
| Mill, 2019 [15] | BRA | ||||
| Lopez-Rodrigez, 2009 [16] | CHL | ||||
| Bisi, 2003 [17] | BRA | ||||
| Cipullo, 2010 [18] | BRA | ||||
| Rodrigues, 2015 [19] | BRA | ||||
| Costa, 1990 [20] | BRA | ||||
| Petermann-Rocha, 2019 [21] | CHL | ||||
| Carrillo-Larco, 2018 [22] | PER | ||||
| Harris, 2018 [9] | BRB | ||||
| Campino, 2016 [23] | CHL |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrillo-Larco, R.M.; Bernabe-Ortiz, A. Sodium and Salt Consumption in Latin America and the Caribbean: A Systematic-Review and Meta-Analysis of Population-Based Studies and Surveys. Nutrients 2020, 12, 556. https://doi.org/10.3390/nu12020556
Carrillo-Larco RM, Bernabe-Ortiz A. Sodium and Salt Consumption in Latin America and the Caribbean: A Systematic-Review and Meta-Analysis of Population-Based Studies and Surveys. Nutrients. 2020; 12(2):556. https://doi.org/10.3390/nu12020556
Chicago/Turabian StyleCarrillo-Larco, Rodrigo M, and Antonio Bernabe-Ortiz. 2020. "Sodium and Salt Consumption in Latin America and the Caribbean: A Systematic-Review and Meta-Analysis of Population-Based Studies and Surveys" Nutrients 12, no. 2: 556. https://doi.org/10.3390/nu12020556