Effect of Flaxseed Intervention on Inflammatory Marker C-Reactive Protein: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
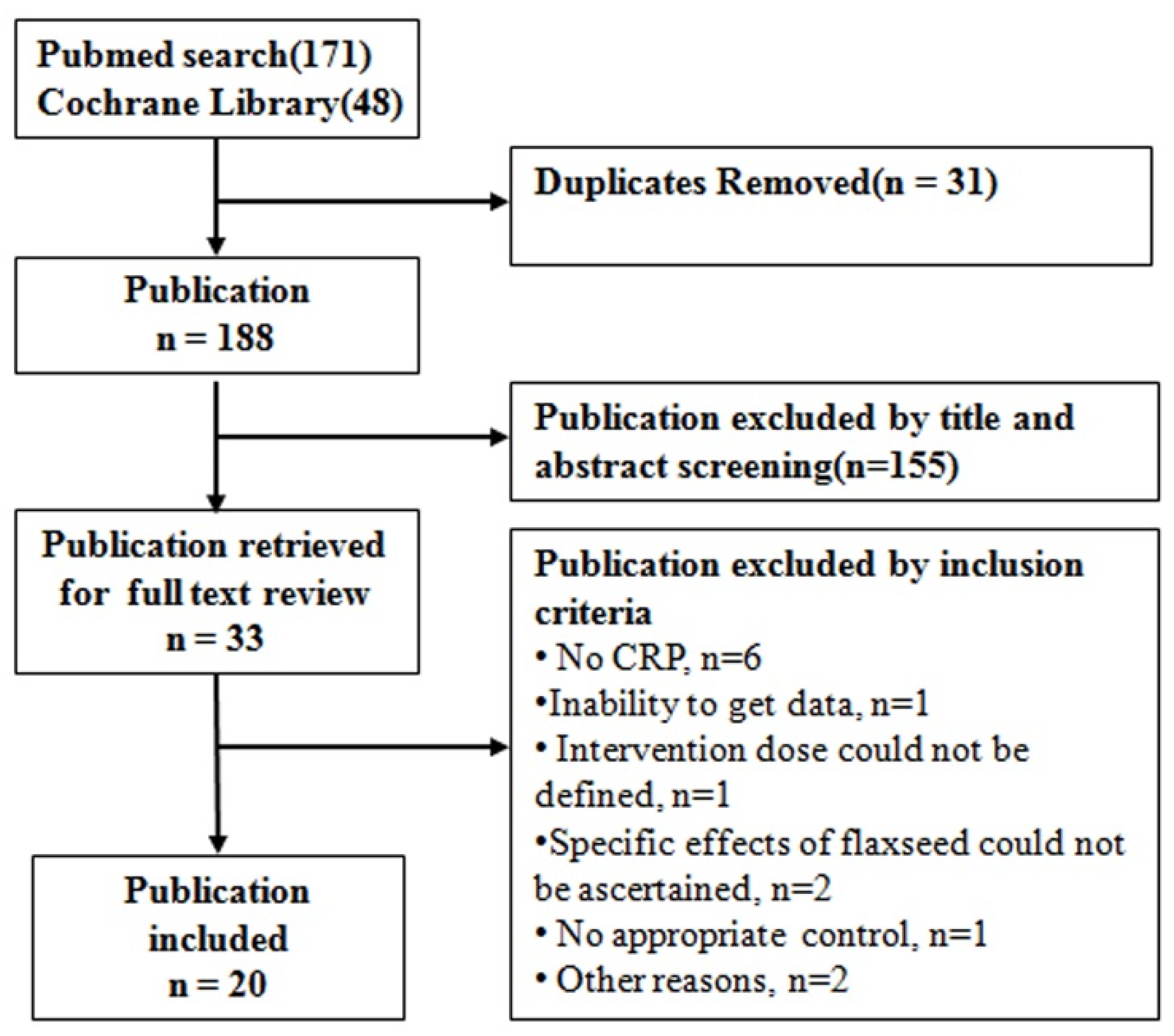
3.1. Study Selection
3.2. Characteristics of the Studies
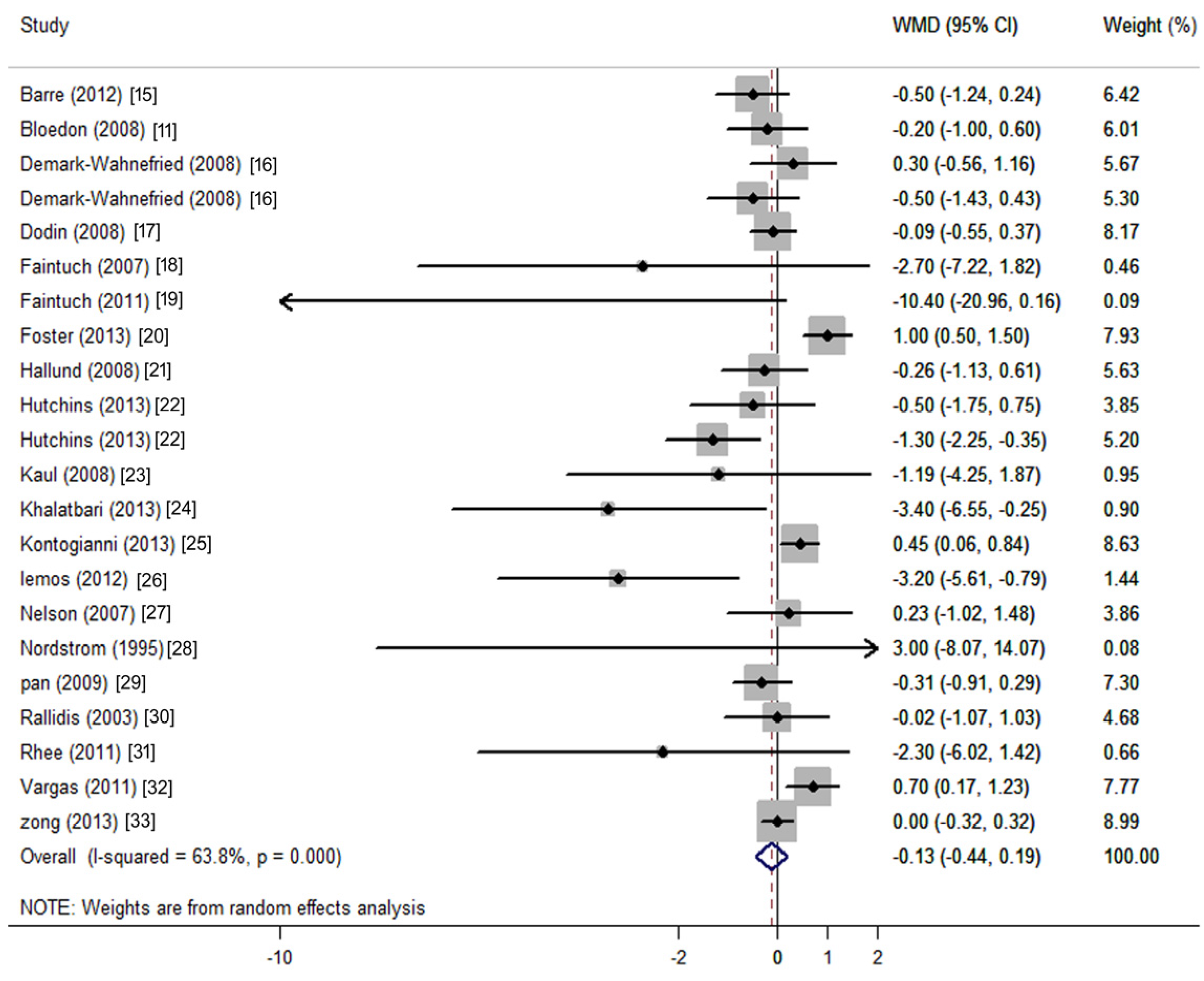
3.3. Changes in CRP Concentration
3.4. Subgroup and Meta-Regression Analysis for CRP
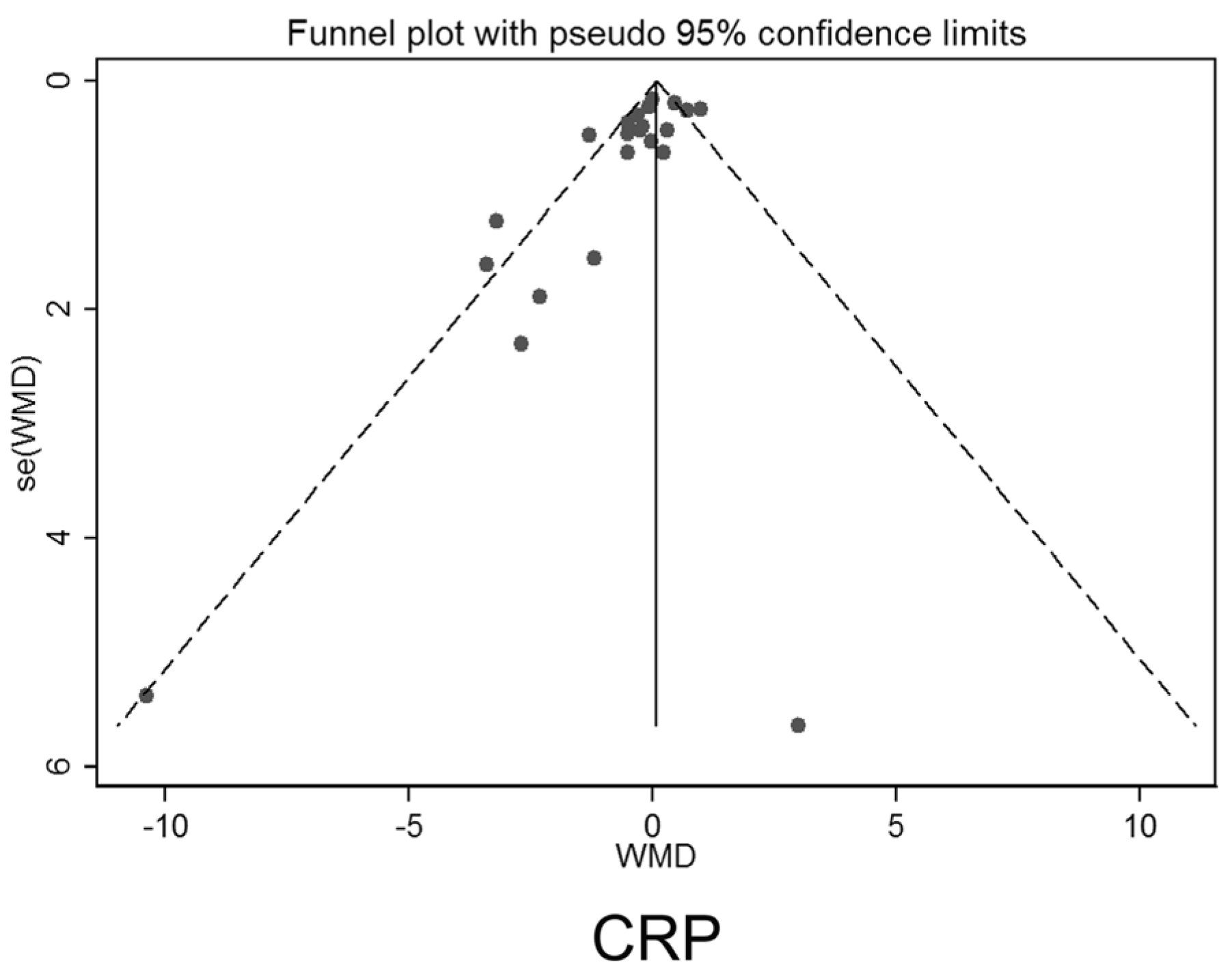
3.5. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kovacic, J.C.; Castellano, J.M.; Fuster, V. Cardiovascular defense challenges at the basic, clinical, and population levels. Ann. N. Y. Acad. Sci. 2012, 1254, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Esser, N.; Paquot, N.; Scheen, A.J. Anti-inflammatory agents to treat or prevent type 2 diabetes, metabolic syndrome and cardiovascular disease. Expert Opin. Investig. Drugs 2015, 24, 283–307. [Google Scholar] [CrossRef] [PubMed]
- Kaptoge, S.; Di Angelantonio, E.; Lowe, G.; Pepys, M.B.; Thompson, S.G.; Collins, R.; Danesh, J. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: An individual participant meta-analysis. Lancet 2010, 375, 132–140. [Google Scholar] [PubMed]
- Kaptoge, S.; Seshasai, S.R.; Gao, P.; Freitag, D.F.; Butterworth, A.S.; Borglykke, A.; Di Angelantonio, E.; Gudnason, V.; Rumley, A.; Lowe, G.D.; et al. Inflammatory cytokines and risk of coronary heart disease: New prospective study and updated meta-analysis. Eur. Heart J. 2014, 35, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Yoshimura, Y.; Kamada, C.; Tanaka, S.; Horikawa, C.; Okumura, R.; Ito, H.; Ohashi, Y.; Akanuma, Y.; Yamada, N.; et al. Intakes of dietary fiber, vegetables, and fruits and incidence of cardiovascular disease in japanese patients with type 2 diabetes. Diabetes Care 2013, 36, 3916–3922. [Google Scholar] [CrossRef] [PubMed]
- Kris-Etherton, P.M.; Harris, W.S.; Appel, L.J. Fish consumption, fish oil, omega-3 fatty acids, and cardiovascular disease. Circulation 2002, 106, 2747–2757. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Yu, D.; Demark-Wahnefried, W.; Franco, O.H.; Lin, X. Meta-analysis of the effects of flaxseed interventions on blood lipids. Am. J. Clin. Nutr. 2009, 90, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Paoletti, R.; Gotto, A.M., Jr.; Hajjar, D.P. Inflammation in atherosclerosis and implications for therapy. Circulation 2004, 109, Iii20–Iii26. [Google Scholar] [CrossRef] [PubMed]
- Muir, A.D. Flax lignans—Analytical methods and how they influence our lunderstanding of biological activity. J. AOAC Int. 2006, 89, 1147–1157. [Google Scholar] [PubMed]
- Hall, C., 3rd; Tulbek, M.C.; Xu, Y. Flaxseed. Adv. Food Nutr. Res. 2006, 51, 1–97. [Google Scholar] [PubMed]
- Bloedon, L.T.; Balikai, S.; Chittams, J.; Cunnane, S.C.; Berlin, J.A.; Rader, D.J.; Szapary, P.O. Flaxseed and cardiovascular risk factors: Results from a double blind, randomized, controlled clinical trial. J. Am. Coll. Nutr. 2008, 27, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Jangale, N.M.; Devarshi, P.P.; Dubal, A.A.; Ghule, A.E.; Koppikar, S.J.; Bodhankar, S.L.; Chougale, A.D.; Kulkarni, M.J.; Harsulkar, A.M. Dietary flaxseed oil and fish oil modulates expression of antioxidant and inflammatory genes with alleviation of protein glycation status and inflammation in liver of streptozotocin-nicotinamide induced diabetic rats. Food Chem. 2013, 141, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Yang, W.; Deng, Q.; Huang, Q.; Yang, J.; Huang, F. Flaxseed oil and alpha-lipoic acid combination reduces atherosclerosis risk factors in rats fed a high-fat diet. Lipids Health Dis. 2012, 11, 148. [Google Scholar] [CrossRef] [PubMed]
- Nounou, H.A.; Deif, M.M.; Shalaby, M.A. Effect of flaxseed supplementation and exercise training on lipid profile, oxidative stress and inflammation in rats with myocardial ischemia. Lipids Health Dis. 2012, 11, 129. [Google Scholar] [CrossRef] [PubMed]
- Barre, D.E.; Mizier-Barre, K.A.; Stelmach, E.; Hobson, J.; Griscti, O.; Rudiuk, A.; Muthuthevar, D. Flaxseed lignan complex administration in older human type 2 diabetics manages central obesity and prothrombosis-an invitation to further investigation into polypharmacy reduction. J. Nutr. Metab. 2012, 2012, 585170. [Google Scholar] [CrossRef] [PubMed]
- Demark-Wahnefried, W.; Polascik, T.J.; George, S.L.; Switzer, B.R.; Madden, J.F.; Ruffin, M.T.; Snyder, D.C.; Owzar, K.; Hars, V.; Albala, D.M.; et al. Flaxseed supplementation (not dietary fat restriction) reduces prostate cancer proliferation rates in men presurgery. Cancer Epidemiol. Biomark. Prev. 2008, 17, 3577–3587. [Google Scholar] [CrossRef] [PubMed]
- Dodin, S.; Cunnane, S.C.; Masse, B.; Lemay, A.; Jacques, H.; Asselin, G.; Tremblay-Mercier, J.; Marc, I.; Lamarche, B.; Legare, F.; et al. Flaxseed on cardiovascular disease markers in healthy menopausal women: A randomized, double-blind, placebo-controlled trial. Nutrition 2008, 24, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Faintuch, J.; Horie, L.M.; Barbeiro, H.V.; Barbeiro, D.F.; Soriano, F.G.; Ishida, R.K.; Cecconello, I. Systemic inflammation in morbidly obese subjects: Response to oral supplementation with alpha-linolenic acid. Obes. Surg. 2007, 17, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Faintuch, J.; Bortolotto, L.A.; Marques, P.C.; Faintuch, J.J.; Franca, J.I.; Cecconello, I. Systemic inflammation and carotid diameter in obese patients: Pilot comparative study with flaxseed powder and cassava powder. Nutr. Hosp. 2011, 26, 208–213. [Google Scholar] [PubMed]
- Foster, M.; Petocz, P.; Samman, S. Inflammation markers predict zinc transporter gene expression in women with type 2 diabetes mellitus. J. Nutr. Biochem. 2013, 24, 1655–1661. [Google Scholar] [CrossRef] [PubMed]
- Hallund, J.; Tetens, I.; Bugel, S.; Tholstrup, T.; Bruun, J.M. The effect of a lignan complex isolated from flaxseed on inflammation markers in healthy postmenopausal women. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Hutchins, A.M.; Brown, B.D.; Cunnane, S.C.; Domitrovich, S.G.; Adams, E.R.; Bobowiec, C.E. Daily flaxseed consumption improves glycemic control in obese men and women with pre-diabetes: A randomized study. Nutr. Res. 2013, 33, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Kaul, N.; Kreml, R.; Austria, J.A.; Richard, M.N.; Edel, A.L.; Dibrov, E.; Hirono, S.; Zettler, M.E.; Pierce, G.N. A comparison of fish oil, flaxseed oil and hempseed oil supplementation on selected parameters of cardiovascular health in healthy volunteers. J. Am. Coll. Nutr. 2008, 27, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Khalatbari, S.S.; Jamaluddin, R.; Tabibi, H.; Mohd Yusof, B.N.; Atabak, S.; Loh, S.P.; Rahmani, L. Effects of flaxseed consumption on systemic inflammation and serum lipid profile in hemodialysis patients with lipid abnormalities. Hemodial. Int. 2013, 17, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Kontogianni, M.D.; Vlassopoulos, A.; Gatzieva, A.; Farmaki, A.E.; Katsiougiannis, S.; Panagiotakos, D.B.; Kalogeropoulos, N.; Skopouli, F.N. Flaxseed oil does not affect inflammatory markers and lipid profile compared to olive oil, in young, healthy, normal weight adults. Metab. Clin. Exp. 2013, 62, 686–693. [Google Scholar] [CrossRef] [PubMed]
- Lemos, J.R.; Alencastro, M.G.; Konrath, A.V.; Cargnin, M.; Manfro, R.C. Flaxseed oil supplementation decreases c-reactive protein levels in chronic hemodialysis patients. Nutr. Res. 2012, 32, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Nelson, T.L.; Stevens, J.R.; Hickey, M.S. Inflammatory markers are not altered by an eight week dietary alpha-linolenic acid intervention in healthy abdominally obese adult males and females. Cytokine 2007, 38, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Nordstrom, D.C.; Honkanen, V.E.; Nasu, Y.; Antila, E.; Friman, C.; Konttinen, Y.T. Alpha-linolenic acid in the treatment of rheumatoid arthritis. A double-blind, placebo-controlled and randomized study: Flaxseed vs. Safflower seed. Rheumatol. Int. 1995, 14, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Demark-Wahnefried, W.; Ye, X.; Yu, Z.; Li, H.; Qi, Q.; Sun, J.; Chen, Y.; Chen, X.; Liu, Y.; et al. Effects of a flaxseed-derived lignan supplement on c-reactive protein, il-6 and retinol-binding protein 4 in type 2 diabetic patients. Br. J. Nutr. 2009, 101, 1145–1149. [Google Scholar] [CrossRef] [PubMed]
- Rallidis, L.S.; Paschos, G.; Liakos, G.K.; Velissaridou, A.H.; Anastasiadis, G.; Zampelas, A. Dietary alpha-linolenic acid decreases c-reactive protein, serum amyloid a and interleukin-6 in dyslipidaemic patients. Atherosclerosis 2003, 167, 237–242. [Google Scholar] [CrossRef]
- Rhee, Y.; Brunt, A. Flaxseed supplementation improved insulin resistance in obese glucose intolerant people: A randomized crossover design. Nutr. J. 2011, 10, 44. [Google Scholar] [CrossRef] [PubMed]
- Vargas, M.L.; Almario, R.U.; Buchan, W.; Kim, K.; Karakas, S.E. Metabolic and endocrine effects of long-chain versus essential omega-3 polyunsaturated fatty acids in polycystic ovary syndrome. Metabolism 2011, 60, 1711–1718. [Google Scholar] [CrossRef] [PubMed]
- Zong, G.; Demark-Wahnefried, W.; Wu, H.; Lin, X. Effects of flaxseed supplementation on erythrocyte fatty acids and multiple cardiometabolic biomarkers among chinese with risk factors of metabolic syndrome. Eur. J. Nutr. 2013, 52, 1547–1551. [Google Scholar] [CrossRef] [PubMed]
- International Prospective Register of Systemic Reviews. http://www.crd.york.ac.uk/prospero (accessed on 4 November 2015).
- Adolphe, J.L.; Whiting, S.J.; Juurlink, B.H.; Thorpe, L.U.; Alcorn, J. Health effects with consumption of the flax lignan secoisolariciresinol diglucoside. Br. J. Nutr. 2010, 103, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Leyva, D.; Dupasquier, C.M.; McCullough, R.; Pierce, G.N. The cardiovascular effects of flaxseed and its omega-3 fatty acid, alpha-linolenic acid. Can. J. Cardiol. 2010, 26, 489–496. [Google Scholar] [CrossRef]
- Prasad, K. Flaxseed and cardiovascular health. J. Cardiovasc. Pharmacol. 2009, 54, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.; Dwyer, J.; Adlercreutz, H.; Scalbert, A.; Jacques, P.; McCullough, M.L. Dietary lignans: Physiology and potential for cardiovascular disease risk reduction. Nutr. Rev. 2010, 68, 571–603. [Google Scholar] [CrossRef] [PubMed]
- Bloedon, L.T.; Szapary, P.O. Flaxseed and cardiovascular risk. Nutr. Rev. 2004, 62, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Follmann, D.; Elliott, P.; Suh, I.; Cutler, J. Variance imputation for overviews of clinical trials with continuous response. J. Clin. Epidemiol. 1992, 45, 769–773. [Google Scholar] [CrossRef]
- Choi, J.; Joseph, L.; Pilote, L. Obesity and c-reactive protein in various populations: A systematic review and meta-analysis. Obes. Rev. 2013, 14, 232–244. [Google Scholar] [CrossRef] [PubMed]
- Singh, T.; Newman, A.B. Inflammatory markers in population studies of aging. Ageing Res. Rev. 2011, 10, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Dewell, A.; Marvasti, F.F.; Harris, W.S.; Tsao, P.; Gardner, C.D. Low- and high-dose plant and marine (n-3) fatty acids do not affect plasma inflammatory markers in adults with metabolic syndrome. J. Nutr. 2011, 141, 2166–2171. [Google Scholar] [CrossRef] [PubMed]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O., 3rd; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Markers of inflammation and cardiovascular disease: Application to clinical and public health practice: A statement for healthcare professionals from the centers for disease control and prevention and the american heart association. Circulation 2003, 107, 499–511. [Google Scholar] [PubMed]
- Schwab, U.; Lauritzen, L.; Tholstrup, T.; Haldorssoni, T.; Riserus, U.; Uusitupa, M.; Becker, W. Effect of the amount and type of dietary fat on cardiometabolic risk factors and risk of developing type 2 diabetes, cardiovascular diseases, and cancer: A systematic review. Food Nutr. Res. 2014, 58. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Huang, T.; Zheng, J.; Wu, K.; Li, D. Effect of marine-derived n-3 polyunsaturated fatty acids on c-reactive protein, interleukin 6 and tumor necrosis factor alpha: A meta-analysis. PLoS ONE 2014, 9, e88103. [Google Scholar]
- Taylor, C.G.; Noto, A.D.; Stringer, D.M.; Froese, S.; Malcolmson, L. Dietary milled flaxseed and flaxseed oil improve n-3 fatty acid status and do not affect glycemic control in individuals with well-controlled type 2 diabetes. J. Am. Coll. Nutr. 2010, 29, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Plourde, M.; Cunnane, S.C. Extremely limited synthesis of long chain polyunsaturates in adults: Implications for their dietary essentiality and use as supplements. Appl. Physiol. Nutr. Metab. 2007, 32, 619–634. [Google Scholar] [CrossRef] [PubMed]
- Haidari, F.; Mohammadshahi, M.; Borsi, S.H.; Haghighizadeh, M.H.; Malgard, S. Comparison of essential fatty acid intakes and serum levels of inflammatory factors between asthmatic and healthy adults: A case-control study. Iran. J. Allergy Asthma Immunol. 2014, 13, 335–342. [Google Scholar] [PubMed]
- Bjermo, H.; Iggman, D.; Kullberg, J.; Dahlman, I.; Johansson, L.; Persson, L.; Berglund, J.; Pulkki, K.; Basu, S.; Uusitupa, M.; et al. Effects of n-6 pufas compared with sfas on liver fat, lipoproteins, and inflammation in abdominal obesity: A randomized controlled trial. Am. J. Clin. Nutr. 2012, 95, 1003–1012. [Google Scholar] [CrossRef] [PubMed]
- Al-Lahham, S.H.; Peppelenbosch, M.P.; Roelofsen, H.; Vonk, R.J.; Venema, K. Biological effects of propionic acid in humans; metabolism, potential applications and underlying mechanisms. Biochim. Biophys. Acta 2010, 1801, 1175–1183. [Google Scholar] [CrossRef] [PubMed]
- Jiao, J.; Xu, J.Y.; Zhang, W.; Han, S.; Qin, L.Q. Effect of dietary fiber on circulating c-reactive protein in overweight and obese adults: A meta-analysis of randomized controlled trials. Int. J. Food Sci. Nutr. 2015, 66, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Scott, K.P.; Antoine, J.M.; Midtvedt, T.; van Hemert, S. Manipulating the gut microbiota to maintain health and treat disease. Microb. Ecol. Health Dis. 2015, 26, 25877. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Bouter, L.M.; McQuillan, G.M.; Wener, M.H.; Harris, T.B. Elevated c-reactive protein levels in overweight and obese adults. JAMA 1999, 282, 2131–2135. [Google Scholar] [CrossRef] [PubMed]
- Ursoniu, S.; Sahebkar, A.; Andrica, F.; Serban, C.; Banach, M. Effects of flaxseed supplements on blood pressure: A systematic review and meta-analysis of controlled clinical trial. Clin. Nutr. 2015. [Google Scholar] [CrossRef] [PubMed]
- Gould, A.L.; Davies, G.M.; Alemao, E.; Yin, D.D.; Cook, J.R. Cholesterol reduction yields clinical benefits: Meta-analysis including recent trials. Clin. Ther. 2007, 29, 778–794. [Google Scholar] [CrossRef] [PubMed]
- Sahebkar, A.; Serban, C.; Ursoniu, S.; Banach, M. Effect of garlic on plasma lipoprotein(a) concentrations: A systematic review and meta-analysis of randomized controlled clinical trials. Nutrition 2016, 32, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Serban, C.; Sahebkar, A.; Antal, D.; Ursoniu, S.; Banach, M. Effects of supplementation with green tea catechins on plasma C-reactive protein concentrations: A systematic review and meta-analysis of randomized controlled trials. Nutrition 2015, 31, 1061–1071. [Google Scholar] [CrossRef] [PubMed]
- Ursoniu, S.; Sahebkar, A.; Serban, M.C.; Banach, M. Lipid profile and glucose changes after supplementation with astaxanthin: A systematic review and meta-analysis of randomized controlled trials. Arch. Med. Sci. 2015, 11, 253–266. [Google Scholar] [CrossRef] [PubMed]
- Banach, M.; Rizzo, M.; Toth, P.P.; Farnier, M.; Davidson, M.H.; Al-Rasadi, K.; Aronow, W.S.; Athyros, V.; Djuric, D.M.; Ezhov, M.V.; et al. Statin intolerance—An attempt at a unified definition. Position paper from an International Lipid Expert Panel. Arch. Med. Sci. 2015, 11, 1–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Author, Publication Year and Reference Number | Enroll | Comp | Mean Age | Mean BMI | Sex Male | Intervention | WF | ALA | LIG | Duration | Patient Features | Jadad Score | Design | Diet Type |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | n | Years | % | g/Day | g/Day | mg/Day | ||||||||
| Barre, 2012 [15] | 24 | 16 | 62.2 | 31.2 | 0 | LIG/PLA | NA | NA | 600 | 12 | Overweight or obese | 3 | RC | Usual |
| Bloedon, 2008 [11] | 62 | 58 | 56.9 | 27.8 | 50 | GF/WB | 40.0 | 3.2 | 640.0 | 10 | Hypercholesterolemia | 4 | RP | LF LC |
| Demark-Wahnefried, 2008 [16] | 80 | 71 | 59.2 | 28.8 | 100 | WF/Control | 30.0 | NR | NR | 4.5 | Prostate cancer | 4 | RP | Usual |
| Demark-Wahnefried, 2008 [16] | 81 | 78 | 59.2 | 28.8 | 100 | WF/Control | 30.0 | NR | NR | 4.5 | Prostate cancer | 4 | RP | LF |
| Dodin, 2008 [17] | 199 | 177 | 54.7 | 26.2 | 0 | WF/WG | 40.0 | 9.1 | 21.0 | 52 | Healthy | 5 | RP | Usual |
| Faintuch, 2007 [18] | 24 | 24 | 40.8 | 47.1 | 17 | FF/MF | 30.0 | 5.0 | NR | 2 | Obese | 4 | RC | Usual |
| Faintuch, 2011 [19] | 20 | 18 | 46.3 | 44.9 | 17 | FF/CF | 60.0 | 10.0 | NR | 12 | Obese | 4 | RP | Usual |
| Foster, 2013 [20] | 20 | 20 | 65.0 | 28.6 | 0 | FXO/OO | NA | 1.2 | NA | 12 | T2DM | 4 | RP | Usual |
| Hallund, 2008 [21] | 23 | 22 | 61.0 | 24.1 | 0 | LIG/PLA | NA | NA | 500.0 | 6 | Healthy | 4 | RC | Usual |
| Hutchins, 2013 [22] | 41 | 25 | 58.6 | 30.4 | 44 | GF/0 | 13.0 | 2.9 | 59.0 | 12 | Overweight or obese | 3 | RP | Usual |
| Hutchins, 2013 [22] | 41 | 25 | 58.6 | 30.4 | 44 | GF/0 | 26.0 | 5.8 | 118.0 | 12 | Overweight or obese | 3 | RP | Usual |
| Kaul, 2008 [23] | 100 | 88 | 33.7 | 24.7 | 38 | FXO/SFO | NA | 1.0 | NA | 12 | Healthy | 3 | RP | Usual |
| Khalatbari, 2013 [24] | 30 | 30 | 54.2 | 26.3 | 53 | GF/Control | 40.0 | NR | NR | 8 | Hemodialysis patients | 3 | RP | Usual |
| Kontogianni, 2013 [25] | 53 | 37 | 25.6 | 21.9 | 21 | FXO/OO | NA | 8.0 | NA | 6 | Healthy | 2 | RC | Usual |
| Lemos, 2012 [26] | 160 | 114 | 57.0 | 24.7 | 58 | FXO/MO | NA | 2.0 | NA | 17 | Renal failure | 3 | RP | Usual |
| Nelson, 2007 [27] | 56 | 51 | 38.0 | 29.8 | 21 | FXO/Control | NA | 11.6 | NA | 8 | Overweight or obese | 2 | RP | Usual |
| Nordstrom, 1995 [28] | 22 | 22 | 52 | NR | NR | FXO/SAO | NA | 9.6 | NA | 12 | Rheumatoid arthritis | 3 | RP | Usual |
| Pan, 2009 [29] | 73 | 70 | 64 | 25.0 | 37 | LIG/PLA | NA | NA | 360.0 | 12 | T2DM | 5 | RC | Usual |
| Rallidis, 2003 [30] | 76 | 76 | 51.2 | 28.2 | 100 | FXO/SAO | NA | 8.0 | NA | 12 | Dyslipidaemic patients | 3 | RP | Usual |
| Rhee, 2011 [31] | 11 | 9 | 54.7 | 31.4 | 44 | GF/WB | 40 | NR | NR | 12 | Obese and glucose intolerant people | 2 | RC | Usual |
| Vargas, 2011 [32] | 34 | 34 | 34.1 | 29.2 | 0 | FXO/SOY | NA | 3.3 | NA | 6 | Polycystic ovary syndrome | 3 | RC | Usual |
| Zong, 2013 [33] | 189 | 173 | 48.8 | 25.3 | 56 | GF/0 | 30 | 7.0 | NR | 12 | Metabolic syndrome | 5 | RP | Usual |
| Subgroups | No. of Comparisons | Net Change (95% CI) | p for Interaction | I2 | p for Heterogeneity | Analysis Models |
|---|---|---|---|---|---|---|
| Type of intervention | ||||||
| Whole flaxseed | 11 | −0.35 (−0.75, 0.05) | 0.008 | 46.3% | 0.045 | Random-effect |
| Flaxseed oil | 8 | 0.39 (−0.09, 0.87) | 55.6% | 0.027 | Random-effect | |
| Lignan | 3 | −0.36 (−0.77, 0.05) | 0.00% | 0.089 | Fixed-effect | |
| Dose of whole flaxseed | ||||||
| <40 g | 6 | −0.34 (−0.85, 0.17) | 0.258 | 47.9% | 0.087 | Random-effect |
| ≥40 g | 5 | −0.63 (−1.62, 0.36) | 55.4% | 0.062 | Random-effect | |
| CRP | ||||||
| <10 mg/L | 19 | −0.10 (−0.41, 0.21) | 0.064 | 65.7% | <0.0001 | Random-effect |
| ≥10 mg/L | 3 | −3.04 (−6.93, 0.85) | 34.1% | 0.220 | Fixed-effect | |
| BMI | ||||||
| <30 kg/m2 | 15 | 0.06 (−0.25, 0.37) | 0.032 | 63.6% | <0.0001 | Random-effect |
| ≥30 kg/m2 | 6 | −0.83 (−1.34, −0.31) | 21.8% | 0.270 | Fixed-effect | |
| Gender | ||||||
| Female | 4 | 0.30 (−0.34, 0.95) | 0.191 | 82.1% | 0.001 | Random-effect |
| Male | 3 | −0.06 (−0.60, 0.49) | 0.00% | 0.464 | Fixed-effect | |
| Both | 15 | −0.39 (−0.82, 0.04) | 57.6% | 0.003 | Random-effect | |
| Study design | ||||||
| Crossover | 7 | 0.01 (−0.47, 0.49) | 0.638 | 65.9% | 0.015 | Random-effect |
| Parallel | 15 | −0.23 (−0.66, 0.20) | 61.9% | <0.0001 | Random-effect | |
| Study duration | ||||||
| <12 weeks | 9 | 0.09 (−0.31, 0.50) | 0.649 | 48.9% | 0.048 | Random-effect |
| ≥12 weeks | 13 | −0.31 (−0.77, 0.16) | 69.1% | <0.0001 | Random-effect | |
| Sample size | ||||||
| <50 | 10 | −0.20 (−0.99, 0.58) | 0.710 | 69.4% | 0.001 | Random-effect |
| ≥50 | 12 | −0.15 (−0.45, 0.15) | 51.7% | 0.019 | Random-effect | |
| Age | ||||||
| <50 years | 7 | 0.27 (−0.17, 0.70) | 0.268 | 52.2% | 0.051 | Random-effect |
| ≥50 years | 15 | −0.32 (−0.74, 0.10) | 66.5% | <0.0001 | Random-effect | |
| Quality Score | ||||||
| <4 | 12 | −0.39 (−0.97, 0.20) | 0.902 | 68.1% | <0.0001 | Random-effect |
| ≥4 | 10 | −0.32 (−0.37, 0.37) | 61.6% | 0.005 | Random-effect |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ren, G.-Y.; Chen, C.-Y.; Chen, G.-C.; Chen, W.-G.; Pan, A.; Pan, C.-W.; Zhang, Y.-H.; Qin, L.-Q.; Chen, L.-H. Effect of Flaxseed Intervention on Inflammatory Marker C-Reactive Protein: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2016, 8, 136. https://doi.org/10.3390/nu8030136
Ren G-Y, Chen C-Y, Chen G-C, Chen W-G, Pan A, Pan C-W, Zhang Y-H, Qin L-Q, Chen L-H. Effect of Flaxseed Intervention on Inflammatory Marker C-Reactive Protein: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients. 2016; 8(3):136. https://doi.org/10.3390/nu8030136
Chicago/Turabian StyleRen, Guan-Yu, Chun-Yang Chen, Guo-Chong Chen, Wei-Guo Chen, An Pan, Chen-Wei Pan, Yong-Hong Zhang, Li-Qiang Qin, and Li-Hua Chen. 2016. "Effect of Flaxseed Intervention on Inflammatory Marker C-Reactive Protein: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Nutrients 8, no. 3: 136. https://doi.org/10.3390/nu8030136