
Uncommon Clinical Presentations of Sporotrichosis: A Two-Case Report

 , ,
, , 
{kind=link}
{kind=link}
Abstract
:1. Introduction
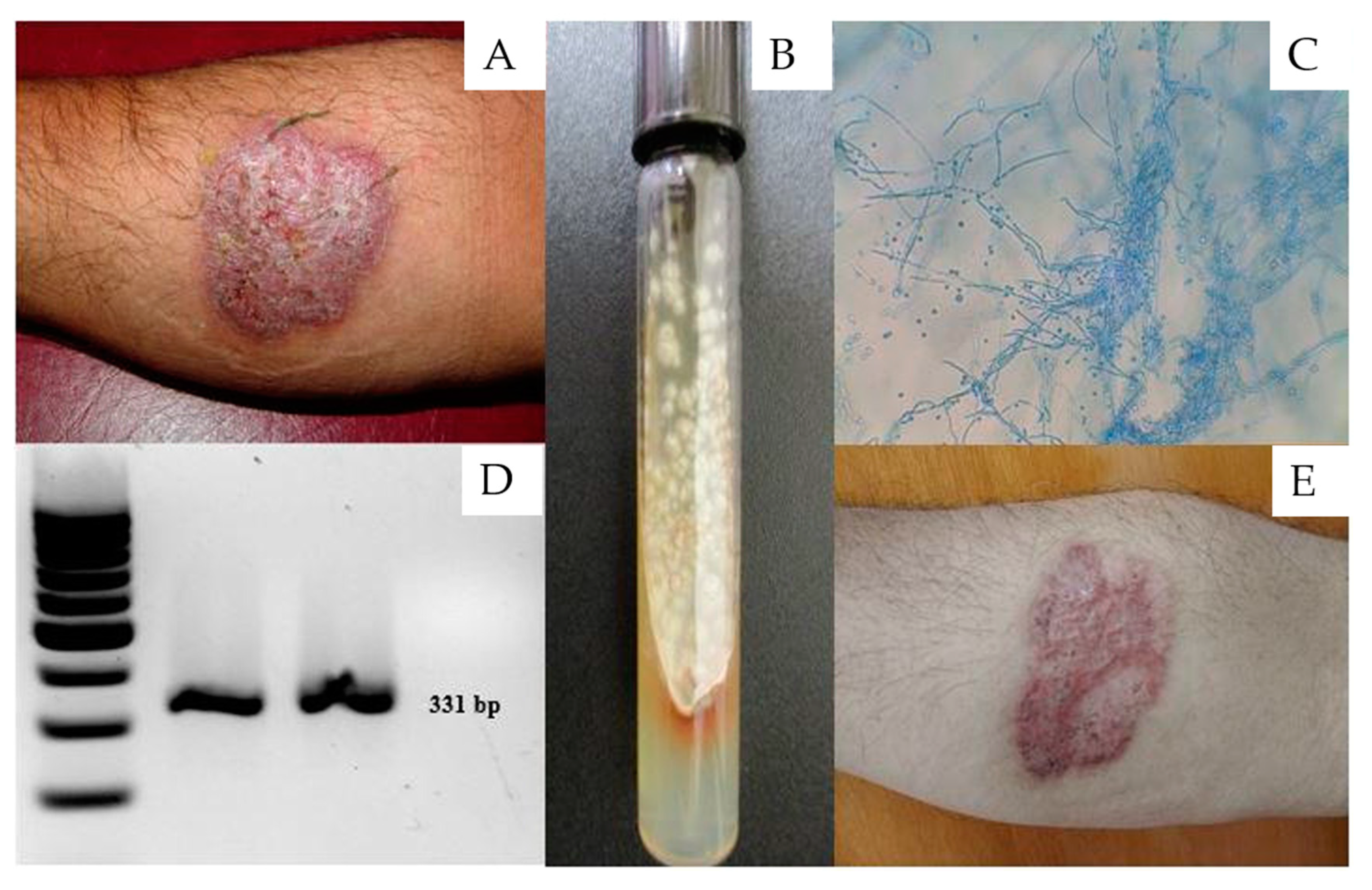
2. Case 1
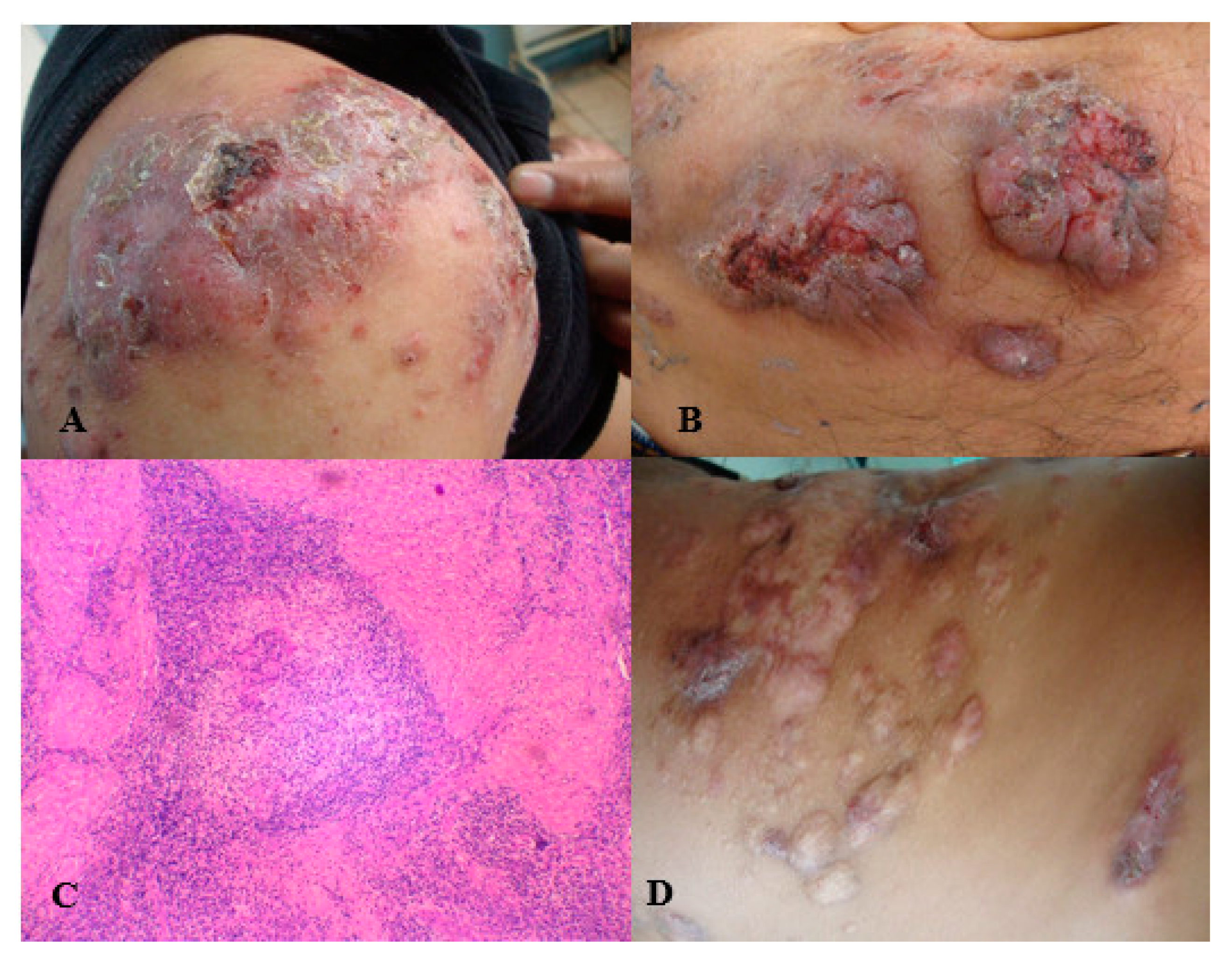
3. Case 2
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Arenas, R.; Sánchez-Cardenas, C.D.; Ramirez-Hobak, L.; Ruíz Arriaga, L.F.; Vega Memije, M.E. Sporotrichosis: From KOH to molecular biology. J. Fungi 2018, 4, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahajan, V.K. Sporotrichosis: An overview and therapeutic options. Dermatol. Res. Pract. 2014, 2014, 272376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, A.M.; de Hoog, G.S.; de Cássia Pires, D.; Brihante, R.S.N.; da Costa Sidrim, J.J.; Gadelha, M.F.; Colombo, A.L.; de Camargo, Z.P. Genetic diversity and antifungal susceptibility profiles in causative agents of sporotrichosis. BMC Infect. Dis. 2014, 14, 219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, A.; Mudenda, V.; Lakhi, S.; Ngalamika, O. A 27-year-old severely immunosuppressed female with misleading clinical features of disseminated cutaneous sporotrichosis. Case Rep. Dermatol. Med. 2016, 2016, 9403690. [Google Scholar] [CrossRef] [Green Version]
- Fischman, O.; Rodrigues, A.; Fernandes, G.; Bentubo, H.; de Camargo, Z.P.; Petri, V. Case report: Atypical clinical presentation of sporotrichosis caused by Sporothrix globosa resistant to itraconazole. Am. J. Trop. Med. Hyg. 2016, 94, 1218–1222. [Google Scholar]
- Monno, R.; Brindicci, G.; Romeo, O.; De Carolis, E.; Criseo, G.; Sanguinetti, M.; Fumarola, L.; Ingravallo, G.; Mariani, M.; Monno, L. Infection caused by Sporothrix schenckii: An autochthonous case in Bari, Southern Italy. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 2457–2460. [Google Scholar] [CrossRef] [PubMed]
- Marques, G.F.; Martins, A.L.; Sousa, J.M.; Brandão, L.S.; Wachholz, P.A.; Masuda, P.Y. Characterization of sporotrichosis cases treated in a dermatologic teaching unit in the state of São Paulo-Brazil, 2003–2013. An. Bras. Dermatol. 2015, 90, 273–275. [Google Scholar] [CrossRef] [Green Version]
- Barros, M.B.; de Almeida Paes, R.; Schubach, A.O. Sporothrix schenckii and sporotrichosis. Clin. Microbiol. Rev. 2011, 24, 633–654. [Google Scholar] [CrossRef] [Green Version]
- Moreira, J.A.; Freitas, D.F.; Lamas, C.C. The impact of sporotrichosis in HIV-infected patients: A systematic review. Infection 2015, 43, 267–276. [Google Scholar] [CrossRef] [PubMed]
- García-Carnero, L.C.; Lozaya-Pérez, N.E.; González-Hernández, S.E.; Martínez-Alvarez, J.A. Inmunity and treatment of sporotrichosis. J. Fungi 2018, 4, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, A.M.; de Hoog, G.S.; de Camargo, Z.P. Molecular diagnosis of pathogenic Sporothrix species. PLoS Negl. Trop. Dis. 2015, 9, e0004190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes-Bezerra, L.M.; Mora-Montes, H.M.; Zhang, Y.; Nino-Vega, G.; Rodrigues, A.M.; de Camargo, Z.P.; De Hoog, S. Sporotrichosis between 1898 and 2017: The evolution of knowledge on a changeable disease and on emerging etiological agents. Med. Mycol. 2018, 56 (Suppl. 1), 126–143. [Google Scholar] [CrossRef] [PubMed]
- Charles, K.; Lowe, L.; Shuman, E.; Cha, K.B. Painful linear ulcers: A case of cutaneous sporotrichosis mimicking pyoderma gangrenosum. JAAD Case Rep. 2017, 3, 519–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonifaz, A.; Vazquez-Gonzalez, D. Sporotrichosis: An update. G. Ital. Dermatol. Venereol. 2010, 145, 659–673. [Google Scholar] [PubMed]
- Yap, F.B. Disseminated cutaneous sporotrichosis in an immunocompetent individual. Int. J. Infect. Dis. 2011, 15, e727–e729. [Google Scholar] [CrossRef] [Green Version]
- Yagnik, K.J.; Skelton, W.P.; Olson, A.; Trillo, C.A.; Lascano, J. A rare case of disseminated Sporothrix schenckii with bone marrow involvement in a patient with idiopathic CD4 lymphocytopenia. IDCases 2017, 9, 70–72. [Google Scholar] [CrossRef] [PubMed]
- White, M.; Adams, L.T.; Phan, C.; Erdag, G.; Totten, M.; Lee, R.; Lu, X.; Mehta, S.; Miller, L.S.; Zhang, S.X.; et al. Disseminated sporotrichosis following iatrogenic immunosuppression for suspected pyoderma gangrenosum. Lancet Infect. Dis. 2019, 19, e385–e391. [Google Scholar] [CrossRef]
- Criseo, G.; Malara, G.; Romeo, O.; Guerra, A.P. Lymphocutaneous sporotrichosis in an immunocompetent patient: A case report from extreme southern Italy. Mycopathologia 2008, 166, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, V.K.; Sharma, N.L.; Shanker, V.; Gupta, P.; Mardi, K. Cutaneous sporotrichosis: Unusual clinical presentations. Indian J. Dermatol. Venereol. Leprol. 2010, 76, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Almeida-Paes, R.; de Oliveira, M.M.E.; Saraiva Freitas, D.F.; do Valle, A.C.F.; Zancopé-Oliveira, R.M.; Gutierrez-Galhardo, M.C. Sporothricosis in Rio de Janeiro, Brazil: Sporothrix braziliensis is associated with a tipical clinical presentation. PLoS Negl. Trop. Dis. 2014, 8, 3094. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Herrera, E.; Arenas, R.; Hernández-Castro, R.; Frías-De-León, M.G.; Rodríguez-Cerdeira, C. Uncommon Clinical Presentations of Sporotrichosis: A Two-Case Report. Pathogens 2021, 10, 1249. https://doi.org/10.3390/pathogens10101249
Martínez-Herrera E, Arenas R, Hernández-Castro R, Frías-De-León MG, Rodríguez-Cerdeira C. Uncommon Clinical Presentations of Sporotrichosis: A Two-Case Report. Pathogens. 2021; 10(10):1249. https://doi.org/10.3390/pathogens10101249
Chicago/Turabian StyleMartínez-Herrera, Erick, Roberto Arenas, Rigoberto Hernández-Castro, María Guadalupe Frías-De-León, and Carmen Rodríguez-Cerdeira. 2021. "Uncommon Clinical Presentations of Sporotrichosis: A Two-Case Report" Pathogens 10, no. 10: 1249. https://doi.org/10.3390/pathogens10101249