
Acceptability, Safety, and Efficacy of Oral Administration of Extracts of Black or Red Maca (Lepidium meyenii) in Adult Human Subjects: A Randomized, Double-Blind, Placebo-Controlled Study

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Composition of Spray-Dried Maca Extracts
2.2. Primary Outcomes: Efficacy of Maca Consumption on Several Variables Associated with Heath Status
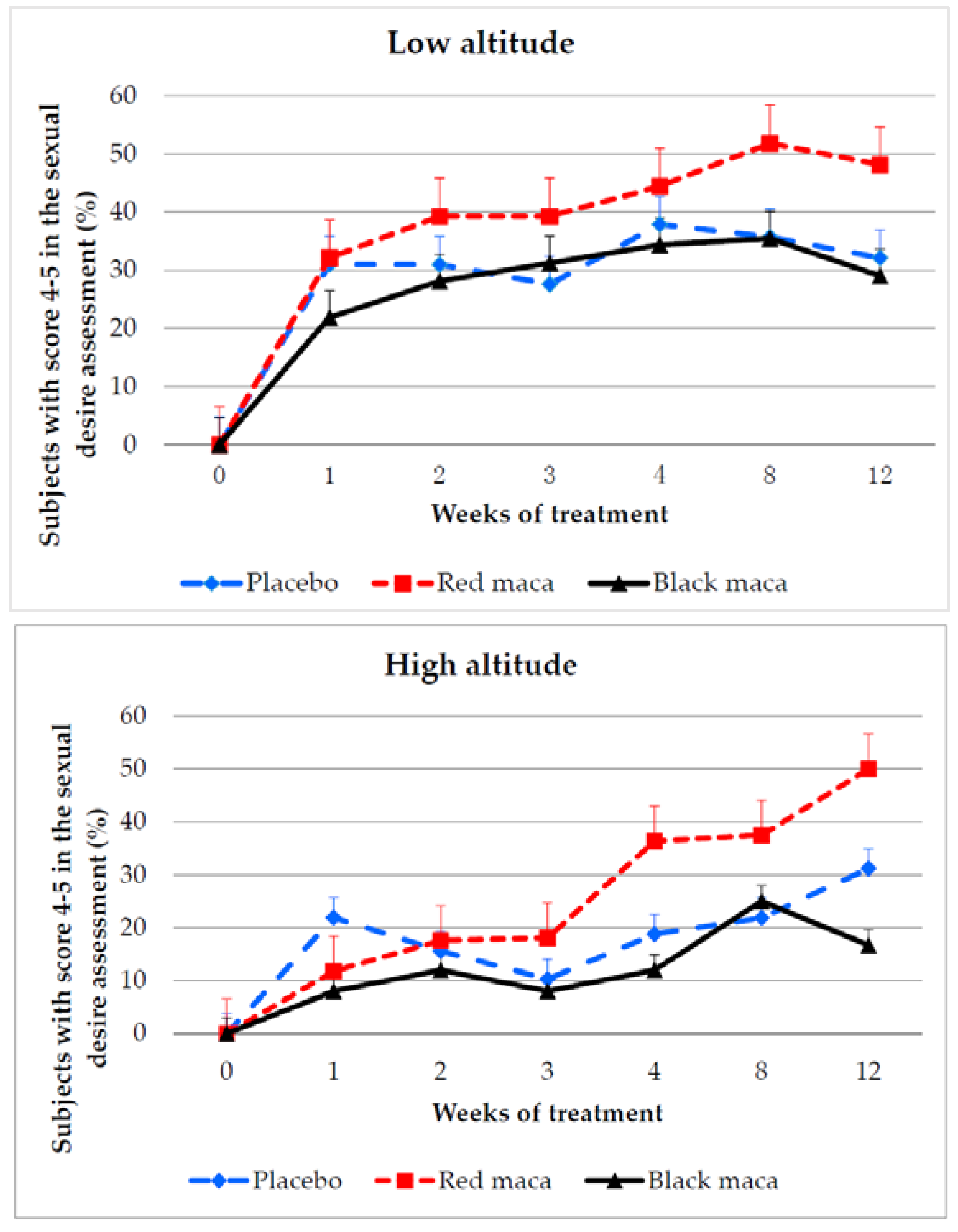
2.2.1. Assessment of Sexual Desire
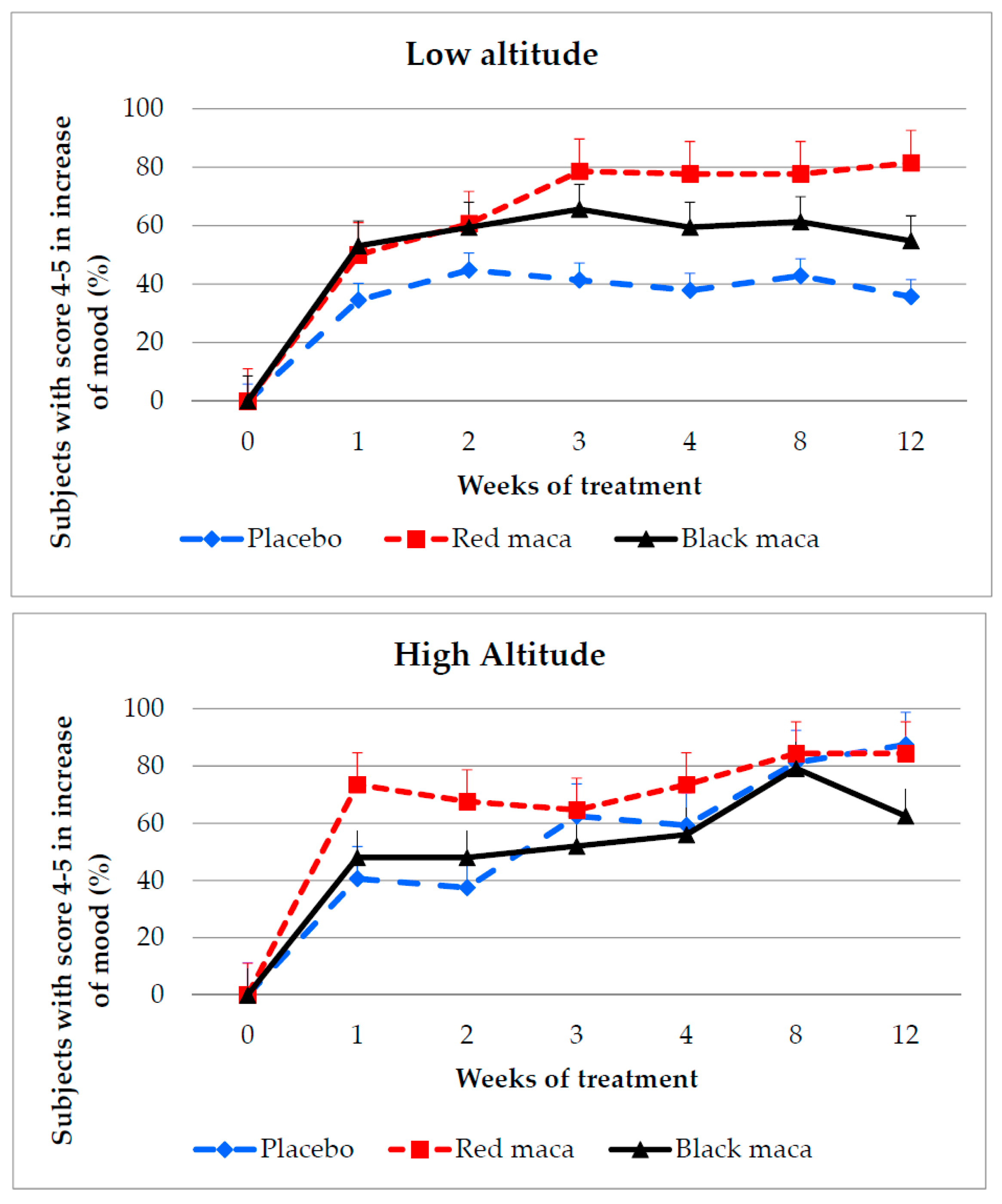
2.2.2. Assessment of Mood
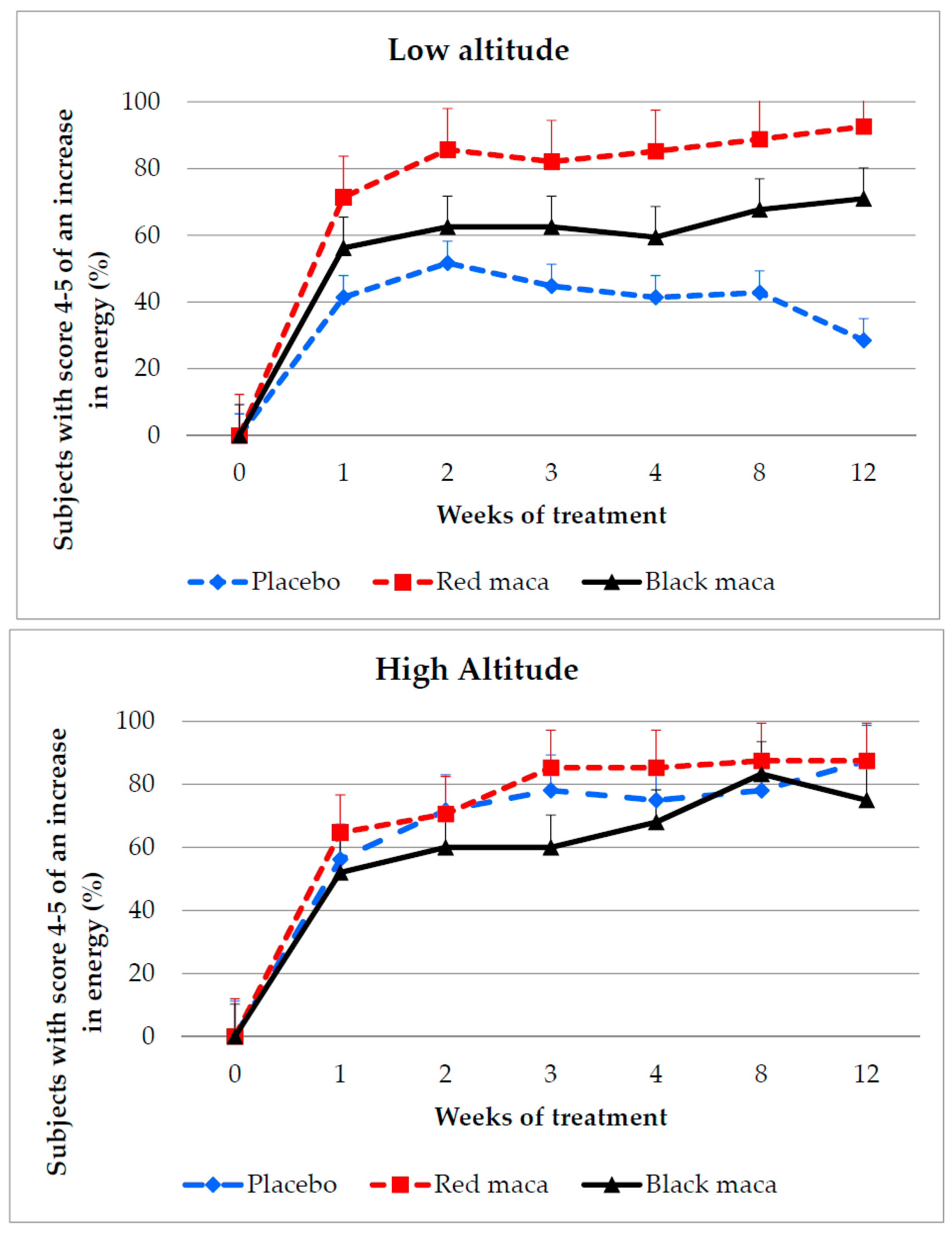
2.2.3. Assessment of Energy
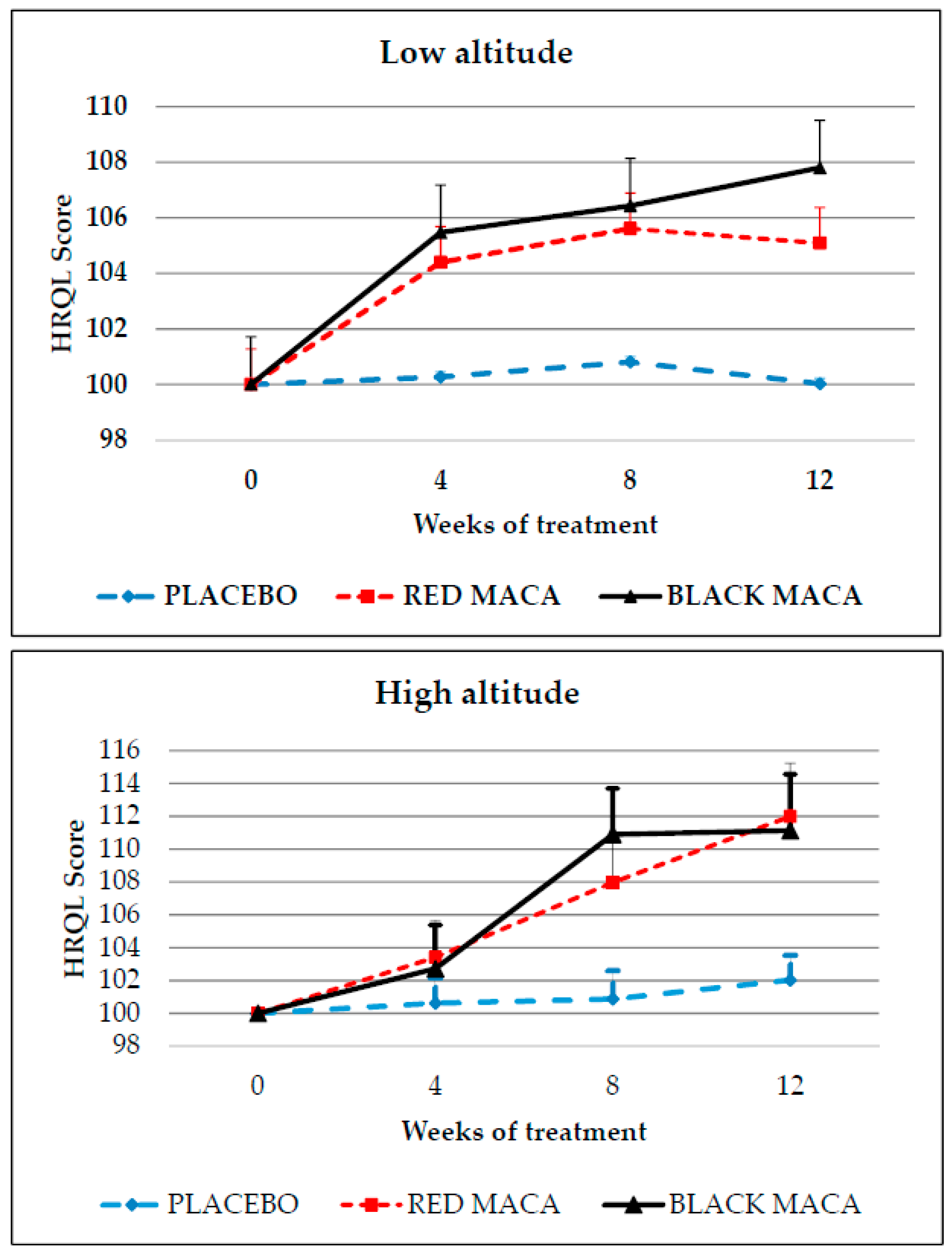
2.2.4. HRQL Score
2.2.5. Pulse Oxygen Saturation (SpO2), Body Mass Index (BMI), Glycaemia, Arterial Blood Pressure, and Hemoglobin
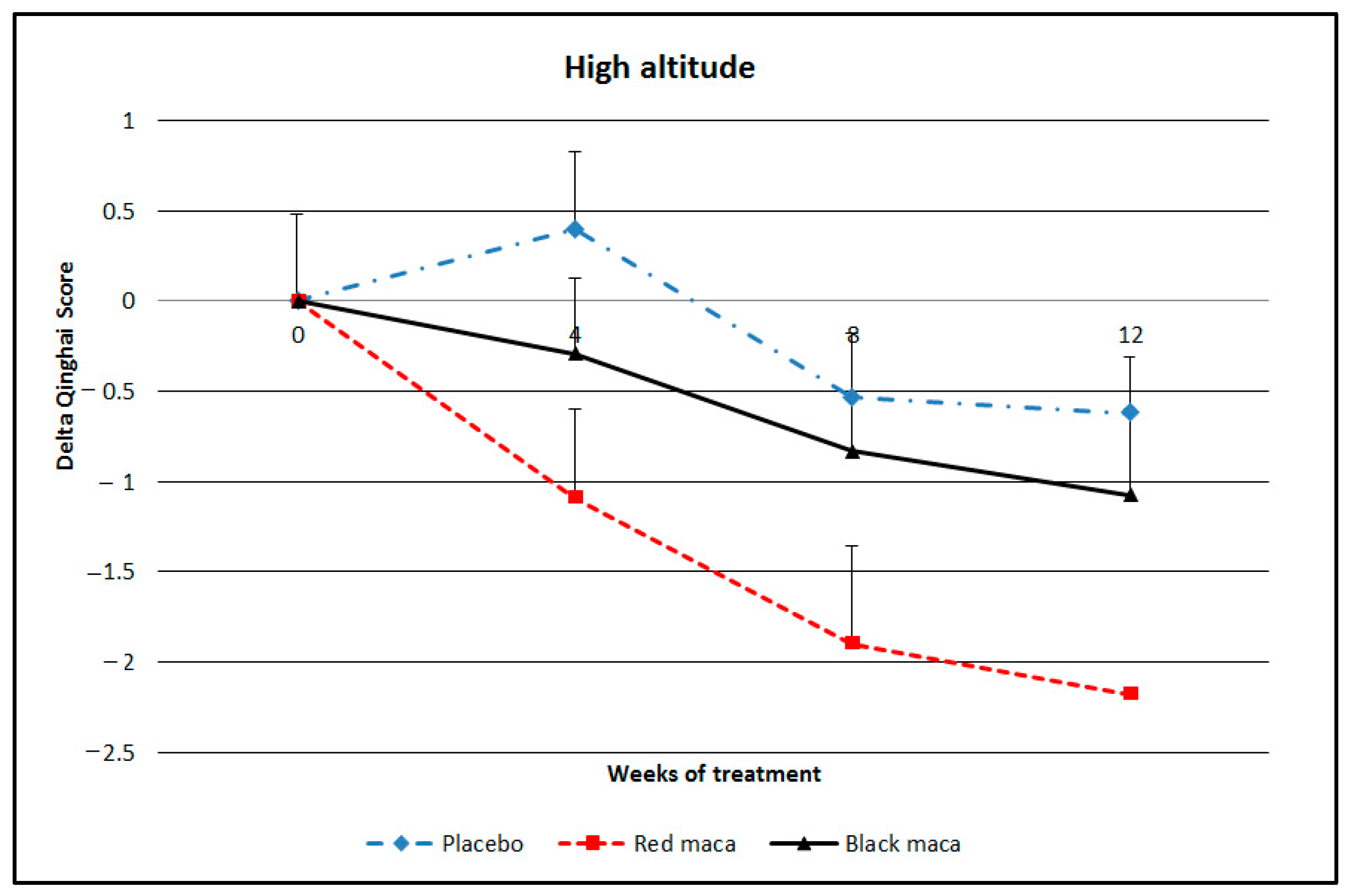
2.2.6. Chronic Mountain Sickness Score
2.3. Secondary Outcomes
2.3.1. Acceptability and Adverse Effects
2.3.2. Effect of Altitude
2.3.3. Blinding
3. Discussion
3.1. Primary Outcomes: Efficacy
3.2. Secondary Outcomes: Acceptability
3.3. Adverse Effects
4. Materials and Methods
4.1. Subjects and Settings
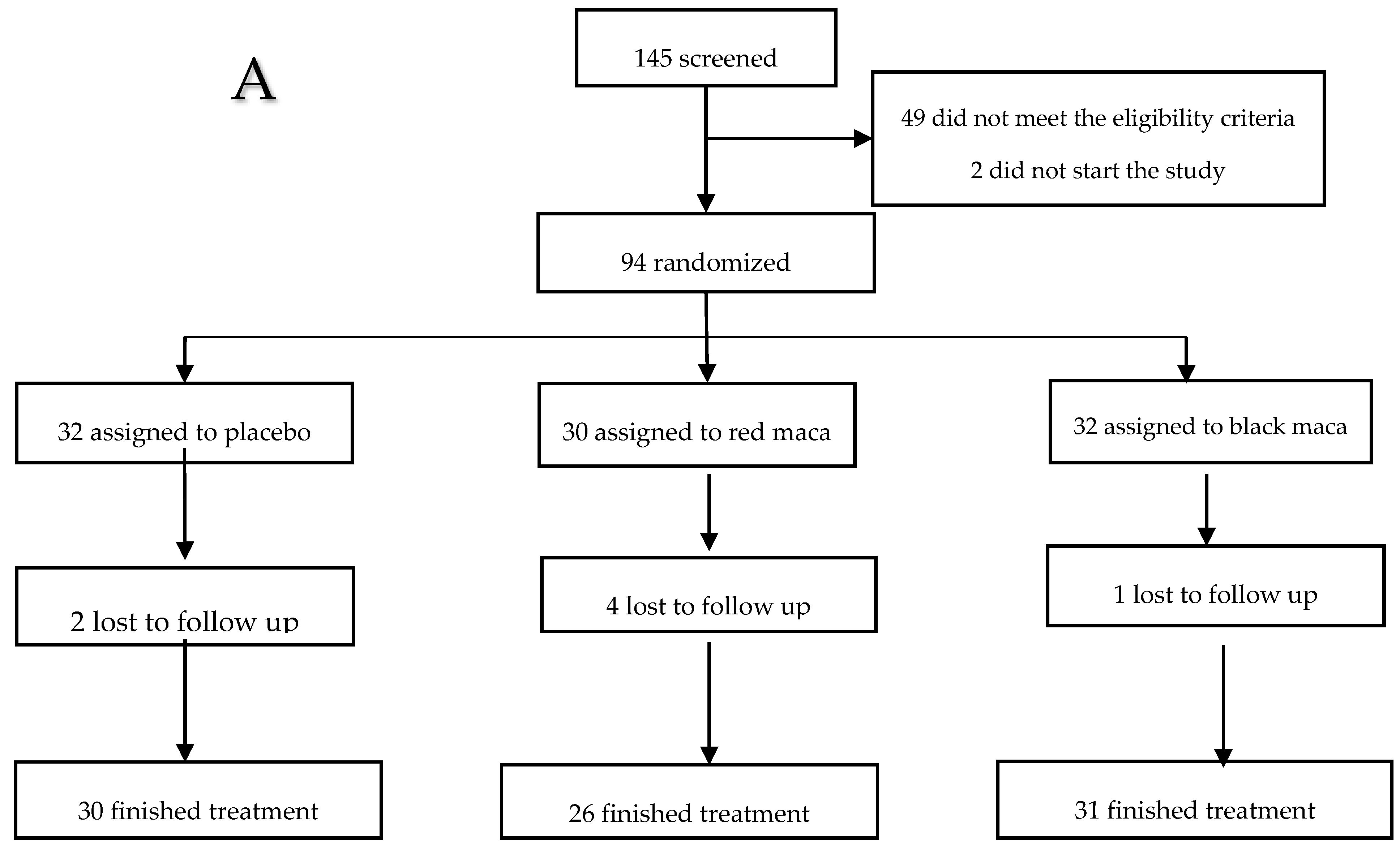
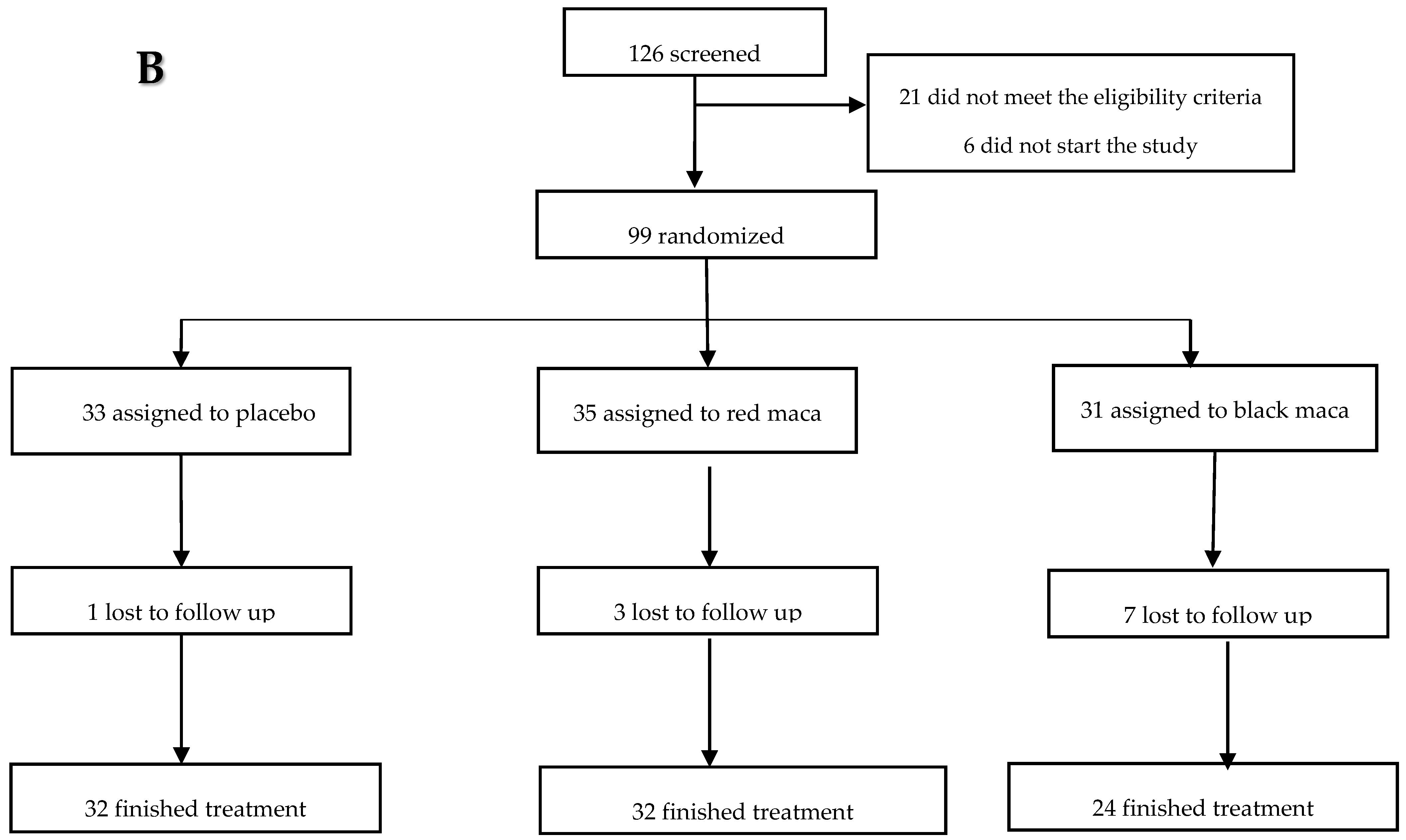
4.2. Recruitment, Randomization, Concealment Allocation, and Lost to Follow-Up
4.3. Design
4.4. Intervention
4.5. Products
4.6. Primary Outcomes: Efficacy
4.6.1. Assessment of Sexual Desire, Mood, and Body Energy Self-Report
4.6.2. Health Status Score
4.6.3. Biological Measurements
4.6.4. Anthropometric Measurements
4.6.5. Chronic Mountain Sickness (CMS) Score
4.7. Secondary Outcomes: Acceptability and Adverse Effects
4.7.1. Acceptability
4.7.2. Safety Self-Recording
4.8. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Valerio, L.; Gonzales, G.F. Toxicological aspects of the South American herbs cat´s claw (Uncaria tomentosa) and Maca (Lepidium meyenii): A critical sypnosis. Toxicol. Rev. 2005, 24, 11–35. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, G.F.; Villaorduña, L.; Gasco, M.; Rubio, J.; Gonzales, C. Maca (Lepidium meyenii Walp), a review of its biological properties. Rev. Peru. Med. Exp. Salud Publica 2014, 31, 100–110. [Google Scholar] [PubMed]
- Gonzales, G.F.; Gasco, M.; Malheiros-Pereira, A.; Gonzales-Castañeda, C. Antagonistic effect of Lepidium meyenii (red maca) on prostatic hyperplasia in adult mice. Andrologia 2008, 40, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, C.; Cárdenas-Valencia, I.; Leiva-Revilla, J.; Anza-Ramirez, C.; Rubio, J.; Gonzales, G.F. Effect of different varieties of Maca (Lepidium meyenii) on bone structure in ovariectomized rats. Forsch. Komplementmed. 2010, 17, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, G.F.; Gonzales-Castañeda, C.; Gasco, M. A mixture of extracts from Peruvian plants (black maca and yacon) improves sperm count and reduced glycemia in mice with streptozotocin-induced diabetes. Toxicol. Mech. Methods 2013, 23, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Rubio, J.; Yucra, S.; Gasco, M.; Gonzales, G.F. Dose-response effect of black maca (Lepidium meyenii) in mice with memory impairment induced by ethanol. Toxicol. Mech. Methods 2011, 21, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Ranilla, L.G.; Kwon, Y.I.; Apostolidis, E.; Shetty, K. Phenolic compounds, antioxidant activity and in vitro inhibitory potential against key enzymes relevant for hyperglycemia and hypertension of commonly used medicinal plants, herbs and spices in Latin America. Bioresour. Technol. 2010, 101, 4676–4689. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, G.F.; Gasco, M.; Lozada-Requena, I. Role of maca (Lepidium meyenii) consumption on serum interleukin-6 levels and health status in populations living in the Peruvian Central Andes over 4000 m of altitude. Plant Foods Hum. Nutr. 2013, 68, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Wu, S.H.; Shu, X.O.; Xiang, Y.B.; Ji, B.T.; Milne, G.L.; Cai, Q.; Zhang, X.; Gao, Y.T.; Zheng, W.; et al. Cruciferous vegetable intake is inversely correlated with circulating levels of proinflammatory markers in women. J. Acad. Nutr. Diet. 2014, 114, 700–709. [Google Scholar] [CrossRef] [PubMed]
- Tilg, H. Cruciferous vegetables: Prototypic anti-inflammatory food components. Clin. Phytosci. 2015, 1, 10. [Google Scholar] [CrossRef]
- Peñaloza, D.; Arias-Stella, J. The heart and pulmonary circulation at high altitudes: Healthy highlanders and chronic mountain sickness. Circulation 2007, 115, 1132–1146. [Google Scholar] [CrossRef]
- Gonzales, G.F. Maca: Del alimento perdido de los Incas al milagro de los Andes: Estudio de seguridad alimentaria y nutricional. Segurança Aliment. Nutr. Camp. 2010, 17, 16–36. [Google Scholar]
- Gonzales, G.F.; Córdova, A.; Vega, K.; Chung, A.; Villena, A.; Góñez, C.; Castillo, S. Effect of Lepidium meyenii (Maca) on sexual desire and its absent relationship with serum testosterone levels in adult healthy men. Andrologia 2002, 34, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Stone, M.; Ibarra, A.; Roller, M.; Zangara, A.; Stevenson, E. A pilot investigation into the effect of maca supplementation on physical activity and sexual desire in sportsmen. J. Ethnopharmacol. 2009, 126, 574–576. [Google Scholar] [CrossRef] [PubMed]
- Stojanovska, L.; Law, C.; Lai, B.; Chung, T.; Nelson, K.; Day, S.; Apostolopoulos, V.; Haines, C. Maca reduces blood pressure and depression, in a pilot study in postmenopausal women. Climacteric 2015, 18, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, G.F.; Córdova, A.; Vega, K.; Chung, A.; Villena, A.; Góñez, C. Effect of Lepidium meyenii (Maca), a root with aphrodisiac and fertility-enhancing properties, on serum reproductive hormone levels in adult healthy men. J. Endocrinol. 2003, 176, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Zenico, T.; Cicero, A.F.; Valmorri, L.; Metrcuriali, M.; Bercovich, E. Subjective effects of Lepidium meyenii (Maca) extract on well-being and sexual performance in patients with mild erectile dysfunction: A randomised, double-blind clinical trial. Andrologia 2009, 41, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Almukadi, H.; Wu, H.; Böhlke, M.; Kelley, C.J.; Maher, T.J.; Pino-Figueroa, A. The macamide N-3-methoxybenzyl-linoleamide is a time-dependent fatty acid amide hydrolase (FAAH) inhibitor. Mol. Neurobiol. 2013, 48, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Hajdu, Z.; Nicolussi, S.; Rau, M.; Lorántfy, L.; Forgo, P.; Hohmann, J.; Csupor, D.; Gertsch, J. Identification of endocannabinoid system-modulating N-alkylamides from Heliopsis helianthoides var. scabra and Lepidium meyenii. J. Nat. Prod. 2014, 77, 1663–1669. [Google Scholar] [CrossRef] [PubMed]
- Bambico, F.R.; Gobbi, G. The cannabinoid CB1 receptor and the endocannabinoid anandamide: Possible antidepressant targets. Expert Opin. Ther. Targets 2008, 12, 1347–1366. [Google Scholar] [CrossRef] [PubMed]
- Shiah, I.-S.; Yatmah, L.N. GABA function in mood disorders: An update and critical review. Life Sci. 1998, 63, 1289–1303. [Google Scholar] [CrossRef]
- Wozniak, J.R.; Fuglestad, A.J.; Eckerle, J.K.; Fink, B.A.; Hoecker, H.L.; Boys, C.J.; Radke, J.P.; Kroupina, M.G.; Miller, N.C.; Brearley, A.M.; et al. Choline supplementation in children with fetal alcohol spectrum disorders: A randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2015, 102, 1113–1125. [Google Scholar] [CrossRef] [PubMed]
- Naber, M.; Hommel, B.; Colzato, L.S. Improved human visuomotor performance and pupil constriction after choline supplementation in a placebo-controlled double-blind study. Sci. Rep. 2015, 5, 13188. [Google Scholar] [CrossRef] [PubMed]
- Knott, V.; de la Salle, S.; Choueiry, J.; Impey, D.; Smith, D.; Smith, M.; Beaudry, E.; Saghir, S.; Ilivitsky, V.; Labelle, A. Neurocognitive effects of acute choline supplementation in low, medium and high performer healthy volunteers. Pharmacol. Biochem. Behav. 2015, 131, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Schenkel, L.C.; Sivanesan, S.; Zhang, J.; Wuyts, B.; Taylor, A.; Verbrugghe, A.; Bakovic, M. Choline supplementation restores substrate balance and alleviates complications of Pcyt2 deficiency. J. Nutr. Biochem. 2015, 26, 1221–1234. [Google Scholar] [CrossRef] [PubMed]
- McCall, N.; Mahadevia, D.; Corriveau, J.A.; Glenn, M.J. Adult emotionality and neural plasticity as a function of adolescent nutrient supplementation in male rats. Pharmacol. Biochem. Behav. 2015, 132, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, N.; Davies, S.; Nadarajah, A.; Rivera, J.; Whittington, R.; Mercier, R.J.; Virag, L.; Wang, S.; Flood, P. Oral choline supplementation for postoperative pain. Br. J. Anaesth. 2013, 111, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Valentová, K.; Stejskal, D.; Bartek, J.; Dvorácková, S.; Kren, V.; Ulrichová, J.; Simánek, V. Maca (Lepidium meyenii) and yacon (Smallanthus sonchifolius) in combination with silymarin as food supplements: In vivo safety assessment. Food Chem. Toxicol. 2008, 46, 1006–1013. [Google Scholar] [CrossRef] [PubMed]
- Vecera, R.; Orolin, J.; Skottová, N.; Kazdová, L.; Oliyarnik, O.; Ulrichová, J.; Simánek, V. The influence of maca (Lepidium meyenii) on antioxidant status, lipid and glucose metabolism in rat. Plant Foods Hum. Nutr. 2007, 62, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Woolcott, O.O.; Ader, M.; Bergman, R.N. Glucose homeostasis during short-term and prolonged exposure to high altitudes. Endocr. Rev. 2015, 36, 149–173. [Google Scholar] [CrossRef] [PubMed]
- Meissner, H.O.; Reich-Bilinska, H.; Mscisz, A.; Kedzia, B. Therapeutic effects of pregelatinized maca (Lepidium peruvianum Chacon) used as non-hormonal alternative to HRT in perimenopausal women-Clinical pilot study. Int. J. Biomed. Sci. 2006, 2, 143–159. [Google Scholar] [PubMed]
- Kaptchuk, T.J. The placebo effect in alternative medicine: Can the performance of a healing ritual have clinical significance? Ann. Intern. Med. 2002, 136, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Kaptchuk, T.J.; Miller, F.G. Placebo effects in medicine. N. Engl. J. Med. 2015, 373, 8–9. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.T.; Loscalzo, J.; Kaptchuk, T.J. Genetics and the placebo effect: The placebome. Trends Mol. Med. 2015, 21, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, F.; Durando, J.; Vighetti, S. Nocebo and placebo modulation of hypobaric hypoxia headeche involves the cyclooxygenase-prostaglandins pathway. Pain 2014, 155, 921–928. [Google Scholar] [CrossRef] [PubMed]
- Andreeva, V.A.; Martin, C.; Issanchou, S.; Hercberg, S.; Kesse-Guyot, E.; Méjean, C. Sociodemographic profiles regarding bitter food consumption: Cross-sectional evidence from a general French population. Appetite 2013, 67, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Wooding, S.; Gunn, H.; Ramos, P.; Thalmann, S.; Xing, C.; Meyerhof, W. Genetics and bitter responses to goitrin, a plant toxin found in vegetables. Chem. Senses 2010, 35, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Ippushi, K.; Ueda, H.; Takeuchi, A. Milk prevents the degradation of daikon (Raphanus sativus L.) isothyocyanate and enhances its absorption in rats. Food Chem. 2014, 161, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Sansom, C.E.; Jones, V.S.; Joyce, N.I.; Smallfield, B.M.; Perry, N.B.; van Klink, J.W. Flavor, glucosinolates, and isothiocyanates of nau (Cook´s scurvy grass, Lepidium oleraceum) and other rare New Zealand Lepidium species. J. Agric. Food Chem. 2015, 63, 1833–1838. [Google Scholar] [CrossRef] [PubMed]
- Posadzki, P.; Watson, L.K.; Ernst, E. Adverse effects of herbal medicines: An overview of systematic reviews. Clin. Med. (Lond.) 2013, 13, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Gasco, M.; Aguilar, J.; Gonzales, G.F. Effect of chronic treatment with three varieties of Lepidium meyenii (Maca) on reproductive parameters and DNA quantification in adult male rats. Andrologia 2007, 39, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Reagan-Shaw, S.; Nihal, M.; Ahmad, N. Dose translation from animal to human studies revisited. FASEB J. 2008, 22, 659–661. [Google Scholar] [CrossRef] [PubMed]
- FDA. IND [Investigational New Drug Application] PHASES of an Investigation. Title 21, Vol 5, Code of Federal Regulations 312.21; Government Printing Office: Washington, DC, USA, 1 April 2012.
- Zhao, J.; Avula, B.; Chan, M.; Clément, C.; Kreuzer, M.; Khan, I.A. Metabolomic differentiation of maca (Lepidium meyenii) accessions cultivated under different conditions using NMR and chemometric analysis. Planta Med. 2012, 78, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Ribera, A.; Domingo-Salvany, A.; et al. The Spanish version of the Short Form 36 Health Survey: A decade of experience and new developments. Gac. Sanit. 2005, 19, 135–150. [Google Scholar] [CrossRef] [PubMed]
- León-Velarde, F.; Maggiorini, M.; Reeves, J.T.; Aldashev, A.; Asmus, I.; Bernardi, L.; Ge, R.L.; Hackett, P.; Kobayashi, T.; Moore, L.G.; et al. Consensus statement on chronic and subacute high altitude diseases. High Alt. Med. Biol. 2005, 6, 147–157. [Google Scholar] [CrossRef] [PubMed]
- McGough, C.; Peacock, N.; Hackett, C.; Baldwin, C.; Norman, A.; Frost, G.; Blake, P.; Tait, D.; Khoo, V.; Harrington, K.; et al. Taste preferences for oral nutrition supplements in patients before and after pelvic radiotherapy: A double-blind controlled study. Clin. Nutr. 2006, 25, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Vacha-Haase, T.; Thompson, B. How to estimate and interpret various effect sizes. J. Couns. Psychol. 2004, 51, 473–481. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compound | Maca Samples | |
|---|---|---|
| Black Maca | Red Maca | |
| Formic acid | 4.10 | 6.94 |
| Adenine | 6.23 | 5.06 |
| Fumaric acid | 13.79 | 15.43 |
| Uridine | 10.82 | 10.71 |
| Sucrose | 1632.36 | 1368.35 |
| Glucotropaeolin | 77.50 | 72.08 |
| Macamides | 55.21 | 39.86 |
| Choline | 327.44 | 366.99 |
| GABA | 40.09 | 76.59 |
| Malic acid | 83.88 | 92.81 |
| Glutamine | 132.01 | 118.27 |
| Proline | 875.25 | 832.98 |
| Fatty acids | 504.55 | 378.36 |
| Alanine | 156.22 | 152.41 |
| Valine | 111.48 | 107.61 |
| Phytosterols | 24.23 | 21.10 |
| Time of Consumption (Weeks) | Placebo | Red Maca | Black Maca | |||
|---|---|---|---|---|---|---|
| LA (32) | HA (33) | LA (30) | HA (35) | LA (32) | HA (31) | |
| 0 | 90.78 ± 1.38 | 71.48 ± 2.25 | 92.81 ± 1.48 | 75.00 ± 2.47 | 91.61 ± 1.12 | 78.96 ± 2.50 a |
| 4 | 89.77 ± 1.40 | 69.84 ± 1.70 | 90.33 ± 1.34 | 72.66 ± 2.04 | 90.23 ± 1.26 | 74.66 ± 1.60 b |
| 8 | 88.90 ± 1.42 | 67.59 ± 2.11 | 87.29 ± 1.60 ** | 67.77 ± 2.04 ** | 86.71 ± 1.31 ** | 70.59 ± 2.44 ** |
| 12 | 84.87 ± 1.49 ** | 71.12 ± 2.48 | 86.15 ± 2.24 ** | 69.62 ± 2.09 | 86.03 ± 1.77 ** | 72.33 ± 2.86 ** |
| Treatment | Time 0 | 4th Week | 8th Week | 12th Week | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SBP | DBP | SBP | DBP | SBP | DBP | SBP | DBP | |||||||||
| LA | HA | LA | HA | LA | HA | LA | HA | LA | HA | LA | HA | LA | HA | LA | HA | |
| Placebo | 101.6 ± 2.33 | 101.75 ± 2.14 | 66.56 ± 1.86 | 62.96 ± 2.15 | 102.9 ± 1.62 | 100.18 ± 1.83 | 71.94 ± 1.57 | 63.96 ± 2.10 | 99.67 ± 1.73 | 96.43 ± 1.48 ** | 68.67 ± 1.47 | 69.18 ± 1.67 ** | 100.33 ± 1.86 | 94.87 ± 1.95 ** | 65.50 ± 1.77 | 68.12 ± 1.59 |
| Red maca | 97.78 ± 1.82 | 103.71 ± 2.12 | 66.30 ± 2.00 | 64.91 ± 1.83 | 103.33 ± 1.41 | 99.58 ± 1.49 | 71.85 ± 1.58 | 65.12 ± 1.94 | 102.86 ± 1.61 | 98.15 ± 2.34 | 70.36 ± 1.66 | 67.34 ± 2.01 | 101.54 ± 1.41 | 98.43 ± 2.46 | 69.62 ± 1.48 | 68.12 ± 1.81 |
| Black maca | 98.71 ± 1.92 | 103.62 ± 1.96 | 67.90 ± 2.30 | 63.28 ± 2.45 | 100.97 ± 1.79 | 99.96 ± 1.46 | 70.00 ± 1.77 | 63.75 ± 1.17 | 103.87 ± 1.63 | 95.08 ± 2.22 * | 70.16 ± 1.75 | 68.33 ± 1.94 | 101.33 ± 1.59 | 93.33 ± 2.38 * | 69.33 ± 1.22 | 64.16 ± 1.69 |
| Time of Consumption (Weeks) | Placebo | Red Maca | Black Maca | |||
|---|---|---|---|---|---|---|
| ¶,¥ LA | HA ¥ | ¶,¥ LA | HA | ¶,¥ LA | HA | |
| 0 | 13.97 ± 0.20 | 17.80 ± 0.36 | 13.58 ± 0.24 | 18.21 ± 0.38 | 13.40 ± 0.23 | 17.47 ± 0.43 |
| 4 | 13.83 ± 0.28 | 18.03 ± 0.30 | 13.69 ± 0.27 | 17.28 ± 0.36 * | 13.61 ± 0.21 | 16.40 ± 0.38 *,a |
| 8 | 13.68 ± 0.28 | 17.96 ± 0.29 | 13.64 ± 0.27 | 17.10 ± 0.37 * | 13.48 ± 0.23 | 16.23 ± 0.38 **,a |
| 12 | 14.48 ± 0.28 | 17.91 ± 0.35 | 14.09 ± 0.28 | 17.38 ± 0.38 ** | 13.73 ± 0.23 | 16.22 ± 0.49 *,a |
© 2016 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzales-Arimborgo, C.; Yupanqui, I.; Montero, E.; Alarcón-Yaquetto, D.E.; Zevallos-Concha, A.; Caballero, L.; Gasco, M.; Zhao, J.; Khan, I.A.; Gonzales, G.F. Acceptability, Safety, and Efficacy of Oral Administration of Extracts of Black or Red Maca (Lepidium meyenii) in Adult Human Subjects: A Randomized, Double-Blind, Placebo-Controlled Study. Pharmaceuticals 2016, 9, 49. https://doi.org/10.3390/ph9030049
Gonzales-Arimborgo C, Yupanqui I, Montero E, Alarcón-Yaquetto DE, Zevallos-Concha A, Caballero L, Gasco M, Zhao J, Khan IA, Gonzales GF. Acceptability, Safety, and Efficacy of Oral Administration of Extracts of Black or Red Maca (Lepidium meyenii) in Adult Human Subjects: A Randomized, Double-Blind, Placebo-Controlled Study. Pharmaceuticals. 2016; 9(3):49. https://doi.org/10.3390/ph9030049
Chicago/Turabian StyleGonzales-Arimborgo, Carla, Irma Yupanqui, Elsa Montero, Dulce E. Alarcón-Yaquetto, Alisson Zevallos-Concha, Lidia Caballero, Manuel Gasco, Jianping Zhao, Ikhlas A. Khan, and Gustavo F. Gonzales. 2016. "Acceptability, Safety, and Efficacy of Oral Administration of Extracts of Black or Red Maca (Lepidium meyenii) in Adult Human Subjects: A Randomized, Double-Blind, Placebo-Controlled Study" Pharmaceuticals 9, no. 3: 49. https://doi.org/10.3390/ph9030049