
Consumption of Herbal Supplements or Homeopathic Remedies to Prevent COVID-19 and Intention of Vaccination for COVID-19 in Latin America and the Caribbean

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Population, Sample, and Sampling
2.3. Variables
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Selection of the Study Sample
3.2. Characteristics of the Samples Included in the Study
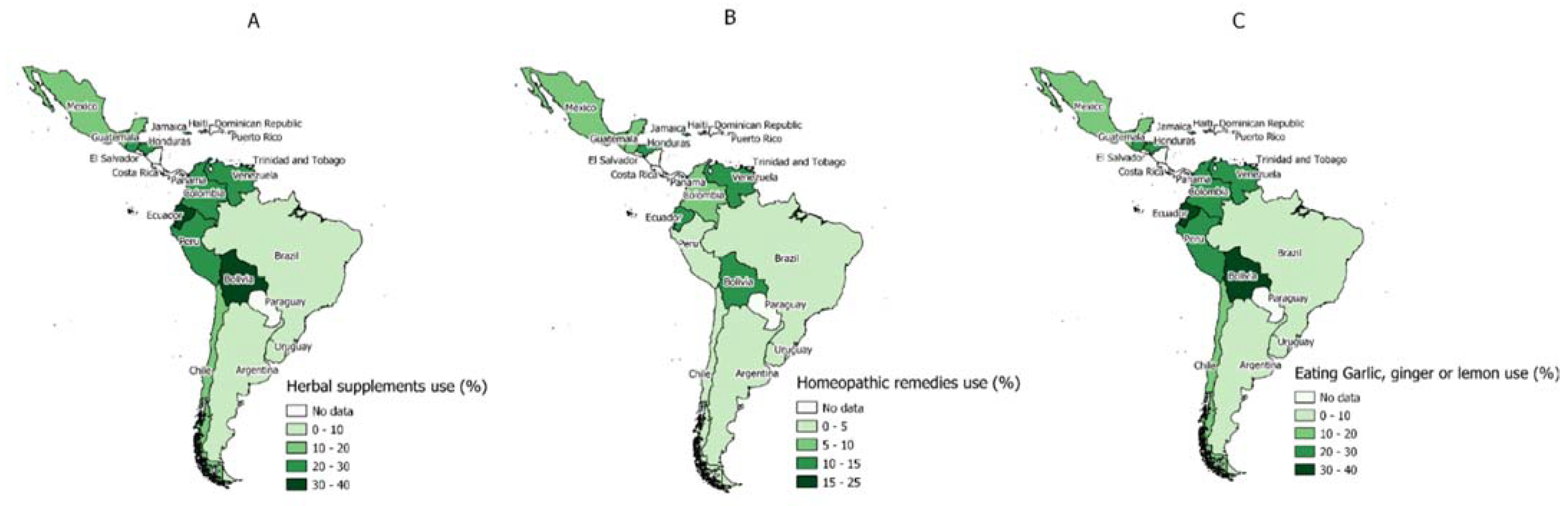
3.3. Prevalence of Using Herbal Supplements to Prevent COVID-19 Infection by Each LAC Country
3.4. Prevalence of the Use of Homeopathic Remedies to Prevent COVID-19 Infection by Each LAC Country
3.5. Prevalence of Garlic, Ginger, and Lemon Consumption to Prevent COVID-19 Infection by Each LAC Country
3.6. Bivariate Analysis According to Each Measure Taken to Prevent COVID-19 Infection
3.7. Association between Using Herbal Supplements to Prevent COVID-19 Infection and Non-Intention from Vaccinating against COVID-19
3.8. Association between the Use of Homeopathic Remedies to Prevent COVID-19 Infection and Non-Intention from Vaccinating against COVID-19
3.9. Association between the Consumption of Garlic, Ginger and Lemon to Prevent Infection by COVID-19 and Non-Intention to Vaccinate against COVID-19
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guarner, J. Three Emerging Coronaviruses in Two Decades: The Story of SARS, MERS, and Now COVID-19. Am. J. Clin. Pathol. 2020, 153, 420–421. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 6 May 2022).
- Center for Systems Science and Engineering COVID-19 Map—Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 11 November 2021).
- World Health Organization. COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 6 May 2022).
- Orensteina, W.A.; Ahmedb, R. Simply Put: Vaccination Saves Lives. Proc. Natl. Acad. Sci. USA 2017, 114, 4031–4033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Vaccines and Immunization: What Is Vaccination? Available online: https://www.who.int/news-room/questions-and-answers/item/vaccines-and-immunization-what-is-vaccination (accessed on 6 May 2022).
- Shah, S. Children and the American Rescue Plan: Countering COVID-19 Vaccine Hesitancy during a Global Pandemic. Pediatr. Res. 2021, 90, 237–239. [Google Scholar] [CrossRef] [PubMed]
- Urrunaga-Pastor, D.; Bendezu-Quispe, G.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Toro-Huamanchumo, C.J.; Rodriguez-Morales, A.J.; Hernandez, A.V.; Benites-Zapata, V.A. Cross-Sectional Analysis of COVID-19 Vaccine Intention, Perceptions and Hesitancy across Latin America and the Caribbean. Travel Med. Infect. Dis. 2021, 41, 102059. [Google Scholar] [CrossRef] [PubMed]
- Thompson, H.S.; Manning, M.; Mitchell, J.; Kim, S.; Harper, F.W.K.; Cresswell, S.; Johns, K.; Pal, S.; Dowe, B.; Tariq, M.; et al. Factors Associated with Racial/Ethnic Group-Based Medical Mistrust and Perspectives on COVID-19 Vaccine Trial Participation and Vaccine Uptake in the US. JAMA Netw. Open 2021, 4, e2111629. [Google Scholar] [CrossRef] [PubMed]
- Bates, B.R.; Villegas-Botero, A.; Costales, J.A.; Moncayo, A.L.; Tami, A.; Carvajal, A.; Grijalva, M.J. COVID-19 Vaccine Hesitancy in Three Latin American Countries: Reasons Given for Not Becoming Vaccinated in Colombia, Ecuador, and Venezuela. Health Commun. 2022, 1–11. [Google Scholar] [CrossRef]
- Wang, Q.; Yang, L.; Jin, H.; Lin, L. Vaccination against COVID-19: A Systematic Review and Meta-Analysis of Acceptability and Its Predictors. Prev. Med. 2021, 150, 106694. [Google Scholar] [CrossRef]
- Sallam, M. Covid-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Al-Amer, R.; Maneze, D.; Everett, B.; Montayre, J.; Villarosa, A.R.; Dwekat, E.; Salamonson, Y. COVID-19 Vaccination Intention in the First Year of the Pandemic: A Systematic Review. J. Clin. Nurs. 2022, 31, 62–86. [Google Scholar] [CrossRef]
- Kohl-Heckl, W.K.; Schröter, M.; Dobos, G.; Cramer, H. Complementary Medicine Use and Flu Vaccination – A Nationally Representative Survey of US Adults. Vaccine 2021, 39, 5635–5640. [Google Scholar] [CrossRef]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J. Vaccine Hesitancy: An Overview. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Díaz Seoane, M.; Berbel Hernández, C.; Allué Tango, M.; García Rodriguez, C.; Sanz López, P.; Pérez Martín, M.I.; Gutiérrez Pérez, M.S. Factors Related to Parents’ Decision Not to Vaccinate Their Children. Vacunas 2020, 21, 4–10. [Google Scholar] [CrossRef]
- Hornsey, M.J.; Lobera, J.; Díaz-Catalán, C. Vaccine Hesitancy Is Strongly Associated with Distrust of Conventional Medicine, and Only Weakly Associated with Trust in Alternative Medicine. Soc. Sci. Med. 2020, 255, 113019. [Google Scholar] [CrossRef] [PubMed]
- Castañeda-Vasquez, D.E.; Ruiz-Padilla, J.P.; Botello-Hernandez, E. Vaccine Hesitancy Against SARS-CoV-2 in Health Personnel of Northeastern Mexico and Its Determinants. J. Occup. Environ. Med. 2021, 63, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Loeb, M.; Russell, M.L.; Neupane, B.; Thanabalan, V.; Singh, P.; Newton, J.; Pullenayegum, E. A Randomized, Blinded, Placebo-Controlled Trial Comparing Antibody Responses to Homeopathic and Conventional Vaccines in University Students. Vaccine 2018, 36, 7423–7429. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Traditional Medicine Strategy 2014–2023. Available online: https://www.who.int/publications/i/item/9789241506096 (accessed on 6 May 2022).
- Ekor, M. The Growing Use of Herbal Medicines: Issues Relating to Adverse Reactions and Challenges in Monitoring Safety. Front. Neurol. 2014, 4, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antwi-Baffour, S.S.; Bello, A.I.; Adjei, D.N.; Mahmood, S.A.; Ayeh-Kumi, P.F. The Place of Traditional Medicine in the African Society: The Science, Acceptance and Support. Am. J. Heal. Res. 2014, 2, 49. [Google Scholar] [CrossRef] [Green Version]
- Naicker, S.; Plange-Rhule, J.; Tutt, R.C.; Eastwood, J.B. Shortage of Healthcare Workers in Developing Countries—Africa. Ethn. Dis. 2009, 19, 60. [Google Scholar]
- Pearson, H.; Fleming, T.; Chhoun, P.; Tuot, S.; Brody, C.; Yi, S. Prevalence of and Factors Associated with Utilization of Herbal Medicines among Outpatients in Primary Health Centers in Cambodia. BMC Complement. Altern. Med. 2018, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Bussmann, R.W. The Globalization of Traditional Medicine in Northern Peru: From Shamanism to Molecules. Evid. -Based Complement. Altern. Med. 2013, 2013, 291903. [Google Scholar] [CrossRef]
- Stanifer, J.W.; Kilonzo, K.; Wang, D.; Su, G.; Mao, W.; Zhang, L.; Zhang, L.; Nayak-Rao, S.; Miranda, J.J. Traditional Medicines and Kidney Disease in Low- and Middle-Income Countries: Opportunities and Challenges. Semin. Nephrol. 2017, 37, 245–259. [Google Scholar] [CrossRef]
- The Lancet COVID-19 in Latin America—Emergency and Opportunity. Lancet 2021, 398, 93. [CrossRef]
- Ruiz, J.B.; Bell, R.A. Predictors of Intention to Vaccinate against COVID-19: Results of a Nationwide Survey. Vaccine 2021, 39, 1080–1086. [Google Scholar] [CrossRef]
- Abdullah Alotiby, A.; Naif Al-Harbi, L. Prevalence of Using Herbs and Natural Products as a Protective Measure during the COVID-19 Pandemic among the Saudi Population: An Online Cross-Sectional Survey. Saudi Pharm. J. 2021, 29, 410–417. [Google Scholar] [CrossRef]
- Chali, B.U.; Melaku, T.; Berhanu, N.; Mengistu, B.; Milkessa, G.; Mamo, G.; Alemu, S.; Mulugeta, T. Traditional Medicine Practice in the Context of Covid-19 Pandemic: Community Claim in Jimma Zone, Oromia, Ethiopia. Infect. Drug Resist. 2021, 14, 3773–3783. [Google Scholar] [CrossRef]
- Srikanth, N.; Rana, R.; Singhal, R.; Jameela, S.; Singh, R.; Khanduri, S.; Tripathi, A.; Goel, S.; Chhatre, L.; Chandra, A.; et al. Mobile App–Reported Use of Traditional Medicine for Maintenance of Health in India During the COVID-19 Pandemic: Cross-Sectional Questionnaire Study. JMIRx Med. 2021, 2, e25703. [Google Scholar] [CrossRef] [PubMed]
- Charan, J.; Bhardwaj, P.; Dutta, S.; Kaur, R.; Bist, S.K.; Detha, M.D.; Kanchan, T.; Yadav, D.; Mitra, P.; Sharma, P. Use of Complementary and Alternative Medicine (CAM) and Home Remedies by COVID-19 Patients: A Telephonic Survey. Indian J. Clin. Biochem. 2021, 36, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Parisius, L.M.; Stock-Schröer, B.; Berger, S.; Hermann, K.; Joos, S. Use of Home Remedies: A Cross-Sectional Survey of Patients in Germany. BMC Fam. Pract. 2014, 15, 116. [Google Scholar] [CrossRef] [Green Version]
- Zeni, A.L.B.; Parisotto, A.V.; Mattos, G.; Helena, E.T.D.S. Utilização de Plantas Medicinais Como Remédio Caseiro Na Atenção Primária Em Blumenau, Santa Catarina, Brasil. Cienc. Saude Coletiva 2017, 22, 2703–2712. [Google Scholar] [CrossRef] [Green Version]
- Alyami, H.S.; Orabi, M.A.A.; Aldhabbah, F.M.; Alturki, H.N.; Aburas, W.I.; Alfayez, A.I.; Alharbi, A.S.; Almasuood, R.A.; Alsuhaibani, N.A. Knowledge about COVID-19 and Beliefs about and Use of Herbal Products during the COVID-19 Pandemic: A Cross-Sectional Study in Saudi Arabia. Saudi Pharm. J. 2020, 28, 1326–1332. [Google Scholar] [CrossRef]
- Lam, C.S.; Koon, H.K.; Chung, V.C.H.; Cheung, Y.T. A Public Survey of Traditional, Complementary and Integrative Medicine Use during the COVID-19 Outbreak in Hong Kong. PLoS ONE 2021, 16, e0253890. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.A.; Kumar, P.; Jyoti; Kumar, N. Spices and Herbs: Potential Antiviral Preventives and Immunity Boosters during COVID-19. Phyther. Res. 2021, 35, 2745–2757. [Google Scholar] [CrossRef] [PubMed]
- Ang, L.; Lee, H.W.; Choi, J.Y.; Zhang, J.; Soo Lee, M. Herbal Medicine and Pattern Identification for Treating COVID-19: A Rapid Review of Guidelines. Integr. Med. Res. 2020, 9, 100407. [Google Scholar] [CrossRef] [PubMed]
- Ochoa Yupanqui, W.W.; Rodríguez Lizana, M. Fitoterapia Altoandina Como Potencial Ante La COVID-19. Rev. Cuba. Investig. Biomédicas 2020, 39, e862. [Google Scholar]
- Ang, L.; Lee, H.W.; Kim, A.; Choi, J.Y.; Lee, M.S. Network Analysis of Herbs Recommended for the Treatment of Covid-19. Infect. Drug Resist. 2021, 14, 1833–1844. [Google Scholar] [CrossRef]
- Zhou, L.P.; Wang, J.; Xie, R.H.; Pakhale, S.; Krewski, D.; Cameron, D.W.; Wen, S.W. The Effects of Traditional Chinese Medicine as an Auxiliary Treatment for COVID-19: A Systematic Review and Meta-Analysis. J. Altern. Complement. Med. 2021, 27, 225–237. [Google Scholar] [CrossRef]
- Rossi, E.G. The Experience of an Italian Public Homeopathy Clinic during the COVID-19 Epidemic, March–May 2020. Homeopathy 2020, 109, 167–168. [Google Scholar] [CrossRef]
- Takacs, M.; Frass, M.; Walder, G.; Fibert, P.; Rottensteiner, M.; Glück, W.; Lechleitner, P.; Oberbaum, M.; Leisser, I.; Chandak, K.; et al. Adjunctive Homeopathic Treatment of Hospitalized COVID-19 Patients (COVIHOM): A Retrospective Case Series. Complement. Ther. Clin. Pract. 2021, 44, 101415. [Google Scholar] [CrossRef]
- Ganguly, S.; Bakhshi, S. Traditional and Complementary Medicine during COVID-19 Pandemic. Phyther. Res. 2020, 34, 3083–3084. [Google Scholar] [CrossRef]
- Shankar, A.; Dubey, A.; Saini, D.; Prasad, C.P. Role of Complementary and Alternative Medicine in Prevention and Treatment of COVID-19: An Overhyped Hope. Chin. J. Integr. Med. 2020, 26, 565–567. [Google Scholar] [CrossRef]
- Kalliantas, D.; Kallianta, M.; Karagianni, C.S. RETRACTED ARTICLE: Homeopathy Combat against Coronavirus Disease (Covid-19). J. Public Health 2021, 29, 253. [Google Scholar] [CrossRef] [PubMed]
- Zuzak, T.; Zuzak-Siegrist, I.; Rist, L.; Simoes-Wüst, A. Attitudes towards Vaccination: Users of Complementary and Alternative Medicine versus Non-Users. Swiss Med. Wkly. 2008, 138, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Deml, M.J.; Notter, J.; Kliem, P.; Buhl, A.; Huber, B.M.; Pfeiffer, C.; Burton-Jeangros, C.; Tarr, P.E. “We Treat Humans, Not Herds!”: A Qualitative Study of Complementary and Alternative Medicine (CAM) Providers’ Individualized Approaches to Vaccination in Switzerland. Soc. Sci. Med. 2019, 240, 112556. [Google Scholar] [CrossRef] [PubMed]
- Eizayaga, J.E.; Waisse, S. What Do Homeopathic Doctors Think of Vaccines? An International Online Survey. Homeopathy 2016, 105, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Soveri, A.; Karlsson, L.C.; Antfolk, J.; Lindfelt, M.; Lewandowsky, S. Unwillingness to Engage in Behaviors That Protect against COVID-19: The Role of Conspiracy Beliefs, Trust, and Endorsement of Complementary and Alternative Medicine. BMC Public Health 2021, 21, 684. [Google Scholar] [CrossRef]
- McCarthy, M. Critics Slam Draft WHO Report on Homoeopathy. Lancet 2005, 366, 705–706. [Google Scholar] [CrossRef]
- National Health Service (NHS). Homeopathy. Available online: https://www.nhs.uk/conditions/homeopathy/ (accessed on 6 May 2022).
- Food and Drug Administration Homeopathic Products. Available online: https://www.fda.gov/drugs/information-drug-class/homeopathic-products (accessed on 6 May 2022).
- Roozenbeek, J.; Schneider, C.R.; Dryhurst, S.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; Van Der Bles, A.M.; Van Der Linden, S. Susceptibility to Misinformation about COVID-19 around the World. R. Soc. Open Sci. 2020, 7, 201199. [Google Scholar] [CrossRef]
- Arif, N.; Al-Jefri, M.; Bizzi, I.H.; Perano, G.B.; Goldman, M.; Haq, I.; Chua, K.L.; Mengozzi, M.; Neunez, M.; Smith, H.; et al. Fake News or Weak Science? Visibility and Characterization of Antivaccine Webpages Returned by Google in Different Languages and Countries. Front. Immunol. 2018, 9, 1215. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 6 May 2022).



{kind=link}
{kind=link}
| Characteristics | Use of Herbal Supplements (N = 28,590) | Use of Homeopathic Remedies (N = 28,566) | Eating Garlic, Ginger, or Lemon (N = 28,632) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Absolute Frequency | Weighted Proportion * | Absolute Frequency | Weighted Proportion * | Absolute Frequency | Weighted Proportion * | ||||
| n | % | 95% CI | N | % | 95% CI | n | % | 95% CI | |
| Gender | |||||||||
| Female | 15,862 | 50.0 | 49.5–50.5 | 15,864 | 50.3 | 49.7–50.8 | 15,808 | 49.7 | 49.3–50.2 |
| Male | 12,665 | 49.8 | 49.2–50.3 | 12,622 | 49.0 | 47.8–50.2 | 12,758 | 50.0 | 49.5–50.4 |
| Not binary | 63 | 0.2 | 0.1–0.3 | 80 | 0.7 | 0.3–1.6 | 66 | 0.3 | 0.2–0.4 |
| Age (years) | |||||||||
| 18–30 | 8665 | 30.8 | 26.4–35.6 | 8701 | 30.3 | 26.8–34.1 | 8726 | 30.2 | 26.0–34.8 |
| 31–40 | 7035 | 20.7 | 19.2–22.4 | 7064 | 20.4 | 20.2–20.7 | 7051 | 21.4 | 20.0–22.9 |
| 41–50 | 5504 | 18.3 | 17.6–18.9 | 5404 | 17.7 | 17.6–17.8 | 5576 | 18.4 | 17.6–19.2 |
| 51–60 | 4405 | 15.7 | 14.9–16.5 | 4397 | 15.9 | 14.4–17.4 | 4345 | 15.6 | 14.7–16.5 |
| 61–70 | 2285 | 11.0 | 9.2–13.1 | 2357 | 11.6 | 9.9–13.4 | 2300 | 10.9 | 9.9–12.1 |
| 71–80 | 621 | 3.0 | 2.2–4.2 | 567 | 3.3 | 2.8–4.0 | 558 | 3.0 | 2.1–4.1 |
| 80 or more | 75 | 0.5 | 0.4–0.6 | 76 | 0.8 | 0.4–1.4 | 76 | 0.5 | 0.4–0.6 |
| Education level | |||||||||
| Less than primary school | 365 | 3.7 | 1.3–10.5 | 368 | 3.8 | 1.2–11.0 | 362 | 3.2 | 1.1–9.1 |
| Primary school | 1709 | 9.8 | 5.9–15.8 | 1773 | 9.6 | 5.4–16.6 | 1653 | 9.1 | 5.4–15.0 |
| Secondary school | 10,829 | 42.4 | 36.2–48.8 | 10,843 | 42.1 | 36.5–47.9 | 10,926 | 43.3 | 37.1–49.6 |
| College/University | 12,097 | 33.7 | 20.8–49.6 | 12,043 | 33.6 | 20.0–50.5 | 12,115 | 33.8 | 20.9–49.7 |
| Graduate school | 3590 | 10.4 | 8.7–12.4 | 3539 | 10.9 | 8.7–13.5 | 3576 | 10.6 | 8.6–13.0 |
| Living area | |||||||||
| City | 23,940 | 86.2 | 75.4–92.7 | 23,791 | 85.9 | 74.2–92.8 | 23,911 | 86.1 | 75.5–92.5 |
| Town | 3227 | 9.0 | 3.4–21.7 | 3352 | 9.2 | 3.3–23.4 | 3266 | 9.2 | 3.4–22.3 |
| Village or rural area | 1423 | 4.8 | 4.1–5.6 | 1423 | 4.9 | 4.1–5.7 | 1455 | 4.8 | 4.0–5.7 |
| Health condition | |||||||||
| Poor | 729 | 3.2 | 2.7–3.8 | 666 | 3.0 | 2.1–4.2 | 713 | 3.2 | 2.1–4.8 |
| Fair | 4213 | 18.1 | 15.9–20.4 | 4278 | 17.9 | 15.8–20.2 | 4339 | 17.6 | 15.5–20.0 |
| Good | 9546 | 34.2 | 31.9–36.5 | 9686 | 34.2 | 30.4–38.3 | 9490 | 33.7 | 31.6–35.9 |
| Very good | 8887 | 27.0 | 25.4–28.7 | 8830 | 28.0 | 26.4–29.6 | 8896 | 28.0 | 26.6–29.4 |
| Excellent | 5215 | 17.5 | 14.1–21.5 | 5106 | 16.9 | 13.5–21.0 | 5194 | 17.4 | 14.0–21.5 |
| Vaccination intention | |||||||||
| Yes | 24,602 | 86.8 | 83.8–89.3 | 24,511 | 87.3 | 84.0–90.0 | 24,662 | 87.3 | 84.4–89.7 |
| No | 3988 | 13.2 | 10.7–16.2 | 4055 | 12.7 | 10.0–16.0 | 3970 | 12.7 | 10.3–15.6 |
| Characteristics | Use of Herbal Supplements (N = 28,590) | Use of Homeopathic Remedies (N = 28,566) | Eating Garlic, Ginger, or Lemon (N = 28,632) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | p-Value * | Yes | No | p-Value * | Yes | No | p-Value * | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | ||||
| Vaccination intention | |||||||||||||||
| Yes | 1713 | 81.0 | 22,889 | 87.2 | <0.001 | 1290 | 79.7 | 23,221 | 87.7 | <0.001 | 3126 | 81.1 | 21,536 | 88.1 | <0.001 |
| No | 458 | 19.0 | 3530 | 12.8 | 340 | 20.3 | 3715 | 12.3 | 772 | 18.9 | 3198 | 11.9 | |||
| Gender | |||||||||||||||
| Female | 1238 | 54.2 | 14,624 | 49.7 | 0.043 | 885 | 51.2 | 14,979 | 50.2 | 0.521 | 2109 | 53.5 | 13,699 | 49.3 | <0.001 |
| Male | 927 | 45.4 | 11,738 | 50.1 | 737 | 48.5 | 11,885 | 49.0 | 1774 | 46.0 | 10,984 | 50.5 | |||
| Not binary | 6 | 0.4 | 57 | 0.2 | 8 | 0.3 | 72 | 0.8 | 15 | 0.5 | 51 | 0.2 | |||
| Age (years) | |||||||||||||||
| 18–30 | 584 | 24.5 | 8081 | 31.3 | <0.001 | 516 | 29.3 | 8185 | 30.4 | 0.052 | 1085 | 24.9 | 7641 | 31.0 | <0.001 |
| 31–40 | 492 | 19.2 | 6543 | 20.9 | 377 | 17.6 | 6687 | 20.6 | 894 | 19.2 | 6157 | 21.7 | |||
| 41–50 | 456 | 19.5 | 5048 | 18.2 | 298 | 19.0 | 5106 | 17.7 | 741 | 17.3 | 4835 | 18.5 | |||
| 51–60 | 376 | 17.0 | 4029 | 15.6 | 278 | 18.9 | 4119 | 15.7 | 680 | 18.7 | 3665 | 15.2 | |||
| 61–70 | 209 | 15.3 | 2076 | 10.7 | 129 | 9.9 | 2228 | 11.6 | 388 | 15.5 | 1912 | 10.3 | |||
| 71–80 | 52 | 4.4 | 569 | 2.9 | 28 | 4.3 | 539 | 3.3 | 97 | 4.0 | 461 | 2.8 | |||
| 80 or more | 2 | 0.1 | 73 | 0.5 | 4 | 1.0 | 72 | 0.8 | 13 | 0.4 | 63 | 0.5 | |||
| Education level | |||||||||||||||
| Less than primary school | 30 | 3.5 | 335 | 3.8 | 0.022 | 11 | 2.6 | 357 | 3.9 | 0.002 | 48 | 3.4 | 314 | 3.2 | 0.320 |
| Primary school | 110 | 11.6 | 1599 | 9.6 | 94 | 8.8 | 1679 | 9.6 | 217 | 9.6 | 1436 | 9.1 | |||
| Secondary school | 671 | 35.6 | 10,158 | 42.9 | 503 | 32.5 | 10,340 | 42.6 | 1378 | 38.8 | 9548 | 43.8 | |||
| College/University | 1022 | 36.1 | 11,075 | 33.5 | 768 | 40.8 | 11,275 | 33.2 | 1746 | 36.9 | 10,369 | 33.4 | |||
| Graduate school | 338 | 13.2 | 3252 | 10.2 | 254 | 15.3 | 3285 | 10.7 | 509 | 11.3 | 3067 | 10.5 | |||
| Living area | |||||||||||||||
| City | 1752 | 84.9 | 22,188 | 86.3 | 0.472 | 1274 | 82.4 | 22,517 | 86.1 | 0.092 | 3095 | 83.6 | 20,816 | 86.4 | 0.297 |
| Town | 298 | 10.5 | 2929 | 8.9 | 237 | 9.8 | 3115 | 9.2 | 540 | 11.4 | 2726 | 8.9 | |||
| Village or rural area | 121 | 4.6 | 1302 | 4.8 | 119 | 7.8 | 1304 | 4.7 | 263 | 5.0 | 1192 | 4.7 | |||
| Health condition | |||||||||||||||
| Poor | 72 | 5.2 | 657 | 3.1 | 0.004 | 44 | 3.6 | 622 | 3.0 | 0.013 | 112 | 3.5 | 601 | 3.2 | 0.007 |
| Fair | 368 | 19.0 | 3845 | 18.0 | 216 | 14.8 | 4062 | 18.0 | 643 | 19.3 | 3696 | 17.4 | |||
| Good | 659 | 30.9 | 8887 | 34.4 | 492 | 31.9 | 9194 | 34.4 | 1184 | 29.1 | 8306 | 34.3 | |||
| Very good | 628 | 24.1 | 8259 | 27.3 | 514 | 27.1 | 8316 | 28.0 | 1141 | 28.3 | 7755 | 28.0 | |||
| Excellent | 444 | 20.8 | 4771 | 17.2 | 364 | 22.6 | 4742 | 16.6 | 818 | 19.7 | 4376 | 17.1 | |||
| Exposure | No Vaccination Intention | |||
|---|---|---|---|---|
| Crude Model a | Adjusted Model a,b | |||
| cPR (95% CI) | p-Value | aPR (95% CI) | p-Value | |
| Use of herbal supplements | ||||
| No | Ref. | --- | Ref. | --- |
| Yes | 1.49 (1.34–1.65) | <0.001 | 1.44 (1.30–1.58) | <0.001 |
| Use of homeopathic remedies | ||||
| No | Ref. | --- | Ref. | --- |
| Yes | 1.64 (1.31–2.06) | <0.001 | 1.58 (1.25–1.98) | 0.001 |
| Eating garlic, ginger or lemon | ||||
| No | Ref. | --- | Ref. | --- |
| Yes | 1.59 (1.56–1.62) | <0.001 | 1.55 (1.50–1.61) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bendezu-Quispe, G.; Benites-Meza, J.K.; Urrunaga-Pastor, D.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Rodriguez-Morales, A.J.; Toro-Huamanchumo, C.J.; Hernandez, A.V.; Benites-Zapata, V.A. Consumption of Herbal Supplements or Homeopathic Remedies to Prevent COVID-19 and Intention of Vaccination for COVID-19 in Latin America and the Caribbean. Trop. Med. Infect. Dis. 2022, 7, 95. https://doi.org/10.3390/tropicalmed7060095
Bendezu-Quispe G, Benites-Meza JK, Urrunaga-Pastor D, Herrera-Añazco P, Uyen-Cateriano A, Rodriguez-Morales AJ, Toro-Huamanchumo CJ, Hernandez AV, Benites-Zapata VA. Consumption of Herbal Supplements or Homeopathic Remedies to Prevent COVID-19 and Intention of Vaccination for COVID-19 in Latin America and the Caribbean. Tropical Medicine and Infectious Disease. 2022; 7(6):95. https://doi.org/10.3390/tropicalmed7060095
Chicago/Turabian StyleBendezu-Quispe, Guido, Jerry K. Benites-Meza, Diego Urrunaga-Pastor, Percy Herrera-Añazco, Angela Uyen-Cateriano, Alfonso J. Rodriguez-Morales, Carlos J. Toro-Huamanchumo, Adrian V. Hernandez, and Vicente A. Benites-Zapata. 2022. "Consumption of Herbal Supplements or Homeopathic Remedies to Prevent COVID-19 and Intention of Vaccination for COVID-19 in Latin America and the Caribbean" Tropical Medicine and Infectious Disease 7, no. 6: 95. https://doi.org/10.3390/tropicalmed7060095