
Characteristics of Respiratory Syncytial Virus versus Influenza Infection in Hospitalized Patients of Peru: A Retrospective Observational Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Source of Data
2.3. Statistical Analyses
2.4. Ethics Statements
3. Results
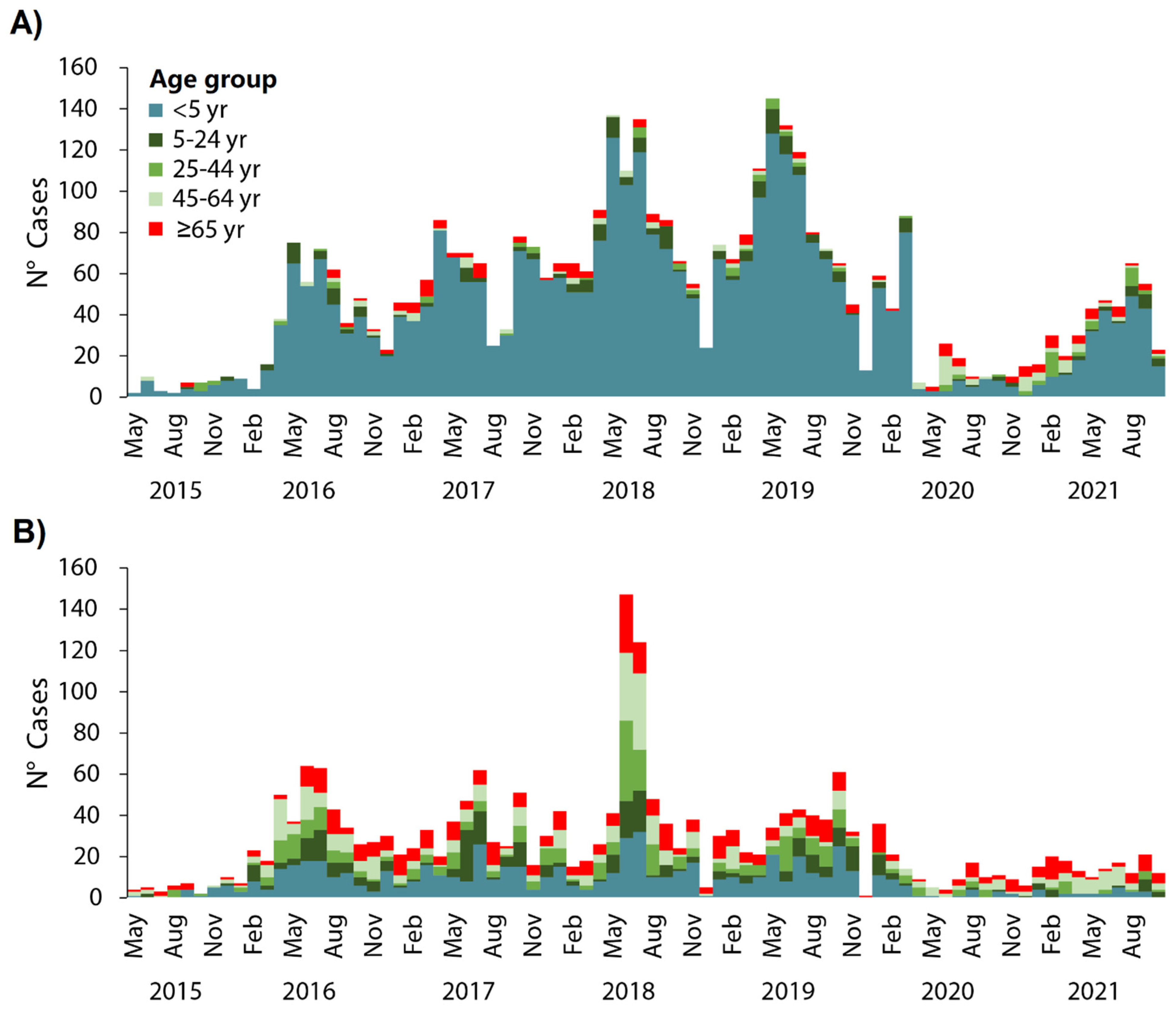
3.1. RSV and Influenza Hospitalization Seasonal Trends
3.2. Comparison of the Demographic and Clinical Characteristics of RSV- and Influenza-Hospitalized Patients
3.3. Comparison of the Complications of RSV-Hospitalized Patients
3.4. Comparison of the Complications of Influenza-Hospitalized Patients
3.5. Comparison of the Pneumonia in RSV- and Influenza-Hospitalized Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD; Lower Respiratory Infections Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef] [Green Version]
- Shi, T.; McLean, K.; Campbell, H.; Nair, H. Aetiological role of common respiratory viruses in acute lower respiratory infections in children under five years: A systematic review and meta-analysis. J. Glob. Health 2015, 5, 010408. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Arnott, A.; Semogas, I.; Falsey, A.R.; Openshaw, P.; Wedzicha, J.A.; Campbell, H.; Nair, H.; RESCEU Investigators. The Etiological Role of Common Respiratory Viruses in Acute Respiratory Infections in Older Adults: A Systematic Review and Meta-analysis. J. Infect. Dis. 2020, 222 (Suppl. 7), S563–S569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simoes, E.A.F.; Campbell, H.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: A systematic analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [PubMed]
- Shi, T.; McAllister, D.A.; O’Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: A systematic review and modelling study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Li, Y.; O’Brien, K.L.; Madhi, S.A.; Widdowson, M.A.; Byass, P.; Omer, S.B.; Abbas, Q.; Ali, A.; Amu, A.; et al. Global burden of respiratory infections associated with seasonal influenza in children under 5 years in 2018: A systematic review and modelling study. Lancet Glob. Health 2020, 8, e497–e510. [Google Scholar] [CrossRef] [Green Version]
- GBD; Influenza Collaborators. Mortality, morbidity, and hospitalisations due to influenza lower respiratory tract infections, 2017: An analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2019, 7, 69–89. [Google Scholar] [CrossRef] [Green Version]
- Wu, A.; Budge, P.J.; Williams, J.; Griffin, M.R.; Edwards, K.M.; Johnson, M.; Zhu, Y.; Hartinger, S.; Verastegui, H.; Gil, A.I.; et al. Incidence and Risk Factors for Respiratory Syncytial Virus and Human Metapneumovirus Infections among Children in the Remote Highlands of Peru. PLoS ONE 2015, 10, e0130233. [Google Scholar] [CrossRef] [Green Version]
- Del Valle-Mendoza, J.; Cornejo-Tapia, A.; Weilg, P.; Verne, E.; Nazario-Fuertes, R.; Ugarte, C.; Del Valle, L.J.; Pumarola, T. Incidence of respiratory viruses in Peruvian children with acute respiratory infections. J. Med. Virol. 2015, 87, 917–924. [Google Scholar] [CrossRef] [Green Version]
- Cherry, C.B.; Griffin, M.R.; Edwards, K.M.; Williams, J.V.; Gil, A.I.; Verastegui, H.; Lanata, C.F.; Grijalva, C.G. Spatial and Temporal Spread of Acute Viral Respiratory Infections in Young Children Living in High-altitude Rural Communities: A Prospective Household-based Study. Pediatr. Infect. Dis. J. 2016, 35, 1057–1061. [Google Scholar] [CrossRef]
- Budge, P.J.; Griffin, M.R.; Edwards, K.M.; Williams, J.V.; Verastegui, H.; Hartinger, S.M.; Johnson, M.; Klemenc, J.M.; Zhu, Y.; Gil, A.I.; et al. A household-based study of acute viral respiratory illnesses in Andean children. Pediatr. Infect. Dis. J. 2014, 33, 443–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Valle-Mendoza, J.; Silva-Caso, W.; Cornejo-Tapia, A.; Orellana-Peralta, F.; Verne, E.; Ugarte, C.; Aguilar-Luis, M.A.; De Lama-Odría, M.D.C.; Nazario-Fuertes, R.; Esquivel-Vizcarra, M.; et al. Molecular etiological profile of atypical bacterial pathogens, viruses and coinfections among infants and children with community acquired pneumonia admitted to a national hospital in Lima, Peru. BMC Res. Notes 2017, 10, 688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochoa, T.J.; Bautista, R.; Dávila, C.; Salazar, J.A.; Bazán, C.; Guerra, O.; Llanos, J.P.; López, L.; Zea-Vera, A.; Ecker, L. Respiratory syncytial virus-associated hospitalizations in pre-mature infants in Lima, Peru. Am. J. Trop. Med. Hyg. 2014, 91, 1029–1034. [Google Scholar] [CrossRef] [Green Version]
- Palekar, R.S.; Rolfes, M.A.; Arriola, C.S.; Acosta, B.O.; Guidos, P.A.; Vargas, X.B.; Bancej, C.; Ramirez, J.B.; Baumeister, E.; Bruno, A.; et al. Burden of influenza-associated respiratory hospitalizations in the Americas, 2010–2015. PLoS ONE 2019, 14, e0221479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinoco, Y.O.; Azziz-Baumgartner, E.; Uyeki, T.M.; Rázuri, H.R.; Kasper, M.R.; Romero, C.; Silva, M.E.; Simons, M.P.; Soto, G.M.; Widdowson, M.-A.; et al. Burden of Influenza in 4 Ecologically Distinct Regions of Peru: Household Active Surveillance of a Community Cohort, 2009–2015. Clin. Infect. Dis. 2017, 65, 1532–1541. [Google Scholar] [CrossRef] [Green Version]
- Rabarison, J.H.; Tempia, S.; Harimanana, A.; Guillebaud, J.; Razanajatovo, N.H.; Ratsitorahina, M.; Heraud, J.M. Burden and epidemiology of influenza- and respiratory syncytial virus-associated severe acute respiratory illness hospitalization in Madagascar, 2011–2016. Influenza Other Respir. Viruses 2019, 13, 138–147. [Google Scholar] [CrossRef]
- Učakar, V.; Sočan, M.; Trilar, K.P. The impact of influenza and respiratory syncytial virus on hospitalizations for lower respiratory tract infections in young children: Slovenia, 2006–2011. Influenza Other Respir. Viruses 2013, 7, 1093–1102. [Google Scholar] [CrossRef] [Green Version]
- Buchan, S.A.; Chung, H.; Karnauchow, T.; McNally, J.D.; Campitelli, M.A.; Gubbay, J.B.; Katz, K.; McGeer, A.J.; Richardson, D.C.; Richardson, S.E.; et al. Characteristics and Outcomes of Young Children Hospitalized with Laboratory-confirmed Influenza or Respiratory Syncytial Virus in Ontario, Canada, 2009–2014. Pediatr. Infect. Dis. J. 2019, 38, 362–369. [Google Scholar] [CrossRef]
- Ackerson, B.; Tseng, H.F.; Sy, L.S.; Solano, Z.; Slezak, J.; Luo, Y.; Fischetti, C.A.; Shinde, V. Severe Morbidity and Mortality Associated with Respiratory Syncytial Virus Versus Influenza Infection in Hospitalized Older Adults. Clin. Infect. Dis. 2019, 69, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Loubet, P.; Lenzi, N.; Valette, M.; Foulongne, V.; Krivine, A.; Houhou, N.; Lagathu, G.; Rogez, S.; Alain, S.; Duval, X.; et al. Clinical characteristics and outcome of respiratory syncytial virus infection among adults hospitalized with influenza-like illness in France. Clin. Microbiol. Infect. 2017, 23, 253–259. [Google Scholar] [CrossRef]
- Superintendencia Nacional de Salud. Consolidated Morbidity in Hospitalization 2015–2021; SUSALUD: Lima, Peru, 2022. Available online: http://datos.susalud.gob.pe/dataset/consulta-d2-consolidado-de-morbilidad-en-hospitalizacion (accessed on 30 August 2022).
- Li, Y.; Reeves, R.M.; Wang, X.; Bassat, Q.; Brooks, W.A.; Cohen, C.; Moore, D.P.; Nunes, M.; Rath, B.; Campbell, H.; et al. Global patterns in monthly activity of influenza virus, respiratory syncytial virus, parainfluenza virus, and metapneumovirus: A systematic analysis. Lancet Glob. Health 2019, 7, e1031–e1045. [Google Scholar] [CrossRef] [Green Version]
- Center for Diseases Control of Ministry of Health of Peru. Pneumonia Situational Room 2022; CDC: Lima, Peru, 2022. Available online: https://www.dge.gob.pe/sala-monkeypox/#an%C3%A1lisis-descriptivo (accessed on 21 August 2022).
- Liu, P.; Xu, M.; Cao, L.; Su, L.; Lu, L.; Dong, N.; Jia, R.; Zhu, X.; Xu, J. Impact of COVID-19 pandemic on the prevalence of respiratory viruses in children with lower respiratory tract infections in China. Virol. J. 2021, 18, 159. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, M.A.; Pollara, C.; Gargiulo, F.; Giacomelli, M.; Caruso, A. Circulation of Respiratory Viruses in Hospitalized Adults before and during the COVID-19 Pandemic in Brescia, Italy: A Retrospective Study. Int. J. Environ. Res. Public Health 2021, 18, 9525. [Google Scholar] [CrossRef]
- Vittucci, A.C.; Piccioni, L.; Coltella, L.; Ciarlitto, C.; Antilici, L.; Bozzola, E.; Midulla, F.; Palma, P.; Perno, C.F.; Villani, A. The Disappearance of Respiratory Viruses in Children during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 9550. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.W.; Bialasiewicz, S.; Dwyer, D.E.; Dilcher, M.; Tellier, R.; Taylor, J.; Hua, H.; Jennings, L.; Kok, J.; Levy, A.; et al. Where have all the viruses gone? Disappearance of seasonal respiratory viruses during the COVID-19 pandemic. J. Med. Virol. 2021, 93, 4099–4101. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, K.G.; Øymar, K.; Dalen, I.; Halvorsen, T.; Mikalsen, I.B. Asthma, atopy and lung function in young adults after hospitalisation for bronchiolitis in infancy: Impact of virus and sex. BMJ Open Respir. Res. 2022, 9, e001095. [Google Scholar] [CrossRef] [PubMed]
- Chuaychoo, B.; Rattanasaengloet, K.; Banlengchit, R.; Horthongkham, N.; Athipanyasilp, N.; Totanarungroj, K.; Muangman, N. Characteristics, complications, and mortality of respiratory syncytial virus compared with influenza infections in hospitalized adult patients in Thailand. Int. J. Infect. Dis. 2021, 110, 237–246. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| RSV-Associated Hospitalization | Influenza-Associated Hospitalization | |||||
|---|---|---|---|---|---|---|
| Male, n (%) | Female, n (%) | Total, n (%) | Male, n (%) | Female, n (%) | Total, n (%) | |
| Age group (in y) | ||||||
| <5 | 1276 (85.6) | 1046 (86.7) | 2322 (86.1) | 273 (35.7) | 231 (28.9) | 504 (32.2) |
| 5–24 | 82 (5.5) | 53 (4.4) | 135 (5.0) | 106 (13.9) | 115 (14.4) | 221 (14.1) |
| 25–44 | 36(2.4) | 26 (2.2) | 62 (2.3) | 105 (13.7) | 129 (16.2) | 234 (15.0) |
| 45–64 | 44 (3.0) | 29 (2.4) | 73 (2.7) | 147 (19.2) | 150 (18.8) | 297 (19.0) |
| ≥65 | 52 (3.5) | 52 (4.3) | 104 (3.9) | 134 (15.7) | 173 (21.7) | 307 (19.6) |
| All ages | 1490 (55.2) | 1206 (44.8) | 2696 (100) | 765 (49.0) | 798 (51.0) | 1563 (100) |
| Year | ||||||
| 2015 | 18 (1.2) | 15 (1.2) | 33 (1.2) | 18 (2.4) | 20 (2.5) | 38 (2.4) |
| 2016 | 186 (12.5) | 162 (13.4) | 348 (12.9) | 136 (17.8) | 168 (21.1) | 304 (19.4) |
| 2017 | 254 (17.0) | 227 (18.8) | 481 (17.8) | 122 (15.9) | 145 (18.2) | 267 (17.1) |
| 2018 | 387 (26.0) | 298 (24.7) | 685 (25.4) | 218 (28.5) | 206 (25.8) | 424 (27.1) |
| 2019 | 374 (25.1) | 299 (24.8) | 673 (25.0) | 157 (20.5) | 159 (19.9) | 316 (20.2) |
| 2020 | 104 (7.0) | 79 (6.6) | 183 (6.8) | 71 (9.3) | 46 (5.8) | 117 (7.5) |
| 2021 | 167 (11.2) | 126 (10.4) | 293 (10.9) | 43 (5.6) | 54 (6.8) | 97 (6.2) |
| Region | ||||||
| Coast | 941 (63.2) | 744 (61.7) | 1685 (62.5) | 549 (71.8) | 547 (68.5) | 1096 (70.1) |
| Highlands | 450 (30.2) | 378 (31.3) | 828 (30.7) | 176 (23.0) | 200 (25.1) | 376 (24.1) |
| Jungle | 99 (6.6) | 84 (7.0) | 183 (6.8) | 40 (5.2) | 51 (6.4) | 91 (5.8) |
| Department | ||||||
| Amazonas | 2 (0.1) | 3 (0.2) | 5 (0.2) | 5 (0.7) | 11 (1.4) | 16 (1.0) |
| Ancash | 53 (3.6) | 47 (3.9) | 100 (3.7) | 13 (1.7) | 5 (0.6) | 18 (1.2) |
| Apurimac | 14 (0.9) | 14 (1.2) | 28 (1.0) | 6 (0.8) | 17 (2.1) | 23 (1.5) |
| Arequipa | 31 (2.1) | 26 (2.2) | 57 (2.1) | 71 (9.3) | 81 (10.2) | 152 (9.7) |
| Ayacucho | 70 (4.7) | 68 (5.6) | 138 (5.1) | 9 (1.2) | 8 (1.0) | 17 (1.1) |
| Cajamarca | 23 (1.5) | 17 (1.4) | 40 (1.5) | 12 (1.6) | 14 (1.8) | 26 (1.7) |
| Callao | 67 (4.5) | 49 (4.1) | 116 (4.3) | 55 (7.2) | 53 (6.6) | 108 (6.9) |
| Cusco | 76 (5.1) | 80 (6.6) | 156 (5.8) | 19 (2.5) | 21 (2.6) | 40 (2.6) |
| Huancavelica | 32 (2.1) | 19 (1.6) | 51 (1.9) | 9 (1.2) | 16 (2.0) | 25 (1.6) |
| Huanuco | 14 (0.9) | 16 (1.3) | 30 (1.1) | 6 (0.8) | 4 (0.5) | 10 (0.6) |
| Ica | 29 (1.9) | 23 (1.9) | 52 (1.9) | 10 (1.3) | 12 (1.5) | 22 (1.4) |
| Junin | 59 (4.0) | 39 (3.2) | 98 (3.6) | 14 (1.8) | 14 (1.8) | 28 (1.8) |
| La Libertad | 17 (1.1) | 15 (1.2) | 32 (1.2) | 25 (3.3) | 46 (5.8) | 71 (4.5) |
| Lambayeque | 100 (6.7) | 82 (6.8) | 182 (6.8) | 33 (4.3) | 32 (4.0) | 65 (4.2) |
| Lima | 653 (43.8) | 522 (43.3) | 1175 (43.6) | 387 (50.6) | 384 (48.1) | 771 (49.3) |
| Loreto | 42 (2.8) | 40 (3.3) | 82 (3.0) | 15 (2.0) | 13 (1.6) | 28 (1.8) |
| Madre de Dios | 12 (0.8) | 5 (0.4) | 17 (0.6) | 2 (0.3) | 2 (0.3) | 4 (0.3) |
| Moquegua | 4 (0.3) | 2 (0.2) | 6 (0.2) | 2 (0.3) | 2 (0.3) | 4 (0.3) |
| Pasco | 3 (0.2) | 3 (0.2) | 6 (0.2) | 3 (0.4) | 1 (0.1) | 4 (0.3) |
| Piura | 51 (3.4) | 45 (3.7) | 96 (3.6) | 31 (4.1) | 13 (1.6) | 44 (2.8) |
| Puno | 75 (5.0) | 49 (4.1) | 124 (4.6) | 14 (1.8) | 19 (2.4) | 33 (2.1) |
| San Martin | 13 (0.9) | 8 (0.7) | 21 (0.8) | 16 (2.1) | 22 (2.8) | 38 (2.4) |
| Tacna | 11 (0.7) | 2 (0.2) | 13 (0.5) | 4 (0.5) | 3 (0.4) | 7 (0.4) |
| Tumbes | 9 (0.6) | 4 (0.3) | 13 (0.5) | 2 (0.3) | 2 (0.3) | 4 (0.3) |
| Ucayali | 30 (2.0) | 28 (2.3) | 58 (2.2) | 2 (0.3) | 3 (0.4) | 5 (0.3) |
| Disease Type | ||||||
| Bronchiolitis | 1188 (79.7) | 974 (80.8) | 2162 (80.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Pneumonia | 244 (16.4) | 184 (15.3) | 428 (15.9) | 416 (54.4) | 403 (50.5) | 819 (52.4) |
| Bronchitis | 58 (3.9) | 48 (4.0) | 106 (3.9) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Other complications by influenza | – | – | – | 349 (45.6) | 395 (49.5) | 744 (47.6) |
| Age Group (in y) | RSV-Associated Hospitalization | Influenza-Associated Hospitalization | p-Value * | ||
|---|---|---|---|---|---|
| N = 2696 | (%) | N = 1563 | (%) | ||
| 2015 | |||||
| <5 | 25 | 75.8 | 16 | 42.1 | 0.004 |
| ≥5 | 8 | 24.2 | 22 | 57.9 | |
| 2016 | |||||
| <5 | 309 | 88.8 | 92 | 31.3 | <0.0001 |
| ≥5 | 39 | 11.2 | 212 | 68.7 | |
| 2017 | |||||
| <5 | 428 | 89 | 104 | 39 | <0.0001 |
| ≥5 | 53 | 11 | 163 | 61 | |
| 2018 | |||||
| <5 | 608 | 88.8 | 123 | 29.0 | <0.0001 |
| ≥5 | 77 | 11.2 | 301 | 71.0 | |
| 2019 | |||||
| <5 | 601 | 89.3 | 118 | 37.3 | <0.0001 |
| ≥5 | 72 | 10.7 | 198 | 62.7 | |
| 2020 | |||||
| <5 | 138 | 75.4 | 33 | 28.2 | <0.0001 |
| ≥5 | 45 | 24.6 | 84 | 71.8 | |
| 2021 | |||||
| <5 | 213 | 72.3 | 18 | 18.6 | <0.0001 |
| ≥5 | 80 | 27.3 | 79 | 81.4 | |
| Covariate | RSV-Associated Hospitalization | Influenza-Associated Hospitalization | Univariate Analysis | Multivariate Analysis ** | ||
|---|---|---|---|---|---|---|
| N = 2696 | N = 1563 | Crude OR (95% CI) | p-Value * | Adjusted OR (95% CI) | p-Value * | |
| Age (in y) | ||||||
| <5 | 2322 | 504 | 1 (ref) | 1 (ref) | ||
| 5–24 | 135 | 221 | 0.13 (0.10–0.16) | <0.0001 | 0.12 (0.10–0.16) | <0.0001 |
| 25–44 | 62 | 234 | 0.05 (0.04–0.07) | <0.0001 | 0.05 (0.04–0.07) | <0.0001 |
| 45–64 | 73 | 297 | 0.05 (0.04–0.07) | <0.0001 | 0.05 (0.04–0.07) | <0.0001 |
| ≥65 | 104 | 307 | 0.07 (0.05–0.09) | <0.0001 | 0.07 (0.05–0.09) | <0.0001 |
| Age group (in y) | ||||||
| <5 | 2322 | 504 | 1 (ref) | 1 (ref) | ||
| ≥5 | 374 | 1059 | 0.08 (0.07–0.09) | <0.0001 | 0.07 (0.06–0.08) | <0.0001 |
| Sex | ||||||
| Male | 1490 | 765 | 1 (ref) | 1 (ref) | ||
| Female | 1206 | 798 | 0.77 (0.68–0.87) | <0.0001 | 0.82 (0.70–0.95) | 0.011 |
| Region | ||||||
| Coast | 1685 | 1096 | 1 (ref) | 1 (ref) | ||
| Highlands | 828 | 376 | 1.43 (1.24–1.65) | <0.0001 | 1.75 (1.46–2.07) | <0.0001 |
| Jungle | 183 | 91 | 1.30 (1.00–1.70) | 0.045 | 1.75 (1.27–2.41) | 0.001 |
| Covariate | Bronchiolitis (n = 2162) | Pneumonia (n = 428) | Bronchitis (n = 106) | Adjusted OR (95% CI) * | ||
|---|---|---|---|---|---|---|
| Bronchiolitis vs. Pneumonia | Bronchiolitis vs. Bronchitis | Pneumonia vs. Bronchitis | ||||
| Age (in y) | ||||||
| <5 | 1993 | 268 | 61 | 1 (ref) | 1 (ref) | 1 (ref) |
| 5–24 | 93 | 22 | 20 | 0.53 (0.32–0.86) ** | 0.13 (0.08–0.24) ** | 0.24 (0.12–0.47) ** |
| 25–44 | 24 | 30 | 8 | 0.08 (0.04–0.14) ** | 0.09 (0.04–0.22) ** | 0.97 (0.41–2.31) |
| 45–64 | 20 | 41 | 12 | 0.04 (0.03–0.08) ** | 0.05 (0.02–0.10) ** | 0.83 (0.40–1.71) |
| ≥65 | 32 | 67 | 5 | 0.04 (0.03–0.8) ** | 0.19 (0.07–0.52) ** | 3.48 (1.31–9.23) ** |
| Age group (in y) | ||||||
| <5 | 1993 | 268 | 61 | 1 (ref) | 1 (ref) | 1 (ref) |
| ≥5 | 169 | 160 | 45 | 0.11 (0.09–0.15) ** | 0.11 (0.07–0.17) ** | 0.81 (0.52–1.27) |
| Sex | ||||||
| Male | 1188 | 244 | 58 | 1 (ref) | 1 (ref) | 1 (ref) |
| Female | 974 | 184 | 48 | 1.08 (0.86–1.37) | 0.94 (0.62–1.42) | 0.84 (0.54–1.31) |
| Region | ||||||
| Coast | 1274 | 331 | 80 | 1 (ref) | 1 (ref) | 1 (ref) |
| Highlands | 732 | 76 | 20 | 3.67 (2.69–5.01) ** | 2.32 (1.38–3.90) ** | 0.69 (0.38–1.27) |
| Jungle | 156 | 21 | 6 | 2.53 (1.49–4.31) ** | 2.09 (0.86–5.06) | 0.70 (0.26–1.86) |
| Covariate | Influenza-Associated Hospitalization | Univariate Analysis | Multivariate Analysis ** | |||
|---|---|---|---|---|---|---|
| Pneumonia (n = 819) | Other Complications (n = 744) | Crude OR (95% CI) | p-Value * | Adjusted OR (95% CI) | p-Value * | |
| Age (in y) | ||||||
| <5 | 264 | 240 | 1 (ref) | 1 (ref) | ||
| 5–24 | 68 | 153 | 0.40 (0.28–0.56) | <0.0001 | 0.40 (0.29–0.56) | <0.0001 |
| 25–44 | 88 | 146 | 0.54 (0.39–0.75) | <0.0001 | 0.55 (0.40–0.76) | <0.0001 |
| 45–64 | 173 | 124 | 1.26 (0.94–1.69) | 0.107 | 1.27 (0.95–1.70) | 0.105 |
| ≥65 | 226 | 81 | 2.53 (1.86–3.45) | <0.0001 | 2.56 (1.88–3.50) | <0.0001 |
| Age group (in y) | ||||||
| <5 | 264 | 240 | 1 (ref) | 1 (ref) | ||
| ≥5 | 555 | 504 | 1.00 (0.80–1.23) | 0.992 | 1.00 (0.81–1.24) | 0.963 |
| Sex | ||||||
| Male | 416 | 349 | 1 (ref) | 1 (ref) | ||
| Female | 403 | 395 | 0.85 (0.70–1.04) | 0.125 | 0.83 (0.67–1.02) | 0.079 |
| Region | ||||||
| Coast | 570 | 526 | 1 (ref) | 1 (ref) | ||
| Highlands | 207 | 169 | 1.13 (0.89–1.43) | 0.307 | 1.08 (0.84–1.38) | 0.535 |
| Jungle | 42 | 49 | 0.79 (0.51–1.21) | 0.284 | 0.87 (0.56–1.37) | 0.571 |
| Covariate | RSV-Associated Hospitalization | Influenza-Associated Hospitalization | Univariate Analysis | Multivariate Analysis ** | ||
|---|---|---|---|---|---|---|
| N = 428 | N = 819 | Crude OR (95% CI) | p-Value * | Adjusted OR (95% CI) | p-Value * | |
| Age (in y) | ||||||
| <5 | 268 | 264 | 1 (ref) | 1 (ref) | ||
| 5–24 | 22 | 68 | 0.31 (0.19–0.53) | <0.0001 | 0.32 (0.19–0.52) | <0.0001 |
| 25–44 | 30 | 88 | 0.33 (0.21–0.52) | <0.0001 | 0.35 (0.22–0.55) | <0.0001 |
| 45–64 | 41 | 173 | 0.23 (0.15–0.34) | <0.0001 | 0.23 (0.16–0.34) | <0.0001 |
| ≥65 | 67 | 226 | 0.29 (021–0.40) | <0.0001 | 0.30 (0.22–0.42) | <0.0001 |
| Age group (in y) | ||||||
| <5 | 268 | 264 | 1 (ref) | 1 (ref) | ||
| ≥5 | 160 | 555 | 0.28 (0.22–0.36) | <0.0001 | 0.29 (0.22–0.37) | <0.0001 |
| Sex | ||||||
| Male | 244 | 416 | 1 (ref) | 1 (ref) | ||
| Female | 184 | 403 | 0.77 (0.61–0.98) | 0.037 | 0.80 (0.63–1.03) | 0.090 |
| Region | ||||||
| Coast | 331 | 570 | 1 (ref) | 1 (ref) | ||
| Highlands | 76 | 207 | 0.63 (0.47–0.84) | 0.002 | 0.85 (0.62–1.17) | 0.345 |
| Jungle | 21 | 42 | 0.58 (0.50–1.47) | 0.588 | 0.97 (0.55–1.72) | 0.937 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramírez-Soto, M.C.; Ortega-Cáceres, G.; Garay-Uribe, J. Characteristics of Respiratory Syncytial Virus versus Influenza Infection in Hospitalized Patients of Peru: A Retrospective Observational Study. Trop. Med. Infect. Dis. 2022, 7, 317. https://doi.org/10.3390/tropicalmed7100317
Ramírez-Soto MC, Ortega-Cáceres G, Garay-Uribe J. Characteristics of Respiratory Syncytial Virus versus Influenza Infection in Hospitalized Patients of Peru: A Retrospective Observational Study. Tropical Medicine and Infectious Disease. 2022; 7(10):317. https://doi.org/10.3390/tropicalmed7100317
Chicago/Turabian StyleRamírez-Soto, Max Carlos, Gutia Ortega-Cáceres, and Jose Garay-Uribe. 2022. "Characteristics of Respiratory Syncytial Virus versus Influenza Infection in Hospitalized Patients of Peru: A Retrospective Observational Study" Tropical Medicine and Infectious Disease 7, no. 10: 317. https://doi.org/10.3390/tropicalmed7100317