
Summary
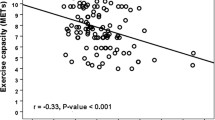
The DEFIANT-I study (Doppler Flow andEchocardiography inFunctional cardiacInsufficiency:Assessment ofNisoldipineTherapy) was a multicenter, multinational double-blind randomized study of the effects of the new calcium channel blocking drug nisoldipine on left ventricular (LV) size and function after acute myocardial infarction. Randomization to placebo or to long-acting nisoldipine core coat (20 mg once daily) was performed in 135 eligible patients with mild to moderate systolic LV dysfunction (LV ejection fraction ≤50%) 20 days (range 7–35) after infarction, with serial clinical, echocardiographic, and Doppler cardiographic measurements during a 4 week follow-up period. At the end of the follow-up period, exercise capacity was determined by bicycle ergometry. Nisoldipine improved indices of diastolic LV function. Early diastolic transmitral blood flow velocity increased, with an increase in peak E wave of 0.06 m/sec (95% confidence intervals [CI], 0.01, 0.11) and an increase in time velocity integral of 1.2 cm (95% CI, 0.16, 2.27). Isovolumic relaxation time was reduced by 14.7 msec (95% CI, −22.5, −6.9), a change not explained by the very small (and not significant) changes in systemic arterial pressure, heart rate, or cardiac output. There was no change in systolic and diastolic LV volume, nor in LV ejection fraction. Exercise capacity was greater by 12 watts (95% CI, 0.8, 23.3) in patients receiving nisoldipine, while the incidence of ≥1 mm ST-segment depression (relative occurrence 0.54, 95% CI, 0.30–0.97) and the incidence of angina pectoris (relative occurrence 0.67, 95% CI, 0.42–1.08) during exercise testing tended to be lower in this group. Although the relations were not exact, peak exercise workload 7 weeks after infarction correlated with resting measurements of diastolic LV function. Exercise workload was inversely related to peak late diastolic transmitral blood flow velocity (A wave, slope, −86.6; 95% CI, −120.9, −52.2) and directly to the E/A ratio (slope, 20.5, 95% CI, 6.0, 35.1). The relations between exercise workload and peak late diastolic flow velocity remained significant after correction for age, sex, resting heart rate, and usage of beta-blocking drugs or nisoldipine. Exercise capacity was not related to measurements of systolic LV function (LV end-diastolic and end-systolic volume, LV ejection fraction, stroke volume, cardiac index). In summary, the calcium channel blocker nisoldipine improved measurements of diastolic LV function in patients recovering from acute myocardial infarction. Exercise capacity was higher in patients receiving the drug, and there was less exercise induced ischemia. In both placebo and nisoldipine groups, exercise capacity was related to measurements of resting diastolic LV function. The observed changes in diastolic LV function during nisoldipine therapy may reflect the antiischemic effect of the drug and/or be due to an improvement in myocardial relaxation. The DEFIANT-II study, presently in progress, will examine the effect of higher doses of nisoldipine on LV function and exercise performance after acute myocardial infarction, with a longer (6 month) follow-up period.
Similar content being viewed by others


References
Wilcox RG, Hampton JR, Banks DC, et al. Trial of early nifedipine in acute myocardial infarction: The TRENT study.Br Med J 1986;293:1204–1208.
The Israeli Sprint Study Group. Secondary prevention reinfarction Israeli nifedipine trial (SPRINT): A randomised intervention trial of nifedipine in patients with acute myocardial infarction.Eur Heart J 1988;9:354–364.
The Multicenter Diltiazem Postinfarction Trial Research Group. The effect of diltiazem on mortality and reinfarction after myocardial infarction.N Engl J Med 1988;319:385–392.
The Danish Study Group on Verapamil in Myocardial Infarction. Effect of verapamil on mortality and major events after acute myocardial infarction (The Danish verapamil infarction trial II—DAVIT II).Am J Cardiol 1990;66:779–785.
Goldbourt U, Behar S, Reicher-Reiss H, Zion MM, Mandelzweig L, Kaplinsky E, for the SPRINT Study Group. Early administration of nifedipine in suspected acute myocardial infarction. The secondary prevention reinfarction Israel nifedipine trial 2 study.Arch Intern Med 1993;153:345–353.
Packer M. Pathophysiologic mechanisms underlying the adverse effects of calcium channel blocking drugs in patients with chronic heart failure.Circulation 1989;80(Suppl 4):59–67.
Nakaya H, Hattori Y, Nakao Y, Kanno M. Cardiac versus vascular effects of a new dihydropyridine derivative, CV-4093. In vitro comparison with other calcium antagonists.Eur J Pharmacol 1988;146:35–43.
Friedel HA, Sorkin EM. Nisoldipine. A preliminary review of its pharmacodynamic and pharmakokinetic properties and therapeutic efficiency in the treatment of angina pectoris, hypertension and related cardiovascular disorders.Drug 1988;36:682–731.
Lewis BS, Shefer A, Merdler A, Flugelman MY, Hardoff R, Halon DA. Effect of the second-generation calcium channel blocker nisoldipine on left ventricular contractility in cardiac failure.Am Heart J 1988;115:1238–1244.
Kimball BP, Watson KR, Bui S, Frankel D. Preservation of left ventricular performance with reduced ischemic dysfunction by intravenous nisoldipine.Am J Cardiol 1990;66:400–405.
Lopez LM, Rubin MR, Holland JP, Mehta JL. Improvement in exercise performance with nisoldipine, a new second generation calcium blocker, in stable angina patients.Am Heart J 1985;110:991–996.
Glasser SP, Arce-Weston B, Clark PI. Silent myocardial ischemia: Improvement with nisoldipine therapy.South Med J 1989;82:32–34.
The DEFIANT Research Group. Improved diastolic function with the calcium antagonist nisoldipine (coat-core) in patients post-myocardial infarction: Results of the DEFIANT study.Eur Heart J 1992;13:1496–1505.
Lewis BS, Emmott SN, Smyllie J, MacNeill AB, Lubsen J and the DEFIANT Study Group. Left ventricular systolic and diastolic function and exercise capacity 6 to 8 weeks after acute myocardial infarction.Am J Cardiol 1993;72:149–153.
Wahr DW, Wong YS, Schiller NB. Left ventricular volumes determined by two-dimensional echocardiography in a normal adult population.J Am Coll Cardiol 1983;1:863–868.
Pfeffer MA, Braunwald E, Moye LA, et al. on behalf of the SAVE investigators. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction.N Engl J Med 1992;327:669–677.
The Norwegian Multicenter Study Group. Timolol-induced reduction in mortality and reinfarction in patients surviving acute myocardial infarction.N Engl J Med 1981;304:801–807.
Beta-Blocker Heart Attack Trial Research Group. A randomized trial of propranolol in patients with acute myocardial infarction. I: Mortality results.JAMA 1982;247:1707–1714.
Yusuf S, Wittes J, Friedman L. Overview of results of randomized clinical trials in heart disease. I: Treatments following myocardial infarction.JAMA 1988;260:2088–2093.
Packer M, Nicod P, Khondheria BR, et al. Randomized multicentre, double-blind, placebo-controlled evaluation of amlodipine in patients with mild to moderate heart failure.J Am Coll Cardiol 1991;17:274.
Packer M. Calcium channel blockers in chronic heart failure. The risks of “physiologically rational therapy.”Circulation 1990;82:2254–2257.
Elkayam U, Amin J, Mehra A, Vasquez J, Weber L, Rahimtoola SH. A prospective, randomised, double-blind, cross-over study to compare the efficacy and safety of chronic nifedipine therapy with that of isosorbide dinitrate and their combination in the treatment of heart failure.Circulation 1990;82:1954–1961.
Barjon JN, Rouleau J-L, Bichet D, Juneau C, DeChamplain J. Chronic renal and neurohumoral effects of the calcium entry blocker nisoldipine in patients with congestive heart failure.J Am Coll Cardiol 1987;9:622–630.
Kassis E, Amtorp O. Long-term clinical, haemodynamic, angiographic, and neurohumoral responses to vasodilation with felodipine in patients with chronic congestive heart failure.J Cardiovasc Pharmacol 1990;15:347–352.
Dunselman PHJM, Kuntze CEE, van Bruggen A, et al. Efficacy of felodipine in congestive heart failure.Eur Heart J 1989;10:354–364.
Franciosa JA, Park M, Levine TB. Lack of correlation between exercise capacity and indexes of resting left ventricular performance in heart failure.Am J Cardiol 1981;47:33–39.
Franciosa JA. Exercise testing in chronic congestive heart failure.Am J Cardiol 1984;53:1447–1450.
McKirnan MD, Sullivan M, Jensen D, Froelicher VF. Treadmill performance and cardiac function in selected patients with coronary heart disease.J Am Coll Cardiol 1984;3:253–261.
Thadani U, Zellner SR, Glasser S, et al. Double-blind, dose-response, placebo-controlled multicenter study of nisoldipine. A new second-generation calcium channel blocker in angina pectoris.Circulation 1991;84:2398–2408.
Pouleur J, van Eyll C, Gurne O, Rousseau MF. Analysis of the mechanisms underlying the changes in left ventricular filling dynamics during oral nisoldipine therapy in patients with anterior myocardial infarction.Eur Heart J 1992;13:952–959.
Pfeffer MA, Lamas GA, Vaughan DE, Parisi AF, Braunwald E. Effect of captopril on progressive ventricular dilatation after anterior myocardial infarction.N Engl J Med 1988;319:80–86.
Linz W, Schaper J, Wiemer G, Albus U, Scholkens BA. Ramipril prevents left ventricular hypertrophy with myocardial fibrosis without blood pressure reduction: A one year study in rats.Br J Pharmacol 1992;107:970–975.
Author information
Authors and Affiliations
Consortia
Additional information
Doppler Flow andEchocardiography inFunctional cardiacInsufficiency:Assessment ofNisoldipineTherapy.
Rights and permissions
About this article
Cite this article
Lewis, B.S., Poole-Wilson, P.A. & on behalf of the DEFIANT Study Group. The DEFIANT study of left ventricular function and exercise performance after acute myocardial infarction. Cardiovasc Drug Ther 8 (Suppl 2), 407–418 (1994). https://doi.org/10.1007/BF00877325
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF00877325