
Abstract
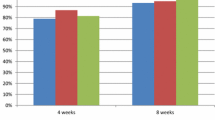
The efficacy and safety of omeprazole, 40 mg once daily for four to eight weeks of treatment, were studied in 61 patients with ulcerative reflux esophagitis. A double-blind controlled study design was used, and the patients were randomly allocated to treatment with either omeprazole 40 mg once daily or ranitidine 150 mg twice daily. Endoscopy was performed prior to inclusion into the study, after four weeks and, if unhealed, again after eight weeks. Healing of esophagitis was defined as complete disappearance of all esophageal ulcerations. Symptoms were recorded before entry, after four weeks, and again after eight weeks in unhealed patients. Fifty-one patients were included in the per-protocol analysis at day 29, and 50 patients at day 57. The healing rate after four weeks of treatment was 22 of 26 patients (85%) treated with omeprazole and 10 of 25 patients (40%) treated with ranitidine (P<0.001). The corresponding figures after eight weeks were 24 of 25 (96%), and 13 of 25 (52%) (P<0.001). These results were confirmed in the intent-to-treat analysis. Patients treated with omeprazole showed a significantly faster and more profound relief in heartburn than patients treated with ranitidine: 85% had no heartburn after four weeks of treatment with omeprazole compared to 24% in patients treated with ranitidine (P=0.00007). The percentage of patients who were free of all reflux symptoms was significantly greater in the omeprazole-treated group as compared to the ranitidine-treated group (62% and 12% respectively, P=0.0001). There were no clinically significant changes in laboratory values in any of the treatment groups. Adverse events were few and mainly mild and transient.
Similar content being viewed by others


References
Lind T, Cederberg C, Haglund U, Olbe L: Effect of omeprazole, a gastric proton-pump-inhibitor, on pentagastrin stimulated acid secretion in man. Gut 24:270–276, 1983
Lind T, Cederberg C, Ekenved G, Olbe L: Inhibition of basal and Betazole and sham-feeding-induced acid secretion by omeprazole in man. Scand J Gastroenterol 21:1004–1010, 1986
Lorentzon P, Eklundh B, BrÄndström A, Wallmark B: The mechanism for inhibition of gastric (H++K+)-ATPase by omeprazole. Biochim Biophys Acta 817:25–32, 1985
Hendrix TR, Yardley JH: Consequences of gastroesophageal reflux. Clin Gastroenterol 5:155–174, 1976
Goldberg HI, Dodds WJ, Gee S, Montgomery C, Zboralske FF: Role of acid and pepsin in acute experimental esophagitis. Gastroenterology 56:223–230, 1969
Demeester TR, Johnson LF, Joseph GJ, Toscano MS, Hall AW, Skinner DB: Patterns of gastroesophageal reflux in health and disease. Ann Surg 184:459–469, 1976
Janssens J, Vantrappen G, Peeters TL, Ghillebert G: How do 24-hour pH measurements distinguish the disease spectrum of reflux patients. Gastroenterology 88:1431, 1985
Sharma BD, Walt RP, Pounder RE, Gomes M de FA, Wood EC, Logan LH: Optimal dose of oral omeprazole for maximal 24-hour decrease of intragastric acidity. Gut 25:957–964, 1984
Naesdal J, Bodemar G, Walan A: Effect of omeprazole, a substituted benzimidazole, on 24-hour intragastric acidity in patients with peptic ulcer disease. Scand J Gastroenterol 19:916–922, 1984
Walt RP, Gomes M de FA, Wood EC, Logan LH, Pounder RE: Effect of daily oral omeprazole on 24-hour intragastric acidity. Br Med J 287:12–14, 1983
Dent J, Hetzel DJ, Reed WD, Narielvala FM, Mitchell BL, McCarthy JH: Healing of peptic esophagitis with omeprazole. Gastroenterology 90:1392, 1986
Vantrappen G, Janssens J, Ghillebert G: The irritable oesophagus, a frequent cause of pseudo-angina. Lancet 2:1232–1234, 1987.
Farrell RL, Roling GT, Castell DO: Cholinergic therapy of chronic heartburn. Ann Intern Med 80:573, 1974
McCallum RW, Ippoliti AF, Cooney RN, Sturdevant RAL: A controlled trial of metoclopramide in symptomatic gastroesophageal reflux. N Engl J Med 296:354–357, 1977
Valenzuela JE: Effects of domperidone on the symptoms of reflux oesophagitis.In Progress with Domperidone, a Gastrokinetic and Anti-emetic Agent. G Towse (ed). London, Academic Press, 1981, pp 51–56
Janssens J, Ceccatelli P, Vantrappen G: Cisapride restores the decreased lower esophageal sphincter pressure (LESP) in reflux patients. Digestion 34:139–140, 1986
Hine KR, Holmes GK, Melikian V, Lucey M, Faerclough PD: Ranitidine in reflux esophagitis. A double-blind placebo -controlled study. Digestion 29:119–123, 1984
Wesdorp E, Bartelsman J, Pape K, Dekker W, Tytgat GN: Oral cimetidine in reflux esophagitis: A double-blind controlled trial. Gastroenterology 74:821–824, 1978
Festen HPM, Diessen WMM, Lamers CBH, Van Tongeren JNM: Cimetidine in the treatment of severe reflux esophagitis; results of an 8-week double-blind study and of subsequent long-term maintenance treatment. Neth J Med 23:237–240, 1980
Lepsien G, Sonnenberg A, Berges W, Weber KB, Wienbeck M, Siewert JR, Blum AL: Die Behandlung der Reflux esophagitis mit Cimetidine. Dtsch M Wochenschr 104:901–906, 1979
Fiasse R, Hanin C, Lepot A, Descamps C, Lamy F, Dive C: Controlled trial of cimetidine in reflux esophagitis. Dig Dis Sci 25:750–755, 1980
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Vantrappen, G., Rutgeerts, L., Schurmans, P. et al. Omeprazole (40 mg) is superior to ranitidine in short-term treatment of ulcerative reflux esophagitis. Digest Dis Sci 33, 523–529 (1988). https://doi.org/10.1007/BF01798351
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01798351