
Abstract
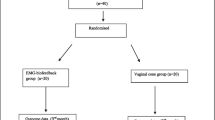
Biofeedback is a method of pelvic floor rehabilitation using a surface electrode inserted into the vagina and a catheter in the rectum. Forty women with genuine urinary stress incontinence were randomized to compare the efficacy of physiotherapy and physiotherapy in combination with biofeedback. The effect of the treatment was determined by a standardized pad-weighing test. Long-term status was determined using a questionnaire after 2–3 years. Thirty-four women completed the treatment. The study showed a statistically significant better improvement in the biofeedback group. The long-term effect in the biofeedback group seemed better and the patients were more motivated for training afterwards.
Similar content being viewed by others

References
Kegel AH. Progressive resistance exercises in the functional restoration of the perineal muscles.Am J Obtet Gynecol 1948;56:238–248
Henella SM, Kirwan P, Castleden CM, Hutchins CJ, Breeson AJ. The effect of pelvic floor exercises in the treatment of genuine urinary stress incontinence in women at two hospitals.Br J Obstet Gynaecol 1988;95:602–606
Kujansuu E. The effect of pelvic floor exercisis on urethral function in female stress urinary incotinence: a urodynamic study.Ann Chir Gynaecol 1983;72:28–32
Wilson PD, Alsamararai T, Deakin M, Kolbe E, Brown ADG. An objective assessment of physiotherapy for female genuine stress incontinence.Br J Obstet Gynecol 1987;94:575–582
Mouritsen L. Pelvic floor exercises for female stress urinary incontinence.Int Urogynecol J 1994;5:44–51
Glavind K, Nøhr SB, Walter S. Pelvic floor training using biofeedback for muscle awareness in the treatment of stress urinary incontinence: preliminary results.Int Urogynecol J 1992;3:288–291
Jacobsen H, Vedel P, Andersen JT. Objective assessment of urinary incontinence; an evaluation of three different pad-weighing tests.Neurourol Urodyn 1987;6:325–330
Lose G, Andersen JT, Kristensen JK. Disposable vaginal surface electrode for urethral sphincter electromyography.Br J Urol 1987;59:408–413
SAS Technical Report P-229. SAS/STAT Software: Changes and Enhancements, Release 6.07. Chapter 16, The MIXED Procedure Cary, NC: SAS Institute 1992
Bump R, Hurt WG, Fanlt JA, Wyman JF. Assessment of Kegel pelvic muscle exercise performance after brief verbal instruction.Am J Obstet Gynecol 1991;165:322–328
Bø K, Larsen S, Oseid S, Kvarstein B, Hagen R, Jorgensen J. Knowledge about the ability to correct pelvic floor muscle exercise in women with urinary stress incontinence.Neurourol Urodyn 1988;7:261–262
Peattie AB, Plevnik S, Stanton SL. Vaginal cones: a conservative method of treating genuine stress incontinence.Br J Obstet Gynaecol 1988;95:1049–1053
Bø K. Vaginal weight cones. Theoretical framework, effect on pelvic floor muscle strength and female stress urinary incontinence.Acta Obstet Gynecol Scand 1995;74:87–92
Sheperd AM, Conservative management. In Drife JO, Hilton P, Stanton SL (eds) Micturition. Springer-Verlag, 1990:209–219
Author information
Authors and Affiliations
Additional information
EDITORIAL COMMENT: These authors have enhanced our knowledge of physiotherapy and biofeedback in this well done study. Its design is prospective and randomized, with objective measurements of urine loss using a standardized format at 1 and 3 months. Further subjective follow-up provided the information that those trained with biofeedback were better off and that a greater proportion continued to do Kegel exercises at the mean of 2.5 years later. We need further information regarding how to predict which patients are going to repond to this type of therapy. In the non-responder group a great deal of time and effort is being wasted, owing to the personnelintensive nature of this type of therapy. Although we are not told of the parity of these patients, presumably many are multiparous, as evidenced by some who could not contract their pelvic floor at all prior to therapy. Are these the non-responders whose pelvic floors were permanently damaged during childbirth? Should all patients have pudendal motor terminal latency studies to rule out pelvic floor neuropathy, as it is unlikely that these patients will respond? These are unanswered questions and this editor would like to encourage investigators to carry this type of study further, to define who is likely to benefit from this therapy.
Rights and permissions
About this article
Cite this article
Glavind, K., Nøhr, S.B. & Walter, S. Biofeedback and physiotherapy versus physiotherapy alone in the treatment of genuine stress urinary incontinence. Int Urogynecol J 7, 339–343 (1996). https://doi.org/10.1007/BF01901111
Issue Date:
DOI: https://doi.org/10.1007/BF01901111