
Summary
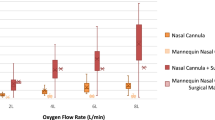
Direct measurement of the inspired trachéal oxygen concentration was made in patients breathing through standard aerosol face masks. Factors affecting the trachéal Fio2, were analyzed using both mechanical and mathematical models. When oxygen is delivered to the face mask at low flow rates, there is considerable patient variation in the measured trachéal Fio2. Delivery of oxygen at higher flow rates (15 litres per minute or greater), reduces such variation. Furthermore, turbulent air currents within and around the face mask reduce the measured Fio2 and contribute to fluctuations in the Fio2. This effect may be virtually eliminated by placing shields around the mask orifices as described. Using the shielded mask, it is possible to deliver the desired oxygen concentration to the patient more accurately and to maintain humidification of the delivered gases. Changes desired in inspired oxygen concentration are accomplished by changing the concentration of the incoming gas mixture, and not by merely changing the flow rate of oxygen delivered to the system.
Using the shielded mask, it is possible to deliver an inspired oxygen concentration of 100 per cent. This is not true with most other commonly used face masks, and, therefore, caution should be used to avoid administration of unnecessary high inspired oxygen concentrations with this type of mask.
Résumé
Grâce à des prélèvements de gaz inspirés au niveau de la trachée, on a pu déterminer la concentration de l’oxygène chez des malades respirant à l’aide de masque à aérosol et l’on a pu analyser les différents facteurs susceptibles de modifier cette concentration d’oxygène trachéal, au moyen des modèles mécaniques et mathématiques.
On a trouvé que le débit de l’oxygène arrivant au masque est d’importance considérable: en effet, à bas débits, on observe des variations très importantes de la concentration d’oxygène d’un malade à l’autre, alors que des débits de 15 litres et plus minimisent ces variations.
De plus, on a observé que la turbulence de l’air dans le masque et autour de celui-ci contribue à réduire les concentrations d’oxygène à la trachée et provoque de grandes variations d’un malade à l’autre. A toutes fins pratiques, on peut éliminer les effets de la turbulence en plaçant des protecteurs vis-à-vis les orifices du masque. Avec un masque ainsi protégé, il devient possible de fournir les concentrations d’oxygène voulues de façon plus précise et d’assurer l’humidification des gaz. Avec ce masque, il devient même possible de fournir une concentration d’oxygène à 100 pour cent, ce qui est difficilement réalisable avec les masques communément employés. Il faut donc se souvenir de la possibilité d’administrer de l’oxygène à concentration trop élevée avec ce genre de masque.
Article PDF
Similar content being viewed by others

References
West, J.B. Ventilation/blood flow and gas exchange. Oxford, Blackwell (1970).
Morgan, A.P. The pulmonary toxicity of oxygen. Anaesthesiology29: 570–579 (1968).
Burgess, A.M. A comparison of common methods of O2, therapy. Amer. J. Nurs.65: 96–99 (1965).
Today’s drugs: a rational approach to oxygen therapy. B.M.J. 5424: 1580-1582.
Flenley, D.C., Hutchison, D.C.S., &Donald, K.W. Behaviour of apparatus of oxygen administration. M.B.J.5365: 1081–1088 (1963).
Bethune, D.W. &Collis, J.M. The evaluation of oxygen masks. Anaesthesia22: 43–54 (1967).
Nunn, J.F. Applied respiratory physiology. P. 300, Butterworths (1969).
Shapiro, B.A. Clinical application of blood gases. Year Book, Chicago (1973).
Wexler, H.R., Levy, H., Cooper, J.D., &Aberman, A. A mathematical model to predict Fio2: description and validation. C.A.S.J.22: 410 (1975).
Author information
Authors and Affiliations
Additional information
Supported in part by grants from Ontario Thoracic Society No. 3-357-289-30, National Sanitarium Association No. 3-333-289-90.
Rights and permissions
About this article
Cite this article
Wexler, H.R., Aberman, A., Scott, A.A. et al. Measurement of intratracheal oxygen concentrations during face mask administration of oxygen: A modification for improved control. Canad. Anaesth. Soc. J. 22, 417–431 (1975). https://doi.org/10.1007/BF03004856
Issue Date:
DOI: https://doi.org/10.1007/BF03004856