
Abstract
Purpose
Epidural anesthesia may be difficult in pregnancy. We intended to evaluate the teaching possibilities of ultrasonography as a diagnostic approach to the epidural region.
Methods
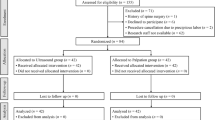
Two groups of residents performed their first 60 obstetric epidurals under supervision. One proceeded in the conventional way using the loss of resistance technique (control group = CG). The other group proceeded in the same way but was supported by prepuncture ultrasound imaging, giving them information about the optimal puncture point, depth and angle (ultrasound group = UG). Success was defined as adequate epidural anesthesia requiring a maximum of three attempts, reaching a visual analogue scale score of less than I, while neither changing the anesthesia technique, nor starting at another vertebral level. In addition, intervention by the supervisor was defined as failure.
Results
In the CG we observed asuccess rate of 60% ± 16% after the first ten attempts followed by a nearly continuous rise of the learning curve. Within the next 50 epidurals the rate of success increased to 84%. In the UG the rate of success started at 86% ± 15%. Wthin 50 epidural insertions it rose up to a level of 94%. The difference between the two groups remained significant (P < 0.001).
Conclusion
Using ultrasound imaging for teaching epidural anesthesia in obstetrics we found a higher rate of success during the first 60 attempts compared to conventional teaching. We believe this shows the possible value of ultrasound imaging for teaching and learning obstetric regional anesthesia.
Résumé
Objectif
L’anesthésie épidurale peut être difficile à réaliser pendant la grossesse. Nous avons voulu évaluer les possibilités d’apprentissage de l’échographie comme approche diagnostique de la région épidurale.
Méthode
Deux groupes de résidents ont réalisé leurs 60 premières anesthésies épidurales sous supervision. Un premier groupe a procédé de manière traditionnelle selon la technique de perte de résistance (groupe témoin = GT). Lautre groupe a fait la même chose, mais bénéficiait de l’assistance de l’échographie qui donnait des informations sur les meilleurs site, profondeur et angle de ponction (groupe d’échographie = GE). La réussite était une anesthésie épidurale adéquate exigeant au plus trois essais, affichant un score de moins de I à l’échelle visuelle analogique et n’exigeant pas de modifier la technique anesthésique, ni de faire la ponction à un autre niveau vertébral. De plus, l’intervention d’un superviseur constituait un échec.
Résultats
Un taux de un succès de 60% ± 16% a été noté dans le GT après les 10 premières tentatives suivies par une hausse presque continue de la courbe d’apprentissage. Pendant les 50 anesthésies suivantes, le taux est monté à 84 %. Dans le GE, le taux a été d’abord de 86 % ± 15 %, puis, pour les 50 anesthésies suivantes, il s’est élevé à 94 %. La différence intergroupe demeurait donc significative. (P < 0,001).
Conclusion
Lutilisation de l’échographie dans l’enseignement de l’anesthésie épidurale obstétricale, comparée à la méthode traditionnelle d’enseignement, a montré un taux de succès plus élevé pendant les 60 premiers essais. Cette expérience démontre la valeur de l’échographie dans l’enseignement et l’apprentissage de l’anesthésie obstétricale régionale.
Article PDF
Similar content being viewed by others


References
Currie JM. Measurement of the depth of the extradural space using ultrasound. Br J Anaesth 1984; 56: 345–7.
Bonazzi M, Bianchi De Grazia L, Di Gennaro S, et al. Ultrasonography-guided identification of the lumbar epidural space (Italian). Minerva Anestesiol 1995; 61: 201–5.
Kopacz DJ, Neal JM, Pollock JE. The regional anesthesia “learning curve”. What is the minimum number of epidural and spinal blocks to reach consistency? Reg Anesth 1996;21: 182–90.
Grau T, Leipold R, Conradi R, Martin E, Motsch J. Ultrasonography and peridural anesthesia. Technical possibilities and limitations of ultrasonic examination of the epidural space (German). Anaesthesist 2001; 50: 94–101.
Grau T, Leipold RW, Conradi R, Martin E. Ultrasound control for presumed difficult epidural puncture. Acta Anaesthesiol Scand 2001; 45: 766–77.
Grau T, Leipold RW, Conradi R, Martin E, Motsch J. Efficacy of ultrasound imaging in obstetric epidural anesthesia. J Clin Anesth 2002; 14: 169–75.
Dashfield AK, Coghill JC, Langton JA. Correlating obstetric epidural anaesthesia performance and psychomotor aptitude. Anaesthesia 2000; 55: 744–9.
Schuepfer G, Konrad C, Schmeck J, Poortmans G, Staffelbach B, Johr M. Generating a learning curve for pediatric caudal epidural block: an empirical evaluation of technical skills in novice and experienced anesthetists. Reg Anesth Pain Med 2000; 25: 385–8.
Konrad C, Schupfer G, Wietlisbach M, Gerber H. Learning manual skills in anesthesiology: is there a recommended number of cases for anesthetic procedures? Anesth Analg 1998; 86: 635–9.
Author information
Authors and Affiliations
Corresponding author
Additional information
Funding: Departmental; Forschungsförderungsprogramm der Universität Heidelberg.
Rights and permissions
About this article
Cite this article
Grau, T., Bartusseck, E., Conradi, R. et al. Ultrasound imaging improves learning curves in obstetric epidural anesthesia: a preliminary study. Can J Anesth 50, 1047–1050 (2003). https://doi.org/10.1007/BF03018371
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018371