
Abstract
Purpose
Several non-opioid drugs have been shown to provide analgesia during and after surgery. We compared sevoflurane anesthesia with fentanyl analgesia to sevoflurane and non-opioid drug treatment for gastric bypass surgery and recovery.
Methods
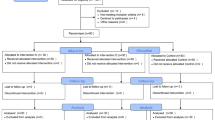
Thirty obese patients (body mass index > 50 kg·m−2) undergoing gastric bypass were randomized to receive sevoflurane anesthesia with either fentanyl or a non-opioid regimen including ketorolac, clonidine, lidocaine, ketamine, magnesium sulfate, and methylprednisolone. Morphine use by patient-controlled analgesia (PCA) pump and pain score measured by visual analogue scale were determined in the postanesthesia care unit (PACU) and for the first 16 hr after surgery. Sedation was evaluated in the PACU. Investigators assessing patient outcomes were blinded to the study group.
Results
Fentanyl treated patients were more sedated in the PACU compared to the non-opioid group. Non-opioid treated patients required 5.2 ± 2.6 mg·hr−1 morphine by PCA during their stay in the PACU while patients anesthetized with fentanyl used 7.8 ± 3.3 mg·hr−1 (P < 0.05). Fentanyl and non-opioid treated patients showed no difference in pain score one or 16 hr after surgery.
Conclusion
Our results show that non-opioid analgesia produced pain relief and less sedation during recovery from gastric bypass surgery compared to fentanyl.
Résumé
Objectif
On reconnaît à certains médicaments non-opioïdes des qualités analgésiques pendant et après une intervention chirurgicale. Nous avons comparé l’anesthésie au sévofurane accompagnée d’une analgésie, soit avec fentanyl, soit avec un non opioïde pendant et après le pontage gastrique.
Méthode
Trente patients obèses (index de masse corporelle > 50 kg·m−2) devant subir un pontage gastrique ont été répartis au hasard et ont reçu une anesthésie au sévofurane avec, soit du fentanyl, soit un schéma posologique comportant kétorolac, clonidine, lidocaïne, kétamine, sulfate de magnésium et méthylprednisolone. L’usage de morphine par une pompe d’analgésie auto-contrôlée (AAC) et le score de douleur par l’échelle visuelle analogique ont été enregistrés à la salle de réveil (SDR) et pendant les seize premières heures après l’opération. La sédation a été évaluée à la SDR. L’évaluation des patients a été faite par des chercheurs impartiaux.
Résultats
La sédation, notée à la SDR, était plus importante chez les patients traités au fentanyl, comparés à ceux traités avec un médicament non-opioïde. Les patients traités aux non-opioïdes ont demandé 5,2 ±2,6 mg·h−1 de morphine en AAC pendant leur séjour en SDR tandis que les patients anesthésiés au fentanyl en ont utilisé 7,8 ± 3,3 mg·h−1 (P < 0,05). Les scores de douleurs des patients des deux groupes n’ont présenté aucune différence, une ou 16 h après l’opération.
Conclusion
Lanalgésie avec des non opioïdes, comparé au fentanyl, a mieux soulagé la douleur et provoqué moins de sédation pendant la récupération qui suit un pontage gastrique.
Article PDF
Similar content being viewed by others


References
Adams JP, Murphy PG. Obesity in anaesthesia and intensive care. Br J Anaesth 2000; 85: 91–108.
Biring MS, Lewis MI, Liu JI, Mohsenifar Z. Pulmonary physiologic changes of morbid obesity. Am J Med Sci 1999; 318: 293–7.
Pelosi P, Croci M, Ravagnan I, et al. The effects of body mass on lung volumes, respiratory mechanics, and gas exchange during general anesthesia. Anesth Analg 1998; 87: 645–60.
Rawal N, Sjostrand U, Christofferson E, Dahlstrom B, Arvill A, Rydman H. Comparison of intramuscular and epidural morphine for postoperative analgesia in the grossly obese. Influence of postoperative ambulation and pulmonary function. Anesth Analg 1984; 63: 583–92.
VanDercar DH, Martinez AP, De Lisser EA. Sleep apnea syndromes: a potential contraindication for patient-controlled analgesia. Anesthesiology 1991; 74: 623–4.
White PF. The role of non-opioid analgesic techniques in the management of pain after ambulatory surgery. Anesth Analg 2002; 94: 577–85.
Groudine SB, Fisher AG, Kaufman RP Jr, et al. Intravenous lidocaine speeds the return of bowel function, decreases postoperative pain, and shortens hospital stay in patients undergoing radical retropubic prostatectomy. Anesth Analg 1998; 86: 235–9.
Schulz-Stubner S, Wettmann G, Reyle-Hahn SM, Rossaint R. Magnesium as part of balanced general anaesthesia with propofol, remifentanil and mivacurium: a double-blind randomized prospective study in 50 patients. Eur J Anaesthesiol 2001; 18: 723–9.
Casati A, Magistris L, Fanelli G, et al. Small-dose clonidine prolongs postoperative analgesia after sciaticfemoral nerve block with 0.75% ropivacaine for foot surgery. Anesth Analg 2000; 91: 388–92.
Adriaenssens G, Vermeyen KM, Hoffmann VLH, Mertens E, Adriaensen HF. Postoperative analgesia with i.v. patient-controlled morphine: effect of adding ketamine. Br J Anaesth 1999; 83: 393–6.
Chow GK, Fabrizio MD, Steer T, et al. Prospective double-blind study of effect of ketorolac administration after laparoscopic urologic surgery. J Endourol 2001; 15: 171–4.
Levanen J, Makela ML, Scheinin H. Dexmedetomidine premedication attenuates ketamine-induced cardiostimulatory effects and postanesthetic delirium. Anesthesiology 1995; 82: 1117–25.
Liu HT, Hollmann MW, Liu WH, Hoenemann CW, Durieux ME. Modulation of NMDA receptor function by ketamine and magnesium: part I. Anesth Analg 2001; 92: 1173–81.
Katz J. Pre-emptive analgesia: importance of timing. Can J Anesth 2001; 48: 105–14.
Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg 2002; 183: 630–41.
Wilder-Smith OH. Pre-emptive analgesia and surgical pain. Prog Brain Res 2000; 129: 505–24.
White PF, Way WL, Trevor AJ. Ketamine —its pharmacology and therapeutic uses. Anesthesiology 1982; 56: 119–36.
Taittonen MT, Kirvela OA, Aantaa R, Kanto JH. The effect of clonidine or midazolam premedication on perioperative responses during ketamine anesthesia. Anesth Analg 1998; 87: 161–7.
Morten RF, Clark LD, Tolan MM, Metz RJ, Tsueda K, Sheppard RA. The effects of small-dose ketamine on propofol sedation: respiration, postoperative mood, perception, cognition, and pain. Anesth Analg 2001; 92: 1465–9.
Menigaux C, Fletcher D, Dupont X, Guignard B, Guirimand F, Chauvin M. The benefits of intraoperative small-dose ketamine on postoperative pain after anterior cruciate ligament repair. Anesth Analg 2000; 90: 129–35.
Celerier E, Rivat C, Jun T, et al. Long-lasting hyperalgesia induced by fentanyl in rats. Anesthesiology 2000; 92: 465–72.
Laulin JP, Maurette P, Corcuff JB, Rivat C, Chauvin M, Simonnet G. The role of ketamine in preventing fentanyl-induced hyperalgesia and subsequent acute morphine tolerance. Anesth Analg 2002; 94: 1263–9.
Hirota K, Zsigmond EK, Matsuki A, Rabito SF. Topical ketamine inhibits albumin extravasation in chemical peritonitis in rats. Acta Anaesthesiol Scand 1995; 39: 174–8.
Handa F, Tanaka M, Nichikawa T, Toyooka H. Effects of oral clonidine premedication on side effects of intravenous ketamine anesthesia: a randomized, doubleblind, placebo-controlled study. J Clin Anesth 2000; 12: 19–24.
Kamibayashi T, Maze M. Clinical uses of α2-adrenergic agonists. Anesthesiology 2000; 93: 1345–9.
Ko SH, Lim HR, Kim DC, Han YJ, Choe H, Song HS. Magnesium sulfate does not reduce postoperative analgesic requirements. Anesthesiology 2001; 95: 640–6.
de Clive-Lowe SG, Desmond J, North J. Intravenous lignocaine anaesthesia. Anaesthesia 1958; 13: 139–46.
Cassuto J, Wallin G, Hogstrom S, Faxen A, Rimback G. Inhibition of postoperative pain by continuous lowdose intravenous infusion of lidocaine. Anesth Analg 1985; 64: 971–4.
Taniguchi S, Shibata K, Yamamoto K, Mizukoshi Y, Kobayashi T. Effects of lidocaine administration on hemodynamics and cytokine responses to endotoxemia in rabbits. Crit Care Med 2000; 28: 755–9.
Hollmann MW, Durieux ME. Local anesthetics and the inflammatory response. A new therapeutic indication? Anesthesiology 2000; 93: 858–75.
McCafferty DM, Sharkey KA, Wallace JL. Beneficial effects of local or systemic lidocaine in experimental colitis. Am J Physiol 1994; 266: G560–7.
Nellgard P, Jonsson A, Bojo L, Tarnow P, Cassuto J. Small-bowel obstruction and the effects of lidocaine, atropine and hexamethonium on inflammation and fluid losses. Acta Anaesthesiol Scand 1996; 40: 287–92.
Wu CL, Tella P, Staats PS, et al. Analgesic effects of intravenous lidocaine and morphine on postamputation pain. Anesthesiology 2002; 96: 841–8.
Himes RS Jr, DiFaxio CA, Burney RG. Effects of lidocaine on the anesthetic requirements for nitrous oxide and halothane. Anesthesiology 1977; 47: 437–40.
Watcha MF, Jones MB, Lagueruela RG, Schweiger C, White PF. Comparison of ketorolac and morphine as adjuvants during pediatric surgery. Anesthesiology 1992; 76: 368–72.
Ding Y, White PF. Comparative effects of ketorolac, dezocine, and fentanyl as adjuvants during outpatient anesthesia. Anesth Analg 1992; 75: 566–71.
Maunuksela EL, Kokki H, Bullingham RE. Comparison ofiv ketorolac with morphine for postoperative pain in children. Clin Pharmacol Ther 1992; 52: 436–43.
Schulze S, Moller IW, Bang U, Rye B, Kehlet H. Effect of combined prednisolone, epidural analgesia and indomethacin on pain, systemic response and convalescence after cholecystectomy. Acta Chir Scand 1990; 156: 203–9.
Glasser RS, Knego RS, Delashaw JB, Fessler RG. The perioperative use of corticosteroids and bupivacaine in the management of lumbar disc disease. J Neurosurg 1993; 78: 383–7.
Ohlms LA, Wilder RT, Weston B. Use of intraoperative corticosteroids in pediatric tonsillectomy. Arch Otolaryngol Head Neck Surg 1995; 121: 737–42.
Aasboe V, Raeder JC, Groegaard B. Betamethasone reduces postoperative pain and nausea after ambulatory surgery. Anesth Analg 1998; 87: 319–23.
Andersen G, Rasmussen H, Rosenstock C, et al. Postoperative pain control by epidural analgesia after transabdominal surgery. Efficacy and problems encountered in daily routine. Acta Anaesthesiol Scand 2000; 44: 296–301.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Feld, J.M., Laurito, C.E., Beckerman, M. et al. Non-opioid analgesia improves pain relief and decreases sedation after gastric bypass surgery. Can J Anesth 50, 336–341 (2003). https://doi.org/10.1007/BF03021029
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03021029