
Abstract
Purpose
To assess the value of serum procalcitonin (PCT) for the differentiation between patients with and without neonatal sepsis.
Methods
We systematically searched PubMed, Scopus, and the Cochrane Library for studies evaluating PCT in neonatal sepsis. PCT had to be measured in neonatal blood samples, at the initial presentation of patients with suspected sepsis, before the administration of antibiotics. We performed a bivariate meta-analysis of sensitivity and specificity, and constructed a hierarchical summary receiver-operating characteristic (HSROC) curve.
Results
Overall, 29 studies eligible for inclusion were identified. We analyzed the 16 studies (involving 1,959 neonates) that evaluated PCT in neonates with culture-proven or clinically diagnosed sepsis in comparison with ill neonates with other conditions. The pooled (95% confidence interval) sensitivity and specificity were 81% (74–87%) and 79% (69–87%), respectively. The area under the HSROC curve (AUC) was 0.87. The diagnostic accuracy of PCT seemed higher for neonates with late-onset sepsis (>72 h of life) than for those with early onset sepsis; the AUC for these analyses was 0.95 and 0.78, respectively. However, fewer data were available for late-onset sepsis. High statistical heterogeneity was observed for all analyses.
Conclusion
Our findings suggest that serum PCT at presentation has very good diagnostic accuracy (AUC = 0.87) for the diagnosis of neonatal sepsis. However, in view of the marked observed statistical heterogeneity, along with the lack of a uniform definition for neonatal sepsis, the interpretation of these findings should be done with appropriate caution.
Similar content being viewed by others


Introduction
Sepsis is an important cause of morbidity and mortality for neonates [1, 2], especially in the developing countries [3]. Rapid and accurate diagnosis of neonatal sepsis is often difficult in routine clinical practice because the clinical manifestations of this condition can overlap with those of non-infectious conditions, such as the meconium aspiration syndrome, respiratory distress syndrome, and hemodynamic instability of various underlying etiologies. Microbiological cultures aid in the identification of serious bacterial infection, but often yield false-negative results, particularly after maternal antibiotic use [4, 5], and might also yield false-positive results because of specimen contamination.
The use of several biochemical markers has been studied with the aim to improve the clinical management of neonates with suspected bacterial infection [6–8]. Yet, no single laboratory test is considered to reliably predict neonatal sepsis at the time of initial presentation. Thus, neonates with clinical manifestations of sepsis or with risk factors for serious bacterial infection are commonly treated empirically with antibiotics, awaiting the results of microbiological and other investigations [9]. This inevitably leads to overuse of antibiotics, which in turn can pose a selection pressure for multidrug-resistant bacteria in the neonatal intensive care unit [10].
Serum procalcitonin (PCT) is a biological marker of increasing interest for detecting serious bacterial infections [11], including sepsis, in adults [12], or pediatric patients and newborns [13, 14]. However, regarding neonates particularly, a physiological postnatal increase of serum PCT occurs in healthy term and preterm neonates, with peak values at 24 h of age [15–17]. Taking all the above into consideration, we aimed to assess the value of PCT for the diagnosis of neonatal sepsis by performing a diagnostic test accuracy meta-analysis of relevant studies.
Methods
Data sources
We systematically reviewed PubMed, Scopus, and the Cochrane Library databases up to 8 June 2009. The PubMed combined search term used was: (procalcitonin OR PCT) AND (neonatal sepsis OR neonatal infections OR sepsis). The search terms applied to the Scopus and the Cochrane Library were “procalcitonin and sepsis” and “procalcitonin,” respectively. The bibliographies of relevant articles were also hand-searched.
Study selection criteria
A study was considered eligible for inclusion in our review if it provided data on serum PCT for neonates with and without sepsis (either microbiologically or clinically documented). In addition, PCT blood measurement had to be performed at the time of clinical presentation with suspected sepsis before the administration of antimicrobial therapy or for asymptomatic neonates at the time of inclusion in the study. We excluded studies that used PCT measurements that were made only on maternal or umbilical cord blood samples. Conference abstracts or studies written in languages other than English, Spanish, French, German, Italian, and Greek were also excluded.
Data extraction
Data extracted from each of the included studies referred to the type of the study design, the size and characteristics of the study population, the number of patients with early/late onset of sepsis, as well as the number of patients >28 days old that were included, and the number and specific characteristics of the patients in the septic and non-septic groups. Specific data regarding the cutoff level of serum PCT evaluated, the sensitivity/specificity, and the positive/negative predictive value (PPV/NPV) of PCT for the diagnosis of neonatal sepsis were also extracted.
In cases in which major discrepancies between the data reported in the included studies and the data calculated were observed, we contacted the first or last authors of the individual studies via e-mail, requesting clarification regarding the raw data of the studied patient groups.
Definitions
Patients included in the septic group had either microbiologically (culture-proven) or clinically diagnosed sepsis, whereas patients included in the non-septic group were patients for whom the diagnosis of sepsis was excluded based on the microbiological/clinical symptoms and signs and/or if they had a benign clinical course. We considered that neonates who presented with a clinical suspicion of sepsis and required antibiotic therapy for no more than 3 days had a negative diagnosis for sepsis, in the case that this was reported in the included studies. In addition, neonatal sepsis was considered as early onset (EOS) if it was diagnosed in the first 72 h of life and late-onset (LOS) if it was diagnosed after this period.
Data analysis
In our primary analysis we included all studies that evaluated PCT in neonates with microbiologically or clinically diagnosed sepsis in comparison with ill neonates that had other conditions. Studies in which the control group consisted of healthy neonates as well as studies in which pediatric patients >28 days old constituted >25% of the total population were also excluded. Studies for which the accurate number of patients with true-/false-positive and true-/false-negative PCT results could not be calculated, such as those that only provided data for PCT sensitivity and specificity that were derived from a computed ROC curve, were also excluded from the analysis. In order to evaluate the performance of PCT for the diagnosis of early onset and late-onset neonatal sepsis separately, we performed two sub-analyses limited to studies that involved exclusively or in the majority (>85%) neonates with early onset and late-onset sepsis, respectively.
We performed a diagnostic test meta-analysis using a bivariate meta-analysis model [18] to calculate the pooled sensitivity, specificity, positive/negative likelihood ratios, as well as the diagnostic odds ratio. We also constructed the respective hierarchical summary receiver-operating characteristic (HSROC) curve that plots sensitivity versus specificity and calculated the area under the curve (AUC) [19]. Moreover, the Spearman correlation coefficient between the logits of sensitivity and specificity was used to evaluate the presence of a threshold effect in the accuracy of PCT. The presence of statistical between-study heterogeneity was assessed by the I 2 test [20]. Values of 25, 50, and 75% for the I 2 test were regarded as indicative of low, moderate, and high statistical heterogeneity, respectively. All the above analyses were performed using the Midas Module in Stata software version 10 [21, 22].
Quality assessment of the included studies
The methodological quality of the analyzed studies was assessed using the QUADAS tool [23]. Nine of the 14 items of the QUADAS tool were considered relevant for the studies included in our review. These were: representative spectrum, clear description of study selection criteria, acceptable reference standard, avoidance of partial/differential verification and incorporation biases, detailed description of index test and reference standard, and explanation of study withdrawals.
We considered the spectrum of the patients to be representative of the target population if all the evaluated patients were neonates (0–28 days) and had critical illness and/or clinical manifestations consistent with possible sepsis. If healthy neonates were included in the non-septic group, the study population was considered as non-representative. The acceptable reference standard consisted of diagnostic criteria for neonatal sepsis matching those presented in the International Pediatric Sepsis Consensus conference [24]. Partial and differential verification biases were considered to have been avoided if all the included children were evaluated with the same reference standard method used in each study, regardless of the PCT results. All calculations and analyses, including the methodological quality analysis, were performed with the use of the Review Manager (RevMan) v. 5.0 Software (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, 2008).
Results
Study selection process
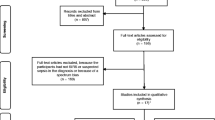
In Fig. 1, we present the flow diagram showing the process of selection of the studies included in our review. Specifically, our search in PubMed generated 623 potentially relevant articles, of which 28 were eligible for inclusion in our review. The search performed in the Cochrane Library yielded no additional articles eligible for inclusion, whereas one additional study that qualified for inclusion was identified from the search of the Scopus database. No additional eligible study was identified from hand searching of the bibliographies of relevant articles. Overall, 29 individual articles were eligible for inclusion in our review [25–53].

Flow diagram of the detailed process of selection of articles for inclusion in our review
Characteristics of the included studies
In Table 1, we present the main characteristics of the 29 included studies. Four studies had a retrospective design [27, 30–32], whereas the remaining were prospective cohort or case control studies. Seven studies exclusively involved patients with early onset neonatal sepsis [4, 27, 31, 40, 47, 49, 52], and six studies exclusively involved patients with late-onset neonatal sepsis [26, 33, 34, 42, 44]. In 4 of the 29 included studies, the comparator group consisted of patients that potentially had sepsis, on the basis of the relevant diagnostic criteria provided, and thus we did not include them in the analysis [29, 30, 41, 48]. With regard to the remaining 25 studies comparing patients with neonatal sepsis to patients without neonatal sepsis, 6 did not provide accurate PCT patient diagnostic data [37, 39, 42, 49, 50, 52], 2 involved healthy subjects as controls [33, 36], and 1 did not provide accurate PCT patient diagnostic data and also involved pediatric patients >28 days old in a percentage >25% [43]. The above-mentioned nine studies were also excluded from the analyses. In Table 2, we present the data derived from each of the 16 analyzed studies regarding the value of serum PCT for the diagnosis of neonatal sepsis. In 13 of these studies, the septic group consisted of neonates with both culture-proven sepsis and clinically diagnosed sepsis [25–27, 31, 34, 35, 38, 40, 44–47, 51], and in the remaining 3 with culture-proven sepsis alone [28, 32, 53]. The non-septic group consisted of ill neonates with other conditions that were hospitalized in the pediatric ICU in all but three of these studies [34, 51, 53].
Methodological quality of the included studies
In Fig. 2, we summarize the results of the methodological assessment for the total of the 29 studies included in the meta-analysis.

Methodological quality graph depicting the cumulative findings of the methodological quality analysis of the studies included in the meta-analysis
Diagnostic accuracy of PCT
Sixteen studies, involving a total of 1,959 neonates, were included in our primary analysis [25–28, 31, 32, 34, 35, 38, 40, 44–47, 51, 53]. The pooled (95% CI) sensitivity of PCT for the diagnosis of neonatal sepsis was 81% (74–87%), and the specificity was 79% (69–87%) (Fig. 3). The pooled (95% CI) diagnostic odds ratio was 16 (8–32), whereas the pooled (95% CI) positive and negative likelihood ratios were 3.9 (2.5–6.0) and 0.24 (0.17–0.34), respectively. The area under the HSROC curve (95% CI) for PCT was 0.87 (0.84–0.90) (Fig. 4). The I 2 index (95% CI) was 96% (92–99%). The effect of the diagnostic threshold (cutoff value) was not found to be important, since a weak negative correlation between the logits of sensitivity and specificity was observed (Spearman correlation coefficient = −0.08).

Forest plot of pooled sensitivity and specificity of BDG for the diagnosis of neonatal sepsis. The point estimates and the respective 95% confidence intervals for each one of the included studies are represented by the circles in the squares and the horizontal lines. The point estimate is represented by the dotted line, whereas the 95% CIs are represented by the diamond shape

Hierarchical summary receiver-operating characteristic curve of the sensitivity versus specificity of PCT for the diagnosis of neonatal sepsis. The curve is represented by the straight line; each of the analyzed studies is represented by a circle; the point estimate to which summary sensitivity and specificity correspond is represented by the diamond shape and the respective 95% confidence intervals by the dashed line, whereas the 95% confidence area in which a new study will be located is represented by the dotted line
Sub-analyses
Diagnostic accuracy of PCT for the diagnosis of EOS
Six studies, involving a total of 780 neonates, were included in the analysis regarding EOS [15, 27, 31, 40, 45, 47]. The pooled (95% CI) sensitivity of PCT for the diagnosis of EOS was 76% (68–82%), and the specificity was 76% (60–87%). The pooled (95% CI) diagnostic odds ratio was 10 (5–22), whereas the pooled (95% CI) positive and negative likelihood ratios were 3.2 (1.8–5.7) and 0.32 (0.23–0.43), respectively. The area under the HSROC curve (95% CI) for PCT was 0.78 (0.74–0.81) (Fig. 5). The I 2 index (95% CI) was 89% (77–100%).
Diagnostic accuracy of PCT for the diagnosis of LOS
Five studies, involving a total of 535 neonates, were included in the analysis regarding LOS [25, 26, 34, 35, 44]. The pooled (95% CI) sensitivity of PCT for the diagnosis of LOS was 90% (73–97%), and the specificity was 88% (72–96%). The pooled (95% CI) diagnostic odds ratio was 67 (23–200), whereas the pooled (95% CI) positive and negative likelihood ratios were 7.7 (3.1–18.9) and 0.11 (0.04–0.31), respectively. The area under the HSROC curve (95% CI) for PCT was 0.95 (0.93–0.97) (Fig. 6). The I 2 index (95% CI) was 93% (86–99%).

Hierarchical summary receiver-operating characteristic curve of the sensitivity versus specificity of PCT for the diagnosis of early onset neonatal sepsis. The curve is represented by the straight line; each of the analyzed studies is represented by a circle; the point estimate that summary sensitivity and specificity correspond to is represented by the diamond shape and the respective 95% confidence intervals by the dashed line, whereas the 95% confidence area in which a new study will be located is represented by the dotted line
Discussion
The main finding of our meta-analysis is that PCT has very good diagnostic accuracy for the diagnosis of neonatal sepsis. Specifically, in our primary analysis involving all studies evaluating PCT in neonates with and without sepsis, the area under the HSROC curve was 0.87, and the pooled sensitivity and specificity were 81 and 79%, respectively. Additionally, the area under the curve for the analyses regarding early-onset and late-onset sepsis was 0.78 and 0.95, respectively. However, marked statistical heterogeneity was present in all analyses, a fact that must not be overlooked in the interpretation of the above findings.

Hierarchical summary receiver-operating characteristic curve of the sensitivity versus specificity of PCT for the diagnosis of late-onset neonatal sepsis. The curve is represented by the straight line; each of the analyzed studies is represented by a circle; the point estimate to which summary sensitivity and specificity correspond is represented by the diamond shape and the respective 95% confidence intervals by the dashed line, whereas the 95% confidence area in which a new study will be located is represented by the dotted line
We should note that an important advantage of any biological marker used for neonates with suspected sepsis would be to correctly identify the septic episodes that are culture-negative and require antibiotic therapy. Ruling out sepsis is important, as if the number of neonates treated with antibiotics can be minimized, the length of hospitalization can be shortened; there may be less selection pressure for the emergence of resistant organisms, with medical and financial advantages that could offset the financial costs of measuring PCT [54]. Indeed, recent randomized controlled studies (RCTs) have suggested that PCT-guided algorithms are associated with a reduction in antibiotic exposure and antibiotic treatment duration [10, 55]. However, as observed with other diagnostic tests, including C-reactive protein (CRP) and total leukocyte count [56, 57], it cannot correctly identify 100% of the septic neonates by itself. Thus, relying on this biomarker has the risk of withholding antibiotic therapy in septic neonates that could otherwise benefit from such potentially life-saving therapy. The use of a lower cutoff value of serum PCT could theoretically increase the sensitivity and negative predictive value of this test for the diagnosis of neonatal sepsis [58].
The considerable heterogeneity regarding the definition of neonatal sepsis observed among the studies included in our review illustrates the lack of a universally acceptable definition of neonatal sepsis, particularly for the clinically septic but culture-negative newborns [9]. Although in neonatology the concept of clinical sepsis is widely used and considerable attempts have been made [24], a uniform definition for this common diagnosis is still lacking. This can be a cause of variability in the criteria for the definition of neonatal sepsis used in the studies that evaluate clinically diagnosed sepsis. Thus, in all likelihood, the spectrum of disorders and disease severity encompassed under the term neonatal sepsis differed among the various studies included in this review, a fact that may potentially account for the considerably high statistical heterogeneity observed in our analyses.
The different cutoff values of PCT incorporated in the analyzed studies were not found to account for a considerable proportion (threshold effect) of the observed statistical heterogeneity. Another potential source of heterogeneity may be the age of the involved pediatric patients. In order to address this issue, we excluded from our analysis the studies that involved a substantial proportion (>25%) of pediatric patients older than 28 days. Moreover, we excluded studies that involved healthy neonates as controls, as they cannot be regarded as representative of the population to whom PCT will be applied in routine clinical practice. The inclusion of premature neonates in the evaluated studies may also be another source of heterogeneity. However, since data regarding the percentage of preterm neonates among the involved patients were scarcely reported in the included studies, we could not assess the effect of this specific factor on the performance of PCT regarding the diagnosis of neonatal sepsis.
Taking into consideration the physiological postnatal increase of serum PCT concentration that is observed in healthy preterm neonates [17], as well as in healthy term neonates [15], with peak values at 24 h of age [16], we performed two sub-analyses limited to studies evaluating the performance of PCT for the diagnosis of early (<72 h) and late-onset (>72 h) neonatal sepsis, respectively. Although our findings suggest that PCT has better diagnostic accuracy for late-onset compared with early onset neonatal sepsis, the available data for late-onset sepsis were not sufficient to allow any firm conclusions.
Several limitations should be taken into consideration in the interpretation of the findings of this meta-analysis, particularly the heterogeneity between the included studies regarding the characteristics of the enrolled neonates (particularly the postnatal age), as well as the broad definition criteria of neonatal sepsis. Until a uniform definition of neonatal sepsis is available, this important limitation will continue to be inherent in the research in this field. Moreover, a considerable proportion of neonates included in the septic group had possible (not microbiologically documented) sepsis. Indeed, possible neonatal sepsis is a diagnosis frequently encountered in routine clinical practice. PCT may aid in the classification of these patients as septic or non-septic. However, since specific data regarding the diagnostic performance of PCT for this sub-group of patients were scarcely reported from the included studies, we did not assess the potential influence of this factor on our study findings. Finally, it is possible that PCT may perform differently in neonatal sepsis because of gram-positive, gram-negative, or fungal pathogens [59]. Hence, not only the clinical characteristics of the enrolled neonates, but also the local microbiological profile in a given ICU are likely to affect the value of PCT in predicting neonatal sepsis. However, we were unable to explore this further because the necessary information was usually unavailable in the studies included in this review.
Conclusion
In conclusion, our findings suggest that serum PCT, measured at the time of clinical presentation, seems to have very good diagnostic accuracy for the discrimination between ill neonates with sepsis and those with other conditions. However, the considerable differences between the analyzed studies, as well as the lack of a uniform definition of neonatal sepsis that can be used as a reference diagnostic standard, cannot allow the establishment of any firm conclusions. Larger studies using appropriate methodology are required to validate the routine use of PCT as a diagnostic marker of neonatal sepsis.
References
Bizzarro MJ, Raskind C, Baltimore RS, Gallagher PG (2005) Seventy-five years of neonatal sepsis at Yale: 1928–2003. Pediatrics 116:595–602
Stoll BJ, Hansen NI, Adams-Chapman I, Fanaroff AA, Hintz SR, Vohr B, Higgins RD (2004) Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. JAMA 292:2357–2365
Osrin D, Vergnano S, Costello A (2004) Serious bacterial infections in newborn infants in developing countries. Curr Opin Infect Dis 17:217–224
Chiesa C, Panero A, Osborn JF, Simonetti AF, Pacifico L (2004) Diagnosis of neonatal sepsis: a clinical and laboratory challenge. Clin Chem 50:279–287
Schelonka RL, Chai MK, Yoder BA, Hensley D, Brockett RM, Ascher DP (1996) Volume of blood required to detect common neonatal pathogens. J Pediatr 129:275–278
Lam HS, Ng PC (2008) Biochemical markers of neonatal sepsis. Pathology 40:141–148
Malik A, Hui CP, Pennie RA, Kirpalani H (2003) Beyond the complete blood cell count and C-reactive protein: a systematic review of modern diagnostic tests for neonatal sepsis. Arch Pediatr Adolesc Med 157:511–516
Mehr S, Doyle LW (2000) Cytokines as markers of bacterial sepsis in newborn infants: a review. Pediatr Infect Dis J 19:879–887
(2003) Clinical policy for children younger than three years presenting to the emergency department with fever. Ann Emerg Med 42:530–545
Bouadma L, Luyt CE, Tubach F, Cracco C, Alvarez A, Schwebel C, Schortgen F, Lasocki S, Veber B, Dehoux M, Bernard M, Pasquet B, Regnier B, Brun-Buisson C, Chastre J, Wolff M (2010) Use of procalcitonin to reduce patients’ exposure to antibiotics in intensive care units (PRORATA trial): a multicentre randomised controlled trial. Lancet 375: 463–474
Simon L, Gauvin F, Amre DK, Saint-Louis P, Lacroix J (2004) Serum procalcitonin and C-reactive protein levels as markers of bacterial infection: a systematic review and meta-analysis. Clin Infect Dis 39:206–217
Tang BM, Eslick GD, Craig JC, McLean AS (2007) Accuracy of procalcitonin for sepsis diagnosis in critically ill patients: systematic review and meta-analysis. Lancet Infect Dis 7:210–217
Gendrel D, Bohuon C (2000) Procalcitonin as a marker of bacterial infection. Pediatr Infect Dis J 19:679–687 (quiz 688)
van Rossum AM, Wulkan RW, Oudesluys-Murphy AM (2004) Procalcitonin as an early marker of infection in neonates and children. Lancet Infect Dis 4:620–630
Chiesa C, Panero A, Rossi N, Stegagno M, De Giusti M, Osborn JF, Pacifico L (1998) Reliability of procalcitonin concentrations for the diagnosis of sepsis in critically ill neonates. Clin Infect Dis 26:664–672
Assumma M, Signore F, Pacifico L, Rossi N, Osborn JF, Chiesa C (2000) Serum procalcitonin concentrations in term delivering mothers and their healthy offspring: a longitudinal study. Clin Chem 46:1583–1587
Turner D, Hammerman C, Rudensky B, Schlesinger Y, Goia C, Schimmel MS (2006) Procalcitonin in preterm infants during the first few days of life: introducing an age related nomogram. Arch Dis Child Fetal Neonatal Ed 91:F283–F286
Arends LR, Hamza TH, van Houwelingen JC, Heijenbrok-Kal MH, Hunink MG, Stijnen T (2008) Bivariate random effects meta-analysis of ROC curves. Med Decis Making 28:621–638
Chappell FM, Raab GM, Wardlaw JM (2009) When are summary ROC curves appropriate for diagnostic meta-analyses? Stat Med 28:2653–2668
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
StataCorp. 2007. Stata Statistical Software: Release 10. College Station, TX: StataCorp LP
Dwamena B. MIDAS: Stata module for meta-analytical integration of diagnostic test accuracy studies. Statistical Software Components 2007
Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J (2003) The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol 3:25
Goldstein B, Giroir B, Randolph A (2005) International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med 6:2–8
Cetinkaya M, Ozkan H, Koksal N, Celebi S, Hacimustafaoglu M (2009) Comparison of serum amyloid A concentrations with those of C-reactive protein and procalcitonin in diagnosis and follow-up of neonatal sepsis in premature infants. J Perinatol 29:225–231
Jacquot A, Labaune JM, Baum TP, Putet G, Picaud JC (2009) Rapid quantitative procalcitonin measurement to diagnose nosocomial infections in newborns. Arch Dis Child Fetal Neonatal Ed
Bender L, Thaarup J, Varming K, Krarup H, Ellermann-Eriksen S, Ebbesen F (2008) Early and late markers for the detection of early-onset neonatal sepsis. Dan Med Bull 55:219–223
Boo NY, Nor Azlina AA, Rohana J (2008) Usefulness of a semi-quantitative procalcitonin test kit for early diagnosis of neonatal sepsis. Singap Med J 49:204–208
Ramirez-Valdivia JM, Perez-Molina JJ, Locheo-Gonzalez M, Troyo-Sanroman R, Perez-Cortez G (2008) Procalcitonin a marker in the diagnostic of the newborn with systemic infection. Rev Med Inst Mex Seguro Soc 46:597–602
Sakha K, Husseini MB, Seyyedsadri N (2008) The role of the procalcitonin in diagnosis of neonatal sepsis and correlation between procalcitonin and C-reactive protein in these patients. Pak J Biol Sci 11:1785–1790
Santuz P, Soffiati M, Dorizzi RM, Benedetti M, Zaglia F, Biban P (2008) Procalcitonin for the diagnosis of early-onset neonatal sepsis: a multilevel probabilistic approach. Clin Biochem 41:1150–1155
Savagner C, Hoppe A, Montcho Y, Leboucher B, Le Bouedec S, Lemarie C, de Boux Casson F, Bouderlique C (2008) Interest of Procalcitonin in neonatal intensive care unit for patients suspected of nosocomial sepsis: retrospective study on 40 children. Journal de pediatrie et de puericulture 21:292–298
Ucar B, Yildiz B, Aksit MA, Yarar C, Colak O, Akbay Y, Colak E (2008) Serum amyloid A, procalcitonin, tumor necrosis factor-alpha, and interleukin-1beta levels in neonatal late-onset sepsis. Mediators Inflamm 2008:737141
Bustos Betanzo RO (2007) Procalcitonin, C-reactive protein and leukocyte count in very-low birth weight infants with late neonatal sepsis. An Pediatr (Barc) 66:541–542
Isidor B, Caillaux G, Gilquin V, Loubersac V, Caillon J, Roze JC, Gras-le Guen C (2007) The use of procalcitonin in the diagnosis of late-onset infection in neonatal intensive care unit patients. Scand J Infect Dis 39:1063–1066
Kocabas E, Sarikcioglu A, Aksaray N, Seydaoglu G, Seyhun Y, Yaman A (2007) Role of procalcitonin, C-reactive protein, interleukin-6, interleukin-8 and tumor necrosis factor-alpha in the diagnosis of neonatal sepsis. Turk J Pediatr 49:7–20
Koksal N, Harmanci R, Cetinkaya M, Hacimustafaoglu M (2007) Role of procalcitonin and CRP in diagnosis and follow-up of neonatal sepsis. Turk J Pediatr 49:21–29
Lopez Sastre JB, Solis DP, Serradilla VR, Colomer BF, Cotallo GD (2007) Evaluation of procalcitonin for diagnosis of neonatal sepsis of vertical transmission. BMC Pediatr 7:9
Pavcnik-Arnol M, Hojker S, Derganc M (2007) Lipopolysaccharide-binding protein, lipopolysaccharide, and soluble CD14 in sepsis of critically ill neonates and children. Intensive Care Med 33:1025–1032
Pastor Peidro JA, de Gonzalez Dios J, Uran Moreno MM, Garcia Aviles B, De la Campillo A, Moya Benavent M (2007) Usefulness of procalcitonin as an early diagnostic test of neonatal sepsis in newborns with risk factors for infection. An Pediatr (Barc) 67:530–535
Lopez Sastre JB, Perez Solis D, Roques Serradilla V, Fernandez Colomer B, Coto Cotallo GD, Krauel Vidal X, Narbona Lopez E, del Garcia Rio M, Sanchez Luna M, Belaustegui Cueto A, Moro Serrano M, Urbon Artero A, Alvaro Iglesias E, Cotero Lavin A, Martinez Vilalta E, Jimenez Cobos B (2006) Procalcitonin is not sufficiently reliable to be the sole marker of neonatal sepsis of nosocomial origin. BMC Pediatr 6:16
Perez Solis D, Lopez Sastre JB, Coto Cotallo GD, Dieguez Junquera MA, Deschamps Mosquera EM, Crespo Hernandez M (2006) Procalcitonin for the diagnosis of nosocomial neonatal sepsis. An Pediatr (Barc) 64:349–353
Verboon-Maciolek MA, Thijsen SF, Hemels MA, Menses M, van Loon AM, Krediet TG, Gerards LJ, Fleer A, Voorbij HA, Rijkers GT (2006) Inflammatory mediators for the diagnosis and treatment of sepsis in early infancy. Pediatr Res 59:457–461
Vazzalwar R, Pina-Rodrigues E, Puppala BL, Angst DB, Schweig L (2005) Procalcitonin as a screening test for late-onset sepsis in preterm very low birth weight infants. J Perinatol 25:397–402
Ballot DE, Perovic O, Galpin J, Cooper PA (2004) Serum procalcitonin as an early marker of neonatal sepsis. S Afr Med J 94:851–854
Chiesa C, Pellegrini G, Panero A, Osborn JF, Signore F, Assumma M, Pacifico L (2003) C-reactive protein, interleukin-6, and procalcitonin in the immediate postnatal period: influence of illness severity, risk status, antenatal and perinatal complications, and infection. Clin Chem 49:60–68
Resch B, Gusenleitner W, Muller WD (2003) Procalcitonin and interleukin-6 in the diagnosis of early-onset sepsis of the neonate. Acta Paediatr 92:243–245
Blommendahl J, Janas M, Laine S, Miettinen A, Ashorn P (2002) Comparison of procalcitonin with CRP and differential white blood cell count for diagnosis of culture-proven neonatal sepsis. Scand J Infect Dis 34:620–622
Guibourdenche J, Bedu A, Petzold L, Marchand M, Mariani-Kurdjian P, Hurtaud-Roux MF, Aujard Y, Porquet D (2002) Biochemical markers of neonatal sepsis: value of procalcitonin in the emergency setting. Ann Clin Biochem 39:130–135
Enguix A, Rey C, Concha A, Medina A, Coto D, Dieguez MA (2001) Comparison of procalcitonin with C-reactive protein and serum amyloid for the early diagnosis of bacterial sepsis in critically ill neonates and children. Intensive Care Med 27:211–215
Franz AR, Kron M, Pohlandt F, Steinbach G (1999) Comparison of procalcitonin with interleukin 8, C-reactive protein and differential white blood cell count for the early diagnosis of bacterial infections in newborn infants. Pediatr Infect Dis J 18:666–671
Maire F, Heraud MC, Loriette Y, Normand B, Begue RJ, Labbe A (1999) The value of procalcitonin in neonatal infections. Arch Pediatr 6:503–509
Lapillonne A, Basson E, Monneret G, Bienvenu J, Salle BL (1998) Lack of specificity of procalcitonin for sepsis diagnosis in premature infants. Lancet 351:1211–1212
Schuetz P, Christ-Crain M, Muller B (2009) Procalcitonin and other biomarkers to improve assessment and antibiotic stewardship in infections–hope for hype? Swiss Med Wkly 139:318–326
Nobre V, Harbarth S, Graf JD, Rohner P, Pugin J (2008) Use of procalcitonin to shorten antibiotic treatment duration in septic patients: a randomized trial. Am J Respir Crit Care Med 177:498–505
Mannan MA, Shahidullah M, Noor MK, Islam F, Alo D, Begum NA (2010) Utility of C-reactive protein and hematological parameters in the detection of neonatal sepsis. Mymensingh Med J 19:259–263
Shaoul R, Lahad A, Tamir A, Lanir A, Srugo I (2008) C reactive protein (CRP) as a predictor for true bacteremia in children. Med Sci Monit 14:CR255–CR261
Maniaci V, Dauber A, Weiss S, Nylen E, Becker KL, Bachur R (2008) Procalcitonin in young febrile infants for the detection of serious bacterial infections. Pediatrics 122:701–710
Charles PE, Ladoire S, Aho S, Quenot JP, Doise JM, Prin S, Olsson NO, Blettery B (2008) Serum procalcitonin elevation in critically ill patients at the onset of bacteremia caused by either Gram negative or Gram positive bacteria. BMC Infect Dis 8:38
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vouloumanou, E.K., Plessa, E., Karageorgopoulos, D.E. et al. Serum procalcitonin as a diagnostic marker for neonatal sepsis: a systematic review and meta-analysis. Intensive Care Med 37, 747–762 (2011). https://doi.org/10.1007/s00134-011-2174-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-011-2174-8