
Abstract
Background
The ideal time for distinguishing a renal scar from acute inflammatory lesions by renal DMSA scintigraphy remains controversial.
Objective
To determine the time needed for resolution of lesions after acute pyelonephritis.
Materials and methods
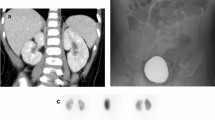
A total of 105 children with acute pyelonephritis underwent renal sonography, voiding cystourethrography and baseline DMSA scintigraphy. Two subsequent scans were performed during the 6th and 12th months in patients with abnormal findings on the previous scan.
Results
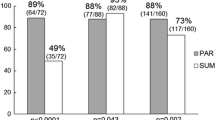
The baseline DMSA scintigraphy revealed cortical lesions in 37 patients. At 6 months, 13 patients (38.2%) were found to have cortical lesions. At 12 months, 6 patients (17.6%) were found to have persistent renal cortical lesions. The resolution rates for lesions detected on the first scan were 61.8% and 82.4% on the 6- and 12-month scans, respectively. Vesicoureteric reflux, and bilaterality or multifocality were not relevant for resolution of lesions. Female gender seemed to be associated with a higher persistence rate.
Conclusions
The renal cortical defects present at 6 months have a high rate of resolution later during follow-up. DMSA scintigraphy performed 12 months after the infection provides more reliable data regarding persistence of renal cortical lesions.

Similar content being viewed by others

References
Barry BP, Hall N, Cornford E et al (1998) Improved ultrasound detection of renal scarring in children following urinary tract infection. Clin Radiol 53:747–751
Hoberman A, Wald ER, Hickey RW et al (1999) Oral versus initial intravenous therapy for urinary tract infections in young febrile children. Pediatrics 104:79–86
Jakobsson B, Berg U, Svensson L et al (1994) Renal scarring after acute pyelonephritis. Arch Dis Child 70:111–115
Majd M, Rushtoh HG (1992) Renal cortical scintigraphy in the diagnosis of acute pyelonephritis. Semin Nucl Med 22:98–111
Patel K, Charron M, Hoberman A et al (1993) Intra- and interobserver variability in interpretation of DMSA scans using a set of standardized criteria. Pediatr Radiol 23:506–509
Ditchfield MR, Summerville D, Grimwood K et al (2002) Time course of transient cortical scintigraphic defects associated with acute pyelonephritis. Pediatr Radiol 32:849–852
Benador D, Benador N, Slosman DO et al (1994) Cortical scintigraphy in the evaluation of renal parenchymal changes in children with pyelonephritis. J Pediatr 124:17–20
Rushton HG, Majd M, Jantausch B et al (1992) Renal scarring following reflux and nonreflux pyelonephritis in children: evaluation with 99mtechnetium-dimercaptosuccinic acid scintigraphy. J Urol 147:1327–1332
International Reflux Study Committee (1981) Medical versus surgical treatment of primary vesicoureteral reflux: a prospective international reflux study in children. J Urol 125:277–283
Paterson A (2004) Urinary tract infection: an update on imaging strategies. Eur Radiol 14 [Suppl 4]:L89–L100
Winberg J, Andersen HJ, Bergstrom T et al (1974) Epidemiology of symptomatic urinary tract infection in childhood. Acta Paediatr Scand Suppl 252:1–20
Mannhardt W, Schofer O, Schulte-Wissermann H et al (1986) Pathogenic factors in recurrent urinary tract infections and renal scar formation in children. Eur J Pediatr 14:330–336
Verber IG, Meller ST (1989) Serial 99mTc dimercaptosuccinic acid (DMSA) scans after urinary infections presenting before the age of 5 years. Arch Dis Child 64:1533–1537
Farnsworth RH, Rossleigh MA, Leighton DM et al (1991) The detection of reflux nephropathy in infants by 99mtechnetium dimercaptosuccinic acid studies. J Urol 145:542–546
Jakobsson B, Svensson L (1997) Transient pyelonephritic changes on 99mTechnetium-dimercaptosuccinic acid scan for at least five months after infection. Acta Paediatr 86:803–807
Jakobsson B, Nolstedt L, Svensson L et al (1992) 99mTechnetium-dimercaptosuccinic acid scan in the diagnosis of acute pyelonephritis in children: relation to clinical and radiological findings. Pediatr Nephrol 6:328–334
Lavocat MP, Granjon D, Guimpied Y et al (1998) The importance of 99Tcm-DMSA renal scintigraphy in the follow-up of acute pyelonephritis in children: comparison with urographic data. Nucl Med Commun 19:703–710
Ditchfield MR, Grimwood K, Cook DJ et al (2004) Persistent renal cortical scintigram defects in children 2 years after urinary tract infection. Pediatr Radiol 34:465–471
Lin KY, Chiu NT, Chen MJ et al (2003) Acute pyelonephritis and sequelae of renal scar in pediatric first febrile urinary tract infection. Pediatr Nephrol 18:362–365
Martinell J, Claesson I, Lidin-Janson G et al (1995) Urinary infection, reflux and renal scarring in females continuously followed for 13–38 years. Pediatr Nephrol 9:131–136
Gleeson FV, Gordon I (1991) Imaging in urinary tract infection. Arch Dis Child 66:1282–1283
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Agras, K., Ortapamuk, H., Naldöken, S. et al. Resolution of cortical lesions on serial renal scans in children with acute pyelonephritis. Pediatr Radiol 37, 153–158 (2007). https://doi.org/10.1007/s00247-006-0362-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-006-0362-4