
Abstract
Initial case series of small number of patients at the beginning of the pandemic reported a rather guarded prognosis for Behçet’s syndrome (BS) patients infected with SARS-CoV-2. In this prospective study, we describe the incidence, clinical characteristics, disease course, management, and outcome in a large cohort of BS patients with laboratory-confirmed infection of SARS-CoV-2. We defined a cohort of 1047 registered BS patients who were aged between 16 and 60 years and seen routinely before the pandemic at the multidisciplinary outpatient clinic. We followed prospectively this cohort from beginning of April 2020 until the end of April 2021. During 13 months of follow-up, of the 1047 (599 M/448 F) patients, 592 (56.5%) were tested for SARS-CoV-2 PCR at least once and 215 (20.5%; 95% CI 0.18–0.23) were tested positive. We observed 2 peaks which took place in December 2020 and April 2021. Of the 215 PCR positive patients, complete information was available in 214. Of these 214, 14 (6.5%) were asymptomatic for COVID-19. In the remaining, the most common symptoms were anosmia, fatigue, fever, arthralgia, and headache. A total of 40 (18.7%) had lung involvement, 25 (11.7%) were hospitalized, 1 was admitted to the intensive care unit while none died. Favipiravir was the most prescribed drug (74.3%), followed by colchicine (40.2%), and hydroxychloroquine (20.1%) in the treatment of COVID-19. After COVID-19, 5 patients (2.3%) were given supplemental O2 and 31 (14.5%) antiaggregant or anticoagulants. During COVID-19, of the 214 PCR positive patients, 116 (54.2%) decreased the dose of their immunosuppressives or stopped taking completely; 36 (16.8%) experienced a BS flare which was mostly oral ulcers (10.3%). None of the patients reported a thrombotic event. A total of 93 (43.5%) patients reported BS flares after a median 45 days of COVID-19 infection and this was found to be significantly associated with immunosuppressive drug discontinuation. Multiple regression analysis adjusted for age and gender indicated that smoking and using interferon-alpha decreased the likelihood of getting COVID-19. The incidence and severity of COVID-19 did not differ between those who were using colchicine or not. The cumulative incidence of COVID-19 in this prospectively followed cohort of BS patients was almost two folds of that estimated for the general population living in Istanbul, Turkey, however, the clinical outcome of COVID-19 was not severe and there was no mortality. The protective effect of smoking and interferon deserves further investigation. On the other hand, colchicine did not have any positive or negative effect against COVID-19. Significant number of patients flared after COVID-19, however, this was significantly associated with immunosuppressive discontinuation during the infection. Contrary to our previous observations, COVID-19 did not seem to exacerbate thrombotic events during or after the infection.
Similar content being viewed by others


Introduction
Since it emerged in December 2019, the Coronavirus disease-2019 (COVID-19) pandemic has affected at least 223 million people and caused more than 4.6 million deaths worldwide [1]. The first case in Turkey was recorded on 11 March 2020 [2], and as of 8 November 2021, there have been 8,231,679 confirmed cases and 72,127 deaths registered due to COVID-19 [1].
Patients with rheumatic diseases (RD) particularly those with autoimmune diseases (AD) have been reported to have a higher infection rate and a worse outcome for COVID-19 [3, 4]. Behçet’s syndrome (BS), a complex inflammatory disorder of unknown etiology, is one of the most prevalent RD in Turkey, with a prevalence rate of 0.4% [5]. It is characterized by recurrent skin mucosa lesions and uveitis, but may also involve joints, vascular, gastrointestinal, and central nervous systems. Although BS cannot be classified as a typical AD [6], immunosuppressive agents including glucocorticoids (GC), TNF inhibitors, and conventional disease-modifying anti-rheumatic drugs (DMARDs) are the mainstay of treatment [6,7,8,9,10,11]. Colchicine, a much-debated promising drug for COVID-19, is also used frequently in BS, especially to treat skin-mucosa lesions [12, 13]. There have been conflicting reports about the outcome of BS patients who were diagnosed with COVID-19 at the beginning of the pandemic [14,15,16,17]. We have previously reported ten patients with severe outcome [14]. Of the ten patients, eight were hospitalized of whom two had to be taken care of in the ICU. Ultimately, one died due to pneumonia and one developed de-novo deep vein thrombosis [14]. On the other hand, two small case series one from Italy and another from Spain reported a mild outcome [16, 17]. Moreover, a consensus based on multinational experts’ opinion suggested that the prevalence of COVID-19 in BS is apparently lower than that in the general population, and that BS appears not to be associated with a more severe COVID-19 course [18].
In this prospective study, we describe the incidence rate, clinical characteristics, disease course, management, and outcomes in a large cohort of patients with BS with laboratory-confirmed infection of SARS-CoV-2.
Patients and methods
Our prospective cohort study was done during the first 13 months of the pandemic at Behçet Disease Research Center in Cerrahpasa Medical Faculty of Istanbul University-Cerrahpasa, Turkey. At the onset of the pandemic, we defined a cohort of 1047 registered BS patients who were aged between 16 and 60 years and seen between the beginning of August 2019 and the end of December 2019 at our multidisciplinary outpatient clinic. We followed prospectively this cohort from the beginning of April 2020 until the end of April 2021. The follow-up was terminated when the vaccination program for immune-compromised individuals started in Turkey [19]. We basically conducted a telephone survey using a standardized questionnaire which was composed of 3 parts. The first part included questions regarding socio-demographic variables such as age, gender, occupation, marital status, educational status, and household size. In the second part, the participants were asked whether they were smokers and have been previously diagnosed with a comorbid disease (such as cardiovascular disease, chronic lung disease, hypertension, diabetes mellitus, or else). The third part included questions regarding COVID-19. Further information on clinical characteristics, disease duration, and prescribed medications were collected from patients’ charts. We first tested the questionnaire on 26 patients to check its usability and to see whether there are unclear, unwelcome or unnecessary questions. After these pre-test evaluations, we were able to refine the survey.
The “Ministry of Health Public Health Data Management System” database has been established at the beginning of the SARS-CoV-2 pandemic in Turkey, on March 2020 to store COVID-19 related hospital records, PCR and other laboratory test results as well as radiological imaging of Turkish citizens. The database was accessed freely only by specialists of clinical infectious diseases (I.I.B. and F.T.). National identity and phone numbers of all study individuals had been stored in our hospital record system. After obtaining patients’ consent, we used the database to screen all the study participants to see which ones were tested for PCR or reported as COVID-19 cases. We recorded how many PCR tests were done and when these tests were performed. We also examined the electronic notes of the family physicians who were responsible for the follow-up of patients if they were diagnosed or suspected with COVID-19 infection. For those who were living outside of Istanbul, we collected all these information through telephone interviews. We screened all patients periodically until the end of April 2021. All patients were called for the third part of the questionnaire between August–September 2020, December 2020-January 2021, and March–April 2021.
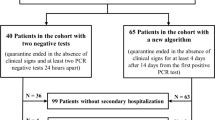
After we defined the subgroup of patients with positive PCR tests for COVID-19, we created a second questionnaire for the investigation of the following factors: current use/discontinuation or dose reduction of BS drugs during the pandemic and during the COVID-19 infection; medical treatment for COVID-19; COVID-19 related symptoms and findings; hospitalization, admission to the intensive care unit, BS exacerbation during or after the COVID-19 infection and any other complaints/symptoms developed after the infection. All these information was obtained from the Ministry of Health Public Health Data Management System database and through telephone interviews. For the hospitalized patients, we requested hospital files/records from the hospital staff or patients themselves. We had complete information in all patients with positive PCR test except one who refused to talk (Fig. 1). This part of the study was terminated by the end of June 2021, however, we continued to check those patients who had pneumonia and those who reported post-COVID symptoms with frequent telephone calls until the manuscript was prepared for submission.

Flow chart of the study population selection according to the PCR test for COVID-19 (the chart breaks down initially into PCR tested vs non-tested then into PCR positive vs PCR negative)
As shown in the flow chart (Fig. 1), we only evaluated those who had positive PCR test. The 10 patients whom we have previously reported at the beginning of the pandemic were not included either [14]. Those who had tested negative but had typical lesions on the thorax CT or who were ascribed as COVID-19 and medically treated as COVID-19 due to similarity of the symptoms were excluded from the study (Fig. 1).
The management of patients with COVID-19 diagnosis was done according to the Ministry of Health guidelines [20] and described in detail in the Supplement.
Ethical statement
This study was approved by the Ethics Committee of Istanbul University-Cerrahpasa, Cerrahpaşa Medical Faculty (12/10/2020–134022) and by the Ministry of Health (2020-08-18T15_54_13). During all the steps of the study, we obtained patients’ consent and followed the ethical principles of the Helsinki declaration.
Statistical analysis
Descriptive data were presented as median and range for the continuous variables and frequency and percentages (%) for the categorical variables. Continuous variables were evaluated for normality distribution using Shapiro–Wilk test. PCR (+) and PCR (−) group were compared with Mann–Whitney U test for non-normally distributed variables. Categorical variables were compared by using Chi-Square or Fisher’s exact test for proportion. Survival analysis to express time to be PCR positive for COVID-19 was shown with Kaplan–Meier plots. Patients whose PCR test were not positive during the follow-up (0–13 months) were censored. Survival curves were compared with Log-Rank test with two-sided significance level of 0.05 for each group. We applied Univariate Logistic Regression Analysis to assess the association between independent factors and risk of COVID-19 and statistically significant independent factors were included Multivariate Logistic Regression model. Similar analyses were done to investigate variables associated with pneumonia due to COVID-19 as well hospitalization. All significance tests were 2-tailed, and values of p < 0.05 were considered statistically significant. Statistical analyses were performed using the RStudio version 4.0.2 software and IBM SPSS Statistics version 21.0.
Sample size calculation
The incidence of COVID-19 in the general population was reported as 0.2% at the beginning of the pandemic [21]. A sample size was calculated assuming the incidence of COVID-19 would be three times higher than that observed in the general population. We utilized simple sample size formula [22]. Minimum sample size was estimated as 916 patients with an absolute precision of 0.5% and 5% level of significance.
Results
Of the 1047 (599 M/448 F) patients, 592 (344 M/248 F) (56.5%) were tested for COVID-19 PCR at least once (median: 2, IQR: 1–5). Of these 592, 215 (127 M/88 F) were tested positive. The median number of PCR tests was significantly higher among those who were tested positive (median: 2, IQR: 1–3) compared to those who were tested negative (median: 1, IQR: 1–2), p < 0.001). Of the 377 (218 M/159 F) patients who were tested negative, 10 had pneumonia specific for COVID-19 and 5 were hospitalized. For the study purposes, we only considered those 215 (127 M/88 F) PCR positive patients as diagnosed with COVID-19 (Fig. 1). There were 92 patients (8.8%) who were living outside of Istanbul in the cohort and of these, 35 (38.0%) were tested positive.
Incidence of COVID-19 in the BS cohort
As shown in the Kaplan Meier plot (Fig. 2), the cumulative incidence of COVID-19 in the cohort rose from 0 to 20.5% (95% CI 18–23%) from April 1, 2020 to April 30, 2021. During 13 months of follow-up, there were two peaks. The first peak occurred in December 2020 in which 51 cases were recorded in a single month. The cumulative incidence surged from 9% (95% CI 10–12%) to 14% (95% CI 12–16%). The second peak occurred in April 2021 in which we observed 41 cases with COVID- 19 in a single month. Hence, the cumulative incidence increased from 16% (95% CI 14–19%) to 20.5% (95% CI 18–23%). These two peaks coincided well with the peaks observed in the general population in Turkey [1]. Additional Kaplan–Meier plots stratified for age (16–40 years vs 41–60 years), gender and presence of comorbid disease did not show any significance, however, those who smoke were shown to have a lower probability for contracting COVID-19 as compared with those who do not smoke (Fig. 3, 4, 5 and 6 in the Supplement).

Cumulative incidence plot indicating patients who developed positive PCR test for COVID-19 during the first 13 months of the pandemic in the whole cohort including 1047 patients with Behçet’s syndrome
Socio-demographic and clinical characteristics of the patients with BS who tested positive for COVID-19
As shown in Table 1, those who were diagnosed as COVID-19 were significantly less likely to smoke and significantly less likely to use interferon-alpha compared to those who were not. Besides these parameters, there were no socio-demographic or clinical characteristics that were significantly different between the two groups. These were also confirmed in the univariate logistic regression analysis (Table 1).
As shown in Table 2, multiple regression analysis adjusted for age and gender indicated that smoking (OR 0.65; 95% CI 0.46–0.92, p = 0.014) and using interferon-alpha (OR 0.13; 95% CI 0.02–1.00) decreased the risk of getting COVID-19.
Presenting symptoms, treatment, and outcome associated with COVID-19 among PCR positive BS patients (Table 3)
There were 215 patients who were tested positive of whom complete information was available in all except one. Of these 214 patients, 14 (6.5%) were asymptomatic and were tested because of the history of COVID-19 in a close contact (Table 3). The remaining 200 patients had one or more symptoms as shown in Table 3. The most common symptoms were anosmia (54.7%), fatigue (53.3%), fever (52.3%), arthralgia (52.3%), and headache (48.1%). A total of 40 (18.7%) had pneumonia, 25 (11.7%) were hospitalized, 1 was admitted to the intensive care unit while none died. Univariate analysis found that smoking and having a comorbid disease were associated with COVID-19 pneumonia (data not shown). Variables associated with hospitalization were smoking, having a comorbid disease, and using GC (data not shown). Age and gender-adjusted multivariate regression analysis revealed that smoking decreased the risk of getting COVID-19 pneumonia (OR 0.25, 95% CI 10–66%; p = 0.005) and hospitalization (OR 0.32, 95% CI 0.11–0.95; p = 0.040). On the other hand, having a comorbid disease was associated with increased risk for both COVID-19 pneumonia (OR 2.78, 95% CI 1.36–5.67; p = 0.005) and hospitalization (OR 2.70, 95% CI 1.13–6.43; p = 0.011). Similarly using prednisolone was found to be associated with increased risk of hospitalization (OR 3.44, 95% CI 1.40–8.47; p = 0.007) (Table 2).
While 23 (10.7) did not receive any COVID-19 related treatment, the remaining received one or more drugs. Favipiravir (74.3%, 159/214) was the most prescribed drug, followed by colchicine (40.2%, 86/214), and hydroxychloroquine (20.1%, 43/214). None of the patients used remdesivir. Oseltamivir and azithromycin were given to a few patients at the beginning of the pandemic. Tocilizumab and dexamethasone were given to 2 and 9 patients, respectively. A total of 27 (12.6%) patients used low-molecular-weight heparin and 42 (19.6%) aspirin. Supplemental O2 was given to 14 (6.5%) patients. After COVID-19 infection, 5 (2.3%) patients were given supplemental O2 and 31 (14.5%) anti-aggregants or anti-coagulants.
BS flare during and after COVID-19 (Table 4)
During the pandemic, a total of 39 (18.2%) patients of 214 PCR positive BS patients decreased (n = 18) or stopped (n = 21) the dose of their medications associated with BS. After having being diagnosed with COVID-19 infection, a total of 116 (54.2%) either discontinued (n = 106) or decreased the dose of their medications (n = 10). During COVID-19 infection, 36 (16.8%) experienced a BS flare which was mostly oral ulcers (10.3%), genital ulcers (3.3%), skin lesions (6.5%), and uveitis (4.7%). None of the patients reported a thrombotic event. BS flares during COVID-19 infection were significantly more likely to be frequent among those who discontinued or decreased the dose of their immunosuppressives (Table 4).
A total of 93 (43.5%) patients reported having an exacerbation associated with BS after a median 45 days [IQR: 21–90] of COVID-19 infection. These were oral ulcers (26.2%), uveitis (13.6%) and skin lesions (11.2%). Genital ulcers (4.2%) and lower extremity vein thrombosis (3.7%) were observed rarely. BS flares that occurred after COVID-19 infection were significantly more common among those who reduced the dose of their medications or stopped taking them (52.6%) compared to those who continued to take their drugs regularly (32.7%), (p = 0.003) (Table 4).
Post-COVID-19 symptoms
A total of 80 (37.4%) patients out of 214, developed at least one miscellaneous symptom after COVID-19. These were mostly dyspnea/chest pain (n = 26), neuropsychiatric complaints (n = 22), and cardio-pulmonary problems such as blood pressure dysregulations, arrhythmia, and cough (n = 16). Further follow-up of these patients revealed that none of the patients has been diagnosed with myocardial infarction, stroke or cerebrovascular event.
Discussion
In this prospective large cohort study, the cumulative incidence of COVID-19 among BS patients was found to be 20.5% by the end of 13 months of the pandemic in Turkey. The clinical outcome seemed not to be severe, with no mortality or thrombotic events associated with COVID-19. Smoking and using interferon seemed to exert protective effects against COVID-19. On the other hand, colchicine was not found to have any protective or worsening effect against COVID-19. BS flares during or after COVID-19 infection were not infrequent but seemed to be associated with discontinuation or dose reduction of the immunosuppressive drugs.
As reported by the Turkish Ministry of Health, there have been overall 47,261,999 (56.2%) who were tested, 4,820,591 confirmed cases (5.77%; 95% CI 4.3–7.2%) and 40,131 (0.83%; 95% CI 0.67-0.99%) deaths registered due to COVID-19 in Turkey (population: 83,614,362) by the end of April 2021 [23]. When only those who were living in Istanbul (the largest city with a population [24] of 15,462,452) are considered, the cumulative incidence of PCR confirmed cases was estimated as 11.27% (95% CI 1.9–13.2%). It has to be noted that the great majority (91.2%) of the BS cohort in our study was residing in Istanbul. The fact that the statistics provided by the government were not categorized by age and gender precludes the ability for direct comparisons with our findings. It would be as well to acknowledge that with only just over half of the BS and general populations having been PCR tested, there may well be ascertainment biases that would make confidence in the comparison between the groups rather weak. Nevertheless, the incidence among BS patients as found in the current survey seems to be roughly two folds of that estimated for the general population living in Istanbul. In line with our findings, a multicentre retrospective study done among patients with RD found an increased infection rate compared to family members with no RD (OR 2.68, 95% CI 1.14–6.27%; p = 0.023) [25]. A meta-analysis of seven case–controlled studies demonstrated that the risk of COVID-19 in AD was significantly higher than in control patients (OR 2.19, 95% CI 1.05–4.58%, p = 0.038) [26]. Similarly, a nation-wide study from South Korea recently reported that patients with inflammatory arthritis had an increased risk of testing positive for SARS-CoV-2 (OR 1.20, 95% CI 1.03–1.40%; p = 0.020) compared to those without inflammatory arthritis [27]. Finally, the high incidence rate of COVID-19 in the BS cohort may be due to the ascertainment bias as we mentioned earlier. BS patients could be more likely to pay frequent visits to places with high risk such as hospitals, outpatients, emergency departments, family physicians or pharmacies. It could be also due to the fact that BS patients could have been less likely to ‘shield themselves from infection’ during the pandemic because of the obligation to go out for work or due to lower educational and socioeconomical status, as we have previously reported [28].
Despite our first report [14] with relatively small sample size (n = 10), we found a favorable outcome in this large prospective cohort of BS patients. Our current observations are also in contrast with a number of studies who reported increased risk for severe COVID-19 infection and COVID-19 related death among patients with RD [4, 26, 27]. In our study, while 18.7% had lung involvement, none of the patients died or had a thrombotic event. We are unable to explain the exact mechanisms responsible for the favorable outcome. High frequency of immunosuppressive use, meticulous follow-up, and better handling of the pandemic during the course could be possible explanations. It has to be noted that colchicine was used by almost 60% of the study population for many years, therefore, while it was not found to have any effect on contracting COVID-19 infection, it may still have an effect for the better outcome. Finally, as we said earlier, the fact that BS is not a typical AD, hence exerting a different immune dysregulation with mostly intact adaptive response might also contribute to the better outcome.
Our results show clearly that the COVID-19 infection did not provoke thrombotic events in BS. This is most probably due to different prothrombotic mechanisms operating in BS and COVID-19, despite the fact that both conditions are associated with substantial arterial and venous thrombotic risk [6, 10, 11, 29, 30]. Mehta et al. suggested that the pathogenesis of thrombosis in patients with COVID-19 pneumonia shares similarities with that in patients with BS [30]. Our study demonstrates that this hypothesis is quite unlikely. In BS, vascular wall inflammation, rather than a hypercoagulable state, seem to play major role in the background of thromboses [6, 30]. In COVID-19 on the other hand, direct viral effects, sepsis-induced hyperinflammatory state, the high levels of D- dimer and many other factors can trigger a coagulopathy [29].
There has been a lot of controversy about the association between the COVID-19 infection and the smoking status. Several cross-sectional studies and one meta-analyses showed that current smokers were less likely to have positive SARS-CoV-2 PCR test results whereas more likely to undergo SARS-CoV-2 PCR tests [31,32,33]. Several studies have shown lower prevalence of smoker status amongst COVID-19 patients and found a negative association between being a smoker and having COVID-19 [34, 35]. Similarly, a low prevalence of current smoker status among hospitalized COVID-19 patients was also observed [36]. Authors suggested that nicotine might be protective against the SARS-CoV-2 infection and once the infection is acquired, nicotinic stimulation might protect against severe forms of the disease by anti-inflammatory actions. These results should be taken with caution due to potential unreported cases of smokers and the fact that elderly population who has the greatest risk against COVID-19 has a lower prevalence of smokers than the general population [37]. On the other hand, many studies and analyses represented higher mortality and complications as well as the severe progression of the disease and worsening conditions among smoker COVID-19 patients [38, 39]. Smoking is reported to be a predisposal factor for various viral and bacterial respiratory tract infections supposedly by disrupting the epithelium, impairing the mucociliary clearance and diminishing the immune protections [40]. Among several theories about how smoking affects SARS-CoV2 infection, the interaction with a nicotinic acetylcholine receptor which is known to be expressed in airway cells is most frequently suggested [41]. While further studies are needed to elucidate the association between the nicotine exposure and COVID-19, we suggest that our findings should be interpreted with caution.
Interferon-alpha (IFNα) is known to have complex immunomodulatory as well as anti-viral actions. It has been shown to be effective in the BS management and in the treatment of virus-related diseases, particularly acute and chronic hepatitis B, and hepatitis C [42,43,44]. IFNα was tested for the treatment of COVID-19 and yielded promising results in line with our results [45, 46]. Recent studies also confirmed that patients having inborn errors of type 1 IFN-related genes and disrupted type 1 IFN response are susceptible to severe COVID-19 infection [47, 48].
Colchicine, an alkaloid, plant-derived secondary metabolite with anti-inflammatory effects, has been used in the treatment of BS, familial Mediterranean fever (FMF), gout, and several inflammatory disorders for decades [49, 50]. It exerts its actions mainly by inhibiting microtubule polymerization which has impacts on several cellular procedures such as signaling, proliferation, formation of the cellular shape, cellular movement, transfer, and migration [49]. It intervenes inflammatory pathways by inhibiting neutrophil adherence and recruitment to the site of inflammation, interfering with inflammasome activation which controls IL-1β-induced pathways [49]. It was also suggested to have some antiviral actions [51]. Throughout the COVID-19 pandemic, the use and efficacy of colchicine for the treatment of COVID-19 has been investigated in several studies. A number of them found a decreased rate of clinical worsening, hospitalization, and mortality [52,53,54]. Although rates of COVID-19 related hospital admissions and death did not show a significant decrease in the whole group in the COLCORONA study, these two parameters were significantly reduced in COVID-19 PCR confirmed colchicine-receiving group [55]. In two cohort studies, colchicine prescription was not found to have a significant protective or hazardous effect on COVID-19 related hospital admissions [56, 57]. Colchicine and COVID-19 association was reported in two case series with FMF [58, 59]. While the Turkish study [58] suggested that colchicine may decrease the symptoms of COVID-19, the French study [59] concluded that neither colchicine usage nor dysfunction of innate immunity composed a risk factor for COVID-19. In our study, we could not find any ameliorating or worsening effect of colchicine associated with COVID-19.
In line with the literature, we showed that chronic use of GC showed an adverse effect on COVID-19-related clinical outcomes [15, 26, 60]. On the other hand, both conventional DMARDs and anti-TNF agents were not found to be associated with an increased risk of getting COVID-19 or severe COVID-19 infection, similar to what have been previously reported [26, 60]. Additionally, we found that having comorbidities was associated with worse clinical outcome for COVID-19 as reported previously in several studies [61].
This study has several limitations. Lack of a diseased control group is an important one. Also, we were not able to compare our results directly with that found in the age and gender-matched general population. Our results may not be generalized for overall Turkey as 91.2% of the study cohort were living in Istanbul. We identified COVID-19 infection based on PCR test results. Therefore, we may have omitted some BS patients who may not have had a PCR test despite symptoms of COVID-19, especially when symptoms are mild. In addition, there is a small probability that PCR testing may have false-negative results.
Conclusions
Patients with BS have an increased risk of testing positive for SARS-CoV-2 suggesting caution during the follow-up these patients. Despite increased incidence, the clinical outcome of COVID-19 was not severe and there was no mortality. The protective effect of smoking and interferon should be investigated. Treatment with conventional DMARDs or anti-TNF agents was not associated with an increased risk of worse clinical outcomes. On the other hand, colchicine did not have any positive or negative effect against COVID-19. Considerable number of patients flared after COVID-19 however, this was significantly associated with immunosuppressive discontinuation during the infection. COVID-19 did not seem to exacerbate thrombotic events during or after the infection. Finally, the favorable outcome may suggest a possible role of a protective effect of BS itself or immune-modulating drugs.
References
https://www.worldometers.info/coronavirus/#countries. Accessed 7 September 2021
https://www.aa.com.tr/en/latest-on-coronavirus-outbreak/turkey-confirms-first-case-of-coronavirus/1761522. Accessed 11 March 2020
Ferri C, Giuggioli D, Raimondo V, L’Andolina M, Tavoni A, Cecchetti R, Guiducci S, Ursini F, Caminiti M, Varcasia G, Gigliotti P, Pellegrini R, Olivo D, Colaci M, Murdaca G, Brittelli R, Mariano GP, Spinella A, Bellando-Randone S, Aiello V, Bilia S, Giannini D, Ferrari T, Caminiti R, Brusi V, Meliconi R, Fallahi P, Antonelli A, COVID-19 & ASD Italian Study Group (2020) COVID-19 and rheumatic autoimmune systemic diseases: report of a large Italian patients series. Clin Rheumatol. 39(11):3195–3204. https://doi.org/10.1007/s10067-020-05334-7
Pablos JL, Galindo M, Carmona L, Lledó A, Retuerto M, Blanco R, Gonzalez-Gay MA, Martinez-Lopez D, Castrejón I, Alvaro-Gracia JM, Fernández Fernández D, Mera-Varela A, Manrique-Arija S, Mena Vázquez N, Fernandez-Nebro A, RIER Investigators Group; RIER investigators group (2020) Clinical outcomes of hospitalised patients with COVID-19 and chronic inflammatory and autoimmune rheumatic diseases: a multicentric matched cohort study. Ann Rheum Dis. 79(12):1544–1549. https://doi.org/10.1136/annrheumdis-2020-218296
Azizlerli G, Köse AA, Sarica R, Gül A, Tutkun IT, Kulaç M, Tunç R, Urgancioğlu M, Dişçi R (2003) Prevalence of Behçet’s disease in Istanbul. Turkey Int J Dermatol 42(10):803–806. https://doi.org/10.1046/j.1365-4362.2003.01893.x
Yazici H, Seyahi E, Hatemi G, Yazici Y (2018) Behçet syndrome: a contemporary view. Nat Rev Rheumatol. 14(2):107–119. https://doi.org/10.1038/nrrheum.2017.208 (Epub 2018 Jan 3. Erratum in: Nat Rev Rheumatol. 2018 Jan 24;14 (2):119)
Yazici H, Pazarli H, Barnes CG, Tüzün Y, Ozyazgan Y, Silman A, Serdaroğlu S, Oğuz V, Yurdakul S, Lovatt GE et al (1990) A controlled trial of azathioprine in Behçet’s syndrome. N Engl J Med 322(5):281–285. https://doi.org/10.1056/NEJM199002013220501 (PMID: 2404204)
Mat C, Yurdakul S, Uysal S, Gogus F, Ozyazgan Y, Uysal O, Fresko I, Yazici H (2006) A double-blind trial of depot corticosteroids in Behçet’s syndrome. Rheumatology (Oxford) 45(3):348–352. https://doi.org/10.1093/rheumatology/kei165 (Epub 2005 Nov 1 PMID: 16263779)
Tugal-Tutkun I, Mudun A, Urgancioglu M, Kamali S, Kasapoglu E, Inanc M, Gül A (2005) Efficacy of infliximab in the treatment of uveitis that is resistant to treatment with the combination of azathioprine, cyclosporine, and corticosteroids in Behçet’s disease: an open-label trial. Arthritis Rheum 52(8):2478–2484. https://doi.org/10.1002/art.21231 (PMID: 16052571)
Emmi G, Vitale A, Silvestri E, Boddi M, Becatti M, Fiorillo C, Fabiani C, Frediani B, Emmi L, Di Scala G, Goldoni M, Bettiol A, Vaglio A, Cantarini L, Prisco D (2018) Adalimumab-based treatment versus disease-modifying antirheumatic drugs for venous thrombosis in Behçet’s Syndrome: a Retrospective Study of Seventy Patients With Vascular Involvement. Arthritis Rheumatol 70(9):1500–1507. https://doi.org/10.1002/art.40531 (Epub 2018 Jul 19 PMID: 29676522)
Vallet H, Riviere S, Sanna A, Deroux A, Moulis G, Addimanda O, Salvarani C, Lambert M, Bielefeld P, Seve P, Sibilia J, Pasquali J, Fraison J, Marie I, Perard L, Bouillet L, Cohen F, Sene D, Schoindre Y, Lidove O, Le Hoang P, Hachulla E, Fain O, Mariette X, Papo T, Wechsler B, Bodaghi B, Rigon MR, Cacoub P, Saadoun D, French Behçet Network (2015) Efficacy of anti-TNF alpha in severe and/or refractory Behçet’s disease: Multicenter study of 124 patients. J Autoimmun 62:67–74. https://doi.org/10.1016/j.jaut.2015.06.005
Yurdakul S, Mat C, Tüzün Y, Ozyazgan Y, Hamuryudan V, Uysal O, Senocak M, Yazici H (2001) A double-blind trial of colchicine in Behçet’s syndrome. Arthritis Rheum 44(11):2686–2692. https://doi.org/10.1002/1529-0131(200111)44:11%3c2686::aid-art448%3e3.0.co;2-h (PMID: 11710724)
Davatchi F, Sadeghi Abdollahi B, Tehrani Banihashemi A, Shahram F, Nadji A, Shams H, Chams-Davatchi C (2009) Colchicine versus placebo in Behçet’s disease: randomized, double-blind, controlled crossover trial. Mod Rheumatol 19(5):542–549. https://doi.org/10.1007/s10165-009-0200-2 (Epub 2009 Jul 14 PMID: 19597921)
Yurttaş B, Oztas M, Tunc A, Balkan İİ, Tabak OF, Hamuryudan V, Seyahi E (2020) Characteristics and outcomes of Behçet’s syndrome patients with Coronavirus Disease 2019: a case series of 10 patients. Intern Emerg Med 15(8):1567–1571. https://doi.org/10.1007/s11739-020-02427-8 (Epub 2020 Jul 9)
Esatoglu SN, Tascilar K, Babaoğlu H, Bes C, Yurttas B, Akar S, Pehlivan O, Akleylek C, Tecer D, Seyahi E, Yuce-Inel T, Alpay-Kanitez N, Bodakci E, Tekgoz E, Colak S, Bolek EC, Koca SS, Kalyoncu U, Icacan OC, Ugurlu S, Oz HE, Hamuryudan V, Hatemi G, Turkish Society for Rheumatology COVID-19 Registry Investigators (2021) COVID-19 among patients with inflammatory rheumatic diseases. Front Immunol. 12:651715. https://doi.org/10.3389/fimmu.2021.651715
Mattioli I, Bettiol A, Silvestri E, Urban ML, Palermo A, Fagni F, Malandrino D, Del Bianco A, Prisco D, Emmi G (2021) Prevalence and clinical course of SARS-CoV-2 infection in patients with Behçet’s syndrome. Clin Exp Rheumatol. 132(5):47–50 (Epub 2021 Jun 9. PMID: 34128795.)
Espinosa G, Araujo O, Amaro S, Bodro M, Moreno PJ, Moreno R, Ugarte A, Cervera R (2020) COVID-19 and Behçet’s disease: clinical case series. Ann Rheum Dis. https://doi.org/10.1136/annrheumdis-2020-217778
Zouboulis CC, van Laar JAM, Schirmer M, Emmi G, Fortune F, Gül A, Kirino Y, Lee ES, Sfikakis PP, Shahram F, Wallace GR (2021) Adamantiades-Behçet’s disease (Behçet’s disease) and COVID-19. J Eur Acad Dermatol Venereol 35(9):e541–e543. https://doi.org/10.1111/jdv.17325
https://covid19asi.saglik.gov.tr/TR-77707/asi-uygulanacak-grup-siralamasi.html. Accessed 27 March 2021
https://covid19.saglik.gov.tr/TR-66301/covid-19-rehberi.html. Accessed 2020˗2021
Emmi G, Bettiol A, Mattioli I, Silvestri E, Di Scala G, Urban ML, Vaglio A, Prisco D (2020) SARS-CoV-2 infection among patients with systemic autoimmune diseases. Autoimmun Rev 19(7):102575. https://doi.org/10.1016/j.autrev.2020.102575
Daniel WW (1999) Biostatistics: a foundation for analysis in the health sciences, 7th edn. Wiley, New York
https://covid19.saglik.gov.tr/TR-66935/genel-koronavirus-tablosu.html. Accessed September 2021
https://data.tuik.gov.tr/Bulten/Index?p=37210. Accessed September 2021
Zhong J, Shen G, Yang H, Huang A, Chen X, Dong L, Wu B, Zhang A, Su L, Hou X, Song S, Li H, Zhou W, Zhou T, Huang Q, Chu A, Braunstein Z, Rao X, Ye C, Dong L (2020) COVID-19 in patients with rheumatic disease in Hubei province, China: a multicentre retrospective observational study. Lancet Rheumatol 2(9):e557–e564. https://doi.org/10.1016/S2665-9913(20)30227-7
Akiyama S, Hamdeh S, Micic D, Sakuraba A (2020) Prevalence and clinical outcomes of COVID-19 in patients with autoimmune diseases: a systematic review and meta-analysis. Ann Rheum Dis. https://doi.org/10.1136/annrheumdis-2020-218946
Shin YH, Shin JI, Moon SY, Jin HY, Kim SY, Yang JM, Cho SH, Kim S, Lee M, Park Y, Kim MS, Won HH, Hong SH, Kronbichler A, Koyanagi A, Jacob L, Smith L, Lee KH, Suh DI, Lee SW, Yon DK (2021) Autoimmune inflammatory rheumatic diseases and COVID-19 outcomes in South Korea: a nationwide cohort study. Lancet Rheumatol 3(10):e698–e706. https://doi.org/10.1016/S2665-9913(21)00151-X
Seyahi E, Poyraz BC, Sut N, Akdogan S, Hamuryudan V (2020) The psychological state and changes in the routine of the patients with rheumatic diseases during the coronavirus disease (COVID-19) outbreak in Turkey: a web-based cross-sectional survey. Rheumatol Int 40(8):1229–1238. https://doi.org/10.1007/s00296-020-04626-0
Miesbach W, Makris M (2020) COVID-19: coagulopathy, risk of thrombosis, and the rationale for anticoagulation. Clin Appl Thromb Hemost. https://doi.org/10.1177/1076029620938149 (PMID: 32677459; PMCID: PMC7370334)
Mehta P, Haskard DO, Laffan MA, Chambers RC, Hunt BJ (2021) Thromboses and COVID-19: reducing inflammation in addition to thromboprophylaxis. Lancet Rheumatol. 3(3):e171–e172. https://doi.org/10.1016/S2665-9913(21)00003-5 (Epub 2021 Jan 7. PMID: 33521654; PMCID: PMC7832098)
Rentsch CT, Kidwai-Khan F, Tate JP, Park LS, King JT Jr, Skanderson M, Hauser RG, Schultze A, Jarvis CI, Holodniy M, Lo RV 3rd, Akgün KM, Crothers K, Taddei TH, Freiberg MS, Justice AC (2020) Patterns of COVID-19 testing and mortality by race and ethnicity among United States veterans: a nationwide cohort study. PLoS Med. 17(9):e1003379. https://doi.org/10.1371/journal.pmed.1003379 (PMID: 32960880; PMCID: PMC7508372)
Trubiano JA, Vogrin S, Smibert OC, Marhoon N, Alexander AA, Chua KYL, James FL, Jones NRL, Grigg SE, Xu CLH, Moini N, Stanley SR, Birrell MT, Rose MT, Gordon CL, Kwong JC, Holmes NE (2020) COVID-MATCH65-A prospectively derived clinical decision rule for severe acute respiratory syndrome coronavirus 2. PLoS ONE 15(12):e0243414. https://doi.org/10.1371/journal.pone.0243414
Simons D, Shahab L, Brown J, Perski O (2021) The association of smoking status with SARS-CoV-2 infection, hospitalization and mortality from COVID-19: a living rapid evidence review with Bayesian meta-analyses (version 7). Addiction 116(6):1319–1368. https://doi.org/10.1111/add.15276
Tsigaris P, Teixeira da Silva JA (2020) Smoking Prevalence and COVID-19 in Europe. Nicotine Tob Res. https://doi.org/10.1093/ntr/ntaa121
González-Rubio J, Navarro-López C, López-Nájera E, López-Nájera A, Jiménez-Díaz L, Navarro-López JD, Nájera A (2020) A systematic review and meta-analysis of hospitalised current smokers and COVID-19. Int J Environ Res Public Health 17(20):7394. https://doi.org/10.3390/ijerph17207394
Farsalinos K, Barbouni A, Poulas K, Polosa R, Caponnetto P, Niaura R (2020) Current smoking, former smoking, and adverse outcome among hospitalized COVID-19 patients: a systematic review and meta-analysis. Ther Adv Chronic Dis 25(11):2040622320935765. https://doi.org/10.1177/2040622320935765
Leung JM, Yang CX, Sin DD (2020) Reply to: “Current smoking is not associated with COVID-19.” Eur Respir J 55(6):2001340. https://doi.org/10.1183/13993003.01340-2020
Reddy RK, Charles WN, Sklavounos A, Dutt A, Seed PT, Khajuria A (2021) The effect of smoking on COVID-19 severity: a systematic review and meta-analysis. J Med Virol 93(2):1045–1056. https://doi.org/10.1002/jmv.26389
Patanavanich R, Glantz SA (2020) Smoking is associated With COVID-19 progression: a meta-analysis. Nicotine Tob Res 22(9):1653–1656. https://doi.org/10.1093/ntr/ntaa082
Dye JA, Adler KB (1994) Effects of cigarette smoke on epithelial cells of the respiratory tract. Thorax 49(8):825–834. https://doi.org/10.1136/thx.49.8.825
Russo P, Bonassi S, Giacconi R, Malavolta M, Tomino C, Maggi F (2020) COVID-19 and smoking: is nicotine the hidden link? Eur Respir J 55(6):2001116. https://doi.org/10.1183/13993003.01116-2020
Yang DS, Taylor SR, Lightman SL (2008) Interferon-alpha in the management of patients with Behçet’s disease. Br J Hosp Med (Lond) 69(10):575–579. https://doi.org/10.12968/hmed.2008.69.10.31317
Lai L, Hui CK, Leung N, Lau GK (2006) Pegylated interferon alpha-2a (40 kDa) in the treatment of chronic hepatitis B. Int J Nanomedicine. 1(3):255–62 (PMID: 17717966; PMCID: PMC2426802)
Feld JJ (2012) Treatment indication and response to standard of care with peginterferon and ribavirin in acute and chronic HCV infection. Best Pract Res Clin Gastroenterol 26(4):429–444. https://doi.org/10.1016/j.bpg.2012.09.013
Zhou Q, Chen V, Shannon CP, Wei XS, Xiang X, Wang X, Wang ZH, Tebbutt SJ, Kollmann TR, Fish EN (2020) Corrigendum: interferon-α2b treatment for COVID-19. Front Immunol 27(11):615275. https://doi.org/10.3389/fimmu.2020.615275.Erratumfor:FrontImmunol.2020May15;11:1061
Loutfy MR, Blatt LM, Siminovitch KA, Ward S, Wolff B, Lho H, Pham DH, Deif H, LaMere EA, Chang M, Kain KC, Farcas GA, Ferguson P, Latchford M, Levy G, Dennis JW, Lai EK, Fish EN (2003) Interferon alfacon-1 plus corticosteroids in severe acute respiratory syndrome: a preliminary study. JAMA 290(24):3222–3228. https://doi.org/10.1001/jama.290.24.3222
Zhang Q, Bastard P, Liu Z et al (2020) Inborn errors of type I IFN immunity in patients with life-threatening COVID-19. Science. https://doi.org/10.1126/science.abd4570
Hadjadj J, Yatim N, Barnabei L, Corneau A, Boussier J, Smith N, Péré H, Charbit B, Bondet V, Chenevier-Gobeaux C, Breillat P, Carlier N, Gauzit R, Morbieu C, Pène F, Marin N, Roche N, Szwebel TA, Merkling SH, Treluyer JM, Veyer D, Mouthon L, Blanc C, Tharaux PL, Rozenberg F, Fischer A, Duffy D, Rieux-Laucat F, Kernéis S, Terrier B (2020) Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients. Science 369(6504):718–724. https://doi.org/10.1126/science.abc6027
Angelidis C, Kotsialou Z, Kossyvakis C, Vrettou AR, Zacharoulis A, Kolokathis F, Kekeris V, Giannopoulos G (2018) Colchicine Pharmacokinetics and Mechanism of Action. Curr Pharm Des 24(6):659–663. https://doi.org/10.2174/1381612824666180123110042
Cocco G, Chu DC, Pandolfi S (2010) Colchicine in clinical medicine. A guide for internists. Eur J Intern Med. 21(6):503–8. https://doi.org/10.1016/j.ejim.2010.09.010
Richter M, Boldescu V, Graf D, Streicher F, Dimoglo A, Bartenschlager R, Klein CD (2019) Synthesis, biological evaluation, and molecular docking of combretastatin and colchicine derivatives and their hCE1-Activated Prodrugs as Antiviral Agents. ChemMedChem 14(4):469–483. https://doi.org/10.1002/cmdc.201800641
Deftereos SG, Giannopoulos G, Vrachatis DA, Siasos GD, Giotaki SG, Gargalianos P, Metallidis S, Sianos G, Baltagiannis S, Panagopoulos P, Dolianitis K, Randou E, Syrigos K, Kotanidou A, Koulouris NG, Milionis H, Sipsas N, Gogos C, Tsoukalas G, Olympios CD, Tsagalou E, Migdalis I, Gerakari S, Angelidis C, Alexopoulos D, Davlouros P, Hahalis G, Kanonidis I, Katritsis D, Kolettis T, Manolis AS, Michalis L, Naka KK, Pyrgakis VN, Toutouzas KP, Triposkiadis F, Tsioufis K, Vavouranakis E, Martinèz-Dolz L, Reimers B, Stefanini GG, Cleman M, Goudevenos J, Tsiodras S, Tousoulis D, Iliodromitis E, Mehran R, Dangas G, Stefanadis C, GRECCO-19 investigators (2020) Effect of Colchicine vs Standard Care on Cardiac and Inflammatory Biomarkers and Clinical Outcomes in Patients Hospitalized With Coronavirus Disease 2019: The GRECCO-19 Randomized Clinical Trial. JAMA Netw Open. 3(6):2013136. https://doi.org/10.1001/jamanetworkopen.2020.13136
Manenti L, Maggiore U, Fiaccadori E, Meschi T, Antoni AD, Nouvenne A, Ticinesi A, Cerundolo N, Prati B, Delsante M, Gandoflini I, Donghi L, Gentile M, Farina MT, Oliva V, Zambrano C, Regolisti G, Palmisano A, Caminiti C, Cocchi E, Ferrari C, Riella LV, Cravedi P, Peruzzi L (2021) Reduced mortality in COVID-19 patients treated with colchicine: results from a retrospective, observational study. PLoS ONE 16(3):e0248276. https://doi.org/10.1371/journal.pone.0248276
Lopes MI, Bonjorno LP, Giannini MC, Amaral NB, Menezes PI, Dib SM, Gigante SL, Benatti MN, Rezek UC, Emrich-Filho LL, Sousa BAA, Almeida SCL, Luppino Assad R, Veras FP, Schneider A, Rodrigues TS, Leiria LOS, Cunha LD, Alves-Filho JC, Cunha TM, Arruda E, Miranda CH, Pazin-Filho A, Auxiliadora-Martins M, Borges MC, Fonseca BAL, Bollela VR, Del-Ben CM, Cunha FQ, Zamboni DS, Santana RC, Vilar FC, Louzada-Junior P, Oliveira RDR (2021) Beneficial effects of colchicine for moderate to severe COVID-19: a randomised, double-blinded, placebo-controlled clinical trial. RMD Open 7(1):e001455. https://doi.org/10.1136/rmdopen-2020-001455
Tardif JC, Bouabdallaoui N, L’Allier PL, Gaudet D, Shah B, Pillinger MH, Lopez-Sendon J, da Luz P, Verret L, Audet S, Dupuis J, Denault A, Pelletier M, Tessier PA, Samson S, Fortin D, Tardif JD, Busseuil D, Goulet E, Lacoste C, Dubois A, Joshi AY, Waters DD, Hsue P, Lepor NE, Lesage F, Sainturet N, Roy-Clavel E, Bassevitch Z, Orfanos A, Stamatescu G, Grégoire JC, Busque L, Lavallée C, Hétu PO, Paquette JS, Deftereos SG, Levesque S, Cossette M, Nozza A, Chabot-Blanchet M, Dubé MP, Guertin MC, Boivin G, COLCORONA Investigators (2021) Colchicine for community-treated patients with COVID-19 (COLCORONA): a phase 3, randomised, double-blinded, adaptive, placebo-controlled, multicentre trial. Lancet Respir Med. 9(8):924–932. https://doi.org/10.1016/S2213-2600(21)00222-8
Gendelman O, Amital H, Bragazzi NL, Watad A, Chodick G (2020) Continuous hydroxychloroquine or colchicine therapy does not prevent infection with SARS-CoV-2: Insights from a large healthcare database analysis. Autoimmun Rev 19(7):102566. https://doi.org/10.1016/j.autrev.2020.102566
Madrid-García A, Pérez I, Colomer JI, León-Mateos L, Jover JA, Fernández-Gutiérrez B, Abásolo-Alcazar L, Rodríguez-Rodríguez L (2021) Influence of colchicine prescription in COVID-19-related hospital admissions: a survival analysis. Ther Adv Musculoskelet Dis. https://doi.org/10.1177/1759720X211002684
Nas K, Eryilmaz N, Geyik MF, Altaş A (2021) COVID-19 in patients with familial Mediterranean fever treated with colchicine: case based review. Rheumatol Int 41(4):811–817. https://doi.org/10.1007/s00296-021-04809-3
Bourguiba R, Delplanque M, Vinit C, Ackermann F, Savey L, Grateau G, Hentgen V, Georgin-Lavialle S (2020) Clinical course of COVID-19 in a cohort of 342 familial Mediterranean fever patients with a long-term treatment by colchicine in a French endemic area. Ann Rheum Dis. https://doi.org/10.1136/annrheumdis-2020-218707
Hyrich KL, Machado PM (2021) Rheumatic disease and COVID-19: epidemiology and outcomes. Nat Rev Rheumatol 17(2):71–72. https://doi.org/10.1038/s41584-020-00562-2.PMID:33339986;PMCID:PMC7747184
Jain V, Yuan JM (2020) Predictive symptoms and comorbidities for severe COVID-19 and intensive care unit admission: a systematic review and meta-analysis. Int J Public Health 65(5):533–546. https://doi.org/10.1007/s00038-020-01390-7
Acknowledgements
We are indebted to Prof. Dorian Haskard (Cardiovascular Medicine, Imperial College, London, UK) for critical reading the manuscript and helpful discussion. We thank Prof. Recep Ozturk (Infectious Diseases, Medipol University, Istanbul, Turkey) and Ass. Prof Gunay Can (Public Health’s Department, University of Istanbul-C, Cerrahpasa Medical Faculty) for constructive comments. We wish to thank Ali Cetin Ezber for his assistance in reaching and contacting patients. Thanks are also due to the patients for their participation in this study.
Funding
We did not receive any financial support.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by GO, TA, ZA, IIB, FT, MO, YO, SU, GH, MM, IF, VH and ES. The first draft of the manuscript was written by GO and ES and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Guzin Ozcifci, Tahacan Aydin, Zeynep Atli, Ilker Inanc Balkan, Mert Oztas, Yesim Ozguler, Melike Melikoglu, Izzet Fresko and Vedat Hamuryudan declare that they have no conflict of interest. Fehmi Tabak, has received honoraria, consulting or speaker fees from GSK, MSD, AbbVie and Gilead. Serdal Ugurlu has received honoraria, consulting or speaker fees from Novartis, Pfizer, Lilly and Celltrion. Gulen Hatemi has received research grant from Celgene, honoraria consulting or speaker fees from AbbVie, Amgen, Celgene, Lilly, Novartis and UCB Pharma. Emire Seyahi has received honoraria, consulting or speaker fees from Novartis, Pfizer, AbbVie and Gilead.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Ozcifci, G., Aydin, T., Atli, Z. et al. The incidence, clinical characteristics, and outcome of COVID-19 in a prospectively followed cohort of patients with Behçet’s syndrome. Rheumatol Int 42, 101–113 (2022). https://doi.org/10.1007/s00296-021-05056-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-021-05056-2