
Abstract
Purpose
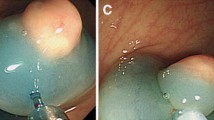
Although small rectal carcinoid tumors can be treated using local excision, complete resection can be difficult because tumors are located in the submucosal layer. We evaluate the factors associated with pathologically complete local resection of rectal carcinoid tumors.
Methods
Data were analyzed of 161 patients with 166 rectal carcinoid tumors who underwent local excision with curative intent from January 2001 to December 2010. A pathologically complete resection (P-CR) was defined as an en bloc resection with tumor-free lateral and deep margins. The study classified treatments into three categories for analysis: conventional polypectomy (including strip biopsy, snare polypectomy, and hot biopsy), advanced endoscopic techniques (including endoscopic mucosal resection with cap and endoscopic submucosal dissection), and surgical local excision (including transanal excision and transanal endoscopic microsurgery). We evaluated the P-CR rate according to treatment method, tumor size, initial endoscopic impression and the use of endoscopic ultrasound (EUS) or transrectal ultrasound (TRUS).
Results
The mean tumor size was 5.51 ± 2.43 mm (range 2–18 mm) and all lesions were confined to the submucosal layer. The P-CR rates were 30.9, 72.0, and 81.8 % for conventional polypectomy, advanced endoscopic techniques, and surgical local excision, respectively. Univariate analysis showed that P-CR was associated with treatment method, use of EUS or TRUS, and initial endoscopic impression. Multivariate analysis showed that only treatment method was associated with P-CR.
Conclusion
Pathologically complete resection of small rectal carcinoid tumors was more likely to be achieved when using advanced endoscopic techniques or surgical local excision rather than conventional polypectomy.
Similar content being viewed by others


References
Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, Abdalla EK, Fleming JB, Vauthey JN, Rashid A, Evans DB (2008) One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 26:3063–3072
Scherübl H (2009) Rectal carcinoids are on the rise: early detection by screening endoscopy. Endoscopy 41:162–165
Higaki S, Nishiaki M, Mitani N, Yanai H, Tada M, Okita K (1997) Effectiveness of local endoscopic resection of rectal carcinoid tumors. Endoscopy 29:171–175
Ishikawa H, Imanishi K, Otani T, Okuda S, Tatsuta M, Ishiguro S (1989) Effectiveness of endoscopic treatment of carcinoid tumors of the rectum. Endoscopy 21:133–135
Soga J (2005) Early-stage carcinoids of the gastrointestinal tract: an analysis of 1914 reported cases. Cancer 103:1587–1595
Modlin IM, Kidd M, Latich I, Zikusoka MN, Shapiro MD (2005) Current status of gastrointestinal carcinoids. Gastroenterology 128:1717–1751
Ono A, Fujii T, Saito Y, Matsuda T, Lee DT, Gatoda T, Saito D (2003) Endoscopic submucosal resection of rectal carcinoid tumors with a ligation device. Gastrointest Endosc 57:583–587
Nagai T, Torishima R, Nakashima H, Ookawara H, Uchida A, Kai S, Sato R, Murakami K, Fujioka T (2004) Saline-assisted endoscopic resection or rectal carcinoids: cap aspiration method versus simple snare resection. Endoscopy 36:202–205
Kajiyama T, Hajiro K, Sakai M, Inoue K, Konishi Y, Takakuwa H, Ueda S, Okuma M (1996) Endoscopic resection of gastrointestinal submucosal lesions: a comparison between strip biopsy and aspiration lympectomy. Gastrointest Endosc 44:404–410
Imada-Shirakata Y, Sakai M, Kajiyama T, Kin G, Inoue K, Torii A, Kishimoto H, Ueda S, Okuma M (1996) Endoscopic resection of rectal carcinoid tumors using aspiration lumpectomy. Endoscopy 29:34–38
Oshitani N, Hamasaki N, Sawa Y, Hara J, Nakamura S, Matsumoto T, Kitano A, Arakawa T (2000) Endoscopic resection of small rectal carcinoid tumours using aspiration method with a transparent overcap. J Int Med Res 28:241–246
Onozato Y, Kakizaki S, Ishihara H, Iizuka H, Sohara N, Okamura S, Mori M, Itoh H (2007) Endoscopic submucosal dissection for rectal tumors. Endoscopy 39:423–427
Sohn DK, Han KS, Hong CW, Chang HJ, Jeong SY, Park JG (2008) Selection of cap size in endoscopic submucosal resection with cap aspiration for rectal carcinoid tumors. J Laparoendosc Adv Surg Tech A 18:815–818
Moon SH, Hwang JH, Sohn DK, Park JW, Hong CW, Han KS, Chang HJ, Oh JH (2011) Endoscopic submucosal dissection for rectal neuroendocrine (carcinoid) tumors. J Laparoendosc Adv Surg Tech A 21:695–699
Lee DS, Jeon SW, Park SY, Jung MK, Cho CM, Tak WY, Kweon YO, Kim SK (2010) The feasibility of endoscopic submucosal dissection for rectal carcinoid tumors: comparison with endoscopic mucosal resection. Endoscopy 42:647–651
Park HW, Byeon JS, Park YS, Yang DH, Yoon SM, Kim KJ, Ye BD, Myung SJ, Yang SK, Kim JH (2010) Endoscopic submucosal dissection for treatment of rectal carcinoid tumors. Gastrointest Endosc 72:143–149
Zhou PH, Yao LQ, Qin XY, Xu MD, Zhong YS, Chen WF, Ma LL, Zhang YQ, Qin WZ, Cai MY, Ji Y (2010) Advantages of endoscopic submucosal dissection with needle-knife over endoscopic mucosal resection for small rectal carcinoid tumors: a retrospective study. Surg Endosc 24:2607–2612
Fahy BN, Tang LH, Klimstra D, Wong WD, Guillem JG, Paty PB, Temple LK, Shia J, Weiser MR (2007) Carcinoid of the rectum risk stratification(CaRRs): a strategy for preoperative outcome assessment. Ann Surg Oncol 14:1735–1743
Jetmore AB, Ray JE, Gathright JB Jr, McMullen KM, Hicks TC, Timmcke AE (1992) Rectal carcinoids: the most frequent carcinoid tumor. Dis Colon Rectum 35:717–725
Acknowledgments
This study was supported in part by the National Cancer Center Grant (grant No. 0910520).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Son, HJ., Sohn, D.K., Hong, C.W. et al. Factors associated with complete local excision of small rectal carcinoid tumor. Int J Colorectal Dis 28, 57–61 (2013). https://doi.org/10.1007/s00384-012-1538-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-012-1538-z